
Abstract
Objective
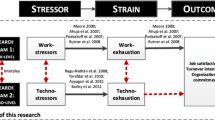
Despite the increasing scholarly interest in the phenomenon technostress, associated biological effects on employee health are under-researched. Chronic low-grade inflammation is suggested as a central pathway linking stress experience to disease development. The aim of this study was to assess associations of technology-related work stressors (technostressors) with low-grade inflammation and burnout symptoms.
Methods
N = 173 (74.6% women, Mage = 31.0 years) university hospital employees participated in a cross-sectional study. Self-report questionnaires were used for the assessment of general psychosocial working conditions (work overload, job control, social climate), a range of different technostressors, burnout symptoms, and relevant confounders. Participants provided capillary blood samples, and high-sensitivity C-reactive protein (hs-CRP) as an inflammatory biomarker was analyzed from dried blood spots.
Results
Based on a factor analysis, we identified four underlying dimensions of technostressors: techno- and information overload, techno-complexity, interruptions and multitasking as well as usability and technical support. In multivariate linear regressions, techno-/information overload and techno-complexity were associated with core (exhaustion, mental distance) and secondary (psychosomatic complaints) symptoms of burnout. Techno-/information overload was a significant predictor of burnout core symptoms, even when general work overload was controlled for. The technostressors were not associated with hs-CRP.
Conclusion
This is the first study on technology-related stress at work and chronic low-grade inflammation. The results suggest that (information) overload caused by digital technology use is a distinct work stressor with genuine consequences for psychological health. To what extent these effects also manifest on a physiological level needs to be subjected to future studies, ideally with prospective designs.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The advancing digitalization has pervasive consequences on the psychosocial work environment and thereby on workers’ health and well-being (Dragano and Lunau 2020; Parker and Grote 2022). These can be negative in terms of stress experience and impaired mental health, but also positive for workers’ health and well-being for instance due to greater flexibility in work organization, better access to information, or automation (Dragano and Lunau 2020; La Torre et al. 2019). Especially in healthcare, there have been fundamental advancements in terms of health information technology (e.g., electronic health records, computerized decision support systems; Abbott and Weinger 2020). At the same time, healthcare professionals are already exposed to a high degree of work stress putting them at an increased risk for adverse health outcomes (Dawe et al. 2016; Adriaenssens et al. 2015; Kaltenegger et al. 2022).
Introduced by Brod in 1982, the definition of the phenomenon technostress changed over time with the latest referring to “stress experienced by end users of Information and Communication Technologies (ICTs)” (Ragu-Nathan et al. 2008, p. 417). Tarafdar et al. (2007) compiled technology-related factors that can cause technostress (techno-overload, techno-invasion, techno-complexity, techno-insecurity, techno-uncertainty), i.e., so-called technostressors (La Torre et al. 2019). Further technostressors include work interruptions by ICTs (Galluch et al. 2015; Ninaus et al. 2015), multitasking (Reinecke et al. 2017), or information overload (Eppler and Mengis 2004; Tarafdar et al. 2007). Existing reviews on technostress report strain reactions in employees related to psychological (e.g., burnout, exhaustion), physiological (e.g., activation of stress hormones), cognitive (e.g., concentration problems) and behavioral (e.g., job performance) symptoms (La Torre et al. 2019; Dragano and Lunau 2020; Berg-Beckhoff et al. 2017; Riedl 2012; Borle et al. 2021). However, these reviews also reveal that research on the health consequences of technostress is still fragmented and the evidence base is limited. In particular, the following knowledge gaps remain:
First, while it is well-researched that exposure to workplace stressors is associated with mental health problems (Madsen et al. 2017; Aronsson et al. 2017), studies on work stressors related to digital technologies and mental health outcomes are sparse with first results suggesting associations with burnout (Dragano and Lunau 2020). Burnout is defined as “a work-related state of exhaustion that occurs among employees, which is characterized by extreme tiredness, reduced ability to regulate cognitive and emotional processes, and mental distancing. These four core dimensions of burnout are accompanied by depressed mood as well as by non-specific psychological and psychosomatic complaints” (Schaufeli et al. 2020, p. 4). The few studies on technostress and burnout were predominantly based on office workers (Berg-Beckhoff et al. 2017). However, burnout is of critical concern especially in clinical work with implications not only for staffs’ health but also for patient care and the entire healthcare system (Dall'Ora et al. 2020; West et al. 2018; Weigl 2022). Recent research in health professionals across different settings showed high to moderate levels of technostress and considerable associations with burnout symptoms amongst other health-related consequences (Golz et al. 2021; Kasemy et al. 2022). Specifically for electronic health record systems, current research among US physicians found that the usability was rated as poor and in turn, that perceived usability was related to provider task load and burnout with task load functioning as a mediator (Melnick et al. 2020a, b). Thus, more investigations on technostress and burnout in healthcare workers are needed.
