
Abstract
Purpose
To analyze the influence of training status on the percentage of maximum oxygen consumption, heart rate and velocity (%VO2max, %HRmax and %Vmax) at which ventilatory threshold 1 and ventilatory threshold 2 occur (VT1 and VT2, respectively), in males and females separately considering age, during a ramp incremental treadmill test.
Methods
791 males (36.8 ± 9.9 years) and 301 females (33.9 ± 11.0 years) performed a ramp incremental exercise test until fatigue where VT1 and VT2 were determined. Participants were classified as low, medium or high training status combining the oxygen consumption at VT1, VT2 and VO2max by clustering analysis.
Results
VO2max is poorly correlated with the %VO2max, %HRmax and %Vmax at which VT1 and VT2 occur (r < 0.3), in contrast, there is a positive correlation between oxygen consumption at VT1 and VT2 with the %VO2max, %HRmax and %Vmax at which VT1 and VT2, respectively, occur in males and females (r = 0.203–0.615). Furthermore, we observed the %VO2max, %HRmax and %Vmax at which thresholds occur were greater the higher the training status (all p < 0.003).
Conclusion
The physiological determinants of the percentage of maximum at which VT1 and VT2 occur are more related to oxygen consumption at VT1 and VT2, respectively, than to VO2max. Moreover, due to the higher percentage of maximum at which VT1 and VT2 occur in individuals with a higher training status, the common strategy consisting of establishing exercise intensity as a fixed percentage of maximum might not be effective to match intensity across individuals with different training status.
Clinical trial registration
NCT06246760.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Among the most common variables used to prescribe exercise intensity is oxygen uptake (VO2). Alternatively, when oxygen uptake measurement is not available, exercise intensity is determined using heart rate (HR) and work rate [power output or velocity (V)]. Traditionally, exercise intensity has been prescribed as a fixed percentage of maximal oxygen uptake (%VO2max), maximal heart rate (%HRmax), and maximum power output (%Wmax) or velocity (%Vmax). These variables are usually expressed relative to their maximum values with the intention of matching intensity between individuals with different training statuses (Mann et al. 2013). It is assumed that exercise performed at the same percentage of maximum produces the same physiological stress across individuals with different training statuses. This strategy is commonly used in recent studies (Coates et al. 2023) and general guidelines (Haskell et al. 2007; Garber et al. 2011).
However, during a graded exercise test, different intensity training zones can be distinguished (moderate, heavy, and severe). These training zones can be identified during an incremental test by determining the first and second thresholds (Meyer et al. 2005; Keir et al. 2015; Weatherwax et al. 2019; Iannetta et al. 2020). The transition from moderate to heavy intensity is indicated by the first threshold, determined through the first lactate or ventilatory threshold (LT1 and VT1, respectively). The transition from heavy to severe intensity is indicated by the second lactate or ventilatory threshold (LT2 and VT2, respectively) (Keir et al. 2022).
Exercise intensity prescription as a fixed percentage of maximum may not be effective if the percentages at which thresholds occur differ between individuals (Meyler et al. 2023). Thus, it is possible that individuals with different threshold percentages could be in different training zones at the same percentage of maximum (Meyler et al. 2023). In this scenario, exercising at the same percentage of maximum would not generate the same physiological stress for everyone due to their differing training zones. An excellent study by Iannetta et al. demonstrated that the percentage of maximum at which thresholds occurred (%VO2max, %HRmax, and %Wmax) varied widely among both males and females, with sex being one of the factors influencing this variability (Iannetta et al. 2020). Despite analyzing males and females separately, they still observed a wide range of percentages at which thresholds occurred (Iannetta et al. 2020). This suggests the potential existence of additional factors contributing to these percentages, highlighting the need to elucidate which factors influence this variation. Contrary to traditional assumptions, they proposed that exercise intensity thresholds do not necessarily occur at higher percentages of VO2max in individuals with higher fitness levels (Iannetta et al. 2020). On the contrary, it has been demonstrated that percentages of VO2max at which thresholds occur are higher in the middle compared to the beginning of the training season, but not significantly different at the end compared to the middle (Zapico et al. 2007). Given these seemingly contradictory findings, it is paramount to determine whether training status affects the percentage of VO2max at which thresholds occur across individuals with varying training statuses, ideally in a study with a large sample size. Moreover, to the best of our knowledge, there is a lack of studies examining differences in the percentage of HRmax and Vmax at which thresholds occur according to training status. If training status impacts the percentage of VO2max, HRmax and Vmax at which thresholds occur, intensity could not be set as a percentage of VO2max, HRmax and Vmax to standardize intensity across individuals with different training status.
On the other hand, while we acknowledge the existence of other articles with larger sample sizes that provide reference standard values for some of the variables discussed in the present study, these variables are typically stratified by sex and age (Loe et al. 2013; Vainshelboim et al. 2020), but not by training status. Therefore, understanding the reference standard values of these variables according to training status would be valuable for interpreting an individual’s fitness level more accurately. Previous studies have already demonstrated that sex (Iannetta et al. 2020; Vainshelboim et al. 2020), age (Vainshelboim et al. 2020), and ergometer type (Vainshelboim et al. 2020) influence the variables used to determine training zones, suggesting that they should be taken into account when investigating the impact of training status.
