
Abstract
Purpose
This study aimed to examine changes in salivary immunoglobulin A (s-IgA) secretion at different intensities or durations of acute exercise.
Methods
Twelve healthy untrained young males were included in randomized crossover trials in Experiment 1 (cycling exercise for 30 min at a work rate equivalent to 35%, 55%, and 75% maximal oxygen uptake [\({\dot{\text{V}}}\)O2max]) and Experiment 2 (cycling exercise at 55% \({\dot{\text{V}}}\)O2max intensity for 30, 60, and 90 min). Saliva samples were collected at baseline, immediately after, and 60 min after each exercise.
Results
Experiment 1: The percentage change in the s-IgA secretion rate in the 75% \({\dot{\text{V}}}\)O2max trial was significantly lower than that in the 55% \({\dot{\text{V}}}\)O2max trial immediately after exercise (− 45.7%). The percentage change in the salivary concentration of cortisol, an s-IgA regulating factor, immediately after exercise significantly increased compared to that at baseline in the 75% \({\dot{\text{V}}}\)O2max trial (+ 107.6%). A significant negative correlation was observed between the percentage changes in saliva flow rate and salivary cortisol concentration (r = − 0.52, P < 0.01). Experiment 2: The percentage change in the s-IgA secretion rate in the 90-min trial was significantly lower than that in the 30-min trial immediately after exercise (−37.0%). However, the percentage change in salivary cortisol concentration remained the same.
Conclusion
Our findings suggest that a reduction in s-IgA secretion is induced by exercise intensity of greater than or equal to 75% \({\dot{\text{V}}}\)O2max for 30 min or exercise duration of greater than or equal to 90 min at 55% \({\dot{\text{V}}}\)O2max in healthy untrained young men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Exercise induces significant changes in various biological responses, including circulation, metabolism, nerve activity, and the immune response. Immune function plays an important role in protecting against infections such as bacteria; however, during and/or after exercise, which induces an increase in ventilation, the state of oral immune function is changed. Salivary immunoglobulin A (s-IgA), secreted by oral epithelial cells, is the predominant antibody in mucosal fluid and plays an important role in neutralizing virus and bacteria during oral and suppressing upper respiratory tract infections (Lamm et al.1995; Marcotte and Lavoie 1998; Woof and Mestecky 2005). However, long-term and/or high-intensity exercise, such as ultra-marathons, increases the incidence of upper respiratory tract infections by reducing the intraoral s-IgA secretion rate, which is calculated as the product of s-IgA concentration and saliva flow rate (Nieman et al. 2003). The transient depression of s-IgA secretion after a bout of exercise is called the “open window theory”, and this repeated depression may lead to chronic decline in oral immune function (Pedersen and Bruunsgaard 1995). Therefore, it is important to clarify transient changes in s-IgA secretion after exercise to prevent upper respiratory tract infection.
In previous studies on changes in s-IgA secretion after a bout of exercise, the s-IgA secretion rate decreased after high-intensity exercise with 75% maximal oxygen uptake (\({\dot{\text{V}}}\)O2max) (Matsubara et al. 2010; Murase et al. 2016). In contrast, other studies have shown that the s-IgA secretion rate does not decrease even after exercise of the same intensity (Allgrove et al. 2008; Usui et al. 2011). Additionally, moderate-intensity exercise for 120 min reduced the s-IgA secretion rate (Laing et al. 2005); however, the s-IgA secretion rate was not changed by moderate-intensity exercise for 40 min (Mackinnon and Hooper 1994) and 22.3 min (Allgrove et al. 2008). Although it is believed that a reduction in s-IgA secretion may be induced by long-term and/or high-intensity exercise, no consensus has been reached on the effects of exercise intensity and/or duration on s-IgA secretion. As causal factors of these discrepancies in the s-IgA secretion response to exercise, the circadian rhythm of saliva flow rate and s-IgA concentration (Hucklebridge et al. 1998; Dimitriou et al. 2002); water intake during and before/after exercise (Bishop et al. 2000); nutritional status of subjects (Gleeson et al. 2001); and saliva collection methods (Bishop and Gleeson 2009) affect the s-IgA secretion rate. In addition, Bishop and Gleeson (2009) pointed out the importance of evaluating the s-IgA secretion rate among the same subjects (Bishop and Gleeson 2009). However, no study has examined the effect of exercise modality on the s-IgA secretion rate among the same subjects; thus, the exercise intensity and/or duration, which reduces s-IgA secretion, remains unclear. Elucidating the effects of exercise intensity and duration on immune function is important for individuals who exercise to improve their health and physical fitness.
Herein, we hypothesized that a single bout of acute exercise of higher intensity or longer duration would induce a decrease in s-IgA secretion. Therefore, we aimed to clarify the changes in s-IgA secretion in response to acute exercise at different intensities or durations in the same subjects. This study examined the effects of different exercise intensities (Experiment 1) or durations (Experiment 2) by acute exercise on s-IgA secretory responses. Furthermore, the induction of circulating cortisol secretion via sympathetic nervous system activation affects the saliva flow rate during acute exercise (Chicharro et al. 1998). Therefore, in this study, we examined the effects of salivary cortisol concentration, as an index of systemic secretion, on different exercise intensities and/or durations and whether salivary cortisol is associated with the s-IgA secretion response to acute exercise. This study clarified, for the first time, the changes in s-IgA secretion after acute exercise at different exercise intensities or durations.
