
Abstract
The purpose of this study was to investigate the effect of age on cardiovascular changes and plasma concentrations of adrenomedullin (ADM), catecholamines, endothelin-1 (ET-1) and plasma renin activity (PRA) in healthy men. A total of 15 young (21 ± 0.3 years) and 15 older (64 ± 0.7 years) healthy men performed two 3-min bouts of static handgrip at 30% of maximal voluntary contraction, alternately with each hand without any break between the bouts. During exercise heart rate (HR), blood pressure (BP), stroke volume (SV) and pre-ejection period (PEP) and left ventricle ejection time (LVET) were measured. Blood samples were taken before exercise, at the end of both exercise bouts and in the fifth minute of the recovery period. The handgrip-induced increases in HR and cardiac output were significantly smaller in older than in young men (p < 0.01). SV decreased only in older men (p < 0.001). There were no differences between groups in BP increases. The baseline plasma ADM and catecholamines were higher in older man compared to young subjects. Handgrip caused increases in plasma ADM, ET-1 and PRA only in older men (p < 0.05). The increases in plasma ADM correlated positively with those of noradrenaline (NA), PRA, ET-1 and LVET and negatively with changes in total peripheral resistance (TPR), SV, PEP and PEP/LVET ratio. The increases in plasma ET-1 correlated positively with those of NA, PRA, TPR, mean BP and SV. These results revealed that ADM, ET-1 and angiotensin II can contribute to maintain vascular tone during static exercise in older but not in younger men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Static exercise is known to increase heart rate (HR) and cardiac output (CO) and raise systolic (SBP) and diastolic (DBP) blood pressures. These responses are related mainly to the neural effects on the heart including changes in the activities of both parasympathetic and sympathetic systems elicited by central command and to ascending mechanoreceptor and metaboreceptor inputs that contribute to the sympathetic response (Shepherd et al.1981; Markel et al. 2003; Lind 1970; Petrofsky and Lind 1975). Additionally, these neural influences are modulated by arterial baroreceptors (Scherrer et al. 1990). Little is known about the role of other factors in the cardiovascular response to static exercise. There are few data showing increases in circulating vasoconstrictor hormones during static exercise, but they have been obtained in subjects varying in age and health status. It was demonstrated, therefore, that static handgrip caused an increase in plasma vasopressin in healthy young men (Nazar et al. 1989), and endothelin-1 in hypertensive patients (Cottone et al. 1998), young normotensive offspring of hypertensive parents (Mangieri et al. 1998) and patients with congestive heart failure (Mangieri et al. 1997). On the other hand, we have recently demonstrated that static handgrip caused also an increase in the plasma adrenomedullin (ADM), which is a potent vasorelaxant probably involved in the fine blood pressure control counteracting the effect of vasoconstrictors. The increase in plasma ADM level was found in older healthy subjects and patients with heart failure (Krzeminski et al. 2002, 2006, 2009).
The role of aging as a factor influencing cardiovascular system function and vasoactive mechanisms has been extensively studied in resting subjects (Ferrari 2002; Ferrari et al. 2003; Lakatta 2002). Baseline activity of the sympathetic nervous system was found to be greater and the plasma endothelin-1 and ADM levels higher in older than in young subjects (Seals and Esler 2000; Thijssen et al. 2007; Kato et al. 2002; Kita et al. 2003). Numerous studies have addressed also the effect of aging on cardiovascular and sympathetic responses to sustained handgrip. It was demonstrated that in older subjects, an increase in muscle sympathetic nerve activity (MSNA) response to handgrip is attenuated (Markel et al. 2003; Housiiere et al. 2006). Since the difference was most pronounced during ischemic handgrip, it was suggested that reflex induced by metabolic changes (metaboreflex) in muscles is attenuated with aging. However, an increase in the plasma NA concentration during reflex activation of the sympathetic nervous system has been reported to be greater in older than in younger men (Palmer et al. 1978; Sachs et al. 1985; Sowers et al. 1983; Seals and Esler 2000). Esler et al. (1995) found that the increase in cardiac spillover of NA during isometric exercise in older men was two to three times larger than in the younger men and concluded that this effect was related to reduced neuronal NA reuptake.
The data concerning the effect of aging on BP and HR responses to static exercise are equivocal. Blood pressure responses in older men were found to be smaller (Markel et al. 2003), larger (Boutcher and Stocker, 1999) or similar (Taylor et al. 1991) to those in younger subjects. However, in the majority of papers, increases in HR in older men were reported to be smaller than those in younger subjects (Kino et al. 1975; Taylor et al. 1991; Housiiere et al. 2006). Since HR is an important determinant of cardiac output, these latter data confirm the concept of Lind et al. (1964) who suggested that older men need greater peripheral vascular resistance to achieve the rise of blood pressure during static handgrip because they increase cardiac output less than young men. The importance of peripheral vasoconstriction in determination of BP response to static exercise was supported by Haskell et al. (1981) and Martin et al. (1974), who examined patients unable to increase heart rate or stroke volume and found that the rise in BP during handgrip can be achieved by increased peripheral vascular resistance alone.