Thus, the aim of the present study is to analyze the influence of training status on different variables (VO2, HR, and V) expressed relative to their maximum values, used to indicate the first and second ventilatory thresholds (VT1 and VT2, respectively), separately for males and females, while also considering age, during a ramp incremental treadmill test. In addition, we offer reference values for these same variables and additional variables according to training status, leveraging the large sample size.
Materials and methods
Participants
This study involved 971 males (75.4 ± 9.6 kg, 175.9 ± 6.7 cm, and 36.8 ± 9.9 years) and 301 females (58.8 ± 7.9 kg, 163.9 ± 5.9 cm, and 33.9 ± 11.0 years) who voluntarily visited our laboratory to undergo an exercise test. Data were collected between 2003 and 2023. Participants were instructed to abstain from vigorous exercise for 2 days prior to the test and to eat at least 2 h before the test. All participants received detailed information about the potential risks and benefits of the study and provided written informed consent to participate. The protocols and procedures were approved by the Ethical Principles for Medical Research Involving Human Subjects of the World Medical Association Declaration of Helsinki (1964) and subsequent amendments. This study was approved by the Human Research Ethics Committee of the Universidad Politécnica de Madrid. Data and information obtained in the project were treated as confidential in accordance with current national legislation governing personal data protection (Organic Law 3/2018). Therefore, access to the database was restricted to researchers involved in the study. Clinical trial registration: NCT06246760.
Procedures
Ramp incremental exercise test
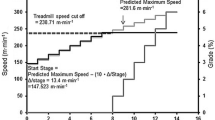
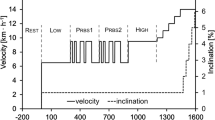
The ramp incremental exercise test was performed on a computerized treadmill (H/P/COSMOS 3PW 4.0, H/P/Cosmos Sports & Medical, Nussdorf-Traunstein, Germany). The incremental tests were tailored to each participant’s training experience (sporting background) to accurately determine VT1, VT2, and VO2max. Two primary considerations guided the individualization process: first, to avoid excessively long protocols (> ~ 26 min) for well-trained individuals, which could hinder reaching VO2max due to fatigue (Midgley et al. 2008), and second, to prevent overly demanding protocols for poorly trained individuals, which could impede the proper determination of VT1 and VT2 due to protocol duration being too short (Bentley et al. 2007). The test commenced with a three-minute warm-up at a constant intensity between 4 and 6 km/h. Subsequently, the incremental phase involved a ramp test starting from 4 to 8 km/h, with the velocity increasing by 1–1.5 km/h per minute. The incremental phase concluded when the participant could no longer maintain the treadmill velocity. Finally, a 3-min active recovery at the same intensity as the warm-up was followed by a 2-min passive recovery period. Throughout the test, breath-by-breath oxygen consumption (VO2) and beat-by-beat heart rate (HR) were analyzed using a Jaeger Oxycon Pro (Erich Jaeger, Viasys Healthcare, Friedberg, Germany) and JAEGER® Vyntus CPX (Jaeger-CareFusion, Hoechberg, Germany), respectively, previously calibrated according to the manufacturer’s specifications.
Data extracted from incremental tests
VT1 and VT2 were determined as previously published (Rabadán et al. 2011). In brief, VT1 was calculated using: a) the V-slope method, where VT1 represents the breakpoint of the VCO2/VO2 relationship; b) the first exponential increment in ventilation (VE) relative to time; and c) the first increase in the VE/VO2 relationship without accompanying increases in the VE/VCO2 relationship relative to time. VT2 was determined: a) as the second exponential increment in ventilation relative to time; b) as the intensity corresponding to the second increase in the VE/VO2 relationship alongside a concurrent rise in the VE/VCO2 relationship relative to time. VO2max was established as the highest value averaged every 15 s. VO2max was considered achieved if three of the following four criteria were met: voluntary exhaustion of the participant, HR ≥ 95% of the theoretical HRmax calculated as 220 minus the age, RER ≥ 1.10, and a plateau in VO2 despite an increase in exercise intensity (Poole et al. 2008). All tests were independently evaluated by two researchers, with a third researcher included in cases of disagreement. The following variables were determined: oxygen consumption values at VT1 (VO2VT1), VT2 (VO2VT2), and maximum (VO2max) relative to body weight; percentage of maximal oxygen consumption at VT1 (%VO2max VT1) and VT2 (%VO2max VT2); absolute heart rate at VT1 (HRVT1), VT2 (HRVT2), and maximum (HRmax); percentage of maximal heart rate at VT1 (%HRmax VT1) and VT2 (%HRmax VT2); velocity at VT1 (VVT1), VT2 (VVT2), and maximum (Vmax); and percentage of maximal velocity at VT1 (%Vmax VT1) and VT2 (%Vmax VT2).
