
Abstract
It is known that a single bout of foam rolling (FR) or stretching can induce changes in range of motion (ROM) and performance in non-directly adjoining areas of the dorsal chain (i.e., remote effects). However, to date, it is not known if such effects exist following long-term interventions. Thus, the purpose of this study was to investigate the remote effects of a 7-week combined stretching and FR training intervention of the plantar foot sole. Thirty-eight recreational athletes were randomly assigned to either an intervention (n = 20) or control (n = 18) group. The intervention group performed stretching and FR exercises of the plantar foot sole for 7 weeks. Before and after the intervention, the dorsiflexion ankle ROM, passive resistive torque at maximum angle (PRTmax) and at a fixed angle, as well as maximum voluntary isometric contraction (MVIC) torque, were measured with a dynamometer. Gastrocnemius medialis and lateralis stiffness was assessed with shear wave elastography. The results showed no interaction effect for any of the parameters. There was a time effect indicating an increase in MVIC and PRTmax, which was more pronounced in the intervention group (+ 7.4 (95% CI 2.5–12.4), + 4.5 (95% CI − 0.2–9.2)) than the control group (+ 3.6 (95% CI − 1.4–8.6), + 4.0 (95% CI − 2.2 to 10.2)). The results indicate no or minor remote effects of combined stretching and FR of the foot sole in the ankle joint. Potential non-significant changes in ROM were accompanied with an increase in stretch tolerance, but not with changes in muscle structure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stretching and foam rolling (FR) training is frequently performed in rehabilitation settings, and also in sports practice. Stretching training with its various methods (e.g., static stretching) for several weeks can induce chronic changes in local range of motion (ROM) (Medeiros and Martini 2018). It has been suggested that high-intensity and/or high-volume stretching must be applied to induce chronic changes in muscle–tendon unit properties, such as a decrease in stiffness (Freitas et al. 2018; Nakamura et al. 2021a, b). Otherwise, changes in the perception to stretch or stretch tolerance rather than structural changes are considered to be the main mechanisms responsible for the increase in ROM following stretching training over several weeks (Konrad and Tilp 2014; Freitas et al. 2018). In addition, it has been shown that high-volume stretching (> 30 min stretching per week) for several weeks can induce an increase in muscle strength (Yahata et al. 2021; Warneke et al. 2022a) as well as induce muscle hypertrophy (Warneke et al. 2022a, b, 2023). With regard to FR training, a recent meta-analysis showed that FR can increase quadriceps and hamstrings (but not triceps surae) ROM in the long term, if performed for more than 4 weeks (Konrad et al. 2022b). It is believed that such an increase in ROM after an FR intervention can be mainly attributed to increased stretch tolerance by, for example, tolerating higher passive torque values at the end ROM (Kasahara et al. 2022). With regard to performance parameters (e.g., maximum voluntary contractions, vertical jump height), another meta-analysis reported no changes following FR training interventions (ES = 0.294; p = 0.281) (Konrad et al. 2022a).
Although, in recent years, the evidence on the long-term local effects of stretching and FR training on various parameters, such as ROM, has grown, to date, there is no clear consensus on the long-term remote effects. Remote effects can be defined as non-local effects which might occur along myofascial chains linked via connective tissue. One of these chains, the dorsal chain, is often referred to as the superficial back line. The superficial back line extends from the plantar fascia over the Achilles tendon, the gastrocnemii muscles, and the hamstring muscles, through the back to the head (Stecco et al. 2019; Wilke et al. 2016). Various studies on acute effects have demonstrated that a single FR treatment on the plantar foot sole causes an increase in ROM of the hamstring muscles and the lower back (Grieve et al. 2015; Patel et al. 2016; Do et al. 2018). Moreover, a single treatment of the plantar foot sole through a combination of massage, FR, and stretching exercises resulted in an acute decrease in the performance of the dorsal chain (Gabriel et al. 2021). According to these studies, it can be assumed that muscle function can be acutely adjusted along the superficial back line. However, to date, it is not clear if this is the case for long-term training interventions.
Therefore, the purpose of this study was to investigate the remote effects of a 7-week combined stretching and FR training intervention of the plantar foot sole three times a week for 15 min per session on ankle ROM and strength and stiffness of the triceps surae muscles. We hypothesized that the 7-week intervention would increase dorsiflexion ankle ROM, but would not have any impact on plantar flexor strength. We further assumed that the change in ankle ROM would be associated with increased stretch tolerance (i.e., an increase in passive torque at maximum dorsiflexion ankle ROM), but without a decrease in stiffness of the triceps surae muscles.