Since our previous study performed in older healthy men and in patients with heart failure (Krzeminski et al. 2002, 2006, 2009) showed interrelationships between changes in plasma ADM, catecholamine and cardiovascular responses to handgrip, it seemed of interest to extend these data to healthy young persons. Our hypothesis is that in healthy older subjects, the contribution of vasoactive hormones to cardiovascular response to static handgrip is greater than in young men. Thus, we measured simultaneously cardiovascular indices including heart rate, blood pressure, stroke volume, systolic time intervals and the endocrine variables including plasma concentrations of ADM, catecholamines, endothelin-1 and plasma renin activity during static handgrip exercise in young (19–23 years) and older (61–67 years) subjects.
Methods
Subjects
The study was performed with 15 young (mean age 21.3 ± 0.3 years) and 15 older (mean age 64 ± 0.7 years) male volunteers. They were recruited from the general community by advertisement and found to be in good health. A comprehensive clinical evaluation was performed on all subjects by a physician, with testing including exercise electrocardiography, echocardiography, hematological testing, and multipanel serum biochemistry screening. All were normotensive, non-obese, non-smokers and were not taking any medication.
All subjects gave their informed consent to participate in the study. The investigation conformed with the principles outlined in the Declaration of Helsinki and was approved by the local ethics committee. The general characteristics of the subjects are presented in Table 1.
Procedure
All the tests were carried out under similar environmental conditions (23–24°C and 40–50% humidity) between 4:00 and 5:00 p.m. The subjects visited the laboratory two times with 1 week interval between the tests. On the first occasion, the subjects were submitted to the incremental, graded exercise test performed on a bicycle ergometer (EM 840, Siemens, Germany) until volitional exhaustion to determine their maximal oxygen uptake (VO2max). The workloads were increased by 50 W every 3 min starting with 50 W. Oxygen uptake, carbon dioxide production and heart rate were continuously recorded using V max 29 (Sensormedics, USA) analyzer. On the second occasion, the subjects were submitted to the static handgrip exercise.
Each subject had maximal voluntary contraction (MVC) of their right and left hand determined using a hand dynamometer (Medipan, Poland). Afterward, a catheter was inserted into the antecubital vein in one arm for sampling of the plasma concentrations of adrenomedullin (ADM), noradrenaline (NA), adrenaline (A), endothelin-1 (ET-1) and plasma renin activity (PRA). After 30 min of rest period in a sitting position, baseline blood sample was taken and subjects performed two consecutive exercise bouts of 3-min handgrip at 30% MVC with each hand, without any resting interval between the bouts. Exercise was started with a catheterized hand and the blood sample was taken after the 3rd minute of exercise immediately after beginning the handgrip with the other hand, thus avoiding sample collection from the congested vein. The next blood sample was collected at the end of exercise also from the unexercising limb. The last blood sample was taken after 5 min of recovery. The subjects were instructed not to hold their breath during the handgrip to avoid a Valsalva maneuver and observation of their respiratory pattern was maintained during the experiment. The two exercise bout protocol was applied to prolong the duration of the stimulus action. The static handgrip at 30% MVC performed by one hand usually cannot be maintained longer than 3–4 min, which was thought to be too short a time period for marked activation of the endocrine system. A similar protocol was previously used by Nazar et al. (1989).
Measurements
Indices of cardiac functions were recorded continuously before and during the whole tests by the impedance cardiography (ICG) technique. The system allows for the off-line, beat-to-beat automatic evaluation of stroke volume (SV), heart rate (HR) and systolic time intervals (STI). The following phases of the cardiac cycle were measured directly and calculated automatically: (1) the total electromechanical systolic interval (QS2), (2) the pre-ejection period (PEP), (3) the left ventricular ejection time (LVET). The system was able to store and print the results of STI, R–R interval and HR as well as their mean values for each 5 s period. All intervals were calculated as a mean of the values from 5-s periods with an accuracy of 5 ms. In addition, the PEP/LVET ratio was calculated. The detailed description of the program for automatic determination of STI and other hemodynamic parameters has been previously published (Cybulski 1988). The validity of STI automatic measurements was checked earlier and verified in various physiological tests (Cybulski et al. 1993). The pre-exercise values of PEP, LVET and ratio PEP/LVET were corrected for HR according to Weissler’s formulas (1972): PEPI = (0.4 × HR) + PEP, LVETI = (1.7 × HR) + LVET, PEP/LVETIndex = (0.0168 × HR) + PEP/LVET. The exercise values of STI were uncorrected for HR because these corrections would mask the inotropic effect. There was evidence against this practice (Levi et al. 1982; Pigott et al. 1971; Spodick and Quarry-Pigott 1973; Whitsett and Naughton 1971).
Cardiac output (CO) was calculated as a product of SV and HR. Cardiac work (CW) was calculated as a product of HR and mean arterial pressure (MAP).
Blood pressure (BP) was measured at rest, before exercise, at the end of each 3-min bout and 5-min after termination of the test by auscultation on the non-exercising arm. MAP was calculated as diastolic pressure plus one-third of the pulse pressure. The total peripheral resistance (TPR) was estimated as TPR = MAP × 79.9/CO, where MAP is expressed in mmHg, CO in l min−1 and 79.9 is the conversion factor to dynes × s cm−5.