Training status classification
Oxygen consumption at each threshold and maximum was chosen to determine training status for two reasons: (a) its significant impact on health and performance (Poole et al. 2021); and (b) because the exercise protocol appears not to influence VO2VT1, VO2VT2, and VO2max (Scheuermann and Kowalchuk 1998; Leo et al. 2017; Iannetta et al. 2019), provided the main considerations outlined in the ramp incremental exercise test section are met. A two-step cluster analysis was conducted to determine the optimal number of clusters based on three quantitative variables (VO2VT1, VO2VT2, and VO2max), using the Bayesian Information Criteria (BIC) to identify the clusters with the lowest BIC. In addition, the Silhouette index was used to assess clustering performance, categorized as poor (less than 0.2), fair (0.2–0.5), or good (> 0.5) (Wendler and Gröttrup 2016). The predictor importance of a variable for cluster formation ranged from 0 to 1, derived from a two-step algorithm. Consequently, participants were classified into low, medium, or high training status categories.
Statistical analysis
All the data are presented as the means ± standard deviation (SD). Outliers were identified as those values that were greater than or less than 3 times the interquartile range. Each outlier was evaluated to decide if it should be removed. The data were tested for normal distribution with the Kolmogorov–Smirnov test and for homogeneity of variances with Levene’s test. All the analysis were performed in males and females independently. Pearson correlation coefficients were calculated to assess the association between VO2VT1, VO2VT2 and VO2max with the %VO2max, %HRmax and %Vmax at which VT1 and VT2 occur. ANCOVA (age as a covariable) was used to study the effect of training status on the different variables determined at VT1 (VO2VT1, %VO2max VT1, HRVT1, %HRmax VT1, VVT1 and %Vmax VT1), at VT2 (VO2VT2, %VO2max VT2, HRVT2, %HRmax VT2, VVT2 and %Vmax VT2) and at maximum (VO2max, HRmax, Vmax). Bonferroni post‐hoc tests were conducted where significant main effects were found in any of the analyzed factors. The effect size of the ANCOVA was calculated by partial eta‐squared (η2) and the small, moderate, and large effects corresponded to values equal or greater than 0.001, 0.059, and 0.138, respectively (Cohen 1988). The criteria to interpret the strength of the r coefficients were as follows: trivial (< 0.1), small (0.1–0.3), moderate (0.3–0.5), high (0.5–0.7), very high (0.7–0.9), or practically perfect (> 0.9) (Hopkins et al. 2009). Statistical analyses were carried out with the statistical software Jamovi V1.6 (Jamovi, Sidney, Australia) and SPSS software 29 version (IBM Corp., Armonk, NY, USA). The significance level was set at p < 0.05.
Results
The physical characteristics of the participants and their incremental exercise results are shown in Tables 1, 2 and 3.
Correlations
In males, VO2max was not correlated with the %VO2max VT1 (r = −0.029; p = 0.364) and %VO2max VT2 (r = 0.058; p = 0.070) and poorly correlated with %HRmax VT1 (r = 0.236; p < 0.001), %HRmax VT2 (r = 0.224; p < 0.001), %Vmax VT1 (r = 0.108; p = 0.005) and %Vmax VT2 (r = 0.112; p = 0.003). Similar results were found in females, finding very low correlations between VO2max and %VO2max VT1 (r = 0.120; p = 0.039), %VO2max VT2 (r = 0.128; p = 0.028), %HRmax VT1 (r = 0.186; p = 0.001), %HRmax VT2 (r = 0.192; p < 0.001), %Vmax VT1 (r = −0.025; p = 0.707) and %Vmax VT2 (r = 0.176; p = 0.009). In contrast, a moderate correlation was found between VO2VT1 and %VO2max VT1, %HRmax VT1 and %Vmax VT1 and between VO2VT2 and %VO2max VT2, %HRmax VT2 and %Vmax VT2 in males and females (Fig. 1).

Correlation between VO2VT1 and %VO2max VT1, %HRmax VT1 and %Vmax VT1 and between VO2VT2 and %VO2max VT2, %HRmax VT2 and %Vmax VT2. VO2VT1 and VO2VT2: relative to body weight values of oxygen consumption at VT1 and VT2, respectively; %VO2max VT1 and %VO2max VT2: percentage of maximal oxygen consumption at VT1 and VT2, respectively; %HRmax VT1 and %HRmax VT2: percentage of maximal heart rate at VT1 and VT2, respectively; %Vmax VT1 and %Vmax VT2 percentage of maximal velocity at VT1 and VT2, respectively
Cluster analysis
According to the two-step cluster analysis, the optimal number of clusters was 3 for males and females, categorized as low, medium and high training status. The model’s Silhouette index was 0.5 in males and 0.6 in females, indicating a good quality of the clustering models. VO2VT2 had the most importance value (1) followed by VO2max (0.9) and VO2VT1 (0.8) in males and in females VO2VT2 was also the most important variable (1) followed by VO2max (0.94) and VO2VT1 (0.89).
Training status
%VO2max VT1 and %VO2max VT2 were different according to training status, observing higher values the higher the training status in both sexes. VO2VT1, VO2VT2 and VO2max were higher the higher the training status of the participant in both sexes (Table 1).