Materials and methods
Participants
In a previous study (Konrad and Tilp 2014), a 6-week static stretching training program of the triceps surae muscles showed a large effect size (Cohen’s d = 1.1) for the increased ankle ROM. Hence, with the power to detect a large effect size, we calculated a minimum sample size of 15 participants for each group for this study (difference between two dependent means, effect size = 0.8, α = 0.05, 1 − β = 0.8) using G*Power software (G*Power version 3.1., Heinrich-Heine-University Düsseldorf, Germany) (Faul et al. 2009). Consequently, taking into account possible drop-outs, 38 healthy recreational athletes (female: n = 15, age: 28.4 ± 4.4 years, weight: 62.9 ± 7.4 kg, height: 167.9 ± 4.9 cm; male: n = 23, age: 26.4 ± 5.3 years, weight: 81.9 ± 7.2 kg, height: 183.3 ± 6.7 cm) volunteered in this study. All participants were free of any injury of the lower extremities and participated in a familiarization session to get used to the testing procedure. Although participants were informed about the testing procedure they were not informed about the hypotheses of this study. Possible risks and benefits were explained to the participants before they signed a written informed consent form. The ethical commission of the University of Graz consented to the ethical approval (approval code GZ. 39/68/63 ex 2020/2021), which conformed to the Declaration of Helsinki.
Procedure
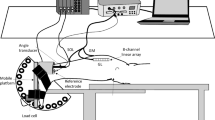
Each participant visited the laboratory three times—for a familiarization session, a pre-session before the 7-week intervention, and a post-session at the end of the intervention period. In the pre-session, the participants were randomly assigned to either the intervention or the control group by picking a hidden card (intervention group n = 20, control group n = 18). Males and females had separate cards to guarantee an equal distribution of the two sexes in both groups. Each appointment started with a 5-min warm-up on a stationary bike (Monark, Ergomedic 874 E, Sweden) at 60 rev.min-1 and 60 W. The measurements were performed on the dominant leg (i.e., the leg used for kicking a ball), and the following parameters were measured: ankle dorsiflexion ROM, passive resistive torque (PRT) in the ankle joint, maximum voluntary isometric contraction (MVIC) peak torque of the plantar flexor muscles, and muscle stiffness of the two gastrocnemius muscles (medialis (GM) and lateralis (GL)), assessed with shear wave elastography (SWE). Muscle activation level was measured via surface electromyography (sEMG) during the passive tests (ROM, PRT, SWE) to confirm that the participants were completely relaxed during the measurements. The order of the measurements is shown in Fig. 1, which was chosen to avoid any interfering effects between tests.

Schematic representation of the project procedure. Note: range of motion (ROM), gastrocnemius medialis (GM), gastrocnemius lateralis (GL), maximum voluntary isometric contraction (MVIC)
Dorsiflexion range of motion (ROM)
For the dorsiflexion ROM testing, the participant was positioned prone on a bench with the ankle fixed on a dynamometer (Con Trex MJ, CMV AG, Dübendorf, Switzerland). The ankle joint axis of the dominant leg was aligned with the rotation axis of the dynamometer using a custom-made laser device, and the foot was fixed to the footplate with straps. The exact position was noted during the familiarization session, to measure the participant in the same position for all appointments. Moreover, to avoid any evasive movements, the participant’s trunk was fixed with two “seatbelt-like” straps and an additional fixation was wrapped around the hip. Operating a remote control, the participant was asked to move their ankle joint with an angular velocity of maximum 5°/s into the maximum possible dorsiflexion position. The maximum position was maintained for a second, and the ankle joint was then moved back into neutral position. This procedure was performed three times, with a 5 s break in between each attempt. The highest ROM value (i.e., the highest dorsiflexion ankle angle) reached was taken for further analysis.
Passive resistive torque (PRT)
In the same position as during the ROM measurement, the ankle joint was moved passively between neutral position (90°) and the participant’s individual dorsiflexion ROM (PRTmax) with an angular velocity of 5 s−1, to avoid any reflexive muscle activation (Kubo et al. 2002). Five cycles were conducted, and the lowest value of the maximum dorsiflexion of the last three cycles was taken for further analysis. In addition, PRT at a given angle (PRTfixed) was determined at the maximum angle achieved in both trials (pre and post). To monitor if the participant remained completely relaxed, the muscle activation level was measured with sEMG continuously during the test. In the case of an activation, the whole procedure was repeated.