Biochemical analyses
Before exercise, at the end of each 3-min exercise bout and 5-min after termination of exercise, blood samples were taken for determination of the plasma concentrations of ADM, NA, A, ET-1 and PRA. The blood samples were taken in ice-chilled tubes. For catecholamine determination, tubes contained EDTA and reduced glutathione, while for ADM the tubes with 1.0 mg/ml of EDTA-2Na and 500 kallikrein inhibitory units (KIU) ml−1 of aprotinin were used. Plasma was obtained by centrifugation at 3,000 rpm for 10 min at 4°C and stored at −70°C until assay. All plasma hormone determinations were performed in duplicate. The plasma ADM concentrations were determined using radioimmunoassay kit for human ADM (Phoenix Pharmaceuticals, Inc.Belmont 94002 CA, USA). Minimal detectable concentration for this assay is 0.5 pg per tube, and the half-maximal inhibition dose of radiodinated ligand binding by ADM was 10 pg per tube. The intra-assay coefficient of variance was 5.3%. Plasma catecholamines were also measured by radioimmunoassay using 2 CAT RIA kit (Bio Source Europe, Nivelle, Belgium). The sensitivity of the assay was 37.5 and 7.5 pg ml−1 for noradrenaline and adrenaline, respectively; whereas the intra-assay coefficients of variance were 4.6 and 4.7%, respectively. For PRA determination Angiotensin I (Immunotech Prague, Czech Republic) kit was used. The sensitivity of the assay was 0.13 ng ml−1; the intra-assay coefficient of variance was 6.2%. The concentration of ET-1 in plasma was determined by ELISA method using commercial test pack from Biomedica (Vienna, Austria). The sensitivity of the assay was 0.1 fmol ml−1; the intra-assay coefficient of variation was 3.1%.
Statistics
The data are presented as means with standard errors (SEM). Two-way analysis of variance for repeated measures was used for statistical evaluation of the results. The two factors are the subjects group and repeated measures of plasma ADM, catecholamine, ET-1, PRA and hemodynamic indices. When significant F value was obtained, a paired Student’s test was used to locate the pairwise differences between means. A comparison between groups was made using a nonparametric Whitney–Mann test. In addition, correlation and linear regression coefficients were calculated. P < 0.05 was accepted as the level of significance. For calculations, the Statistica (2001) version 6. (Statsoft Inc., Tulsa, OK, USA) was used.
Results
Subject characteristics
The characteristics of subjects are summarized in Table 1. The aerobic capacities of the young and older men were within the normal range for men of their respective ages. The older men had a lower aerobic capacity compared with the young men. The peak oxygen uptake of the older men was smaller than that of the young men (P < 0.05).
Adrenomedullin, noradrenaline, adrenaline, endothelin-1 and plasma renin activity (Fig. 1)
Baseline values of plasma ADM, NA and A concentrations were significantly higher in older than in the young men (P < 0.05), while plasma ET-1 concentration and PRA did not differ between the groups.

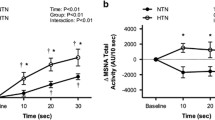
Plasma adrenomedullin, endothelin-1, noradrenaline and plasma renin activity (circles) and adrenaline (triangles), concentrations at rest, during handgrip (3’ and 6’) and at the fifth minute of the recovery period (rec.). Full symbols (closed circle, closed triangle) denote older men; open symbols (open circle, open triangle) denote young men. Values are mean ± SEM. Asterisks denote significant differences from the resting values: *P < 0.05, **P < 0.01 or less. Crosses denote significant differences between the groups of subjects: x P < 0.05, xx P < 0.01 or less
The static handgrip caused significant increases in plasma ADM, ET-1 and PRA only in the older subjects (P < 0.001). The exercise-induced increases in NA and A were significantly greater in the older subjects than in the young subjects (P < 0.001).
At the fifth minute of the recovery period, plasma ADM, NA, A, ET-1 and PRA did not differ significantly from the resting values.
A significant positive relationships between baseline values of plasma ADM and plasma NA concentrations were ascertained for older and younger groups of subjects (r = 0.76, P < 0.001; r = 0.62, P < 0.01; respectively). The exercise-evoked increases in plasma ADM concentrations expressed as percentage of baseline values correlated with those of plasma NA, ET-1 and PRA only in the older men (r = 0.80, P < 0.001; r = 0.74, P < 0.001 and r = 0.84, P < 0.001; respectively; Fig. 2). The exercise-evoked increases in plasma ET-1 concentrations expressed as percentage of baseline values correlated with those of plasma NA only in the older men (r = 0.56, P < 0.05).

The relationships between the changes in plasma adrenomedullin (∆ADM) and those of: noradrenaline (∆NA), endothellin-1 (∆ET-1), plasma renin activity (∆PRA) as well as between ∆ET-1 and ∆PRA in older subjects. All variables are expressed as percentage of baseline values
Significant positive relationships between baseline values of PRA and plasma ADM (r = 0.69; P < 0.01), and between the exercise-evoked increases in PRA expressed as percentage of baseline values and those of plasma NA and ET-1 (Fig. 2) were ascertained in the older men (r = 0.55, P < 0.05; r = 0.61, P < 0.001; respectively).
Heart rate, stroke volume and cardiac output (Fig. 3)
The resting values of HR, SV and CO did not differ significantly between the groups. Handgrip caused significant increases in HR and CO in both groups of subjects (P < 0.001). Stroke volume decreased in older men (P < 0.001), while in young men it was not affected by exercise. The handgrip-induced increases in HR and CO at the end of exercise were significantly lower in older men than in the young men (P < 0.01).