Methods
Subjects
Twelve healthy untrained young males with no exercise habits (mean ± SD: age 21.7 ± 1.6 years; height 174.6 ± 3.6 cm; body weight 65.6 ± 5.2 kg; \({\dot{\text{V}}}\)O2max 41.4 ± 4.3 ml/kg/min; maximal heart rate (HRmax) 197.6 ± 5.3 beats/min) participated in this study. In this study, individuals were excluded if, in the last year, they had physiological disorders or chronic diseases, were currently taking any medications, smoked or consumed alcohol daily, or exercised more than 3 h/week. All participants were given verbal and written briefings on the study and provided written informed consent. This study was approved by the Ethics Committee of Ritsumeikan University (BKC-LSMH-2021–054) and conducted in accordance with the Declaration of Helsinki.
Experimental procedures
\({\dot{\text{V}}}\)O2max was measured approximately 1 week before the main trials. The cycling exercise load for each exercise trial was calculated from the relationship between \({\dot{\text{V}}}\)O2max and work rate, equivalent to 35% \({\dot{\text{V}}}\)O2max, 55% \({\dot{\text{V}}}\)O2max, and 75% \({\dot{\text{V}}}\)O2max. Subjects were instructed not to perform excessive exercise and not to consume both caffeine and alcohol for 24 h before each exercise trial. The subjects performed each exercise trial after fasting and drinking water from 10:00 PM. Hydration status was standardized to 500 ml before each exercise trial (Li and Gleeson 2005). The subjects were instructed to drink 250 ml water before bedtime and after waking up. To eliminate the effect of the circadian rhythm on the saliva flow rate and s-IgA concentration (Hucklebridge et al. 1998; Dimitriou et al. 2002), each measurement was conducted from 9:00 AM to 12:00 PM. The participants arrived at the laboratory at 9:00 AM and remained in a sitting position for 30 min before each exercise trial (Fig. 1). Body weight was measured using a digital platform scale (Innerscan DUAL; TANITA, Tokyo, Japan), and hydration status was checked at rest before exercise; it was confirmed that there was no change between each exercise trial within the subjects (Walsh et al. 2004). This was a randomized crossover study. After each exercise trial, the subjects were allowed to rest in a sitting position for 60 min. The heart rate (HR) (WEP-5204; Nihon Kohden, Tokyo, Japan) was measured 1 min before the end of exercise. Saliva samples were collected before (baseline), immediately after (post), and 60 min after the end of exercise (post-60) according to a previous study (Allgrove et al. 2008). The participants were instructed to fast and not drink anything until 60 min after the end of the exercise. The laboratory temperature and relative humidity were 23.1 ± 1.5 °C and 71.2 ± 12.1%, respectively.

Experimental protocol in this study. Experiment 1: Trial 1 (cycling exercise for 30 min at 35% \({\dot{\text{V}}}\)O2max), Trial 2 (cycling exercise for 30 min at 55% \({\dot{\text{V}}}\)O2max), Trial 3 (cycling exercise for 30 min at 75% \({\dot{\text{V}}}\)O2max). Experiment 2: Trial 2 (cycling exercise for 30 min at 55% \({\dot{\text{V}}}\)O2max), Trial 4 (cycling exercise for 60 min at 55% \({\dot{\text{V}}}\)O2max), Trial 5 (cycling exercise for 90 min at 55% \({\dot{\text{V}}}\)O2max). \({\dot{\text{V}}}\)O2max: maximal oxygen uptake
Exercise trials
All subjects randomly performed five exercise trials (Trial 1: cycling exercise for 30 min at 35% \({\dot{\text{V}}}\)O2max, Trial 2: cycling exercise for 30 min at 55% \({\dot{\text{V}}}\)O2max, Trial 3: cycling exercise for 30 min at 75% \({\dot{\text{V}}}\)O2max, Trial 4: moderate-intensity continuous cycling exercise at 55% \({\dot{\text{V}}}\)O2max for 60 min, Trial 5: moderate-intensity continuous cycling exercise at 55% \({\dot{\text{V}}}\)O2max for 90 min) with a washout period of at least 3 days between each trial as a reference to a previous study (Allgrove et al. 2008). To determine the effect of exercise intensity on salivary parameters (Experiment 1), continuous cycling exercise at three different exercise intensities (35% [low], 55% [moderate], and 75% \({\dot{\text{V}}}\)O2max [high]) was performed for 30 min. Additionally, to determine the effect of exercise duration on salivary parameters (Experiment 2), continuous cycling exercise at 55% \({\dot{\text{V}}}\)O2max as a moderate-intensity exercise at three different exercise durations (30 min [short], 60 min [medium], and 90 min [long]) was performed. In this study, considering the burden on the participant, 55% \({\dot{\text{V}}}\)O2max for 30 min was performed only once and the duplicate was not implemented in either experiment. Furthermore, it was divided into 30-min intervals, and exercise trials were set for 30 min (short duration), 60 min (medium duration), and 90 min (long duration).
