
Abstract
Purpose
The physical activity paradox states occupational physical activity (OPA) to be hazardous and leisure time physical activity (LTPA) to be beneficial for health. Yet, the acute effects of OPA and LTPA on cardiovascular risk factors are sparsely investigated. The aim of this study was to investigate the acute effects on ambulatory blood pressure (ABP) from steps/hour during work and leisure time among cleaners.
Methods
Data were obtained from a cluster randomized worksite intervention among 91 cleaners in Denmark and included a questionnaire, objective physical measurements, ABP (measured across 24 h), and steps/hour (measured during work and leisure time). A preliminary linear regression analysis was conducted as a mixed model including random intercept and slope, allowing for both within- and between-participant variability. We adjusted for sex, age, job seniority, medication use, smoking, self-reported fitness and BMI. Changes in ABP (mmHg) were estimated per 100 steps/hour.
Results
The number of steps taken was not associated with ABP during either work or leisure. Moreover, the ABP did not seem to differ between exposure to steps taken during work (systolic − 0.42 mmHg, 95% Confidence Interval (CI): − 1.10–0.25, diastolic − 0.03 mmHg, 95% CI, − 0.45–0.39) and leisure time (systolic -0.47 mmHg, 95% CI, − 1.66–0.72, diastolic 0.25 mmHg, 95% CI, − 0.46–0.97).
Conclusion
Our findings show no significant association between steps/hour and ABP and no contrasting effects between work and leisure time. These mechanisms fostering the divergent results need to be further investigated to improve the understanding of the physical activity paradox.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Previous literature suggests that occupational physical activity (OPA) is hazardous to health while leisure time physical activity (LTPA) has beneficial health effects (Coenen et al. 2018a, b; Holtermann et al. 2018; Li et al. 2013). For example, a review reports that a high level of OPA increases the risk of cardiovascular disease (CVD), whereas high levels of LTPA decrease the CVD risk (Li et al. 2013). These domain-specific differences in health effects of physical activity, known as the physical activity paradox, can partly be explained by higher heart rate during walking at work than during walking in leisure, perhaps indicating extra stimulus at work, which in turn, could contribute to the explanation of the negative effect on health (Coenen et al. 2018a, b). Yet, findings across studies investigating the physical activity paradox are inconsistent (Dalene et al. 2021).
An elevated intensity of OPA, measured as the relative aerobic workload (Karvonen et al. 1957), for several hours each working day, repetitive work, and prolonged static postures can lead to raised blood pressure (BP) (Gupta et al. 2020), and eventually hypertension (Clays et al. 2012). Hypertension is known as the leading preventable risk factor for cardiovascular disease, e.g. myocardial infarction and stroke, and all-cause mortality worldwide (Roth et al. 2018; Stanaway et al. 2018). One way to prevent hypertension is by increasing physical activity (Pedersen and Saltin 2006). As walking is a physical activity accessible to a large proportion of the population worldwide, as well as being independent of skill level and access to equipment (Oja et al. 2018; Saint-Maurice et al. 2020) and has minimal adverse effects (Morris and Hardman 1997), walking has the potential to prevent hypertension across individuals in different contexts.
The majority of research on the association between walking and health has focused on the number of steps per day omitting information on a domain, such as activity during work or leisure hours (Gupta et al. 2020). One study has investigated the effects of walking on BP in different domains, i.e. working and leisure time (Crowley et al. 2021). However, opposite to the physical activity paradox, this study finds a beneficial association between the number of steps, during work, and systolic BP, among blue-collar workers, and no associations among white-collar workers (Crowley et al. 2021). Hence, the mechanisms fostering such divergent effects in the different domains need to be further investigated.
Ambulatory BP (ABP) measurements have been found to be superior to conventional BP (CBP) measurements in predicting cardiovascular events (Hansen et al. 2007), and it has the advantage of possible measurements of BP in different domains (Clays et al. 2012). Thereby, ABP can be measured as an acute response to actual physical activity or body posture. Thus, ABP measurements offer an opportunity to measure BP without the biases of white-coat- and masked hypertension, leading to more accurate and non-biased measurements and diagnostics of patients with suspected hypertension (O’Brien et al. 2013). However, to our knowledge, no previous study has used this method to investigate the domain-specific effects of steps/hour. Furthermore, examining the acute impact of steps on ABP instead of separating measurements of steps and BP might lead to more precise results on the domain-specific effects of steps on ABP (Hansen et al. 2007). Therefore, the aim of this study was to investigate the association between time-synchronized ABP and the number of steps during work and leisure time among cleaners in Denmark.