Shear wave elastography (SWE)
For the SWE testing, an ultrasound scanner (Aixplorer V12.3, Supersonic Imaging, Aix-en-Provence, France) was used. A linear transducer array (4–15 MHz, SuperLinear 15–4, Vermon, Tours, France) measured the muscle stiffness of the GM and GL in SWE mode (musculoskeletal preset, penetration mode, smoothing level 5, persistence off, scale 0–450 kPa). The participant was in the same position as described for the ROM measurements. The proceeding PRT measurement was used as conditioning for the SWE, to ensure the same condition at every appointment. SWE measurements were performed with a handheld technique (according to Lacourpaille et al. (2012)) in neutral ankle joint position (90°). We used a reusable foil, where the individual characteristics of the participant’s skin and the probe position were marked. A B-mode picture of the first measurement was also taken, to ensure reliable measurements (see Reiner et al. 2021). The shear modulus measurement position of both muscles (i.e., the GM and GL) was at the proximal third between the popliteal fossa (medially and laterally, respectively) and the calcaneus. Care was taken to avoid any deformation of body tissue due to pressure applied by the ultrasound probe during the measurement procedure (Kot et al. 2012). Aligning the probe in plane with the muscle fascicles, the region of interest (ROI) of the SWE was defined as the maximum possible size between, but not including, the aponeuroses. The participant’s passivity in the tested muscle tissue was checked visually with sEMG throughout the testing phase. For each muscle, three videos with a duration of 15 s each were recorded. For the further analysis, the mean of five consecutive frames with the lowest standard deviation within the ROI (averaged values) within one video was taken. The shear modulus of a muscle was then calculated as the mean between the two closest values of the three videos (Morales-Artacho et al. 2017).
Maximum voluntary isometric contraction (MVIC) peak torque
The MVIC peak torque measurements of the plantar flexors were performed in the same position as all the other tests (prone position, ankle = 90°, proper fixation on hip and trunk). Each participant performed three MVICs of 5 s each, with a break of 1 min in between each attempt. The participant was verbally encouraged to push as hard as possible during the trial. The highest value was considered for further analysis. As with the previous measurements, the sEMG-signal was also recorded during the test.
Surface electromyography (sEMG)
The sEMG (myon 320; myon AG, Zurich, Switzerland) was assessed during all the measurements (ROM, PRT, SWE, and MVIC), with a sample rate of 2000 Hz. The skin was prepared and the surface electrodes (Blue Sensor N, Ambu A/S, Ballerup, Denmark) were positioned on the GL in the proximal third of the muscle belly according to the “European Recommendations for surface Electromyography” (SENIAM) (Hermens et al. 1999). The inter-electrode distance was 2 cm. The raw sEMG values were monitored live during the ROM, PRT, and SWE measurements. If necessary, from the MVIC trials, the sEMG signals were high pass filtered (10 Hz, Butterworth) and the root mean square (RMS, 50 ms window) was calculated.
Seven-week stretching and foam rolling intervention
Each participant was asked to perform three exercises for 5 min each (continuously, without a resting phase during each exercise), three times a week (recommendation: Monday, Wednesday, Friday), for a period of 7 weeks. Therefore, the total training duration per session was 15 min, with a total weekly training load of 45 min. Exercise 1 was a plantar foot sole stretch, where the participant positioned themselves in front of a wall, facing the wall. The participant’s toes and the ball of the foot were placed on the wall, while the heel stayed on the floor. To induce a stretch sensation, the ball of the foot should be pushed toward the floor. The participant was asked to maintain the position with the greatest tolerable stretching intensity. If the stretching intensity was too low in the standing position, the participant could either take a seat or cross their calf over the contralateral thigh and induce a plantar facia stretch by pulling their toes and the ball of their foot in the dorsal direction until they experienced a significant stretching intensity (see Fig. 2A). Exercise 2 was a rolling exercise performed with a custom-made wooden cylinder (diameter = 5.5 cm, length = 15 cm). The participant was asked to roll constantly along the plantar foot sole, linearly between the ball of the foot and the heel at a slow speed (i.e., ~ 2 s back and forth) and with as much pressure as tolerable (see Fig. 2B). Exercise 3 was another rolling exercise, but was performed with a foam roller ball (Ball 08, Blackroll, Bottighofen, CH). The participant was asked to roll constantly and slowly in small circles, and to cover the part of the sole of the foot between the ball of the foot and the heel (see Fig. 2C). The added pressure should again be as high as tolerable. Exercises 2 and 3 could be performed while sitting on a chair or standing with support while touching a wall or a desk. The participant was asked to perform the exercises in the same way during the whole intervention period. If interested, the participant was allowed to perform both exercises bilaterally.

Figures of the stretching exercise (A) and foam rolling exercises (B, C) done within this study
The investigators supervised every single training session of the participants. In addition, the participants were asked to fill in a training diary. A minimum of 80% of the intervention volume was needed to positively finish the intervention.