Measurement of \({\dot{\text{V}}}\)O2max
\({\dot{\text{V}}}\)O2max was determined during an incremental cycling exercise test using a cycle ergometer (828E; Monark, Stockholm, Sweden) by monitoring breath-by-breath oxygen consumption and carbon dioxide production (AE-310SRD; Minato, Osaka, Japan). The subjects were instructed to maintain a minimum pedaling rate of 60 rpm according to the protocol of a previous study (Hasegawa et al. 2016). Following a 5-min warm-up at 60 W, they began cycling at 60 W ± 30 W in increments of 15 W each minute until exhaustion (Hasegawa et al. 2016). During the incremental cycling exercise test, the heart rate (HR) (WEP-5204; Nihon Kohden, Tokyo, Japan) and rating of perceived exertion (RPE) were continuously measured every minute during the cycling exercise. The test was considered valid if at least three of the four following criteria were met: [1] plateau in \({\dot{\text{V}}}\)O2 with an increase in maximal effort, [2] HRmax of the age-predicted maximum (220-age ± 5 beats/min), [3] maximal respiratory exchange ratio of ≧1.1, and [4] an RPE of ≧18 (Borg 1982; American College of Sports Medicine 2000).
Saliva collection and analysis
Saliva samples were collected between 9:00 AM and 1:00 PM. According to a previous study (Usui et al. 2011), the subjects rinsed their mouths with distilled water (30 s × 3 times). Saliva production was stimulated by chewing a piece of paraffin wax (B.S.A paraffin wax; B.S.A, Aichi, Japan) for 1 min at a frequency of 1 chew/sec (Libicz et al. 2006; Balsalobre-Fernández et al. 2014; Gomar-Vercher et al. 2018). The collected saliva was separated from the paraffin wax by centrifugation at 4 °C, 1500 g, for 5 min. The saliva flow rate (ml/min) was measured by weighing and the saliva density was estimated to be 1.0 g/ml (Usui et al. 2011). Saliva supernatants were stored at − 20 °C until analysis.
Salivary IgA and cortisol concentrations were measured using an enzyme-linked immunosorbent assay (Salimetrics, State College, PA, USA) according to previous studies (Mc Naughton et al. 2006; Peñailillo et al. 2015). The absorbance was measured at 450 nm using a microplate reader and an xMark microplate spectrophotometer (Bio-Rad Laboratories, Hercules, CA, USA). The salivary IgA secretion rate (μg/min) was calculated from the saliva flow rate per minute (ml/min) and salivary IgA concentration (μg/ml), according to a previous study (Koch et al. 2007). In this study, salivary cortisol concentrations were measured based on the assumption that the concentration of cortisol in the saliva reflects the concentration secreted into the blood (Chicharro et al. 1998; Hackney and Walz 2013). The average coefficients of variation for IgA and cortisol assays were 3.3% and 2.6%, respectively.
Statistical analysis
All statistical analyses were performed using the StatView software (5.0; SAS Institute, Tokyo, Japan). All values are expressed as mean ± SD. In the Experiment 1, the saliva flow rate, s-IgA concentration, salivary cortisol concentration, and s-IgA secretion rate at different exercise intensities (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max) were compared using three trials × three time points (baseline, post, and post-60) of a two-way repeated-measures ANOVA. Fisher’s post-hoc test was used to correct for multiple comparisons when the ANOVA revealed significant differences. The relationship between the change in saliva flow rate and the change in salivary cortisol concentration was determined using Pearson’s correlation coefficient. In the Experiment 2, the comparison of saliva flow rate, s-IgA concentration, salivary cortisol concentration, and s-IgA secretion rate at different exercise durations (30, 60, and 90 min) was performed using three trials × three time points (baseline, post, and post-60) in a two-way repeated-measures ANOVA. Fisher’s post-hoc test was used to correct for multiple comparisons when the ANOVA revealed significant differences. Statistical significance was defined as P < 0.05. We calculated the effect size of 0.25 (large) for the two-way repeated-measures ANOVA using G*Power (version 3.1), which determined the sample size needed for this study. To detect the effect size at alpha levels of 0.05 and 80% power, the sample size was set to 12 participants.
Results
The HRs recorded 1 min before the end of each exercise trial were as follows:
Experiment 1: 35% \({\dot{\text{V}}}\)O2max; 55% \({\dot{\text{V}}}\)O2max; 75% \({\dot{\text{V}}}\)O2max (112.6 ± 13.9; 150.8 ± 10.6; 186.4 ± 7.7 beats/min, respectively, data not shown).
Experiment 2: 30 min; 60 min; 90 min (150.8 ± 10.6; 158.7 ± 13.4; 165.6 ± 12.6 beats/min, respectively, data not shown).
Experiment 1: exercise intensity study.