Methods
Data were obtained from baseline measures and subsequent technical diurnal measurements from a cluster randomized worksite intervention among cleaners. The study was approved by the Danish Data Protection Agency and the Ethics Committee for the regional capital in Denmark (journal number H-2–2011-116) and was conducted in accordance with the Helsinki Declaration. The study was registered as ISRCTN86682076 in the current controlled trials (2014) and is described in a protocol paper (Korshøj et al. 2012).
Recruitment and participants
Cleaning companies in the suburban area of Copenhagen, Denmark were recruited by direct contact. All cleaning employees were invited to an information meeting where the project was described and assignment to voluntary participation was conducted via a screening questionnaire. A detailed recruitment procedure is described elsewhere (Korshøj et al. 2015). Participants were included if they were: employed as a cleaner ≥ 20 h/week, between 18 and 65 years of age, non-pregnant, and if they had signed an informed consent to participate in the study.
Data collection
Data were collected at a baseline test and subsequently through technical diurnal measurements of ABP and steps/hour during work and leisure time within a maximum of four continuous days. The baseline test consisted of a structured interview, where information on sex, age, job seniority, medication use, smoking, and self-reported cardiorespiratory fitness were obtained. Moreover, the baseline test included objective physical measurements (body weight (Tanita BC418), height (seca model 213 1,721,009) and body mass index (BMI) = [body weight (kg)/body height (m2)] (Canoy 2008)), and BP measured on the left upper arm after 15 min of sitting at rest (Omron M6 comfort) (Korshøj et al. 2012). Technical diurnal measurements of ABP and steps/hour were processed in a custom-made software (Acti4) to synchronize time and domain (Skotte et al. 2014).
Ambulatory blood pressure measurements
ABP measurements were performed with Spacelabs90217 (www.spacelabshealthcare.com) (Baumgart & Kamp 1998), by oscillometry, mounted on the non-dominant upper arm with a tube connecting the sampler to the cuff. The data sampler was mounted with elastic straps around the waist, and the frequency of measurements was every 20 min during waking hours and every 40 min during sleep (Clays et al. 2007, 2012). The participants were instructed to keep still and the arm at rest while the measurement was proceeding. If a measurement failed, the monitor automatically repeated the measure again a few minutes later. The participants were asked to wear the monitors 24 h/day on a day including work. They were instructed on how to treat the monitors and to remove the ABP device during showering. The 24-h recording was performed on the first or second day of the four days where steps/hour were measured. Furthermore, the 24-h recording was split into periods classified as work, leisure or sleep based on information from self-reported dairies where the participants were asked to write a log of working hours (when they started and ended work), sleeping time (got up in the morning and went to bed in the evening) and periods spent without monitors. ABP measurements were included when a minimum of 25% of measurements were complete (corresponding to the amount of measurements: five during work, eight during leisure and three during sleep), and all measures of ABP were visually checked and physiological outliers were excluded from analysis (systolic blood pressure < 80 and > 240 mmHg, diastolic blood pressure < 50 and > 130 mmHg) (Korshøj et al. 2016).
Measurements of the number of steps
The number of steps was sampled by Actigraph GT3X + , a triaxial accelerometer, with a dynamic range of ± 6 G, sampled with the precision of 12 bit. The Acti4 software was used to process raw data and estimate time spent in different body positions and activities (Skotte et al. 2014; Stemland et al. 2015). The accelerometers were initialized for recording and data were downloaded using the manufacturer’s software (ActiLife version 5.5). Actigraphs were mounted on the skin with adhesive tape on the right thigh at the most muscular part of the quadriceps femoris, medial to the front of the iliac crest and the top of the patella, orientated with the x-axis pointing downwards, y-axis horizontally to the left and z-axis horizontally forward (Skotte et al. 2014). The Actigraph signals were sampled at 30 Hz to derive the number of steps.