Second, technostress has mostly been assessed with self-report questionnaires, while objectively measurable biological effects have largely been overlooked. Few studies suggest that technostressors activate physiological stress responses. This was shown for the sympathetic nervous system as one domain of the autonomic nervous system (ANS; e.g., Galluch et al. 2015) and the hypothalamic-pituitary-adrenocortical (HPA) axis (Riedl et al. 2012; Arnetz and Berg 1996; Kasemy et al. 2022). However, these findings relate to acute stress rather than to the long-term effects of chronic stress. As in modern digitalized work environments, technostressors may occur recurrently over prolonged periods, they might lead to chronic stress experience (Day et al. 2010). The human stress response includes—beyond the activation of the main stress systems (ANS and HPA axis)—complex effects of the immune system, most importantly up-regulation of inflammatory pathways (Ulrich-Lai and Herman 2009; Segerstrom and Miller 2004; Morey et al. 2015; Chrousos 2009). In the short-term, these changes are critical for survival, however, in the long-term, wear-and-tear effects of the stress systems can occur (cf. allostatic load model (McEwen 1998; McEwen and Stellar 1993))—as for instance the phenomenon of chronic systemic low-grade inflammation. Low-grade inflammation is suggested as a central pathophysiological mechanism in the development of chronic conditions encompassing cardiovascular, metabolic, and neurodegenerative diseases, depression as well as cancer (Couzin-Frankel 2010; Liu et al. 2017). It is usually assessed by measuring concentrations of the acute phase protein C-reactive protein (CRP) or of cytokines (such as interleukins) in blood or saliva (Rohleder 2019). Adverse psychosocial factors at work were associated with low-grade inflammation in employees, yet with limited evidence (Kaltenegger et al. 2021; Wright et al. 2020). For a better understanding of the long-term psychophysiological health effects of technostressors, it is essential to assess biomarkers indicative of biological alterations of the stress systems, such as chronic low-grade inflammation.
Third, it is unclear whether technostressors are genuinely new, distinct stressors or if they are just antecedents or specific forms of other general psychosocial work stressors like work overload or job insecurity (Dragano and Lunau 2020). Therefore, it is crucial to investigate technostressors in their interplay with other job characteristics and to test for individual as well as interactive effects. For example, technostress in terms of a system breakdown in a human–computer interaction task only increased the skin conductance of male participants if they were under time pressure (Riedl et al. 2013).
As a theoretical foundation, we use the well-established job demand-control(-support) (JDCS) model (Karasek 1979; Johnson and Hall 1988; Johnson et al. 1989): It proposes that the combination of high job demands, low job control, and low social support at work leads to mental strain, which is linked to cardiovascular disease (CVD) morbidity and mortality. Furthermore, we draw on the challenge-hindrance stressor framework (Cavanaugh et al. 2000; LePine et al. 2005; Podsakoff et al. 2007) that has been applied to the technostress concept (Califf and Sarker 2020; Tarafdar et al. 2019): Based on the notion of a duality of negative and positive sides of technology, technostressors can be divided into hindrance technostressors and challenge technostressors. Hindrance technostressors are technology characteristics appraised by the user as disturbing or threatening and comprise the aforementioned technostressors; challenge technostressors in contrast, are appraised as promoting task accomplishment and hence, alleviate technostress (Tarafdar et al. 2019; Califf and Sarker 2020). Several challenge technostressors have been proposed in the literature, such as technical support provision by solving users’ ICT problems (Ragu-Nathan et al. 2008), and usability features consisting of usefulness, i.e., the degree to which technology improves job performance, as well as reliability, i.e., consistency and dependability of technology (Ayyagari et al. 2011).
In sum, we are only at the beginning of understanding the psychophysiological effects of technology-related stress at work—the research base is limited and there is a striking lack of studies on inflammatory (re-)activity as a major pathway in the transition to disease (Becker et al. 2022a, b; Kaltenegger et al. 2021). Therefore, this study sought to investigate associations of different risk factors at work, including technostressors and general psychosocial working conditions (job demands, control, social support), with burnout symptoms and low-grade inflammation among employees of a university hospital. In particular, we examined the following research questions:
-
(1)
Are technostressors associated with burnout symptoms?
-
(2)
Are technostressors associated with low-grade inflammation?
-
(3)
If associations in (1) and (2) are significant, (3a) are they also existent, when controlling for general psychosocial work factors? (3b) are associations moderated by other technostressors or by general work factors (i.e., interaction effects)?
Methods
Design and ethics
This cross-sectional analysis is based on data collected in 2021 (June-November) as part of a larger cohort study on work stress and health sequelae in employees of the University Hospital of Ludwig-Maximilian University (LMU) Munich, Germany. The study protocol has been registered (for more information see: https://osf.io/94p6n/). The study was approved by the Ethics Committee at the Medical Faculty of LMU (20–0914) and is being performed in accordance with the ethical standards of the 1964 Helsinki Declaration. All participants included in the study provided written informed consent.
Participants
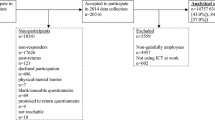
Persons undergoing an obligatory pre-employment medical examination at the Outpatient Clinic for Occupational, Social, and Environmental Medicine were invited to participate in the study. The sample thus consists of new employees at LMU University Hospital with different kinds of professions including nurses, physicians, (medical-) technical, research and administrative staff, etc. Prior to inclusion, participants received information concerning study objectives and procedures. Data collection took place on-site at the outpatient clinic in medical examination rooms. For this study, a subsample of N = 173 (74.6% women, Mage = 31.0 years) was analyzed consisting of participants who had already started their job or who had not started at that time, but who had been employed prior to the beginning of their employment at LMU University Hospital. The following eligibility criteria were applied: Persons with a temporary contract of less than six months were not included. Furthermore, persons reporting current symptoms indicating acute infection or inflammation (such as acute cold, fever, acute injuries, cystitis, etc.), permanent anti-inflammatory medication intake, recent intake of anti-coagulant drugs (last 12 h before testing), pregnancy, or insufficient German language knowledge were excluded. Participants with CRP levels > 10 mg/L were discarded a posteriori since concentrations above this cut-off suggest a medical source of infection or inflammation, what may bias the prediction of low-grade inflammation (Pearson et al. 2003).