Significant differences were found in %HRmax VT1 and %HRmax VT2 according to training status in in both sexes. Specifically, in males, both variables increased as training status increased; while in females, %HRmax VT1 and %HRmax VT2 were higher in high and moderate training status compared to low. HRVT1 was higher the higher the training status of the participant in males, but in females, it was only higher in high training status compared to low. HRVT2 was higher in high and moderate training status in males, while in females, it was not significantly different across training status. In contrast, HRmax was not different across training status in any sex (Table 2).
%Vmax VT1 and %Vmax VT2 were significantly different across training status in both sexes. Concretely, in males, both variables were higher the higher the training status. In females, %Vmax VT1 was higher in high training status compared to moderate and low, while %Vmax VT2 was higher the higher the training status. VVT1, VVT2 and Vmax were higher the higher the training status of the participant in both sexes (Table 3).
Discussion
The key findings of this study revealed a very weak or no correlation between VO2max and the percentages of maximum at which thresholds occur (%VO2max VT1 and VT2, %HRmax VT1 and VT2, %Vmax VT1 and VT2). However, there was a correlation between VO2VT1 and %VO2max VT1, %HRmax VT1, and %Vmax VT1, as well as between VO2VT2 and %VO2max VT2, %HRmax VT2, and %Vmax VT2. These results indicate that the physiological determinants influencing the percentage of maximum at which VT1 and VT2 occur are more closely associated with VO2VT1 and VO2VT2, respectively, rather than with VO2max. Moreover, the percentages of VO2max, HRmax, and Vmax at which thresholds occur were higher in individuals with higher training status. This suggests that the conventional approach of establishing exercise intensity relative to maximum may not effectively standardize intensity across individuals with differing training statuses. These findings contribute to a better understanding of the factors influencing the wide variability of threshold positions and aid in determining exercise intensity based on training zones in individuals with diverse training statuses. Furthermore, the data from this study can serve as standard reference values for these variables in relation to training status, facilitating the interpretation of an individual’s fitness level. The novelty of this work lies in the classification of individuals, which is particularly relevant as detecting the effect of training status on threshold positions necessitates considering oxygen consumption the three main physiological points (VT1, VT2, and VO2max). Conversely, if only VO2max is considered, as is traditionally done, no effect of training status on threshold positions is observed. In addition, this novel classification of individuals helps establish reference values for the variables reported in this article according to training status.
In the present study, a very low correlation was found between VO2max and the percentage of maximum at which VT1 and VT2 occur. This could be attributed to the possibility that when specifically training to enhance VO2max, improvements in VO2max may outpace those in VO2VT1 or VO2VT2. In essence, VO2max could be diverging from VO2VT1 or VO2VT2, thereby reducing %VO2max VT1 and VT2. Conversely, a correlation was observed between VO2VT1 and VO2VT2 and the position of the respective thresholds relative to VO2max, HRmax, and Vmax. This finding is relevant because relying solely on VO2max fails to capture the impact of training status on other submaximal variables (e.g., %VO2max VT1 and VT2). This indicates that VO2max alone may not adequately distinguish certain critical submaximal variables, such as %VO2max VT1 and VT2. Moreover, the decision to consider VO2VT1, VO2VT2, and VO2max instead of exclusively utilizing VO2max appears highly pertinent. This is because the oxygen consumption at thresholds has been shown to hold considerable importance for both health and performance, sometimes even surpassing the significance of VO2max (Poole et al. 2021). Therefore, we opted to classify participants by combining VO2VT1, VO2VT2, and VO2max. We provide a practical tool incorporating reference standard values based on specific training statuses at the three physiological points, aiming to aid in participant classification according to training status at these key physiological points (see Figure S1).