Assessments of potential confounders
The selection of covariates (potential confounders) was based on prior related studies and findings in the literature (Coenen et al. 2018a, b; Coenen et al. 2018a, b; Kjeldsen 2018; Kodama 2009; Merellano-Navarro et al. 2017; Reckelhoff 2001), e.g. associations between BP and age have previously been found (Kjeldsen 2018), and other findings show age to associate with physical fitness performance, such as walking (Merellano-Navarro et al. 2017). Furthermore, sex differences in BP (Reckelhoff 2001) as well as walking (Allen and Vella 2015; Pollard and Wagnild 2017) have been observed. Additionally, it is well-established that drug therapy is associated with BP control (Williams et al. 2018). Also, smoking has been associated with BP (Virdis et al. 2010) as well as walking (Allen and Vella 2015). Cardiorespiratory fitness has previously been associated with cardiovascular events (Kodama 2009) and BP (Cornelissen and Smart 2013). Previous findings, however, also indicate that cardiorespiratory fitness moderates the association between OPA and ischemic heart disease (Holtermann et al. 2010). Therefore, cardiorespiratory fitness was included first as a confounder and later as a moderator in our analyses.
Participants were asked to indicate their sex, date of birth, for estimation of age, and the number of years they had had their current job type, for estimation of job seniority. In this study, participants were asked if they within the past four weeks had used any medication prescribed by a doctor, i.e. cholesterol-lowering drugs, diuretics, antihypertensives, antidepressants, pain killers and/or others (response options: yes or no). Participants were asked: “Do you smoke?” (response options: 1) yes, on a daily basis; 2) yes, sometimes; 3) I have previously smoked, but not anymore and 4) I have never smoked). Smoking responses were dichotomized into yes; yes, sometimes and no, never, previously. To measure self-reported cardiorespiratory fitness, the participants were asked: “How would you perceive your fitness compared to other people in your age group and the same sex as you?” The participants could range their level on a scale from 1 to 10; with 1 representing poor and 10 representing good (Strøyer et al. 2007). Fitness was also objectively measured by a step test (Aadahl et al. 2013). However, self-reported cardiorespiratory fitness was chosen over objectively measured cardiorespiratory fitness to ensure a higher number of participants to be included in the analysis. To test if self-reported cardiorespiratory fitness corresponded to the actual level of the participants’ objectively measured cardiorespiratory fitness, the normal distribution curves of each variable were assessed and concluded to be comparable.
Statistical analysis
IBM SPSS software version 27.0 was used for all statistical analyses. The distribution of step data and ABP were checked and considered normally distributed. The remaining continuous variables (age, BMI, job seniority, self-reported cardiorespiratory fitness) were likewise checked and considered normally distributed.
Descriptive analyses of baseline characteristics were performed (Table 1). The number of participants and percentage distribution were reported for categorical variables and means, and Standard Division (SD) were calculated for the continuous variables.
As we included repeated measurements of the (continuous) dependent outcome variables for all participants, a linear regression analysis was conducted as a mixed model including random intercept and random slope, allowing for both within-participant and between-participant variability. For exposure variables (steps/hour) we calculated the mean values for work hours and leisure time, respectively. Changes in ABP (mmHg) were estimated as an increase/decrease in APB per 100 steps/hour. Independent exposure variables were included as continuous variables in all analyses. Missing measurements were not imputed (Twisk et al. 2013). To avoid unnecessary adjustment, covariates were included stepwise in the analyses. First, we conducted a raw model (Model 1, Table 2) with no adjustments. Second, we adjusted for demographic characteristics, i.e. sex, age, and job seniority (Model 2, Table 2). Next, we adjusted for behavioral factors, i.e. use of medicine, smoking habits, self-reported cardiorespiratory fitness, and BMI (Model 3, Table 2).
In the sensitivity analyses, we repeated Model 3 with the inclusion of a multiplicative interaction term (steps/hour x self-reported cardiorespiratory fitness) to capture the potential moderating effect of cardiorespiratory fitness on the association between steps/hour and ABP during working hours and leisure time, respectively.
Results
Study population and baseline characteristics
All of the three contacted companies in the suburban area of Copenhagen, Denmark, agreed to participate. The study was presented to 250 cleaning assistants at these companies. Of those, 137 (45%) agreed to participate and 116 underwent the baseline measurements. In total, 96 participants had an ABP monitor mounted (23 male and 73 female), and 91 participants had a sufficient number of ABP measurements to be included in the statistical analysis (Fig. 1).