Measures
Predictors
General psychosocial work factors
A comprehensive questionnaire was developed for participants’ self-report of their individual work situation. In line with the JDCS model, it included three scales for the assessment of psychosocial working conditions derived from a well-established tool for work analysis (Glaser et al. 2020): Work overload was measured with two items (item example: “I often have to hurry and still cannot complete my work”). Scale reliability was determined with Cronbach’s α = 0.85. Job control was assessed with three items (e.g., “I can determine for myself how to do my work”; α = 0.86). Social climate was captured by two items (e.g.; “In this unit, work relationships with supervisors are based on trust”; α = 0.91). All items were answered on a five-point scale ranging from not at all to to a very great extent.
Technology-related work factors (“technostressors”)
For the measurement of work factors specifically related to digital technologies, we used 11 scales capturing a broad spectrum of potential technostressors:
For hindrance technostressors, four scales developed by Ragu-Nathan et al. (2008) (German translations based on Gimpel et al. (2018)) were applied: techno-overload (3 items; e.g., “I am forced by digital technologies to do more work than I can handle”; α = 0.84), techno-complexity (3 items; e.g., “I do not know enough about digital technologies to handle my job satisfactorily”; α = 0.87), techno-uncertainty (2 items; e.g., “There are always new developments in the digital technologies we use in our organization”; α = 0.75) and techno-insecurity (3 items; e.g., “I have to constantly update my skills on digital technologies to avoid being replaced”; α = 0.63). Further scales captured: work interruptions (3 items, adapted from Glaser et al. 2020; Büssing and Glaser 2002; e.g., “I often have to interrupt my work due to electronic messages [e.g., e-mail, device message]”; α = 0.70); multitasking requirements (2 items, adapted from Semmer et al. 1999; e.g., “Due to digital technologies I have to work on several tasks at the same time”; α = 0.90); and information overload (2 items, Piecha and Hacker 2020; e.g., “I feel that the information I receive via on-duty digital media is too much”; α = 0.93).
For challenge technostressors, the following scales were utilized: reliability (2 items, Ayyagari et al. 2011; Gimpel et al. 2018; e.g., “The digital technologies I use behave in a highly consistent way”; α = 0.90); usefulness (3 items, Ayyagari et al. 2011; Moore and Benbasat 1991; e.g., “Use of digital technologies improves the quality of my work”; α = 0.94); involvement (2 items, e.g.: “Our end users are consulted before the introduction of new digital technologies”; α = 0.79) and technical support provision (2 items, e.g.: “Our end-user help desk is easily accessible”; α = 0.89) (Ragu-Nathan et al. 2008; Gimpel et al. 2018).
Outcomes
Burnout (core and secondary symptoms)
Burnout was measured using the German translation of the Burnout Assessment Tool (BAT) with the two scales core symptoms, consisting of the subscales exhaustion and mental distance, and secondary symptoms (Schaufeli et al. 2019; Glaser and Seubert 2020). The BAT was shown to have good psychometric properties (Schaufeli et al. 2020). Core symptoms were captured by two items per subscale; a sample item for exhaustion is “At work, I feel mentally exhausted”, and for mental distance “I struggle to find any enthusiasm for my work”. A total score for burnout core symptoms was calculated for each participant based on the mean of both subscales. The reliability for this scale was α = 0.79. Secondary symptoms, i.e., psychological and psychosomatic complaints, were assessed with six items; a sample item is “I suffer from headaches”. For each participant, a mean score was computed. Scale reliability was α = 0.69. Answering options ranged from never to always on a five-point scale.
Low-grade inflammation: C-reactive protein
We measured high-sensitivity C-reactive Protein (hs-CRP) in participants’ capillary blood using the minimally invasive dried blood spot method (McDade et al. 2007). In short, blood drops from a prick into the participant’s fingertip with a disposable lancet were collected on filter papers. The filter paper was dried at room temperature for at least 8 h and then stored in an envelope at – 26 °C. Hs-CRP was analyzed with a “Human C-Reactive Protein/CRP Quantikine ELISA Kit” (IBL International) in the laboratory of the Chair of Health Psychology, Friedrich-Alexander University Erlangen-Nürnberg, in Nürnberg, Germany (Becker et al. 2022c for further details). The intra-assay coefficient of variation was 4.18%. Based on established cut-offs, values below 1.0 mg/L indicate a low, between 1.0 and 3.0 mg/L an average and above 3.0 mg/L a high risk for the development of cardiovascular diseases (e.g., Pearson et al. 2003).
Covariates
The following variables were assessed in the questionnaire as potential covariates:
Sociodemographic characteristics: sex (f/m/d), age (in years).
Health-related characteristics: body-mass index (BMI; kg/m2), physical activity (“Overall, how much do you care about getting enough physical activity?”, 1 = not at all – 5 = very much), smoking (no, former, current), alcohol intake (“How often do you have a drink containing alcohol, e.g., glass of wine, beer, cocktail, liquor or liqueur?”; dichotomized at ≥ 2–3 times a week; translated, Bush et al. 1998), chronic conditions (yes, no), hormone medication (for contraception and for other reasons; only for CRP).