Heart rate, stroke volume (SV), cardiac output (CO), mean blood pressure (MAP), total peripheral resistance (TPR) as well as pre-ejection period (PEP), ejection period (LVET) and PEP/LVET ratio at rest, during handgrip (3’ and 6’) and at the fifth minute of the recovery period (rec.). Full points (closed circle) denote older men, and open points (open circle) denote young men. Values are mean ± SEM. Asterisks denote significant differences from the resting values: *P < 0.05, **P < 0.01 or less; Crosses denote significant differences between the groups of subjects: x P < 0.05, xx P < 0.01 or less
At the fifth minute of the recovery period, the HR, SV and CO returned to the baseline values in both groups of subjects.
A significant inverse relationships between baseline values of SV and TPR (r = −0.54, P < 0.05), as well as between the exercise-induced changes in SV expressed as percentage of baseline values and those of plasma ADM (r = −0.80, P < 0.001), TPR (r = −0.78, P < 0.001), PEP (r = −0.76, P < 0.001), LVET (r = 0.65, P < 0.01) and PEP/LVET (r = −0.60, P < 0.01) were ascertained in the older subjects.
Blood pressure and total peripheral resistance (Fig. 3)
Baseline systolic (SBP), diastolic (DBP) and mean arterial pressures (MAP) were similar in both groups of subjects. Handgrip increased SBP and DBP in both groups of subjects (P < 0.001). The magnitudes of the exercise-induced increments in SBP, DBP and MAP did not differ significantly between the groups.
Baseline TPR tended to be higher in older men. At the end of exercise, the absolute value of TPR was significantly higher in older than in the young men (P < 0.01). At the fifth minute of the recovery period, the values of SBP, DBP and TPR returned to the resting level.
A significant positive relationships between the exercise-evoked increases in SBP, MAP and TPR expressed as percentage of baseline values and those of ET-1 were ascertained in the older men (r = 0.68, P < 0.001; r = 0.62, P < 0.001; r = 0.57, P < 0.01; respectively; Fig. 4).

The relationships between the changes in plasma endothellin-1 (∆ET-1) and those of mean arterial pressure (∆MAP) and total peripheral resistance (∆TPR) in older subjects. All variables are expressed as percentage of baseline values

The relationships between the changes in plasma adrenomedullin (∆ADM) and those of: PEP/LVET ratio (∆PEP/LVET) in older subjects. All variables are expressed as percentage of baseline values
A significant inverse relationship between the exercise-induced increases in TPR expressed as a percentage of baseline values and those of plasma ADM were ascertained in the older subjects (r = −0.62, P < 0.001).
Cardiac work
There was no difference in cardiac work at rest, during handgrip or at the fifth minute of the recovery period between the two groups of subjects.
Systolic time intervals (Fig. 3)
The pre-exercise values of PEP, LVET, PEP/LVET ratio and their indices (PEPI and LVETI calculated according to Weissler) were similar in both groups of subjects.
Handgrip resulted in prolonged PEP, shortened LVET and increased PEP/LVET ratio in older men (P < 0.001), whereas in young men PEP and PEP/LVET ratio were not affected by exercise. Shortening of LVET during exercise was more marked in the older subjects (P < 0.001).
After 5 min of the recovery period, the values of PEP, LVET and PEP/LVET did not differ from the resting values (P < 0.05).
The exercise-induced changes in PEP, LVET and PEP/LVET ratio expressed as percentage of baseline values correlated significantly with those of plasma ADM in older subjects (r = −0.70, P < 0.001; r = 0.81, P < 0.001; r = −0.72, P < 0.001, (Fig. 5); respectively). The exercise-induced changes in PEP and PEP/LVET ratio expressed as percentage of baseline values, obtained in older subjects correlated also with those of plasma NA, A and TPR (r = −0.59, P < 0.01; r = −0.58, P < 0.01; r = 0.53, P < 0.05 and r = −0.60, P < 0.01; r = −0.71, P < 0.001; r = 0.69, P < 0.01; respectively).
Discussion
The new finding of this study is that despite similar increases in BP during static handgrip in young and older men, plasma ET-1, PRA and ADM increases were observed only in the latter. Furthermore, significant correlations were found between exercise-induced changes in cardiovascular indices and those in the hormone concentrations: namely positive correlations were ascertained between plasma ∆ET-1 and ∆ΜΑP, and ∆TPR; negative relationships between ∆ADM and ∆SV, ∆TPR or ∆PEP/LVET ratio. Also significant correlations were found between changes in the hormone concentrations: ∆ADM correlated positively with ∆ET-1, ∆PRA and ∆NA and there was correlation between ∆ET-1 and ∆PRA. Increases in plasma catecholamine concentrations indicated that static handgrip activated sympathetic adrenergic system in both groups of subjects, but the increases in plasma NA concentrations were accompanied by increases in plasma ET-1 and PRA only in the older men. Thus, a high level of sympathetic activity combined with activation of circulatory ET-1 and PRA could provide a mechanism for blood pressure increase during static exercise in older men.