Control group
The participants in the control group were asked to perform a stretching program with three exercises of the pectoralis muscles, with the same instructions regarding duration, intensity, and period as the intervention group.
Statistical analyses
Statistical analyses were performed using SPSS (Version 28, SPSS Inc., Chicago, Illinois). The tested variables were dorsiflexion ROM, PRTmax, PRTfixed, MVIC plantar flexion peak torque, and shear modulus of the GM and GL. The baseline measurements did not differ between the two groups in any parameter. The data of all the parameters were tested for a normal distribution (Shapiro–Wilk test), and all were found to be normally distributed. A repeated measures ANOVA [factor: time (pre vs. post) and inter-subject factor: group (intervention vs. control)] was performed. If significant results were detected in the ANOVA, a paired t test was performed. Effect size partial eta square (η2) was defined as small, medium, and large for effect sizes greater than 0.01, 0.06, and 0.14, respectively (Cohen 1988). The alpha level was set to 0.05.
Results
Significant time effects were revealed for PRT at maximum ROM (p < 0.01, F = 11.08; η2 = 0.28) and MVIC (p = 0.03, F = 5.13; η2 = 0.13) (Table 1). The increase for PRT at maximum ROM was 7.4 Nm in the intervention group and 3.6 Nm in the control group. Moreover, the increase in MVIC was 6.1 Nm, 2.2 Nm in the intervention group, control group, respectively.
There were no significant main effects for time with dorsiflexion ROM (p = 0.28; F = 1.19; η2 = 0.03), PRT at a fixed angle (p = 0.39; F = 0.76; η2 = 0.03), GM muscle stiffness (p = 0.34; F = 0.94; η2 = 0.03) or GL muscle stiffness (p = 0.67, F = 0.19; η2 = 0.01). Furthermore, there were no interaction effects for dorsiflexion ROM (p = 0.08; F = 3.26; η2 = 0.09), PRT at maximum ROM (p = 0.26, F = 1.32; η2 = 0.04), PRT at a fixed angle (p = 0.91; F = 0.01; η2 = 0.0), MVIC force (p = 0.29, F = 1.15; η2 = 0.03), GM muscle stiffness (p = 0.21; F = 1.67; η2 = 0.05) or GL muscle stiffness (p = 0.52, F = 0.42; η2 = 0.01) (Table 1).
Discussion
The purpose of this study was to investigate the remote effects of a comprehensive 7-week combined stretching and FR training intervention of the plantar foot sole on the function (ROM, strength, passive torque) and structure (muscle stiffness) of the plantar flexors. The intervention did not lead to significantly different changes in any parameter, compared to a control group, but an increase of MVIC and PRTmax was seen in both groups. This indicates that a combined stretching and FR training for 7 weeks (3 × week for 15 min) of the plantar sole does not have a remote effect on the plantar flexors.
Dorsiflexion ROM of the ankle was unchanged following the 7-week intervention of combined stretching and FR training. However, there was a tendency of an interaction effect for dorsiflexion ROM (p = 0.08). The pre-to-post comparison showed an increase in ROM in the intervention group of 2.0° (p = 0.05), while the change in the control group was − 0.1° (p = 0.62). A potential increase in ROM in the intervention group was underlined by the 95% CI of − 0.03 to 4.0. However, compared to local interventions, the long-term stretching and FR of the foot sole seems to have no or only minor effects, as it has been found that direct stretching training of the lower leg for several weeks leads to increases in ankle joint ROM of > 5.0° in young healthy adults (e.g., Konrad and Tilp 2014; Medeiros and Martini 2018)).
To the best of the authors’ knowledge, this study is the first to have investigated the long-term remote effects of a plantar foot sole treatment via stretching and FR training on the dorsiflexion ankle ROM. However, previous studies have investigated the acute remote effects of FR along the superficial back line and reported increases in ROM in the hamstrings and lower back following a single FR treatment of the plantar foot sole (Grieve et al. 2015; Patel et al. 2016; Do et al. 2018). Similarly, Wilke et al. (2017) showed that stretching of the hamstrings also increases ROM in non-directly adjacent areas of the superficial back line, namely, the neck. A recent review reported that acute changes in non-local tissue ROM following a single bout of stretching are likely due to altered global pain perception (Behm et al. 2021). Although this is not yet clear, it can be assumed that an adjusted global change in pain perception following a single bout of FR or stretching will increase ROM in all non-treated joints, due to the conditioning effects.