Employment-related characteristics: Shiftwork (yes, no), night shift (yes, no), profession (nurse, physician, medical(-technical) personnel, research staff, administration, other), professional tenure (in years), full-time job (yes, no), leadership responsibility (yes, no), extended vacation during the previous 4 weeks before testing (≥ 3 weeks; yes, no), caring for COVID-19 patients (yes, no).
Statistical analyses
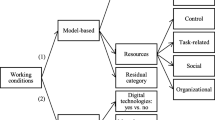
For the technostressor scales, first an exploratory factor analysis (Principal Component Analysis [PCA] with varimax rotation) was conducted to (1) explore the structure of the variables, (2) examine the validity of the items for the measurement of technostressors, and (3) reduce variables for the sake of parsimony and to limit multi-collinearity (Field 2009). For the retrieved factors, mean scores were calculated. Prior to performing parametric tests, measures were checked for normal distribution. Due to positive skewness, both burnout scales (core symptoms = 0.79; secondary symptoms = 0.70) and hs-CRP-values (= 2.81) were transformed using natural logarithm. All predictor variables were centered using grand mean centering. Cronbach’s alpha (α) was calculated for the assessment of internal consistency.
After descriptive analyses, relevant confounders for burnout symptoms and CRP were identified using Pearson correlations, t-tests, and univariate variance analysis. For the analysis of our research questions, we applied linear regressions for each outcome: First, bivariate regressions for one control and one predictor variable at a time were calculated (crude model). Next, multivariate regressions for each predictor variable adjusted for all control variables were performed (model 1–7). Only control variables that showed significant associations with the outcomes in the first place were included in the regression models for reasons of parsimony. We applied the method of hierarchical regression with the identified covariates entered in the first step and each predictor (general work factors and technostressors) entered individually in the second step (research questions 1 and 2). Furthermore, in case of significant associations of technostressors with the outcomes, we additionally controlled for general psychosocial work factors (research question 3a), and if still significant, we tested for moderation effects of technostressors and general psychosocial work factors by including interaction terms into the multivariate models (research question 3b). Assumptions of regression analysis were checked using correlation matrices, variance inflation factor (VIF) values, Durbin-Watson test, histograms, and normal probability plots of residuals. Regarding multi-collinearity, correlations between predictors and covariates for the individual outcomes (burnout, core symptoms: r ≤ 0.55; burnout, secondary symptoms: r ≤ 0.56; CRP: r ≤ 0.30) and VIF values (burnout, core symptoms: ≤ 1.56; burnout, secondary symptoms: ≤ 1.54; CRP: ≤ 1.17), indicated no too strong relationships (Field 2009). All statistical analyses were performed using SPSS Statistics version 26 (IBM SPSS Inc., Chicago, Il, USA).
Results
Factorial validity of technostressors
Bartlett-Test (Chi2 (351) = 2925.67, p < 0.001) and Kaiser–Meyer–Olkin Measure of Sampling Adequacy (KMO = 0.83) indicated meritorious suitability of the variables for factor analysis (Kaiser 1970, 1974). The PCA revealed a six-factor-structure following the Kaiser criterion (Eigenvalue > 1). However, based on the scree-plot and theoretical as well as empirical considerations (Guadagnoli and Velicer 1988), we selected a four-factor solution explaining 61.3% of the total variance. Observed factors could be interpreted in line with the challenge-hindrance model: Factor I was classified as a challenge technostressor relating to usability characteristics and technical support provision (7 items, factor loadings: 0.59–0.88). The other three factors were conceptualized as hindrance technostressors: Factor II describes techno-overload and information overload due to digital technologies (5 items, factor loadings: 0.69–0.82); Factor III pertains to the complexity of digital technologies and associated perceived lack of skills (4 items, factor loadings: 0.72–0.87); and factor IV relates to work interruptions and multitasking demands in the context of digital technologies (5 items, factor loadings: 0.56–0.69). Items showing cross-loadings and/or loadings on a factor with only a few other variables were excluded from the analysis (n = 6 items). The factor loadings per item can be seen in Table S1 (Appendix). For the wording of the items, we refer to Ayyagari et al. (2011), Ragu-Nathan et al. (2008), and Gimpel et al. (2018) for German translations. The newly composed scales had high internal consistencies: α = 0.90 (factor I), α = 0.88 (factors II and III), and α = 0.84 (factor IV).
Descriptive statistics
Five participants were excluded from the analyses because of CRP > 10 mg/L (n = 4) or due to incomplete survey responses (n = 1). Further, one person of diverse gender had to be excluded, because group comparisons were not possible. The final sample size was n = 167. The sample consisted of 125 women (74.9%), the mean age was 31.1 years (standard deviation, SD = 9.6, range: 17–60), and the average BMI was 24.1 (SD = 5.1, range: 16.6–45.6). Most participants were nurses (n = 46, 27.5%), followed by physicians (n = 33, 19.8%), and research staff (n = 30, 18.0%). The remaining participants were medical-technical personnel (for labs, pharmacy, etc.; n = 22, 13.2%), administrative staff (n = 10, 6.0%), and other (such as therapists, midwives, nutritionists, social workers, etc.; n = 24, 14.4%). The majority was working full-time (n = 129, 77.2%), and 69 (41.3%) were working on a shift schedule with 57 participants doing night shifts. Nineteen (11.4%) employees had leadership responsibilities and 26 (15.6%) were involved in the care of COVID-19 patients. Means and SDs as well as frequencies of all included variables are presented in Table 1.