The study showed also that a decrease in SV, prolongation of PEP, shortening of LVET, and an increase in TPR occurred only in older men, but not in the young subjects. In young men, cardiac output reached significantly higher values than in the older men, whereas changes in PEP, PEP/LVET ratio and TPR were negligible. The alterations in systolic time intervals during handgrip observed in this study are consistent with the findings of Kino et al. (1975) and Krzeminski et al. (2006) who reported increases in isovolumic contraction time (IVCT), PEP and PEP/LVET ratio during static exercise both in patients with coronary artery disease and in the older healthy subjects. The authors concluded that increased PEP/LVET ratio may result from a reduced velocity of myocardial fiber shortening during the ejection period. It should be noted that PEP/LVET ratio has been proposed as an inverse index of left ventricular myocardial performance (Weissler et al. 1969; Weissler 1972; Martin et al. 1971. The prolongation of PEP during handgrip in the older men might be explained by failure of the heart to respond to acutely increased left ventricle afterload. On the other hand, the lack of changes in PEP during handgrip in young men may indicate that there is an increase in myocardial contractility or in ventricular end-diastolic fiber length, or both, to counterbalance the acute increase of systemic arterial pressure. The rise of systolic and diastolic blood pressures was similar in young and older subjects. Thus, the present results are in agreement with a number of studies indicating that vascular resistance plays a minor role in the pressor response to exercise in younger subjects, but is an important determinant of this response in older men.
Among several players involved in the regulation of vascular tone, the ET-1 and nitric oxide (NO) appears to be the predominant members of the family generated by vascular endothelial cells (Cardillo et al. 2000; Warner 1999). Endothelin-1 contributes to maintenance of basal vascular tone through activation of vascular smooth muscle ET-A specific receptors and acts through endothelial ET-B receptors to stimulate production of NO to oppose vasoconstriction (Haynes and Webb 1998; Cardillo et al. 2000, 2009). Because aging is associated with reduced nitric oxide action, the vasoconstriction effect of ET-1 on smooth muscle receptors may remain unopposed (Donato et al. 2009; Padilla et al. 2011; Seals et al. 2011; Thorin and Webb 2010). Donato et al. (2009) found that changes in ET-1 expression, production and bioactivity contribute to vascular endothelial dysfunction with age. In addition to direct action on vascular system, ET-1 alters central and peripheral sympathetic activity (Bruno et al. 2011) and stimulates the renin–agiotensin–aldosterone system (Miller et al.1989). Mishima et al. (2001) found that ET-1 stimulates ADM production from cultured rat cardiomyocytes and augments intracellular cAMP accumulation with upregulation of the RAMP3 mRNA expression. This suggests the possibility of local interaction between ADM and ET-1. The site and the stimulus for ADM secretion during exercise remain unclear. The findings obtained in rats showing that stress evoked by acute restraint (Khan et al. 1999) or cold exposure (Yűksel et al. 2002), known to increase markedly sympathetic nervous system activity, stimulates also ADM secretion. This suggests that stimulation of ADM release may depend on the effect of catecholamines on the secretory cells. The present study showing the correlations between exercise-induced changes in plasma NA and ADM and between changes in plasma ET-1 and those of ADM in older men supports both these mechanisms. However, the plasma ADM release from vascular endothelium during handgrip may be induced by acute BP increase and subsequent shear stress.
The inverse relationships between exercise-induced changes in PEP, PEP/LVET ratio, SV, TPR and those of plasma ADM shown in this study confirmed the data obtained in our previous investigations performed in patients with heart failure (Krzeminski et al. 2009). The relationship between ADM and PEP/LVET ratio may be at least partly associated with inotropic action of ADM on the heart. Based on previous studies (Szokodi et al. 1998; Evans 1986), it may be speculated that this inotropic action is due to activation of adenylate cyclase and cyclic AMP production in cardiomyocytes by ADM. Thus, it seems likely that ADM acts to increase left ventricular function during static exercise by both decrease in systemic vascular resistance and an increase in myocardial contractility. Charles et al. (1997, 2000, 2003) have reported significant hemodynamic and hormonal actions of ADM including reduction of peripheral vascular resistance and arterial pressure, attenuation of angiotensin II-induced rise in blood pressure, as well as a direct inhibitory action on aldosterone secretion from the adrenal glomerulosa. The authors found that ADM acts rather as a functional antagonist to angiotensin II than to norepinephrine, and that the adrenoceptor-mediated vasoconstriction fully overwhelms the vasodilator effects of ADM. It has been shown that ADM increases NO production by stimulation of adenylate cyclase and inducible endothelial NO syntase (eNOS) and potentiates interleukin-1 (Hattori et al. 1999; Zhang and Hintze 2001). Furthermore, in some tissues ADM can act by both NO-dependent and K+ channel-dependent mechanisms (Terata et al. 2000; Sabates et al. 1997). However, there is a variety of mechanisms by which ADM may induce vascular relaxation, with the major pathway mediated by either calcitonin gene-related peptide (CGRP) or ADM-selective receptors directly (Martínez-Alvarez et al. 2008; Fukai and Hirata 2004; Huang et al. 1999).
It should be noted that the values of plasma concentration of ADM achieved during static exercise by the older subjects were within the normal resting range, which was reported to be as wide as 1.1–10 pmol l−1 (Hinson et al. 2000). We assumed, however, that ADM might play a role in the cardiovascular responses to static exercise since the significant inverse relationships between ΔADM and ΔTPR, ΔSV or ΔPEP/LVET ratio were ascertained.
In the present study, after 5 min of the recovery period, plasma ADM concentration returned to the pre-exercise values. This does not corroborate the data of Meeran et al. (1997), who demonstrated that the plasma half-life of ADM was as long as 22 ± 1.6 min. However, this value was obtained when a high dose of the exogenous hormone was given and the very high plasma concentration was achieved. It is not certain whether the rate of disappearance of ADM from plasma is similar with the relatively small changes in the endogenous hormone concentration, especially in the presence of acute hemodynamic changes.