Contrary to this theory, prior studies investigating myofascial connections have shown, for example, that ankle position and passive torque influence hip mobility, and vice versa (Palmer et al. 2015; Andrade et al. 2016; Marinho et al. 2017). Cadaveric studies have provided evidence for a potential transfer of tension between adjacent myofascial structures in the superficial back line (Krause et al. 2016); however, only a few in-vivo studies have suggested that force transmission along the superficial back line might be possible (Cruz-Montecinos et al. 2015; Wilke et al. 2020). Wilke et al. (2020), for example, investigated the superficial back line via SWE and found tissue displacement in the hamstrings region after passive ankle dorsiflexion. In addition, Ahmad et al. (2021) showed that hamstrings stretching in combination with suboccipital manual techniques is more effective in increasing hamstring muscles ROM than local stretching alone. In terms of force generation, it has been shown that ankle position and training of the foot muscles influence hamstrings strength (Sulowska et al. 2019; Nishida et al. 2022). These findings suggest strain transfer along the superficial back line via fascial pathways in the lower extremity and beyond. However, there is still a need for in-vivo studies regarding myofascial transmission along the superficial back line and other myofascial connections (Wilke et al. 2020).
With regard to long-term stretching and FR training studies on non-local ROM, in recent years, various training studies on the contralateral effects have been conducted. In these studies, unilateral interventions (i.e., FR, stretching) for several weeks were performed, and the ROM of the contralateral homologous muscle was obtained. Following both long-term FR (Kasahara et al. 2022) and stretching studies (Caldwell et al. 2019; Panidi et al. 2021; Nakamura et al. 2022), an increase in ROM has been reported in the contralateral limb. The potential mechanism for such an increase in ROM of the contralateral limb is related to increased pain perception.
In this study, a time effect was found in PRTmax (i.e., stretch tolerance), although it was indeed more pronounced and significant (post-hoc p = 0.01) in the intervention group (+ 7.4 ((95% CI 2.5–12.4)) than the control group (+ 3.6 ((95% CI − 1.4–8.6) p = 0.14). Even though a comprehensive stretching and FR intervention (45 min per week) of the plantar foot sole was used, no significant changes in muscle stiffness or PRTfixed in the triceps surae were found in this study. This was likely because no mechanical load was applied on the triceps surae during the stretching and FR training. Consequently, this study confirmed that muscle stiffness of the gastrocnemii muscles and PRTfixed are not affected by non-local and long-term stretching and FR training. These findings are underlined by a previous study which studied the contralateral effects of a high-intensity stretching training intervention (Nakamura et al. 2022) and FR training of the triceps surae muscles (Kasahara et al. 2022). Although the authors found an increase in dorsiflexion ankle ROM in the contralateral limb, no changes in muscle stiffness on the contralateral side occurred. Similar to the findings of the present study, these authors found increased stretch tolerance to be the main mechanism for an increase in ROM in the contralateral limb following a stretching (Nakamura et al. 2022) or FR training intervention (Kasahara et al. 2022) of several weeks. Thus, according to the findings of the previous studies on stretching and FR training on the contralateral effects and our current findings on the remote effects, it can be concluded that direct stress (e.g., stretching load) has to be applied on the respective tissue to cause changes in structure.
Another explanation for the unaltered muscle stiffness of the gastrocnemii in the current study might be the dense and strongly connected structures of the plantar foot sole (Chaudhry et al. 2008), which impede structural changes even when high loads are applied.
In the current study, plantar flexion MVIC was also assessed. The results showed a significant time effect, although the pairwise comparison and confidence intervals showed a more pronounced and significant (post-hoc p = 0.04) effect in the intervention group for an increase in MVIC (+ 4.5 (95% CI − 0.2–9.2)), compared to the control group (+ 4.0 (95% CI − 2.2–10.2) p = 0.18). With regard to the local effects of stretching, it has been reported that high-volume stretching for several weeks can induce an increase in muscle strength, which is likely due to the repeated tension applied on the target tissue (Yahata et al. 2021; Warneke et al. 2022a). With regard to long-term FR, a recent meta-analysis reported no changes in muscle performance following an FR training intervention (ES = 0.294; p = 0.281) (Konrad et al. 2022a). However, it has to be noted that the included studies in this meta-analysis did not perform a comprehensive FR training intervention, with the total load ranging from 1080 to 3685 s over the whole intervention duration. Thus, more load with repeated stretches during FR might be required to induce changes in muscle performance, as has been seen in stretching training (Yahata et al. 2021; Warneke et al. 2022a). The findings on the remote effects of the current study are in agreement with a study which investigated the contralateral effects of stretching and FR training on MVIC. Kasahara et al. (2022) reported a non-significant increase in the contralateral plantar flexion MVIC of 0.64% and 2.02% following a 6-week conventional FR and vibration FR training intervention of the ipsilateral limb, respectively. A potential mechanism for the increase in plantar flexion MVIC seen in the current study might be the activation of the lower limb muscles (i.e., tibialis anterior, triceps surae), to support balance during the repeated stretching and FR exercises. Kokkonen et al. (2007) suggested that the increase in muscle performance seen after 10 weeks of stretching might not be related to the stretching stimulus itself, but instead could be due to the stabilization tasks performed during stretching (e.g., standing on the contralateral leg while stretching the ipsilateral leg). Similarly, Zahiri et al. (2022) showed that the muscle activity of the core muscles during a plank or reverse plank position is similar to that with quadriceps and hamstrings FR, respectively. Hence, tasks other than the intervention itself might be responsible for the adaptations in MVIC seen in the current study. A further explanation for the increase in plantar flexion MVIC throughout the intervention period in the current study might be that the participants were recreational athletes, and hence were following individual training regimes. Consequently, this would also explain the significant time effect in MVIC, indicating an increase in both the intervention group and control group.