Associations of work stressors with burnout (core and secondary symptoms)
Burnout core symptoms (exhaustion and mental distance) were significantly negatively associated with physical activity and longer vacations prior to testing (results not shown), and therefore, these variables were entered as covariates into the models. Results of the regression analyses on bivariate (crude) and multivariate (adjusted) associations of the covariates and predictors (general work factors and technostressors; models 1–11) with employees’ burnout core symptoms are presented in Table 2. Work overload was a significant predictor of burnout symptoms (Model 1: non-standardized regression coefficient B = 0.19, p < 0.001). For job control and social climate, no significant associations were observed. However, for all three hindrance technostressors, there were significant positive relationships with burnout core symptoms in crude and adjusted models (techno-/information overload: Model 5: B = 0.19, p < 0.001; techno-complexity: Model 6: B = 0.13, p < 0.001; interruptions and multitasking: Model 7: B = 0.12, p < 0.001). Moreover, techno-/information overload remained a significant predictor of burnout, when general work overload was controlled for (Model 8: B = 0.09, p = 0.005). We also tested for potential moderation effects, but the interaction between work overload and techno-/information overload was not significant. Concerning the included covariates physical activity and prior vacation, robust negative associations with burnout core symptoms were observed in the crude and adjusted models (Table 2).
For burnout secondary symptoms, i.e., psychological and psychosomatic complaints, participants’ sex, physical activity, smoking, and leadership responsibility were identified as relevant covariates. Results of the bivariate and multivariate regression analyses including these covariates, general work factors, and technostressors are depicted in Table 3. Again, work overload significantly predicted secondary symptoms (Model 1: B = 0.05, p = 0.014). Additionally, techno-/information overload (Model 5: B = 0.07, p = 0.004) and techno-complexity (Model 6: B = 0.06, p = 0.038) were significantly related to secondary burnout symptoms. However, when including general work overload in the models (model 8 and 9), associations of the technostressors were not statistically significant. As for the covariates, sex was a significant predictor of burnout secondary symptoms across all models, such that the female sex was associated with increased ratings. In addition, smoking was consistently a significant positive predictor for reporting secondary symptoms. On the contrary, there were trends across the models for negative associations between both physical activity (i.e., higher level of physical activity was associated with lower symptom ratings) and leadership responsibilities with secondary burnout symptoms (i.e., leaders reported less symptoms).
Associations of work stressors with low-grade inflammation (C-reactive protein)
Bivariate (crude) and multivariate (adjusted) regressions for the covariates, predictors (general and technostressors) and hs-CRP are presented in Table 4. Regarding relevant covariates, age (only in the crude model), BMI, use of contraceptives, and leadership responsibility were consistently positively associated with employees’ hs-CRP levels. Physical activity was negatively associated with hs-CRP (only in the crude model). For the predictors, results showed a statistical trend for a relation of work overload and hs-CRP (only in the crude model: B = 0.15, p = 0.071). For the other general work factors and the technostressors, no significant associations were observed neither in the crude nor in the adjusted models.
Discussion
The aim of this study was to assess associations of technostressors at work with psychological (i.e., burnout symptoms) and biological (i.e., hs-CRP as an inflammatory marker) health outcomes. To the best of our knowledge, this is the first study to investigate the potential effects of technostressors on immune activity in terms of chronic low-grade inflammation. Research on technostress as a risk factor for adverse psychophysiological health is still “work-in-progress” and there is a broad range of different theoretical terms and measures largely due to the interdisciplinary character of research on this phenomenon (Dragano and Lunau 2020, p. 411). With the ever-increasing digitalization and the ubiquity of digital technologies in employees’ workplaces, it is timely to advance our understanding of the phenomenology of technostress and the consequences for employee health, both positive and negative.