No significant differences in saliva flow rate, s-IgA concentration, or s-IgA secretion rate were observed among the three exercise intensity trials (Table 1). However, there was a significant interaction of salivary cortisol concentrations between the three trials (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max) and three time points (baseline, post, and post-60) (F = 4.470, interaction: P < 0.01, Table 1). The salivary cortisol concentration in the 75% \({\dot{\text{V}}}\)O2max trial at post and post-60 were significantly higher than that at baseline (P < 0.05 respectively; Table 1). The salivary cortisol concentration in the 75% \({\dot{\text{V}}}\)O2max trial was significantly higher than that in the 35% \({\dot{\text{V}}}\)O2max trial at post and post-60 (P < 0.01, respectively; Table 1). The 75% \({\dot{\text{V}}}\)O2max trial was significantly higher than the 55% \({\dot{\text{V}}}\)O2max trial at post and post-60 (P < 0.01, respectively; Table 1).
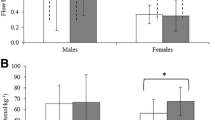
There was a significant interaction in the percentage change in the saliva flow rate between the three trials (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max) and the three time points (baseline, post, and post-60) (F = 2.815, interaction: P < 0.05, Fig. 2A). The percentage change in saliva flow rate in the 35% \({\dot{\text{V}}}\)O2max and 75% \({\dot{\text{V}}}\)O2max trials at post was significantly lower than that at baseline (35% \({\dot{\text{V}}}\)O2max trial, P < 0.05; 75% \({\dot{\text{V}}}\)O2max trial, P < 0.01; Fig. 2A). In addition, the percentage change in saliva flow rate in the 75% \({\dot{\text{V}}}\)O2max trial was significantly lower than that in the 35% \({\dot{\text{V}}}\)O2max and 55% \({\dot{\text{V}}}\)O2max trials at post (P < 0.01, Fig. 2A). In contrast, the percentage change in saliva flow rate in the 35% \({\dot{\text{V}}}\)O2max and 75% \({\dot{\text{V}}}\)O2max trials post-60 was significantly higher than that at post (35% \({\dot{\text{V}}}\)O2max trial, P < 0.01; 75% \({\dot{\text{V}}}\)O2max trial, P < 0.01; Fig. 2A). The percentage changes in s-IgA concentrations were not significantly different between the three exercise intensity trials (Fig. 2B). There was a significant interaction between the percentage change in the s-IgA secretion rate between the three trials (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max) and the three time points (baseline, post, and post-60) (F = 3.365, P < 0.05, Fig. 2C). The percentage change in the s-IgA secretion rate in the 75% \({\dot{\text{V}}}\)O2max trial was significantly lower than that in the 55% \({\dot{\text{V}}}\)O2max trial (P < 0.01, Fig. 2C). The 75% \({\dot{\text{V}}}\)O2max trial post-60 was significantly higher than that at post (P < 0.05, Fig. 2C).

Effects of different exercise intensities on the percentage change in saliva flow rate (A), salivary IgA concentration (B), and salivary IgA secretion rate (C) from baseline in healthy untrained young males (n = 12). Data are expressed as mean ± SD. IgA: Immunoglobulin A; \({\dot{\text{V}}}\)O2max: maximal oxygen uptake. *P < 0.01 vs post at 35% \({\dot{\text{V}}}\)O2max. †P < 0.01 vs post at 55% \({\dot{\text{V}}}\)O2max. ‡P < 0.05 vs baseline at 35% \({\dot{\text{V}}}\)O2max. §P < 0.01 vs baseline at 75% \({\dot{\text{V}}}\)O2max. ¶P < 0.01 vs post in each trial. #P < 0.05 vs post in each trial
There was a significant interaction of the percentage change in salivary cortisol concentration between the three trials (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max) and the three time points (baseline, post, and post-60) (F = 4.469, interaction: P < 0.05, Fig. 3). The percentage changes in salivary cortisol concentration at post and post-60 were significantly higher than that at baseline in the 75% \({\dot{\text{V}}}\)O2max trial (P < 0.05, respectively; Fig. 3). The percentage change in salivary cortisol concentration in the 75% \({\dot{\text{V}}}\)O2max trial was significantly higher than that in the 35% \({\dot{\text{V}}}\)O2max trial at post and post-60 (P < 0.01, respectively; Fig. 3). The percentage change in salivary cortisol concentration in the 75% \({\dot{\text{V}}}\)O2max trial was significantly higher than that in the 55% \({\dot{\text{V}}}\)O2max trial at post and post-60 (P < 0.01, respectively; Fig. 3).

Effects of different exercise intensities on the percentage change in salivary cortisol concentration from baseline in healthy untrained young males (n = 12). Data are expressed as mean ± SD. \({\dot{\text{V}}}\)O2max: maximal oxygen uptake. *P < 0.01 vs post at 35% \({\dot{\text{V}}}\)O2max. **P < 0.01 vs post-60 at 35% \({\dot{\text{V}}}\)O2max. †P < 0.01 vs post at 55% \({\dot{\text{V}}}\)O2max. ††P < 0.01 vs post-60 at 55% \({\dot{\text{V}}}\)O2max. ‡P < 0.05 vs baseline at 75% \({\dot{\text{V}}}\)O2max. §P < 0.01 vs baseline at 35% \({\dot{\text{V}}}\)O2max. ¶P < 0.01 vs post at 35% \({\dot{\text{V}}}\)O2max
A significant negative correlation of percentage changes between saliva flow rate and salivary cortisol concentration was observed from baseline to post in each exercise trial (r = -0.52, P < 0.01, Fig. 4).