There are some limitations of the current study. First, the control group has performed stretching exercises of the upper limbs and hence, a potential cross-over training effect in ROM as has been seen after a single bout of stretching (Behm et al. 2021) or FR (Konrad et al. 2023) cannot be ruled out completely. Second, since the intervention was performed as a combination of stretching and FR exercises, an isolated effect of either stretching or FR cannot be assessed.
Conclusions
This study is the first to have investigated the remote effects of a 7-week combined stretching and FR training intervention of the plantar foot sole on the function and structure of the triceps surae. The results indicate no or only minor remote effects for this intervention. A non-significant increase in ROM in the intervention group might be explained by an increase in stretch tolerance (PRTmax), but not by changes in the muscle structure (muscle stiffness), which was unaltered. Increases in plantar flexion MVIC were also observed in the control group, indicating that the 7-week intervention of the plantar foot sole was not the main reason for these changes.
Data availability
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Abbreviations
- CI:
-
Confidence intervals
- ES:
-
Effect size
- FR:
-
Foam rolling
- GM:
-
Gastrocnemius medialis
- GL:
-
Gastrocnemius lateralis
- MVIC:
-
Maximum voluntary isometric contraction
- PRT:
-
Passive resistive torque
- PRTfixed :
-
Passive resistive torque at a given angle
- PRTmax :
-
Passive resistive torque at participant’s individual dorsiflexion range of motion
- ROM:
-
Range of motion
- sEMG:
-
Surface electromyography
- SWE:
-
Shear wave elastography
References
Ahmad I, Manzoor T, Riaz S, et al (2021) Effects of remote myofascial release of sub-occipital region in asymptomatic individuals with hamstrings tightness. Pakistan Biomed J https://doi.org/10.54393/PBMJ.V4I2.101
Andrade RJ, Lacourpaille L, Freitas SR et al (2016) Effects of hip and head position on ankle range of motion, ankle passive torque, and passive gastrocnemius tension. Scand J Med Sci Sport 26:41–47. https://doi.org/10.1111/SMS.12406
Behm DG, Alizadeh S, Anvar SH et al (2021) Non-local acute passive stretching effects on range of motion in healthy adults: a systematic review with meta-analysis. Sport Med. https://doi.org/10.1007/s40279-020-01422-5
Caldwell SL, Bilodeau RLS, Cox MJ, Behm DG (2019) Cross education training effects are evident with twice daily, self-administered band stretch training. J Sport Sci Med 18:544–551
Chaudhry H, Schleip R, Ji Z et al (2008) Three-dimensional mathematical model for deformation of human fasciae in manual therapy. J Am Osteopath Assoc 108:379–390. https://doi.org/10.7556/JAOA.2008.108.8.379
Cohen J (1988) Statistical Power Analysis for the Behavioral Sciences. Lawrence Erlbaum Associates
Cruz-Montecinos C, González Blanche A, López Sánchez D et al (2015) In vivo relationship between pelvis motion and deep fascia displacement of the medial gastrocnemius: anatomical and functional implications. J Anat 227:665–672. https://doi.org/10.1111/JOA.12370
Do K, Kim J, Yim J (2018) Acute effect of self-myofascial release using a foam roller on the plantar fascia on hamstring and lumbar spine superficial back line flexibility. Phys Ther Rehabil Sci 7:35–40. https://doi.org/10.14474/PTRS.2018.7.1.35
Faul F, Erdfelder E, Buchner A, Lang A-G (2009) Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods 41:1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Freitas SR, Mendes B, Le Sant G et al (2018) Can chronic stretching change the muscle-tendon mechanical properties? A review. Scand J Med Sci Sport 28:794–806. https://doi.org/10.1111/SMS.12957
Gabriel A, Konrad A, Roidl A, et al (2021) Myofascial treatment techniques on the plantar surface influence functional performance in the dorsal kinetic chain. J Sport Sci Med 21:13–22. https://doi.org/10.52082/JSSM.2022.13