To this end, our research approach comprised two steps: We measured technostress with a comprehensive questionnaire including 27 items from 11 scales based on the literature. In an attempt to identify underlying, latent dimensions within this compilation of variables, we first conducted an exploratory factor analysis (Field 2009). We extracted four factors and interpreted them in line with the challenge-hindrance model (Califf and Sarker 2020; Tarafdar et al. 2019). Factor I—the challenge technostressor “usability and technical support”—reflects the positive aspect of technostress, i.e., technology characteristics appraised as beneficial for work-related achievement (Podsakoff et al. 2007; Califf and Sarker 2020). This factor includes reliability of digital technologies, their usefulness for the execution of job tasks, and technical support provision at work. Factors II-IV represent hindrance technostressors, i.e., stressors appraised as thwarting job-related accomplishment (Podsakoff et al. 2007). Factor II (“techno- and information overload”) can be interpreted as an extension of the well-established stressor techno-overload (Tarafdar et al. 2007), i.e., increased workload and work pace due to ICTs, by information overload, i.e., the feeling of too much information (“information flood”) transmitted through ICTs (Piecha and Hacker 2020). Factor III (“techno-complexity and lack of skills”) describes the users’ feeling of inadequacy regarding their skills due to high complexity of ICTs requiring extra effort; this is accompanied by the feeling of pressure through coworkers with better ICT knowledge and skills (Tarafdar et al. 2007). And lastly, factor IV (“interruptions and multitasking”) represents frequent interruptions of the workflow due to digital technologies and the requirement to perform several tasks simultaneously or alternately (i.e., multitasking) (Baethge and Rigotti 2013, 2010). As a second step, we investigated associations of these four factors with employees’ burnout symptoms and low-grade inflammation under consideration of other job characteristics (work overload, control, social climate) and a broad range of potential confounders. Regarding our research questions, we yielded the following results:
First, we found associations of hindrance technostressors and burnout symptoms. In particular, techno-/information overload, techno-complexity as well as interruptions and multitasking were positively related to core symptoms of burnout. Moreover, techno-/information overload and techno-complexity were associated with secondary burnout symptoms. Our results thus add to the preliminary evidence for a positive association of technostressors and burnout (Dragano and Lunau 2020; Berg-Beckhoff et al. 2017). A prior study showed that high quantity and poor quality (i.e., high ambiguity) of workplace e-mail contributed to emotional exhaustion (Brown et al. 2014). E-mail stressors can be regarded as manifestations of our identified dimensions techno-/information overload, in terms of overstraining users’ information-processing capacity (Eppler and Mengis 2004), and interruptions/multitasking by causing immediate interruptions of the workflow and the perceived requirement to perform several tasks simultaneously, in order to manage the amount of emails. Concerning techno-complexity, however, other studies did not find effects on burnout, but—similar to our results—effects of techno-overload and techno-insecurity (Califf and Brooks 2020; Day et al. 2012). With regard to secondary burnout symptoms, our observations are consistent with a previous investigation showing associations of telecommunication system engineers’ perceived mental workload and lack of skills with psychosomatic symptoms such as headache, mental fatigue, or restlessness (Arnetz and Wiholm 1997). Altogether, our observations call for a more nuanced picture with potentially differential effects of distinct technostressors on various aspects of burnout.
Second, even after adjusting for work overload, techno-/information overload still significantly predicted burnout core symptoms and also secondary symptoms on a trend level. In contrast to previous studies (Califf and Sarker 2020; Ayyagari et al. 2011), we did not find any associations of the challenge technostressor with our outcomes, i.e., no direct health-promoting effects. Nonetheless, we observed a small negative effect of social climate on secondary burnout symptoms, in that good social climate was related to fewer symptoms. Drawing upon the buffer hypothesis of the JDC model (Karasek 1979; van der Doef and Maes 1999), we sought to identify interaction effects between the job characteristics, i.e., whether job control, social climate or the challenge technostressor reduces the potential associations of work overload and the hindrance technostressors with the outcomes. We did not detect any interactions of technostressors and general work stressors. This is in line with a current review suggesting strong evidence for the absence of the theorized interaction effect between job demands and control in the prediction of workers’ well-being (Huth and Chung-Yan 2022).
Third, we did not observe associations of technostressors with low-grade inflammation (hs-CRP). We just observed one, yet non-significant association of work overload in the crude model. This preliminary finding adds to the research base on the JDC(S) model and inflammatory markers, which heretofore is limited and inconclusive (Kaltenegger et al. 2021; Wright et al. 2020; Nakata 2012). Again, we could not identify any effects of job control and social climate on hs-CRP, whereas few previous investigations reported protective effects of job resources such as supervisor support (Eguchi et al. 2016), control (Shirom et al. 2008) or organizational justice (Elovainio et al. 2010) in terms of reduced inflammation. In hospital employees, respective investigations are sparse. One recent study surprisingly found a positive relationship of job autonomy and CRP among geriatric care professionals, perhaps due to greater responsibilities and experiences of excessive demands (Kaltenegger et al. 2022).
With regard to the included covariates, physical activity was consistently negatively associated with burnout symptoms and hs-CRP (significantly only in the crude model). While it is well-documented that physical activity during leisure time has beneficial effects on physical and mental health, occupational physical activity can be detrimental—a phenomenon called the physical activity health paradox (Holtermann et al. 2012; Lee et al. 2021). This aspect deserves careful consideration especially in the healthcare sector, where many professions face high physical demands such as lifting heavy loads, working in awkward postures, or walking long distances. Interestingly, participants in leadership positions had higher levels of CRP but reported less secondary burnout symptoms. Although higher occupational position has been associated with lower inflammation (e.g., Fraga et al. 2015), one can speculate that this small group of employees with leadership responsibilities at a large university hospital might be exposed to a particularly high work stress level and that confounding factors, such as profession, sex, age and professional tenure might explain this observation.
In sum, our results suggest that technostress in the form of techno- and information overload is associated with burnout symptoms. The association remained significant when work overload was included in the multivariate model. This finding indicates that (information) overload caused by digital technology use is a distinct work stressor with genuine consequences for psychological health. However, these might not be “strong” enough to manifest on a biological level in terms of chronic physiological activity, such as low-grade inflammation.