In terms of %VO2max at the thresholds, we observed higher %VO2max VT1 and VT2 with increasing training status. This suggests that greater proportional improvements (greater responsiveness) occur in VO2VT1 or VO2VT2 compared to VO2max as training status improves. We hypothesize that this phenomenon can be attributed to the specificity of training principle, which posits that adaptations primarily occur at the specific intensity at which training is conducted. Given that endurance athletes typically adhere to a pyramidal training intensity distribution (with decreasing training volume from moderate to heavy to severe zones) (Zapico et al. 2007; Casado et al. 2022), it seems reasonable to assume that VO2VT1 or VO2VT2 experience greater enhancement compared to VO2max. An alternative explanation could be the differing impact of genetics on VO2max versus VO2VT1 or VO2VT2. There is evidence indicating a significant genetic influence on VO2max (Williams et al. 2017), although the impact on VO2VT1 or VO2VT2 remains unclear. Our findings align with a previous study that observed higher %VO2max VT1 and VT2 in well-trained compared to recreationally trained runners (Hetlelid et al. 2015). Furthermore, the present results are aligned with another study observing that %VO2max VT1 and VT2 differed between professional, U23 and junior cyclist (Alejo et al. 2022). In addition, our results are consistent with another study that noted VT1 and VT2 occurred at higher percentages of VO2max as the training season progressed (Zapico et al. 2007). Contrary, another study found a similar percentage of maximum at which LT occurred between runners of different competitive levels (Støa et al. 2020). In a study by Iannetta et al. (Iannetta et al. 2020), it was specified that the percentage of VO2max at which lactate threshold (%VO2max LT1) and maximal lactate steady state occur (%VO2max MLSS), reflections of VT1 and VT2 when measuring lactate, respectively, did not differ among individuals with different fitness levels. They based this assertion on the lack of correlation between VO2max and the position of the thresholds (%VO2max LT1 and %VO2max MLSS) found in their study (Iannetta et al. 2020). We also observed this lack of correlation between VO2max and %VO2max VT1 and VT2 in the present study. Iannetta et al. suggested that the lack of correlation may be due to the narrow range of VO2max in their study, but this does not seem to be the case because we also found this lack of correlation with a much broader range of VO2max in the present study. In addition, Iannetta et al. (Iannetta et al. 2020) perfectly noted that the lack of correlation could be because the physiological determinants of VO2max are not the same as the physiological determinants of the thresholds. We addressed this issue by evaluating the association between VO2VT1 and VO2VT2 with %VO2max VT1 and %VO2max VT2, respectively, finding a positive association. These results demonstrate that the physiological determinants of %VO2max VT1 and %VO2max VT2 are more closely related to VO2VT1 and VO2VT2, respectively, than to VO2max. Overall, individuals with a higher specific training status at VT1 and VT2 exhibit a rightward shift in the position of the respective thresholds. Hence, a higher %VO2max VT1 and %VO2max VT2 appear to be adaptations to training. Therefore, we propose them as possible indicators to assess an individual’s progress. However, we do not recommend solely evaluating an individual’s progress or making training decisions based on %VO2max VT1 or VT2, as threshold positions depend on VO2max. Thus, a higher %VO2max VT1 or VT2 could result from a lower VO2max with similar VO2VT1 or VO2VT2, respectively, and this does not necessarily indicate an improvement in training status. The changes in %VO2max VT1 or VT2 with training status observed in our data do not support the recommendations of general guidelines that establish exercise intensity based on percentages of VO2max (Haskell et al. 2007; Garber et al. 2011), since a specific percentage of VO2max could elicit different physiological responses as %VO2max VT1 or VT2 change with training. In other words, at the same percentage of VO2max, individuals with different training statuses (different %VO2max VT1 or VT2) could be in different training zones.
Regarding heart rate, we observed higher HRVT1 and HRVT2 with increasing training status, independently of age. This suggests that HR at the thresholds is sensitive to changes in training status, this interpretation should be taken with caution because this is a cross-sectional study and a longitudinal study would be necessary to confirm this. This finding is the most controversial, as previous studies have reported no significant changes in HR at the thresholds with training over a season (Lucía et al. 2000; Zapico et al. 2007, 2014). One possible explanation is that it may take more than one season to observe changes in HR at the thresholds. If this is true, a single incremental test per season would suffice to determine training zones based on HR data, while additional tests would be necessary to adjust training zones based on HR as training progresses over the years. However, the amount of time needed for training to affect HR at thresholds is currently unknown. Regarding HRmax, there were no significant differences across training statuses. This result aligns with a previous study that found similar HRmax in well-trained compared to recreationally trained runners (Hetlelid et al. 2015). Moreover, it is supported by previous studies that observed similar HRmax with training over a season (Lucía et al. 2000; Zapico et al. 2014).
Due to the higher HRVT1 and HRVT2 and the lack of difference on HRmax according to training status, %HRmax VT1 and VT2 was significantly higher as the training status increased. This points out that training only can affect HR at thresholds, but not at maximum. These results would indicate that percentage of HRmax at which VT1 and VT2 occur increase with training and could be used as an indicator of training status of the participants. This is supported by the significant correlation between VO2VT1 and VO2VT2 with %HRmax VT1 and VT2, respectively. In this case, since training status does not influence HRmax, it is possible to evaluate the evolution of a participant focusing exclusively on changes in %HRmax VT1 and VT2, in contrast to %VO2max VT1 or VT2. Nevertheless, these recommendations should be taken with cautions because the correlation between VO2VT1 and VO2VT2 with %HRmax VT1 and VT2, respectively, was moderate to low in general. As occurred with %VO2max, this finding does not support the general guidelines which stablish exercise intensity based on percentages of HRmax (Haskell et al. 2007; Garber et al. 2011). Since individuals with different training status (different %HRmax VT1 and VT2) could be at different training zones at the same percentage of HRmax.
VVT1, VVT2 and Vmax were significantly higher the higher the training status. These results are aligned with a previous study showing a higher VVT1 and VVT2 in well-trained compared to recreationally trained runners (Hetlelid et al. 2015). Furthermore, these results agree with previous studies observing an increment in power output at VT1, VT2, and maximum with training during a season (Lucía et al. 2000; Zapico et al. 2007, 2014). Thus, the velocity obtained at the different points seems to be one of the main adaptations to training and deserves special attention when evaluating the evolution of a subject. On the other hand, in case of using velocity to set intensity based on training zones it is necessary to determine velocity at thresholds frequently. This is due to the high impact of training on velocity at the different physiological points.