Correlation between percentage changes in salivary cortisol concentration and percentage changes in saliva flow rate among different exercise intensities in healthy untrained young males (n = 12)
Experiment 2: exercise duration study.
No significant differences were observed in saliva flow rate, s-IgA concentration, s-IgA secretion rate, or salivary cortisol concentration in each exercise trial (Table 2). There was no significant interaction between the percentage change in saliva flow rate and s-IgA concentration (Fig. 5A, B). However, the percentage change in the s-IgA secretion rate showed a significant interaction between the three trials (30, 60, and 90 min) and the three time points (baseline, post, and post-60) (F = 2.471, P < 0.05, Fig. 5C). The percentage change in the s-IgA secretion rate in the 90-min trial was significantly lower than that in the 30-min trial at post (P < 0.05, Fig. 5C). The percentage change in the s-IgA secretion rate in the 90-min trial at post-60 was significantly higher than that at post (P < 0.05, Fig. 5C).

Effects of different exercise durations on the percentage change in saliva flow rate (A), salivary IgA concentration (B), and salivary IgA secretion rate (C) from baseline in healthy untrained young males (n = 12). Data are expressed as mean ± SD. IgA: Immunoglobulin A. *P < 0.05 vs post at 30 min. †P < 0.05 vs post in each trial
There was no significant interaction effect in the percentage change in salivary cortisol concentrations (Fig. 6).

Effects of different exercise durations on the percentage change in salivary cortisol concentration from baseline in healthy untrained young males (n = 12). Data are expressed as mean ± SD
Discussion
The main findings of the experiment 1 revealed that the s-IgA secretion rate was transiently reduced after cycling exercise at 75% \({\dot{\text{V}}}\)O2max in healthy untrained young men, as examined using 30-min acute exercise at different intensities (35%, 55%, and 75% \({\dot{\text{V}}}\)O2max). Furthermore, the experiment 2 showed a reduction in the s-IgA secretion rate after cycling exercise for 90 min, as examined using an acute 55% \({\dot{\text{V}}}\)O2max bout of exercise at different exercise durations (30, 60, and 90 min). Since s-IgA neutralizes the invasion of viruses and bacteria into the oral cavity, it is important to maintain oral s-IgA secretions (Lamm et al.1995; Marcotte and Lavoie 1998; Woof and Mestecky 2005). These results suggest that depression in s-IgA secretion is transiently induced by exercise intensity of greater than or equal to 75% \({\dot{\text{V}}}\)O2max for 30 min or exercise duration of greater than or equal to 90 min at 55% \({\dot{\text{V}}}\)O2max exercise intensity in healthy untrained young men.
Previous studies examining the response of s-IgA secretion to transient cycling exercise have shown no consistent evidence that the rate of s-IgA secretion is reduced or unchanged by various exercise intensities (Allgrove et al. 2008; Matsubara et al. 2010; Usui et al. 2011; Murase et al. 2016) or durations (Mackinnon and Hooper 1994; Laing et al. 2005; Allgrove et al. 2008). MacDowell et al. (1991) examined the effects of different exercise intensities (50, 65, and 80% \({\dot{\text{V}}}\)O2max) with the same exercise duration (20 min) or different durations (15, 30, and 45 min) with the same exercise intensity (60% \({\dot{\text{V}}}\)O2max) on s-IgA concentration but did not examine the same subjects to compare exercise intensity and duration. Moreover, they only assayed IgA concentration (McDowell et al. 1991). However, measurement of the IgA secretion rate by multiplying the s-IgA concentration and saliva flow rate may be more accurate because the s-IgA concentration is decreased/increased by the saliva flow rate (Bishop and Gleeson 2009). To clarify these issues, the present study compared different exercise intensities and durations in the same subjects. Consequently, the experiment 1 showed no change in the s-IgA secretion rate after cycling exercise at 35% and 55% \({\dot{\text{V}}}\)O2max exercise intensities for 30 min, whereas the change in the 75% \({\dot{\text{V}}}\)O2max trial was significantly lower than that in the 55% \({\dot{\text{V}}}\)O2max trial immediately after exercise (-45.7%). Additionally, the s-IgA secretion rate after cycling exercise at 55% \({\dot{\text{V}}}\)O2max exercise intensity for 30 and 60 min was not statistically significant; however, a − 37.0% decrease in the s-IgA secretion rate after cycling exercise for 90 min was observed compared to the 30-min trial in the experiment 2. Furthermore, in this study, the secretion rate during exercise for 30–90 min was dependent on time, and this at 35–75% \({\dot{\text{V}}}\)O2max exercise intensities was dependent on exercise intensity. Mackinnon et al. (1993) showed that the s-IgA secretion rate decreased by 27% after a 30-min interval exercise (Mackinnon et al. 1993). In addition, Laing et al. (2005) and Nieman et al. (2003) showed that long-term exercise (120 min and 13 h) decreased s-IgA secretion rates by 34% and 50%, respectively (Nieman et al. 2003; Laing et al. 2005). Therefore, in the case of much higher intensities or longer-term exercise than those in the present study, the s-IgA secretion rate may decrease even more.