Limitations
Some important limitations need to be considered when interpreting our results. First, this study is cross-sectional and, therefore, no inferences concerning causality can be drawn. Second, based on the a-priori power analysis for the complete prospective cohort study yielding a required sample size of N = 200, our sample size may be regarded as too small and hence, our study might have been underpowered. However, as this sample consists of new employees, for a valid assessment of their work situation and associated influences, we rigorously had to exclude a large amount of the original sample. Participants who had not started their job at the university hospital at the time of examination and who were not working prior to the start of employment (because of studies/school, parental leave, unemployment or similar) were not included. Nonetheless, the heterogeneity in participants’ life and work situations remains a critical issue. Therefore, we sought to control for potentially influencing factors, such as professional tenure and long vacation or leave in the weeks before testing. Due to the specific sampling procedure and the strict exclusion criteria, our sample consisted mainly of healthy participants of rather young age and short professional tenure, potentially resulting in a floor effect in terms of chronic stress experience. This might explain the comparatively low values in the burnout scales. However, the mean hs-CRP level was in the range of average risk for cardiovascular disease (Pearson et al. 2003). Participants’ age might have also played a role in the evaluation of technostressors, as age has been identified as an important moderator (Reinecke et al. 2017; Tams et al. 2014). In sum, our recruitment method (i.e., pre-employment medical check) may have introduced bias concerning the sample and associations. The cohort was younger compared to the average healthcare worker, what might limit the external validity of our results. We checked for associations of participants’ professions with the outcomes and did not find any significant differences. Therefore, we did not include profession as a covariate in our analyses. It can be assumed that most of the jobs at this large university hospital were affected by the ever-increasing computerization, both in direct (such as medical care) and indirect clinical work (such as administration and research). Nonetheless, different professions might have been affected differently by technology exposure and inherent technostressors. Future research should hence distinguish between professional groups more clearly, in order to identify groups at particular risk for technostress, for instance due to a lack of digital competence (Golz et al. 2021). Further limitations pertain to the measurement of our outcomes: Burnout core symptoms were measured with only two subscales of the BAT with just few items; only hs-CRP concentrations were utilized as an inflammatory marker, while there a many other indicators of low-grade inflammation, such as cytokines (Kaltenegger et al. 2020, for a list). Although we collected broad screening information, we acknowledge that several, potentially confounding lifestyle and behavioral factors were not measured in sufficient detail, such as step count or weight change. Moreover, the inclusion of additional biomarkers of other stress systems, such as ANS (e.g., heart rate [variability]) and HPA-axis (e.g., cortisol), would be promising for a more comprehensive picture and deeper understanding of the linkage of (techno-)stress, biomarkers and burnout.
Implications for further research and occupational practice
Given that research on psychophysiological effects of technostressors is scarce, our results should be considered preliminary until further investigations can replicate them. Nonetheless, our study provides valuable methodological implications for future research. In particular, we suggest the following avenues with regard to design, measures, and samples: First, prospective studies are needed for a deeper understanding of dynamic and causal processes. Full-panel designs where each predictor and outcome variable is assessed at all measurement time points are suitable to identify both normal (i.e., stressor-to-strain) and reversed (i.e., strain-to-stressor) effects (Taris and Kompier 2014). Second, our operationalization of technostressors and the four-factor-structure should be scrutinized in future studies, and beyond the commonly studied negative aspects of technostress (i.e., hindrance technostressors), also positive (i.e., challenge technostressors) should be taken into account. Moreover, it is crucial to apply multiple methods, i.e., a combination of self-report data with measurable markers for biological stress, especially for chronic stress given its key role in long-term health. There is a long-standing debate on viable approaches to measure work-related stress (Semmer et al. 2003). The inclusion of biomarkers as outcome variables overcomes the problem of common method variance when both predictor and outcome variables are measured with self-report (Semmer et al. 2003). Moreover, self-report can be biased by individual response tendencies, whereas physiological data are less easily influenced by the participant or the examiners’ expectations. However, also biomarkers have been discussed regarding conceptual, such as ambiguities in interpretation, as well as methodological issues, including limited reliability and potential confounding influences. Thus, self-report should not just be replaced—instead for an optimal assessment of psychobiological effects of work stress, a combination of various methods and multiple information sources is desirable (Semmer et al. 2003). Lastly, more research on technostress in hospital employees is necessary against the backdrop of the vast implementation of health information technology in hospitals.
For occupational health and safety management, there have been calls to consider job stressors related to the digitalization of work in the psychosocial risk assessment (Diebig et al. 2018; Chiappetta 2017). This will facilitate effective prevention and intervention measures on an organizational/structural as well as individual/behavioral level. Several strategies to cope with technostress have been described by healthcare managers, referring to establishing norms, such as good email culture, individual resources, such as digital literacy, and organizational resources, such as accessible and efficient IT support (Stadin et al. 2020). However, there is a lack of systematic prevention and intervention studies on work-related technostress (Rohwer et al. 2022). In general, workplace physical exercise interventions have been proven useful in the reduction of low-grade inflammation (Kaltenegger et al. 2021) and burnout (i.e., exhaustion) (Naczenski et al. 2017).
Conclusions
To the best of our knowledge, this is the first study on technology-related stress at work and chronic low-grade inflammation. Low-grade inflammation is a key pathway through which stress “gets under the skin” and ultimately affects humans’ health. However, biological effects of technostress have been under-researched. We did not find associations of technostressors with inflammation, but techno- and information overload was consistently associated with burnout symptoms in employees of a university hospital. Nevertheless, due to peculiarities of our sample we cannot negate additional biological effects of this stressor in general and deem future research on this question as highly necessary.
Data availability
The dataset generated during and/or analyzed during the current study are not publicly available due to them containing information that could compromise research participant privacy/consent. Public data availability was not considered in the application for ethical approval. However, upon reasonable request data are available from the corresponding author (HK).