Flowchart of inclusion and exclusion of participants in the study on the association between steps/hour and ambulatory blood pressure (ABP) among cleaners in Denmark during working hours and leisure time, respectively
In total, 75.8% of participants were women, 13.2% used medication and 25.3% smoked (Table 1). The mean age for all participants was 45.4 years (SD ± 8.2), the mean BMI was 27.0 kg/m2 (SD ± 4.6), mean job seniority was 12.2 years (SD ± 7.7), and participants on average perceived their cardiorespiratory fitness level as moderate (mean = 5.1, SD ± 1.96) compared to peers. Mean steps/hour were 1332.6 (SD ± 404.1) during work and 526.0 (SD ± 234.1) during leisure time. The systolic BP was 123.3 mmHg (SD ± 20.8) and the mean diastolic BP was 83.1 mmHg (SD ± 12.1) at baseline (Table 1).
The effect of steps/hour on ABP at work and in leisure time
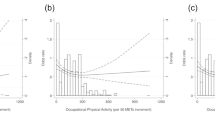
The analyses showed no associations between ABP and steps/hour in work and leisure time. The ABP did not seem to differ by the domain of the exposure to steps; during work (systolic − 0.42 mmHg/100 steps/hour, 95% CI: − 1.10–0.25, diastolic -0.03 mmHg/100 steps/hour, 95% CI, − 0.45–0.39) and leisure (systolic -0.47 mmHg/100 steps/hour, 95% CI, − 1.66–0.72, diastolic 0.25 mmHg/100 steps/hour, 95% CI, − 0.46–0.97) (Model 3, Table 2).
Sensitivity analysis
The sensitivity analyses did not show self-reported cardiorespiratory fitness to moderate the association between steps/hours during work hours and the systolic or diastolic ABP. Neither did fitness level moderate the association between steps/hours in leisure time and the diastolic ABP. However, we cannot rule out the possibility that cardiorespiratory fitness moderates the association between steps/hour in leisure time and the systolic ABP on an 80% significance level (p = 0.132) (Krause et al. 2017). A complementary analysis stratified by cardiorespiratory fitness level above/below the median (i.e. 5.00) was therefore conducted. However, when stratified on fitness level, we found no statistically significant changes in the estimate, thus, these analyses did not change our overall conclusion and are therefore not presented in detail.
Discussion
Comparison with previous findings
The literature describing the associations between physical activity and CVD is inconsistent, and it has been convincingly argued that more research that differentiates between the role of physical activity during work vs. leisure time for CVD is needed (Krause 2010). Moreover, there is evidence that daytime ABP monitoring is superior to CBP measurement in the prediction of CVD, however, studies that include such ABP measurements are lacking (Hansen et al. 2007). This study examined the association between the domain-specific number of steps/hour and time-synchronized ABP among 91 cleaners in Denmark. Thus, to our knowledge, this study is the first one investigating the acute effect of steps on BP, and a direct comparison with previous studies may not be possible.
The main findings of this study are that there were no significant effects of the number of steps on the ABP as well as no contrasting effects between work and leisure time in the associations of ABP and steps/hour. Thus, we did not find any adverse health effects of OPA, nor any beneficial health effect of LTPA, which is distinct from the physical activity paradox advocating that LTPA promotes health, while high OPA impairs health (Gupta et al. 2020; Holtermann et al. 2012). Previously, Johansson et al. (2022) reported that reallocating time from being sedentary to walking, during leisure, was beneficial for BP, whereas during work, it was harmful for BP. Also, the results from our study could not support the previously shown association between steps/hour during work and a lowered CBP (Crowley et al. 2021) during neither work nor leisure time. Additionally, our findings are opposite to a number of previous studies showing harmful effects of self-reported OPA, such as lifting and carrying loads, on the CBP (Allesøe et al. 2016; Virkkunen et al. 2007; Åstrand et al. 2003), as well as the ABP (Clays et al. 2012). But, similarly to our results, Clays et al. (2012) found no associations between objectively measured OPA and ABP. Holtermann et al. (2018) introduced six reasons for the physical activity paradox; one being that the intensity of OPA does not reach a level where individuals will gain cardiorespiratory fitness. Other explanations for the effects of OPA included insufficient time for recovery, long durations, and static and constrained postures and activities (Holtermann et al. 2018). Considering the contrasting results regarding the effects of OPA on BP with respect to the work of Holtermann et al. (2018), one explanation for not finding an association between steps/hour and ABP could be that different types of OPA, such as steps vs. heavy lifting, have different effects on the cardiovascular system and thus the BP.