In the experiment 1, the saliva flow rate and s-IgA secretion rate transiently decreased after cycling exercise at 75% \({\dot{\text{V}}}\)O2max for 30 min. Saliva secretion is regulated by the autonomic nervous system (Chicharro et al. 1998). Therefore, after cycling exercise using an exercise intensity that exceeds the anaerobic threshold, such as 90% HRmax and increased exercise intensity, the saliva flow rate decreases through increased sympathetic nervous activity (Chicharro et al. 1998; Jamnick et al. 2020). In the experiment 1, the HR during each cycling exercise was equivalent to 57.0% HRmax for 35% \({\dot{\text{V}}}\)O2max exercise intensity, 76.3% HRmax for 55% \({\dot{\text{V}}}\)O2max, and 94.3% HRmax for 75% \({\dot{\text{V}}}\)O2max. Therefore, an exercise intensity of 75% \({\dot{\text{V}}}\)O2max for 30 min in this study may have decreased the saliva flow rate by increasing sympathetic nervous activity. Several studies have shown that exercise-induced hypothalamic–pituitary–adrenal (HPA) axis activity may regulate the saliva flow rate via adrenergic stimulation by enhancing circulating cortisol secretion from the adrenal cortex (Chicharro et al. 1998; Hackney and Walz 2013). In this experiment 1, an increase in salivary cortisol concentration, an index of systemic secretion, was observed after cycling exercise at 75% \({\dot{\text{V}}}\)O2max for 30 min, but it did not change after cycling exercise at 35% and 55% \({\dot{\text{V}}}\)O2max. Furthermore, a significant negative correlation was found between the change in saliva flow rate and change in salivary cortisol concentration before and after exercise (r = − 0.52, P < 0.01), suggesting that the change in cortisol secretion may be involved in the decrease in saliva flow rate. Therefore, high-intensity exercise-induced upregulation of the autonomic nervous system and/or HPA axis activity may have caused the decrease in the s-IgA secretion rate by decreasing the saliva flow rate at 75% \({\dot{\text{V}}}\)O2max cycling exercise for 30 min.
In this study, the s-IgA secretion rate was transiently reduced after cycling exercise at 55% \({\dot{\text{V}}}\)O2max for 90 min; however, no significant changes in the saliva flow rate or s-IgA concentration were observed. Walsh et al. (2004) have shown decreased saliva flow rates after cycling exercise at 60% \({\dot{\text{V}}}\)O2max for 100 min (Walsh et al. 2004). Furthermore, Mc Naughton et al. (2006) have showed reduced s-IgA concentrations after cycling exercise at 60% \({\dot{\text{V}}}\)O2max for 90 min (Mc Naughton et al. 2006). As the s-IgA secretion rate was calculated by multiplying the s-IgA concentration and saliva flow rate, a slight decrease in s-IgA concentration and saliva flow rate, which were not statistically visible, may have led to the reduction of the s-IgA secretion rate in this study. To test this hypothesis, it is necessary to examine using the protocol of exercise durations for more than 90 min.
This study had certain limitations. First, in the experiment 1, s-IgA secretion decreased compared to that before exercise in 5 out of 12 subjects at 35% \({\dot{\text{V}}}\)O2max, 3 at 55% \({\dot{\text{V}}}\)O2max, and 9 at 75% \({\dot{\text{V}}}\)O2max. Furthermore, in the experiment 2, s-IgA secretion decreased compared to that before exercise in 3 out of 12 subjects at 30 min, 7 at 60 min, and 8 at 90 min. Thus, the threshold of exercise intensity or duration required to reduce s-IgA secretion may vary depending on the individuals. The threshold of intensity or duration required for exercise to induce the same decrease in s-IgA secretion may be higher or longer, respectively. Further studies are required to examine the response of s-IgA to higher exercise intensities or longer exercise durations. Second, the experiments 1 and 2 did not measure fluid intake during or after exercise. In the experiment 1, only four participants had measured their weight preliminarily before and after exercise: 35% \({\dot{\text{V}}}\)O2max exercise intensity for 30-min had a 0.2% decrease, 55% \({\dot{\text{V}}}\)O2max had a 0.4% decrease, and 75% \({\dot{\text{V}}}\)O2max had a 0.7% decrease after exercise. In the experiment 2, 55% \({\dot{\text{V}}}\)O2max exercise intensity for 30-min had a 0.4% decrease, 60-min had a 0.8% decrease, and 90-min had a 1.3% decrease after exercise. Previous studies have reported that a decrease in saliva flow rate due to dehydration is affected by a decrease in body weight of 3.0% or more (Walsh et al. 2004). However, since this study showed both a trend of increasing dehydration and decreasing saliva flow rate at dehydration levels of less than 3.0% change in body weight, future studies are needed to examine the effects of lower levels of exercise induced dehydration on the saliva flow rate. In addition, these saliva flow rate-related differences might affect the s-IgA and cortisol secretion responses to exercise. Further studies would thus be required to examine the influence of minimized changes in the saliva flow rate.