Finally, we observed higher %Vmax VT1 and VT2 as the training status of the participants increased. This indicates that greater proportional improvements (greater responsiveness) are observed in VVT1 or VVT2 compared to Vmax as training status increases. These results are consistent with those found for %VO2max VT1 and VT2; therefore, they could be explained by the same reasons. %Vmax VT1 and VT2 could serve as indicators of the training status of the participants due to the higher values observed with higher training statuses. This is supported by the significant correlation between VO2VT1 and VO2VT2 with %Vmax VT1 and VT2, respectively, although these recommendations should be interpreted cautiously because the correlation between VO2VT1 and VO2VT2 with %Vmax VT1 and VT2, respectively, was generally moderate to low. However, as with %VO2max VT1 and VT2, we do not recommend evaluating the progress of a participant based solely on %Vmax VT1 or VT2 because a higher value in these variables could be due to a lower Vmax with similar VVT1 or VVT2, respectively, and this does not necessarily indicate an improvement in training status. The changes in %Vmax VT1 or VT2 with training status observed in our data do not support the recommendations of general guidelines that establish exercise intensity based on percentages of maximum work rate, since a specific percentage of Vmax could elicit different physiological responses as %Vmax VT1 or VT2 change with training.
Methodological considerations
Like any study, the present one is not without considerations. One consideration is that participants underwent different incremental ramp exercise protocols depending on their fitness levels. However, various slopes of load increment during the test do not seem to affect VO2VT1, VO2VT2, or VO2max (Scheuermann and Kowalchuk 1998; Leo et al. 2017; Iannetta et al. 2019), while excessively long protocols (> ~ 26 min) may hinder reaching true VO2max due to fatigue (Midgley et al. 2008). Therefore, it is advisable to avoid an excessively low slope of load increment when assessing a subject’s evolution in VO2max. This is the primary reason why participants in the present study did not undergo the same incremental test. Similarly, different slopes of load increment do not appear to affect HRVT1, HRVT2, or HRmax (Scheuermann and Kowalchuk 1998). However, exercise protocols with steeper slopes of load increment yield higher workload values at different physiological points (Jamnick et al. 2018). Regarding reference standard values, other studies report data with larger sample sizes, but they classify individuals based on age and sex rather than training status (Loe et al. 2013; Vainshelboim et al. 2020). Although we acknowledge that our study does not provide data from such a large sample size, to the best of our knowledge, it is currently the only study available in the literature that reports reference values considering training status. Another consideration is that respiratory gas exchange was analyzed using two different analyzers. However, previous studies have already validated the analyzers used in the present study (Rietjens et al. 2001; Perez-Suarez et al. 2018). Finally, like any cross-sectional study, we cannot assert that training itself is the cause of the differences found between training statuses. However, it seems highly impractical to conduct a training program with the sample size of the present study.
Conclusion
VO2max shows a poor correlation with the percentage of VO2max, HRmax, and Vmax at which thresholds occur. In contrast, there is a positive correlation between VO2VT1 and VO2VT2 with the percentage of maximum at which VT1 and VT2 occur, respectively. These results indicate that the physiological determinants of the percentage of maximum at which VT1 and VT2 occur are more closely related to VO2VT1 and VO2VT2, respectively, than to VO2max. This means that VO2max cannot discern some of the differences between different training statuses, such as %VO2max VT1 and VT2. Furthermore, our findings suggest that the %VO2max, %HRmax, and %Vmax at which thresholds occur were higher with higher training statuses when individuals are classified according to training status combining VO2VT1, VO2VT2, and VO2max. Hence, a higher %VO2max, %HRmax, and %Vmax appear to be adaptations to training. These results indicate that, despite smaller differences between different training statuses in the variables normalized to the maximum compared to the absolute variables, the common strategy of establishing exercise intensity relative to maximum is not effective in matching intensity across individuals with different training statuses. We offer a practical tool using reference standard values based on specific training status of the three physiological points (VT1, VT2 and maximum) with the intention of helping to classify participant according to training status of the three main physiological points.
Data availability
The data that support the findings of this study are available from the corresponding author, JABM, upon reasonable request.