Our study did not find a significant association between the number of steps at leisure and ABP, i.e. ABP did not decrease significantly with a greater number of steps taken during LTPA. In the same way, the study by Crowley et al. (2021) showed no statistically significant association between the number of steps during leisure and systolic BP (Crowley et al. 2021). These results are in contrast to previous findings of LTPA having a protective effect on health (Clays et al. 2012; Saint-Maurice et al. 2019) and being associated with a reduced risk of CVD (Holtermann et al. 2021). More research on the domain-specific acute effects of different physical activities, in particular steps/hour, would shed light on this.
The combination of high physical work demands and low cardiorespiratory fitness has been associated with increased risk for cardiovascular disease mortality (Holtermann et al. 2021). This is important knowledge considering the fact that cleaners often experience high physical work demands (Korshøj et al. 2012), and therefore are at risk of overload or damage to the cardiovascular system (Holtermann et al. 2009). In this study, we could not rule out the possibility of cardiorespiratory fitness level to moderate the association between steps/hour during leisure time and the systolic ABP, which somehow indicates that fitness level may protect against or worsen the effects of OPA on risk factors for CVD, such as increased ABP. However, when stratified on cardiorespiratory fitness level, we found no statistically significant results. Thus, whether the number of steps during work hours is beneficial or harmful to cleaners’ cardiovascular health and whether the cardiorespiratory fitness level moderates the effect of steps, cannot be concluded from this study.
Strengths and limitations
This study is strengthened by the use of objective measurements of steps/hour, ABP, and BMI among cleaners, which decreases the risk of subjective recall bias. Furthermore, this study was strengthened by technical diurnal measurements ABP measurements, previously found to be a stronger predictor for cardiovascular disease than CBP measurements (Hansen et al. 2007). ABP measurements that are time-synchronized to step counts, seem to be a reliable method to measure the acute effect of steps/hour on the ABP. However, cleaning also involves several physically demanding tasks that increase the risk of high BP (Korshøj et al. 2012). Thus, the associations we investigated in this study might have been biased by the exposure of other risk factors for high BP, such as high relative aerobic workload (Korshøj et al. 2015).
To minimize the risk of bias the analyses were adjusted for several confounders, however, we cannot preclude that our findings may have been affected by unmeasured confounding. Moreover, a limitation of this study may be, that we chose to adjust the analyses for self-reported cardiorespiratory fitness level and not objectively measured fitness, to include more participants in the analyses. The drawback of this is that we may have increased the risk of recall bias on this specific topic. However, by comparing the normal distribution curves for objective and self-reported cardiorespiratory fitness we found that the two measurements were comparable. Additionally, self-reported fitness has previously been identified as a strong independent predictor of risk factors of CVD and all-cause mortality (Holtermann et al. 2015). Thus, it is likely that self-reported fitness did not introduce a bias in our study.
Conclusion
In conclusion, this study among cleaners in Denmark demonstrated no significant association between diurnal time-synchronized steps/hour and ABP, and no contrasting findings of ABP when exposed to walking during work and leisure time. All in all, this study underlines the need to investigate the acute mechanisms contributing to divergent results in studies on the physical activity paradox. This is important to be able to identify and develop preventive initiatives in the future for those workers who actually experience harmful effects from OPA on their cardiovascular health.
Availability of data and material
The data that support the findings of this study are available from Mette Korshøj on reasonable request.
Abbreviations
- ABP:
-
Ambulatory blood pressure
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CBP:
-
Conventional blood pressure
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- LTPA:
-
Leisure time physical activity
- OPA:
-
Occupational physical activity
- SD:
-
Standard division
References
Aadahl M, Zacho M, Linneberg A, Thuesen BH, Jørgensen T (2013) Comparison of the Danish step test and the watt-max test for estimation of maximal oxygen uptake: the Health 2008 study. Eur J Prev Cardiol 20(6):1088–1094. https://doi.org/10.1177/2047487312462825
Allen MS, Vella SA (2015) Longitudinal determinants of walking, moderate, and vigorous physical activity in Australian adults. Prev Med 78:101–104. https://doi.org/10.1016/j.ypmed.2015.07.014
Allesøe K, Søgaard K, Aadahl M, Boyle E, Holtermann A (2016) Are hypertensive women at additional risk of ischaemic heart disease from physically demanding work? Eur J Prev Cardiol 23(10):1054–1061. https://doi.org/10.1177/2047487316631681
Åstrand P-O, Rodahl K, Dahl HA, Stromme SB. (Red.). (2003). Textbook of Work Physiology: Physiological Bases of Exercise (4. ed). Human Kinetics.