Grieve R, Goodwin F, Alfaki M et al (2015) The immediate effect of bilateral self myofascial release on the plantar surface of the feet on hamstring and lumbar spine flexibility: A pilot randomised controlled trial. J Bodyw Mov Ther 19:544–552. https://doi.org/10.1016/J.JBMT.2014.12.004
Hermens HJ, Freriks B, Merletti R, et al (1999) European recommendations for surface electromyography. Roessingh Res Dev 8–11
Kasahara K, Konrad A, Yoshida R et al (2022) Comparison between 6-week foam rolling intervention program with and without vibration on rolling and non-rolling sides. Eur J Appl Physiol. https://doi.org/10.1007/S00421-022-04975-7
Kokkonen J, Nelson AG, Eldredge C, Winchester JB (2007) Chronic static stretching improves exercise performance. Med Sci Sports Exerc 39:1825–1831. https://doi.org/10.1249/mss.0b013e3181238a2b
Konrad A, Tilp M (2014) Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech 29:636–642. https://doi.org/10.1016/j.clinbiomech.2014.04.013
Konrad A, Nakamura M, Behm DG (2022a) Foam Rolling Training Effects on Performance Parameters. Int J Environ Res Public Health, A Systematic Review and Meta-Analysis
Konrad A, Nakamura M, Tilp M et al (2022b) Foam rolling training effects on range of motion: a systematic review and meta-analysis. Sport Med 2022:1–13. https://doi.org/10.1007/S40279-022-01699-8
Konrad A, Nakamura M, Warneke K et al (2023) The contralateral effects of foam rolling on range of motion and muscle performance. Eur J Appl Physiol. https://doi.org/10.1007/s00421-023-05142-2
Kot BCW, Zhang ZJ, Lee AWC et al (2012) Elastic modulus of muscle and tendon with shear wave ultrasound elastography: variations with different technical settings. PLoS ONE 7:2–7. https://doi.org/10.1371/journal.pone.0044348
Krause F, Wilke J, Vogt L et al (2016) Intermuscular force transmission along myofascial chains: a systematic review. Wiley Online Libr 228:910–918. https://doi.org/10.1111/joa.12464
Kubo K, Kanehisa H, Fukunaga T (2002) Effects of resistance and stretching training programmes on the viscoelastic properties of human tendon structures in vivo. J Physiol 538:219–226. https://doi.org/10.1013/jphysiol.2001.012703
Lacourpaille L, Hug F, Bouillard K et al (2012) Supersonic shear imaging provides a reliable measurement of resting muscle shear elastic modulus. Physiol Meas. https://doi.org/10.1088/0967-3334/33/3/N19
Marinho HVR, Amaral GM, Moreira BS et al (2017) Myofascial force transmission in the lower limb: An in vivo experiment. J Biomech 63:55–60. https://doi.org/10.1016/J.JBIOMECH.2017.07.026
Medeiros DM, Martini TF (2018) Chronic effect of different types of stretching on ankle dorsiflexion range of motion: Systematic review and meta-analysis. Foot 34:28–35. https://doi.org/10.1016/J.FOOT.2017.09.006
Morales-Artacho AJ, Lacourpaille L, Guilhem G (2017) Effects of warm-up on hamstring muscles stiffness: Cycling vs foam rolling. Scand J Med Sci Sport 27:1959–1969. https://doi.org/10.1111/sms.12832
Nakamura M, Yoshida R, Sato S et al (2021b) Comparison between high- and low-intensity static stretching training program on active and passive properties of plantar flexors. Front Physiol 12:2287. https://doi.org/10.3389/FPHYS.2021.796497/BIBTEX
Nakamura M, Yahata K, Sato S et al (2021a) Training and detraining effects following a static stretching program on medial gastrocnemius passive properties. Front Physiol. https://doi.org/10.3389/FPHYS.2021.656579/FULL
Nakamura M, Yoshida R, Sato S et al (2022) Cross-education effect of 4-week high- or low-intensity static stretching intervention programs on passive properties of plantar flexors. J Biomech 133:110958. https://doi.org/10.1016/J.JBIOMECH.2022.110958
Nishida S, Ito W, Ohishi T, et al (2022) The effect of ankle position on peak eccentric force during the nordic hamstring exercise. J Sport Sci Med 21:43–48. https://doi.org/10.52082/JSSM.2022.43
Palmer TB, Akehi K, Thiele RM et al (2015) Dorsiflexion, plantar-flexion, and neutral ankle positions during passive resistance assessments of the posterior hip and thigh muscles. J Athl Train 50:467–474. https://doi.org/10.4085/1062-6050-49.6.04