Abbreviations
- ANCOVA:
-
Analysis of covariance
- HR:
-
Heart rate
- HRVT1 :
-
Absolute heart rate at VT1
- HRVT2 :
-
Absolute heart rate at VT2
- HRmax :
-
Maximum heart rate
- LT1:
-
Lactate threshold 1
- LT2:
-
Lactate threshold 2
- MLSS:
-
Maximal lactate steady state
- V:
-
Velocity
- VCO2:
-
Carbon dioxide production
- VE:
-
Ventilation
- VO2 :
-
Oxygen consumption
- VO2VT1 :
-
Oxygen consumption relative to body weight at VT1
- VO2VT2 :
-
Oxygen consumption relative to body weight at VT2
- VO2max :
-
Maximum oxygen consumption relative to body weight
- VT1:
-
Ventilatory threshold 1
- VT2:
-
Ventilatory threshold 2
- VVT1 :
-
Velocity at VT1
- VVT2 :
-
Velocity at VT2
- Vmax :
-
Velocity at maximum
- SD:
-
Standard deviation
- ηp 2 :
-
Partial eta‐squared
- %HRmax :
-
Percentage of maximum heart rate
- %HRmax :
-
VT1 percentage of maximal heart rate at VT1
- %HRmax :
-
VT2 percentage of maximal heart rate at VT2
- %VO2max :
-
Percentage of maximum oxygen consumption
- %VO2max :
-
VT1 percentage of maximal oxygen consumption at VT1
- %VO2max :
-
VT2 percentage of maximal oxygen consumption at VT2
- %Vmax :
-
Percentage of maximum velocity
- %Vmax :
-
VT1 percentage of maximal velocity at VT1
- %Vmax :
-
VT2 percentage of maximal velocity at VT2
- %Wmax :
-
Percentage of maximum power output
References
Alejo LB, Montalvo-Pérez A, Valenzuela PL et al (2022) Comparative analysis of endurance, strength and body composition indicators in professional, under-23 and junior cyclists. Front Physiol. https://doi.org/10.3389/fphys.2022.945552
Bentley DJ, Newell J, Bishop D (2007) Incremental exercise test design and analysis: Implications for performance diagnostics in endurance athletes. Sport Med 37:575–586. https://doi.org/10.2165/00007256-200737070-00002
Casado A, González-Mohíno F, González-Ravé JM, Foster C (2022) Training periodization, methods, intensity distribution, and volume in highly trained and elite distance runners: a systematic review. Int J Sports Physiol Perform 17:820–833. https://doi.org/10.1123/ijspp.2021-0435
Coates AM, Joyner MJ, Little JP et al (2023) A perspective on high-intensity interval training for performance and health. Sport Med. https://doi.org/10.1007/s40279-023-01938-6
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates Inc., Hillsdale
Garber CE, Blissmer B, Deschenes MR et al (2011) Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med Sci Sports Exerc 43:1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb
Haskell WL, Lee IM, Pate RR et al (2007) Physical activity and public health: updated recommendation for adults from the american college of sports medicine and the american heart association. Circulation 116:1081–1093
Hetlelid KJ, Plews DJ, Herold E et al (2015) Rethinking the role of fat oxidation: Substrate utilisation during high-intensity interval training in well-trained and recreationally trained runners. BMJ Open Sport Exerc Med 1:1–9. https://doi.org/10.1136/bmjsem-2015-000047
Hopkins WG, Marshall SW, Batterham AM, Hanin J (2009) Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc 41:3–12
Iannetta D, De Almeida AR, Keir DA, Murias JM (2019) Establishing the VO2 versus constant-work-rate relationship from rampincremental exercise: Simple strategies for an unsolved problem. J Appl Physiol 127:1519–1527. https://doi.org/10.1152/japplphysiol.00508.2019
Iannetta D, Inglis EC, Mattu AT et al (2020) A critical evaluation of current methods for exercise prescription in women and men. Med Sci Sports Exerc 52:466–473. https://doi.org/10.1249/MSS.0000000000002147
Jamnick NA, Botella J, Pyne DB, Bishop DJ (2018) Manipulating graded exercise test variables affects the validity of the lactate threshold and VO2peak. PLoS ONE. https://doi.org/10.1371/journal.pone.0199794
Keir DA, Fontana FY, Robertson TC et al (2015) Exercise intensity thresholds: identifying the boundaries of sustainable performance. Med Sci Sports Exerc 47:1932–1940. https://doi.org/10.1249/MSS.0000000000000613
Keir DA, Iannetta D, Mattioni Maturana F et al (2022) Identification of non-invasive exercise thresholds: methods, strategies, and an online app. Sport Med 52:237–255. https://doi.org/10.1007/s40279-021-01581-z
Leo JA, Sabapathy S, Simmonds MJ, Cross TJ (2017) The Respiratory compensation point is not a valid surrogate for critical power. Med Sci Sports Exerc 49:1452–1460. https://doi.org/10.1249/MSS.0000000000001226
Loe H, Rognmo Ø, Saltin B, Wisløff U (2013) Aerobic capacity reference data in 3816 healthy men and women 20–90 years. PLoS ONE 8:e64319. https://doi.org/10.1371/journal.pone.0064319
Lucía A, Hoyos J, Perez M, Chicharro JL (2000) Heart rate and performance parameters in elite cyclists: a longitudinal study. Med Sci Sport Exerc 32:1777–1782
Mann T, Lamberts RP, Lambert MI (2013) Methods of prescribing relative exercise intensity: Physiological and practical considerations. Sport Med 43:613–625. https://doi.org/10.1007/s40279-013-0045-x
Meyer T, Lucía A, Earnest CP, Kindermann W (2005) A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters ± theory and application. Int J Sport Med 26:S38-48. https://doi.org/10.1055/s-2004-830514
Meyler S, Bottoms L, Wellsted D, Muniz-Pumares D (2023) Variability in exercise tolerance and physiological responses to exercise prescribed relative to physiological thresholds and to maximum oxygen uptake. Exp Physiol 108:581–594. https://doi.org/10.1113/EP090878