Baumgart P, Kamp J (1998) Accuracy of the SpaceLabs Medical 90217 ambulatory blood pressure monitor. Blood Press Monit 3(5):303–307
Canoy D (2008) Distribution of body fat and risk of coronary heart disease in men and women. Curr Opin Cardiol 23(6):591–598. https://doi.org/10.1097/HCO.0b013e328313133a
Clays E, Leynen F, De Bacquer D, Kornitzer M, Kittel F, Karasek R, De Backer G (2007) High job strain and ambulatory blood pressure in middle-aged men and women from the Belgian Job Stress Study. J Occup Environ Med 49(4):360–367. https://doi.org/10.1097/JOM.0b013e31803b94e2
Clays E, De Bacquer D, Van Herck K, De Backer G, Kittel F, Holtermann A (2012) Occupational and leisure time physical activity in contrasting relation to ambulatory blood pressure. BMC Public Health 12(1):1002. https://doi.org/10.1186/1471-2458-12-1002
Coenen P, Huysmans MA, Holtermann A, Krause N, van Mechelen W, Straker LM, van der Beek AJ (2018a) Do highly physically active workers die early? a systematic review with meta-analysis of data from 193 696 participants. Br J Sports Med 52(20):1320–1326. https://doi.org/10.1136/bjsports-2017-098540
Coenen P, Korshøj M, Hallman DM, Huysmans MA, van der Beek AJ, Straker LM, Holtermann A (2018b) Differences in heart rate reserve of similar physical activities during work and in leisure time—a study among Danish blue-collar workers. Physiol Behav 186:45–51. https://doi.org/10.1016/j.physbeh.2018.01.011
Cornelissen VA, Smart NA (2013) Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc 2(1):e004473. https://doi.org/10.1161/JAHA.112.004473
Crowley P, Gupta N, Vuillerme N, Madeleine P, Holtermann A (2021) Number of steps and systolic blood pressure: Do work and leisure matter? Scand J Med Sci Sports 31(10):1962–1970. https://doi.org/10.1111/sms.14010
Dalene KE, Tarp J, Selmer RM, Ariansen IKH, Nystad W, Coenen P, Anderssen SA, Steene-Johannessen J, Ekelund U (2021) Occupational physical activity and longevity in working men and women in Norway: A prospective cohort study. Lancet Public Health 6(6):e386–e395. https://doi.org/10.1016/S2468-2667(21)00032-3
Gupta N, Dencker-Larsen S, Lund Rasmussen C, McGregor D, Rasmussen CDN, Thorsen SV, Jørgensen MB, Chastin S, Holtermann A (2020) The physical activity paradox revisited: A prospective study on compositional accelerometer data and long-term sickness absence. Int J Behav Nutr Phys Act 17(1):93. https://doi.org/10.1186/s12966-020-00988-7
Hansen TW, Kikuya M, Thijs L, Björklund-Bodegård K, Kuznetsova T, Ohkubo T, Richart T, Torp-Pedersen C, Lind L, Jeppesen J, Ibsen H, Imai Y, Staessen JA (2007) Prognostic superiority of daytime ambulatory over conventional blood pressure in four populations: a meta-analysis of 7030 individuals. J Hypertens 25(8):1554–1564. https://doi.org/10.1097/HJH.0b013e3281c49da5
Holtermann A, Mortensen OS, Burr H, Søgaard K, Gyntelberg F, Suadicani P (2009) The interplay between physical activity at work and during leisure time – risk of ischemic heart disease and all-cause mortality in middle-aged Caucasian men. Scand J Work Environ Health 35(6):466–474. https://doi.org/10.5271/sjweh.1357
Holtermann A, Mortensen OS, Burr H, Søgaard K, Gyntelberg F, Suadicani P (2010) Physical demands at work, physical fitness, and 30-year ischaemic heart disease and all-cause mortality in the Copenhagen Male Study. Scand J Work Environ Health 36(5):357–365. https://doi.org/10.5271/sjweh.2913
Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G (2012) The health paradox of occupational and leisure-time physical activity. Br J Sports Med 46(4):291–295. https://doi.org/10.1136/bjsm.2010.079582
Holtermann A, Marott JL, Gyntelberg F, Søgaard K, Mortensen OS, Prescott E, Schnohr P (2015) Self-reported cardiorespiratory fitness: prediction and classification of risk of cardiovascular disease mortality and longevity—a prospective investigation in the Copenhagen City Heart Study. J Am Heart Assoc 4(1):e001495. https://doi.org/10.1161/JAHA.114.001495