Additional finding of the present investigation is that in older men the increase in PRA occurred at the end of static exercise. This is in agreement with the previous data showing that static handgrip at the 30% level of maximal voluntary contraction for 4 min induced a significant increase in PRA in both normotensive and hypertensive subjects (Uchida et al. 1978). Since pretreatment with propranolol abolished this response, it is concluded that isometric handgrip can induce an augmentation in renin release mainly by stimulation of the sympathetic nervous system. The data obtained by Jindra et al. (1990) in men exercising on bicycle ergometer further emphasized the relationship between the sympathetic adrenomedullary and renin–angiotensin systems during acute stimulation. Also, our results on the relationships between plasma catecholamine and PRA increases in the group of older subjects indicate the role of sympathetic activity on PRA response. It is, however, unclear why PRA did not rise during handgrip in young subjects. In this regard, it seems worth mentioning the study of Laitinen et al. (1998), who have found that healthy older men (>60 years old) had markedly depressed baroreflex sensitivity (BRS) and that there was a significant positive correlation between BRS and PRA. On the other hand, the increase in PRA may be related to ADM action as a consequence of its renal vasodilatory effect or by release of cyclic AMP stimulating the juxtaglomerular cells.
One of the limitations of this study is that we have only two age groups of subjects. A larger population incorporating a wide spectrum of age is needed to analyze the relationships between age and cardiovascular or hormonal response to handgrip and to state the unique role of ADM in maintaining the vascular tone in different stages of the life. Nitric oxide was not determined, although changes in its availability and reactivity to its action occur with age (Donato et al. 2009) and may play a role in blood pressure response to exercise.
In summary, this study demonstrated that handgrip-induced increases in HR and cardiac output were significantly smaller in older than in young men. Stroke volume decreased and PEP to LVET ratio increased during handgrip only in older men. Total peripheral resistance was higher in older men, while increases in BP were similar in both groups of subjects.
The most important finding is that handgrip caused increases in plasma ADM, ET-1 and PRA only in the older men. These results suggest that ADM, ET-1 and angiotensin II with their opposite vasoactive properties can contribute to maintain vascular tone during static exercise in the older men. The baseline plasma ADM and catecholamines concentrations were higher in older man compared to young subjects.
References
Boutcher SH, Stocker D (1999) Cardiovascular responses to light isometric and aerobic exercise in 21- and 59-year old males. Eur J Appl Physiol Occup Physiol 80:220–226
Bruno RM, Sudano I, Ghiadoni L, Masi L, Taddei S (2011) Interactions between sympathetic nervous system and endogenous endothelin in patients with essential hypertension. Hypertension 57:79–84
Cardillo C, Kilcoyne CM, Cannon RO, Panza JA (2000) Interactions between nitric oxide and endothelin in the regulation of vascular tone of human resistance vessels in vivo. Hypertension 35:1237–1241
Cardillo C, Schinzari F, Melina D et al (2009) Improved endothelial function after endothelin receptor blockade in patients with systemic sclerosis. Arthritis Rheum 60:1840–1844
Charles CJ, Rademaker MT, Richards AM et al (1997) Hemodynamic, hormonal, and renal effects of adrenomedullin in conscious sheep. Am J Physiol 272:R2040–R2047
Charles CJ, Rademaker MT, Richards AM, Cooper GJ, Coy DH, Nicholls MG (2000) Adrenomedullin attenuates pressor response to angiotensin II in conscious sheep. J Cardiovasc Pharmacol 36:526–532
Charles CJ, Lainchbury JG, Nicholls MG, Rademaker MT, Richards AM, Troughton RW (2003) Adrenomedullin and the renin–angiotensin–aldosterone system. Regul Pept 112:41–49
Cottone S, Vella MC, Vadalà A, Neri AL, Riccobene R, Cerasola G (1998) Influence of vascular load on plasma endothelin-1, cytokines and catecholamine levels in essential hypertensives. Blood Press 7:144–148
Cybulski G (1988) Computer method for automatic determination of stroke volume using impedance cardiography signals. Acta Physiol Pol 39:494–503
Cybulski G, Miskiewicz Z, Szulc J, Torbicki A, Pasierski T (1993) A comparison between the automatized impedance cardiography and pulsed-wave Doppler echocardiography methods for measurements of stroke volume (SV) and systolic time intervals (STI). J Physiol Pharmacol 44:251–258
Donato AJ, Gano LB, Eskurza I, Silver AE, Gatek PE, Jablonski K, Seals DR (2009) Vascular endothelial dysfunction with aging: endothelin-1 and endothelial nitric oxide synthase. Am J Pysiol Heart Circ Physiol 297:H425–H432