Midgley AW, Bentley DJ, Luttikholt H et al (2008) Challenging a dogma of exercise physiology: does an incremental exercise test for valid VO2max determination really need to last between 8 and 12 minutes? Sport Med 38:441–447
Perez-Suarez I, Martin-Rincon M, Gonzalez-Henriquez JJ et al (2018) Accuracy and precision of the COSMED K5 portable analyser. Front Physiol. https://doi.org/10.3389/fphys.2018.01764
Poole DC, Wilkerson DP, Jones AM (2008) Validity of criteria for establishing maximal O2 uptake during ramp exercise tests. Eur J Appl Physiol 102:403–410. https://doi.org/10.1007/s00421-007-0596-3
Poole DC, Rossiter HB, Brooks GA, Gladden LB (2021) The anaerobic threshold: 50+ years of controversy. J Physiol 599:737–767. https://doi.org/10.1113/JP279963
Rabadán M, Díaz V, Calderón FJ et al (2011) Physiological determinants of speciality of elite middle- and long-distance runners. J Sports Sci 29:975–982. https://doi.org/10.1080/02640414.2011.571271
Rietjens GJ, Kuipers H, Kester AD, Keizer HA (2001) Validation of a computerized metabolic measurement system (Oxycon-Pro) during low and high intensity exercise. Int J Sports Med 22:291–294. https://doi.org/10.1055/s-2001-14342
Scheuermann BW, Kowalchuk JM (1998) Attenuated respiratory compensation during rapidly incremented ramp exercise. Respir Physiol 114:227–238. https://doi.org/10.1016/S0034-5687(98)00097-8
Støa EM, Helgerud J, Rønnestad BR et al (2020) Factors influencing running velocity at lactate threshold in male and female runners at different levels of performance. Front Physiol. https://doi.org/10.3389/fphys.2020.585267
Vainshelboim B, Arena R, Kaminsky LA, Myers J (2020) Reference standards for ventilatory threshold measured with cardiopulmonary exercise testing: the fitness registry and the importance of exercise: a national database. Chest 157:1531–1537. https://doi.org/10.1016/j.chest.2019.11.022
Weatherwax RM, Harris NK, Kilding AE, Dalleck LC (2019) Incidence of VO2max responders to personalized versus standardized exercise prescription. Med Sci Sports Exerc 51:681–691. https://doi.org/10.1249/MSS.0000000000001842
Wendler T, Gröttrup S (2016) Data mining with SPSS modeler: theory, exercises and solutions. Springer
Williams CJ, Williams MG, Eynon N et al (2017) Genes to predict VO2max trainability: a systematic review. BMC Genomics 18:831. https://doi.org/10.1186/s12864-017-4192-6
Zapico AG, Calderón FJ, Benito PJ et al (2007) Evolution of physiological and haematological parameters with training load in elite male road cyclists: a longitudinal study. J Sports Med Phys Fitn 47:191–196
Zapico AG, Benito PJ, Diaz V et al (2014) Heart rate profile in highly trained. Rev Int Med y Ciencias La Act Fis y El Deport 14:619–632
Acknowledgements
The authors of the present article would like to thank all the people who helped with the data collection during the whole history of the laboratory of exercise physiology of the LFE Research Group.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. JABM and IGC were supported by a grant provided by Universidad Politécnica de Madrid. RC was supported by a grant for the Requalification of the Spanish University System 2021–2023 from the Spanish Ministry of Universities (RD 289/2021), funded by the European Union-NextGenerationEU.
Author information
Authors and Affiliations
Contributions
JABM: conceptualization, methodology, formal analysis, investigation, writing—original draft, visualization. PJB: conceptualization, methodology, formal analysis, investigation, writing—review and editing, visualization. IGC: methodology, formal analysis, investigation, writing—review and editing, visualization. RC: methodology, formal analysis, investigation, writing—review and editing, visualization. ABP: methodology, formal analysis, investigation, writing—review and editing, visualization, project administration. All the authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interests.
Ethical approval
The protocols and procedures were approved by the Ethical Principles for Medical Research Involving Human Subjects of the World Medical Association Declaration of Helsinki (1964) and further amendments. This study was approved by the Human Research Ethics Committee of the Universidad Politécnica de Madrid. The data and information obtained in the project were considered as confidential following current Spanish legislation regulating personal data protection (Organic Law 3/2018). Therefore, database was restricted to the researchers that participated in the study.
Informed consent
All the participants were carefully informed about the possible risk and benefits of the project and they provided written informed consent to participate in the study.
Additional information
Communicated by Michael I Lindinger.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Benítez-Muñoz, J.A., Benito, P.J., Guisado-Cuadrado, I. et al. Differences in the ventilatory thresholds in treadmill according to training status in 971 males and 301 females: a cross-sectional study. Eur J Appl Physiol (2024). https://doi.org/10.1007/s00421-024-05622-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00421-024-05622-z