Holtermann A, Krause N, van der Beek AJ, Straker L (2018) The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med 52(3):149–150. https://doi.org/10.1136/bjsports-2017-097965
Holtermann A, Schnohr P, Nordestgaard BG, Marott JL (2021) The physical activity paradox in cardiovascular disease and all-cause mortality: The contemporary Copenhagen General Population Study with 104 046 adults. Eur Heart J 42(15):1499–1511. https://doi.org/10.1093/eurheartj/ehab087
Johansson MS, Holtermann A, Marott JL, Prescott E, Schnohr P, Korshøj M, Søgaard K (2022) The physical activity health paradox and risk factors for cardiovascular disease: a cross-sectional compositional data analysis in the Copenhagen City Heart Study. PLoS ONE 17(4):e0267427. https://doi.org/10.1371/journal.pone.0267427
Karvonen MJ, Kentala E, Mustala O (1957) The effects of training on heart rate: a longitudinal study. Ann Med Exp Biol Fenn 35:307–315
Kjeldsen SE (2018) Hypertension and cardiovascular risk: General aspects. Pharmacol Res 129:95–99. https://doi.org/10.1016/j.phrs.2017.11.003
Kodama S (2009) Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 301(19):2024. https://doi.org/10.1001/jama.2009.681
Korshøj M, Krustrup P, Jørgensen MB, Prescott E, Hansen ÅM, Kristiansen J, Skotte JH, Mortensen OS, Søgaard K, Holtermann A (2012) Cardiorespiratory fitness, cardiovascular workload and risk factors among cleaners; a cluster randomized worksite intervention. BMC Public Health 12(1):645. https://doi.org/10.1186/1471-2458-12-645
Korshøj M, Lidegaard M, Skotte JH, Krustrup P, Krause N, Søgaard K, Holtermann A (2015) Does aerobic exercise improve or impair cardiorespiratory fitness and health among cleaners? a cluster randomized controlled trial. Scand J Work Environ Health 41(2):140–152. https://doi.org/10.5271/sjweh.3475
Korshøj M, Clays E, Lidegaard M, Skotte JH, Holtermann A, Krustrup P, Søgaard K (2016) Is aerobic workload positively related to ambulatory blood pressure? a cross-sectional field study among cleaners. Eur J Appl Physiol 116(1):145–152. https://doi.org/10.1007/s00421-015-3259-9
Krause N (2010) Physical activity and cardiovascular mortality—disentangling the roles of work, fitness, and leisure. Scand J Work Environ Health 36(5):349–355. https://doi.org/10.5271/sjweh.3077
Krause N, Arah OA, Kauhanen J (2017) Physical activity and 22-year all-cause and coronary heart disease mortality. Am J Ind Med 60(11):976–990. https://doi.org/10.1002/ajim.22756
Li J, Loerbroks A, Angerer P (2013) Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr Opin Cardiol 28(5):575–583. https://doi.org/10.1097/HCO.0b013e328364289c
Merellano-Navarro E, Collado-Mateo D, García-Rubio J, Gusi N, Olivares PR (2017) Validity of the International Fitness Scale “IFIS” in older adults. Exp Gerontol 95:77–81. https://doi.org/10.1016/j.exger.2017.05.001
Morris JN, Hardman AE (1997) Walking to health: sports. Medicine 23(5):306–332. https://doi.org/10.2165/00007256-199723050-00004
O’Brien E, Parati G, Stergiou G (2013) Ambulatory blood pressure measurement: what Is the International Consensus? Hypertension 62(6):988–994. https://doi.org/10.1161/HYPERTENSIONAHA.113.02148
Oja P, Kelly P, Murtagh EM, Murphy MH, Foster C, Titze S (2018) Effects of frequency, intensity, duration and volume of walking interventions on CVD risk factors: a systematic review and meta-regression analysis of randomised controlled trials among inactive healthy adults. Br J Sports Med 52(12):769–775. https://doi.org/10.1136/bjsports-2017-098558
Pedersen BK, Saltin B (2006) Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 16(S1):3–63. https://doi.org/10.1111/j.1600-0838.2006.00520.x
Pollard TM, Wagnild JM (2017) Gender differences in walking (for leisure, transport and in total) across adult life: a systematic review. BMC Public Health 17(1):341. https://doi.org/10.1186/s12889-017-4253-4
Reckelhoff JF (2001) Gender differences in the regulation of blood pressure. Hypertension 37(5):1199–1208. https://doi.org/10.1161/01.HYP.37.5.1199
Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, Abdollahpour I, Abdulkader RS, Abebe HT, Abebe M, Abebe Z, Abejie AN, Abera SF, Abil OZ, Abraha HN, Murray CJL (2018) Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159):1736–1788. https://doi.org/10.1016/S0140-6736(18)32203-7
Saint-Maurice PF, Coughlan D, Kelly SP, Keadle SK, Cook MB, Carlson SA, Fulton JE, Matthews CE (2019) Association of leisure-time physical activity across the adult life course with all-cause and cause-specific mortality. JAMA Netw Open 2(3):e190355. https://doi.org/10.1001/jamanetworkopen.2019.0355
Saint-Maurice PF, Troiano RP, Bassett DR, Graubard BI, Carlson SA, Shiroma EJ, Fulton JE, Matthews CE (2020) Association of daily step count and step intensity with mortality among US adults. JAMA 323(12):1151. https://doi.org/10.1001/jama.2020.1382
Skotte J, Korshøj M, Kristiansen J, Hanisch C, Holtermann A (2014) Detection of physical activity types using triaxial accelerometers. J Phys Act Health 11(1):76–84. https://doi.org/10.1123/jpah.2011-0347
Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, Abdollahpour I, Abdulkader RS, Abebe M, Abebe Z, Abera SF, Abil OZ, Abraha HN, Murray CJL (2018) Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392(10159):1923–1994. https://doi.org/10.1016/S0140-6736(18)32225-6
Stemland I, Ingebrigtsen J, Christiansen CS, Jensen BR, Hanisch C, Skotte J, Holtermann A (2015) Validity of the Acti4 method for detection of physical activity types in free-living settings: comparison with video analysis. Ergonomics 58(6):953–965. https://doi.org/10.1080/00140139.2014.998724
Strøyer J, Jensen LD, Avlund K, Essendrop M, Warming S, Schibye B (2007) Validity and reliability of self-assessed physical fitness using visual analogue scales. Percept Mot Skills 104(2):519–533. https://doi.org/10.2466/pms.104.2.519-533
Twisk J, de Boer M, de Vente W, Heymans M (2013) Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J Clin Epidemiol 66(9):1022–1028. https://doi.org/10.1016/j.jclinepi.2013.03.017
Virdis A, Giannarelli C, Fritsch Neves M, Taddei S, Ghiadoni L (2010) Cigarette smoking and hypertension. Curr Pharm Des 16(23):2518–2525. https://doi.org/10.2174/138161210792062920
Virkkunen H, Härmä M, Kauppinen T, Tenkanen L (2007) Shift work, occupational noise and physical workload with ensuing development of blood pressure and their joint effect on the risk of coronary heart disease. Scand J Work Environ Health 33(6):425–434. https://doi.org/10.5271/sjweh.1170
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, De Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Brady A (2018) 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 39(33):3021–3104. https://doi.org/10.1093/eurheartj/ehy339
Acknowledgements
We would like to thank Andreas Holtermann, Karen Søgaard and Peter Krustrup for their valuable support and supervision in the performance of the study.
Funding
Open access funding provided by Zealand Region. The study was funded by The Working Environment Research Fund (journal number 20100019624/5).
Author information
Authors and Affiliations
Contributions
MK conceived the idea, executed the study, collected the data and planned the statistical analysis for this article. VRP processed and analyzed the data, drafted the first version of the manuscript and edited it based on the co-authors´ comments. MB contributed to the interpretation of the results and critical revision of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest relating to the material presented in this article. Its contents, including any opinions and/or conclusions expressed, are solely those of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Poulsen, V.R., Baumann, M. & Korshøj, M. The association between number of steps and the ambulatory blood pressure during leisure vs. work hours among cleaners. Int Arch Occup Environ Health 96, 1373–1381 (2023). https://doi.org/10.1007/s00420-023-02015-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-023-02015-1