Esler MD, Thompson JM, Kaye DM et al (1995) Effects of aging on the responsiveness of the human cardiac sympathetic nerves to stressors. Circulation 91:351–358
Evans DB (1986) Modulation of cAMP: mechanism for positive inotropic action. J Cardiovasc Pharmacol 8:S22–S29
Ferrari AU (2002) Modifications of the cardiovascular system with aging. Am J Geriatr Cardiol 11:30–33
Ferrari AU, Radaelli A, Centola M (2003) Aging and the cardiovascular system. J Appl Physiol 95:2591–2597
Fukai N, Hirata Y (2004) Adrenomedullin receptor and its signal transduction. Nippon Rinsho 62(9):189–192
Haskell WL, Savin WM, Schroeder JS et al (1981) Cardiovascular responses to handgrip isometric exercise in patients following cardiac transplantation. Circ Res 48:156–161
Hattori Y, Nakanishi N, Gross SS, Kasai K (1999) Adrenomedullin augments nitric oxide and tetrahydrobioptein synthesis in cytokine-stimulated vascular smooth muscle cells. Cardiovasc Res 44:207–214
Haynes WG, Webb DJ (1998) Endothelin as a regulator of cardiovascular function in health and disease. J Hypertens 16:1081–1098
Hinson JP, Kapas S, Smith DM (2000) Adrenomedullin, a multifunctional regulatory peptide. Endocr Rev 21:138–167
Housiiere A, Najem B, Pathak A, Xhaet O, Naeije R, Van De Borne P (2006) Chemoreflex and metaboreflex responses to static hypoxic exercise in aging humans. Med Sci Sports Exerc 38:305–312
Huang MH, Knight PR III, Izzo JL Jr (1999) Ca2+-induced Ca2+ release involved in positive inotropic effect mediated by CGRP in ventricular myocytes. Am J Physiol Regul Integr Comp Physiol 276:R259–R264
Jindra A Jr, Savliková J, Bultas J (1990) Relationship between plasma catecholamines and the renin–aldosterone system during exercise in normal and essential hypertensive subjects. Clin Exp Hypertens 12:415–435
Kato J, Kitamura K, Uemura T, Kuwasko K, Kita T, Kangawa K, Eto T (2002) Plasma levels of adrenomedullin and atrial and brain natriuretic peptides in the general population: their relations to age and pulse pressure. Hypertens Res 25:887–892
Khan S, Michaud D, Moody TW, Anisman H, Merali Z (1999) Effects of acute restraint stress on endogenous adrenomedullin levels. NeuroReport 10:2829–2833
Kino M, Lance VQ, Spodick DH (1975) Effects of age on responses to isometric exercise Isometric handgrip in noninvasive screening for cardiovascular disease. Am Heart J 90:575–581
Kita T, Kitamura K, Hashida S, Morishita K, Eto T (2003) Plasma adrenomedullin is closely correlated with pulse wave velocity in middle-aged and elderly patients. Hypertens Res 26:887–893
Krzeminski K, Kruk B, Wojcik-Ziolkowska E, Kozera J, Cybulski G, Nazar K (2002) Effect of static handgrip on plasma adrenomedullin concentration in patients with heart failure and in healthy subjects. J Physiol Pharmacol 53:199–210
Krzeminski K, Nazar K, Cybulski G, Mikulski T (2006) Effect of adrenergic blockade on plasma adrenomedullin concentration during static handgrip in patients with heart failure. Clin Physiol Funct Imaging 26:328–334
Krzeminski K, Cybulski G, Nazar K (2009) Relationships between plasma adrenomedullin concentration and systolic time intervals during static handgrip in patients with heart failure. Clin Physiol Funct Imaging 29:114–122
Laitinen T, Hartikainen J, Vanninen E, Niskanen L, Geelen G, Länsimies E (1998) Age and gender dependency of baroreflex sensitivity in healthy subjects. J Appl Physiol 84:576–583
Lakatta EG (2002) Age-associated cardiovascular changes in health: impact on cardiovascular disease in older persons. Heart Fail Rev 7(1):29–49
Levi GF, Ratti S, Cardone G, Basagni M (1982) On the reliability of systolic time intervals. Cardiology 69:157–165
Lind AR (1970) Cardiovascular responses to static exercise. Circulation 41:173–176
Lind AR, Taylor SH, Humphreys PW, Kenelly BM, Donald KW (1964) Circulatory effects of sustained voluntary muscle contractions. Clin Sci 27:229–244
Mangieri E, Tanzilli G, Barillà F et al (1997) Isometric handgrip exercise increases endothelin-1 plasma levels in patients with chronic congestive heart failure. Am J Cardiol 79:1261–1263
Mangieri E, Tanzilli G, Barillà F et al (1998) Handgrip increases endothelin-1 secretion in normotensive young male offspring of hypertensive parents. J Am Coll Cardiol 31:1362–1366
Markel TA, Daley JC, Hogeman CS et al (2003) Aging and the exercise pressor reflex in humans. Circulation 107:675–678
Martin CE, Shaver JA, Thompson ME, Reddy PS, Leonard JJ (1971) Direct correlation of external systolic time intervals with internal indices of left ventricular function in man. Circulation 44:419
Martin CE, Shaver JA, Leon DF, Thompson ME, Reddy PS, Leonard JJ (1974) Autonomic mechanisms in hemodynamic responses to isometric exercise. J Clin Invest 54:104–115
Martínez-Alvarez RM, Volkoff H, Cueto JA, Delgado MJ (2008) Molecular characterization of calcitonin gene-related peptide (CGRP) related peptides (CGRP, amylin, adrenomedullin and adrenomedullin-2/intermedin) in goldfish (Carassius auratus): cloning and distribution. Peptides 29:1534–1543