Panidi I, Bogdanis GC, Terzis G et al (2021) Muscle architectural and functional adaptations following 12-weeks of stretching in adolescent female athletes. Front Physiol. https://doi.org/10.3389/FPHYS.2021.701338
Patel DG, Vyas NJ, Sheth MS (2016) Immediate effect of application of bilateral self myo-fascial release on the plantar surface of the foot on hamstring and lumbar spine flexibility: a quasi experimental study. Int J Ther Appl 32:94–99. https://doi.org/10.20530/IJTA_32_94-99
Reiner M, Tilp M, Guilhem G et al (2021) Effects of a single proprioceptive neuromuscular facilitation stretching exercise with and without post-stretching activation on the muscle function and mechanical properties of the plantar flexor muscles. Front Physiol to Be Printed. https://doi.org/10.3389/FPHYS.2021.732654
Stecco C, Pirri C, Fede C et al (2019) Dermatome and Fasciatome. Wiley Online Libr 32:896–902. https://doi.org/10.1002/ca.23408
Sulowska I, Mika A, Oleksy Ł, Stolarczyk A (2019) The influence of plantar short foot muscle exercises on the lower extremity muscle strength and power in proximal segments of the kinematic chain in long-distance runners. Biomed Res Int. https://doi.org/10.1155/2019/6947273
Warneke K, Zech A, Wagner CM et al (2023) Sex differences in stretch-induced hypertrophy, maximal strength and flexibility gains. Front Physiol 13:1–13. https://doi.org/10.3389/fphys.2022.1078301
Warneke K, Brinkmann A, Hillebrecht M, Schiemann S (2022a) Influence of long-lasting static stretching on maximal strength, muscle thickness and flexibility. Front Physiol. https://doi.org/10.3389/FPHYS.2022.878955/FULL
Warneke K, Keiner M, Hillebrecht M, Schiemann S (2022b) Influence of one hour versus two hours of daily static stretching for six weeks using a calf-muscle-stretching orthosis on maximal strength. Int J Environ Res Public Health. https://doi.org/10.3390/IJERPH191811621
Wilke J, Krause F, Vogt L, Banzer W (2016) What is evidence-based about myofascial chains: a systematic review. Arch Phys Med Rehabil 97:454–461. https://doi.org/10.1016/J.APMR.2015.07.023
Wilke J, Vogt L, Niederer D, Banzer W (2017) Is remote stretching based on myofascial chains as effective as local exercise? A randomised-controlled trial. J Sports Sci 35:2021–2027. https://doi.org/10.1080/02640414.2016.1251606
Wilke J, Debelle H, Tenberg S et al (2020) Ankle motion is associated with soft tissue displacement in the dorsal thigh: an in vivo investigation suggesting myofascial force transmission across the knee joint. Front Physiol. https://doi.org/10.3389/FPHYS.2020.00180
Yahata K, Konrad A, Sato S et al (2021) Effects of a high-volume static stretching programme on plantar-flexor muscle strength and architecture. Eur J Appl Physiol 121:1159–1166. https://doi.org/10.1007/S00421-021-04608-5
Zahiri A, Alizadeh S, Daneshjoo A et al (2022) Core muscle activation with foam rolling and static planks. Front Physiol 13:852094
Acknowledgements
This study was supported by a grant (Project P 32078-B) from the Austrian Science Fund FWF.
Funding
Open access funding provided by Austrian Science Fund (FWF).
Author information
Authors and Affiliations
Contributions
AK and MT were concepting the study design. MR was responsible for the data acquisition. AK and MRr performed the data analysis. The data interpretation was undertaken by all authors. AK wrote the main draft of the manuscript. All authors were involved in drafting and critically revising the manuscript for intellectual content.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Communicated by Philip D Chilibeck.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Konrad, A., Reiner, M.M., Gabriel, A. et al. Remote effects of a 7-week combined stretching and foam rolling training intervention of the plantar foot sole on the function and structure of the triceps surae. Eur J Appl Physiol 123, 1645–1653 (2023). https://doi.org/10.1007/s00421-023-05185-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-023-05185-5