In conclusion, the present findings suggest a transient decrease in the s-IgA secretion rate in response to acute exercise at greater than or equal to 75% \({\dot{\text{V}}}\)O2max exercise intensity for 30 min or at 55% \({\dot{\text{V}}}\)O2max exercise intensity for greater than or equal to 90 min in healthy untrained young men.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- HPA:
-
Hypothalamic–pituitary–adrenal
- HR:
-
Heart rate
- HRmax:
-
Maximal heart rate
- RPE:
-
Rating of perceived exertion
- \({\dot{\text{V}}}\)O2max :
-
Maximal oxygen uptake
- s-IgA:
-
Salivary immunoglobulin A
References
Allgrove JE, Gomes E, Hough J, Gleeson M (2008) Effects of exercise intensity on salivary antimicrobial proteins and markers of stress in active men. J Sports Sci 26:653–661. https://doi.org/10.1080/02640410701716790
American College of Sports Medicine (2000) American College of Sports Medicine’s Guidelines for Exercise Testing and Prescription. 6th ed. Baltimore, Maryland.
Balsalobre-Fernández C, Tejero-González CM, del Campo-Vecino J (2014) Hormonal and neuromuscular responses to high-level middle- and long-distance competition. Int J Sports Physiol Perform 9:839–844. https://doi.org/10.1123/ijspp.2013-0539
Bishop NC, Gleeson M (2009) Acute and chronic effects of exercise on markers of mucosal immunity. Front Biosci 14:4444–4456. https://doi.org/10.2741/3540
Bishop NC, Blannin AK, Armstrong E, Rickman M, Gleeson M (2000) Carbohydrate and fluid intake affect the saliva flow rate and IgA response to cycling. Med Sci Sports Exerc 32:2046–2051. https://doi.org/10.1097/00005768-200012000-00013
Borg GA (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14:377–381
Chicharro JL, Lucía A, Pérez M, Vaquero AF, Ureña R (1998) Saliva composition and exercise. Sports Med 26:17–27. https://doi.org/10.2165/00007256-199826010-00002
Dimitriou L, Sharp NC, Doherty M (2002) Circadian effects on the acute responses of salivary cortisol and IgA in well trained swimmers. Br J Sports Med 36:260–264. https://doi.org/10.1136/bjsm.36.4.260
Gleeson M, Lancaster GI, Bishop NC (2001) Nutritional strategies to minimise exercise-induced immunosuppression in athletes. Can J Appl Physiol 26(Suppl):S23–S35. https://doi.org/10.1139/h2001-039
Gomar-Vercher S, Simón-Soro A, Montiel-Company JM, Almerich-Silla JM, Mira A (2018) Stimulated and unstimulated saliva samples have significantly different bacterial profiles. PLoS ONE 13:e0198021. https://doi.org/10.1371/journal.pone.0198021
Hackney AC, Walz EA (2013) Hormonal adaptation and the stress of exercise training: the role of glucocorticoids. Trends Sport Sci 20:165–171
Hasegawa N, Fujie S, Kurihara T, Homma T, Sanada K, Sato K, Hamaoka T, Iemitsu M (2016) Effects of habitual aerobic exercise on the relationship between intramyocellular or extramyocellular lipid content and arterial stiffness. J Hum Hypertens 30:606–612. https://doi.org/10.1038/jhh.2016.28
Hucklebridge F, Clow A, Evans P (1998) The relationship between salivary secretory immunoglobulin a and cortisol: neuroendocrine response to awakening and the diurnal cycle. Int J Psychophysiol 31:69–76. https://doi.org/10.1016/s0167-8760(98)00042-7
Jamnick NA, Pettitt RW, Granata C, Pyne DB, Bishop DJ (2020) An Examination and critique of current methods to determine exercise intensity. Sports Med 50:1729–1756. https://doi.org/10.1007/s40279-020-01322-8
Koch AJ, Wherry AD, Petersen MC, Johnson JC, Stuart MK, Sexton WL (2007) Salivary immunoglobulin a response to a collegiate rugby game. J Strength Cond Res 21:86–90. https://doi.org/10.1519/00124278-200702000-00016
Laing SJ, Gwynne D, Blackwell J, Williams M, Walters R, Walsh NP (2005) Salivary IgA response to prolonged exercise in a hot environment in trained cyclists. Eur J Appl Physiol 93:665–671. https://doi.org/10.1007/s00421-004-1270-7
Lamm ME, Nedrud JG, Kaetzel CS, Mazanec MB (1995) IgA and mucosal defense. APMIS 103:241–246. https://doi.org/10.1111/j.1699-0463.1995.tb01101.x
Li TL, Gleeson M (2005) The effects of carbohydrate supplementation during repeated bouts of prolonged exercise on saliva flow rate and immunoglobulin a. J Sports Sci 23:713–722. https://doi.org/10.1080/02640410400022151
Libicz S, Mercier B, Bigou N, Le Gallais D, Castex F (2006) Salivary IgA response of triathletes participating in the French Iron Tour. Int J Sports Med 27:389–394. https://doi.org/10.1055/s-2005-865747