Meeran K, O’Shea D, Upton PD et al (1997) Circulating adrenomedullin does not regulate systemic blood pressure but increases plasma prolactin after intravenous infusion in humans: a pharmacokinetic study. J Clin Endocrinol Metab 82:95–100
Miller WL, Redfield MM, Burnett JC Jr (1989) Integrated cardiac, renal, and endocrine actions of endothelin. J Clin Invest 83:317–320
Mishima K, Kato J, Kuwasako K, Ito K, Imamura T, Kitamura K, Eto T (2001) Effects of endothelin on adrenomedullin secretion and expression of adrenomedullin receptors in rat cardiomyocytes. Biochem Biophys Res Commun 287:264–269
Nazar K, Jezova D, Kowalik-Borówka E (1989) Plasma vasopressin, growth hormone and ACTH responses to static handgrip in healthy subjects. Eur J Appl Physiol 58:400–404
Padilla J, Simmons GH, Fadel PJ, Laughlin MH, Joyner MJ, Casey DP (2011) Impact of aging on conduit artery retrograde and oscillatory shear at rest and during exercise: role of nitric oxide. Hypertension 57:484–489
Palmer GJ, Ziegler MG, Lake CR (1978) Response of norepinephrine and blood pressure to stress increases with age. J Gerontol 33:482–487
Petrofsky JS, Lind AR (1975) Aging, isometric strength and endurance, and cardiovascular responses to static effort. J Appl Physiol 38:91–95
Pigott VM, Spodick DH, Rectra EH, Khan AH (1971) Cardiocirculatory responses to exercise: physiologic study by noninvasive techniques. Am Heart J 82:632–636
Sabates BL, Pigott JD, Choe EU et al (1997) Adrenomedullin mediates coronary vasodilation through adenosine receptors and KATP channels. J Surg Res 67:163–168
Sachs C, Hamberger B, Kaijser L (1985) Cardiovascular responses and plasma catecholamines in old age. Clin Physiol 5:553–565
Scherrer U, Pryor SL, Bertocci LA, Victor RG (1990) Arterial baroreflex buffering of sympathetic activation during exercise-induced elevations in arterial pressure. J Clin Invest 86:1855–1861
Seals DR, Esler MD (2000) Human ageing and the sympathoadrenal system. J Physiol 528:407–417
Seals DR, Jablonski KL, Donato AJ (2011) Aging and vascular endothelial function in humans. Clin Sci Lond 120:357–375
Shepherd JT, Blomqvist GB, Lind AR, Mithell JH, Saltin B (1981) Static (isometric) exercise. Supp. I. Circ Res 48(I):179–188
Sowers JR, Rubenstein LZ, Stern N (1983) Plasma norepinephrine responses to posture and isometric exercise increase with age in the absence of obesity. J Gerontol 38:315–317
Spodick DH, Quarry-Pigott VM (1973) Effects of posture on exercise performance; measurement by systolic time intervals. Circulation 48:74
Szokodi I, Kinnunen P, Tavi P, Weckström M, Toth M, Ruskoaho H (1998) Evidence for cAMP-independent mechanisms mediating the effects of adrenomedullin, a new inotropic peptide. Circulation 97:1062–1070
Taylor JA, Hand GA, Johnson DG, Seals DR (1991) Sympathoadrenal-circulatory regulation during sustained isometric exercise in young and older men. Am J Physiol 261:R1061–R1069
Terata K, Miura H, Liu Y, Loberiza F, Gutterman DD (2000) Human coronary arteriolar dilation to adrenomedullin: role of nitric oxide and K+ channels. Am J Physiol Heart Circ Physiol 279:H2620–H2626
Thijssen DHJ, Rongen GA, Dijk A, Smits P, Hopman MTE (2007) Enhanced endothelin-1 mediated leg vascular tone in healthy older subjects. J Appl Physiol 103:852–857
Thorin E, Webb DJ (2010) Endothelium-derived endothelin-1. Pflugers Arch 459:951–958
Uchida K, Yamamoto I, Ishise S, Morimoto S, Takeda R (1978) Plasma renin activity response to isometric handgrip exercise in normotensive and hypertensive. Nippon Naibunpi Gakkai Zasshi 54:752–758
Warner TD (1999) Relationships between the endothelin and nitric oxide pathways. Clin Exp Pharmacol Physiol 26:247–252
Weissler AM (1972) Resting and exercise systolic time intervals. Circulation 46:633
Weissler AM, Harris WS, Schoenfeld CD (1969) Bedside techniques for the evaluation of ventricular function in man. Am J Cardiol 23:577
Whitsett TL, Naughton J (1971) The effect of exercise on systolic time intervals in sedentary and active individuals and rehabilitated patients with heart disease. Am J Cardiol 27:352
Yűksel S, Akbay A, Yűrekli M (2002) Contribution of adrenomedullin to homeostatic response to cold stress in rat model. Pathophysiology 8:243–247
Zhang X, Hintze TH (2001) C-AMP signal transduction cascade, a novel pathway for the regulation of endothelial nitric oxide production in coronary blood vessels. Arterioscler Thromb Vasc Biol 21:797–803
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Niels H. Secher.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Krzemiński, K., Cybulski, G., Ziemba, A. et al. Cardiovascular and hormonal responses to static handgrip in young and older healthy men. Eur J Appl Physiol 112, 1315–1325 (2012). https://doi.org/10.1007/s00421-011-2069-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-011-2069-y