Mackinnon LT, Hooper S (1994) Mucosal (secretory) immune system responses to exercise of varying intensity and during overtraining. Int J Sports Med 15(Suppl 3):S179–S183. https://doi.org/10.1055/s-2007-1021134
Mackinnon LT, Ginn E, Seymour GJ (1993) Decreased salivary immunoglobulin a secretion rate after intense interval exercise in elite kayakers. Eur J Appl Physiol Occup Physiol 67:180–184. https://doi.org/10.1007/BF00376664
Marcotte H, Lavoie MC (1998) Oral microbial ecology and the role of salivary immunoglobulin a. Microbiol Mol Biol Rev 62:71–109. https://doi.org/10.1128/MMBR.62.1.71-109.1998
Matsubara Y, Shimizu K, Tanimura Y, Miyamoto T, Akimoto T, Kono I (2010) Effect of acupuncture on salivary immunoglobulin a after a bout of intense exercise. Acupunct Med 28:28–32. https://doi.org/10.1136/aim.2009.001677
Mc Naughton L, Bentley DJ, Koeppel P (2006) The effects of a nucleotide supplement on salivary IgA and cortisol after moderate endurance exercise. J Sports Med Phys Fitness 46:84–89
McDowell SL, Chaloa K, Housh TJ, Tharp GD, Johnson GO (1991) The effect of exercise intensity and duration on salivary immunoglobulin A. Eur J Appl Physiol Occup Physiol 63:108–111. https://doi.org/10.1007/BF00235178
Murase Y, Shimizu K, Tanimura Y, Hanaoka Y, Watanabe K, Kono I, Miyakawa S (2016) Salivary extracellular heat shock protein 70 (eHSP70) levels increase after 59 min of intense exercise and correlate with resting salivary secretory immunoglobulin A (SIgA) levels at rest. Cell Stress Chaperones 21:261–269. https://doi.org/10.1007/s12192-015-0656-2
Nieman DC, Dumke CI, Henson DA, McAnulty SR, McAnulty LS, Lind RH, Morrow JD (2003) Immune and oxidative changes during and following the western states endurance run. Int J Sports Med 24:541–547. https://doi.org/10.1055/s-2003-42018
Pedersen BK, Bruunsgaard H (1995) How physical exercise influences the establishment of infections. Sports Med 19:393–400. https://doi.org/10.2165/00007256-199519060-00003
Peñailillo L, Maya L, Niño G, Torres H, Zbinden-Foncea H (2015) Salivary hormones and IgA in relation to physical performance in football. J Sports Sci 33:2080–2087. https://doi.org/10.1080/02640414.2015.1064151
Usui T, Yoshikawa T, Orita K, Ueda SY, Katsura Y, Fujimoto S, Yoshimura M (2011) Changes in salivary antimicrobial peptides, immunoglobulin A and cortisol after prolonged strenuous exercise. Eur J Appl Physiol 111:2005–2014. https://doi.org/10.1007/s00421-011-1830-6
Walsh NP, Laing SJ, Oliver SJ, Montague JC, Walters R, Bilzon JL (2004) Saliva parameters as potential indices of hydration status during acute dehydration. Med Sci Sports Exerc 36:1535–1542. https://doi.org/10.1249/01.mss.0000139797.26760.06
Woof JM, Mestecky J (2005) Mucosal immunoglobulins. Immunol Rev 206:64–82. https://doi.org/10.1111/j.0105-2896.2005.00290.x
Acknowledgements
This work was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (KAKENHI: 22H03487, to M. Iemitsu) and a Leading-edge Research Project for Sports Medicine and Science of Japan Sports Agency (to T. Isaka). We would like to thank Editage (www.editage.com) for the English language editing.
Funding
Open Access funding provided by Ritsumeikan University. Grant-in-Aid for Scientific Research from the Ministry of Education,Culture, Sports, Science and Technology of Japan, 22H03487, Motoyuki Iemitsu, Leading-edge Research Project for Sports Medicine and Science of Japan Sports Agency.
Author information
Authors and Affiliations
Contributions
TU, MU, SF and MI conceived and designed this study. TU, MU, RI, SF, KI, CK, YS, TH and MI analyzed and collection of data. MN, KS and YT contributed and revising for critical intellectual content. TI and MI obtained funding. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest. The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
Ethical approval
This study was approved by the Ethics Committee of Ritsumeikan University (BKC-LSMH-2021–054) and conducted in accordance with the Declaration of Helsinki. All participants were given verbal and written briefings on the study and provided informed written information.
Additional information
Communicated by Fabio Fischetti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uchino, T., Uchida, M., Ito, R. et al. Effects of different exercise intensities or durations on salivary IgA secretion. Eur J Appl Physiol 124, 2687–2696 (2024). https://doi.org/10.1007/s00421-024-05467-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-024-05467-6