References
Abbott PA, Weinger MB (2020) Health information technology: Fallacies and Sober realities - Redux A homage to Bentzi Karsh and Robert Wears. Appl Ergonom 82:102973. https://doi.org/10.1016/j.apergo.2019.102973
Adriaenssens J, de Gucht V, Maes S (2015) Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud 52(2):649–661. https://doi.org/10.1016/j.ijnurstu.2014.11.004
Arnetz BB, Berg M (1996) Melatonin and adrenocorticotropic hormone levels in video display unit workers during work and leisure. J Occupat Environm Med 38(11):1108–1110
Arnetz BB, Wiholm C (1997) Technological stress: psychophysiological symptoms in modern offices. J Psychosom Res 43(1):35–42. https://doi.org/10.1016/S0022-3999(97)00083-4
Aronsson G, Theorell T, Grape T, Hammarström A, Hogstedt C, Marteinsdottir I, Skoog I, Träskman-Bendz L, Hall C (2017) A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 17(1):264. https://doi.org/10.1186/s12889-017-4153-7
Ayyagari R, Grover V, Purvis R (2011) Technostress: technological antecedents and implications. MIS Q 4(35):831–858
Baethge A, Rigotti T (2010) Arbeitsunterbrechungen und Multitasking: Ein umfassender Überblick zu Theorien und Empirie unter besonderer Berücksichtigung von Altersdifferenzen ; Forschung Projekt F 1963. BAuA, Dortmund, Berlin, Dresden
Baethge A, Rigotti T (2013) Interruptions to workflow: Their relationship with irritation and satisfaction with performance, and the mediating roles of time pressure and mental demands. Work Stress 27(1):43–63. https://doi.org/10.1080/02678373.2013.761783
Becker L, Kaltenegger HC, Nowak D, Rohleder N (2022a) Weigl M (2022a) Differences in stress system (re-) activity between single and dual- or multitasking in healthy adults: a systematic review and meta-analysis. Health Psychol Rev. https://doi.org/10.1080/17437199.2022.2071323
Becker L, Kaltenegger HC, Nowak D, Weigl M, Rohleder N (2022b) Physiological stress in response to multitasking and work interruptions: Study protocol. PLoS ONE 17(2):e0263785. https://doi.org/10.1371/journal.pone.0263785
Becker L, Keck A, Rohleder N, Müller-Voggel N (2022c) Higher Peripheral Inflammation Is Associated With Lower Orbitofrontal Gamma Power in Chronic Tinnitus. Front Behav Neurosci 16:883926. https://doi.org/10.3389/fnbeh.2022.883926
Berg-Beckhoff G, Nielsen G, Ladekjær Larsen E (2017) Use of information communication technology and stress, burnout, and mental health in older, middle-aged, and younger workers - results from a systematic review. Int J Occup Environ Health 23(2):160–171. https://doi.org/10.1080/10773525.2018.1436015
Borle P, Reichel K, Niebuhr F, Voelter-Mahlknecht S (2021) How are techno-stressors associated with mental health and work outcomes? a systematic review of occupational exposure to information and communication technologies within the technostress model. Int J Environ Res Public Health 18(16):8673. https://doi.org/10.3390/ijerph18168673
Brod C (1982) Managing technostress: optimizing the use of computer technology. Pers J 61(10):753–757
Brown R, Duck J, Jimmieson N (2014) E-mail in the workplace: The role of stress appraisals and normative response pressure in the relationship between e-mail stressors and employee strain. Int J Stress Manag 21(4):325–347. https://doi.org/10.1037/a0037464
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA (1998) The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol use disorders identification test. Arch Int Med 158(16):1789–1795. https://doi.org/10.1001/archinte.158.16.1789
Büssing A, Glaser J (2002) Das Tätigkeits- und Arbeitsanalyseverfahren für das Krankenhaus - Selbstbeobachtungsversion (TAA-KH-S). Hogrefe, Göttingen
Califf CB, Brooks S (2020) An empirical study of techno-stressors, literacy facilitation, burnout, and turnover intention as experienced by K-12 teachers. Comput Educat 157:103971. https://doi.org/10.1016/j.compedu.2020.103971
Califf CB, Sarker S (2020) The bright and dark sides of technostress: a mixed-methods study involving healthcare IT. MIS Q 44(2):809–856
Cavanaugh MA, Boswell WR, Roehling MV, Boudreau JW (2000) An empirical examination of self-reported work stress among U.S. managers. J Appl Psychol 85(1):65–74. https://doi.org/10.1037/0021-9010.85.1.65
Chiappetta M (2017) The technostress: definition, symptoms and risk prevention. Senses Sci 4(1):358–361
Chrousos GP (2009) Stress and disorders of the stress system. Nat Rev Endocrinol 5(7):374–381. https://doi.org/10.1038/nrendo.2009.106
Couzin-Frankel J (2010) Inflammation bares a dark side. Science (New York, N.Y.) 330(6011):1621. https://doi.org/10.1126/science.330.6011.1621
Dall’Ora C, Ball J, Reinius M, Griffiths P (2020) Burnout in nursing: a theoretical review. Hum Resour Health 18(1):41. https://doi.org/10.1186/s12960-020-00469-9
Dawe K, Montgomery A, McGee H, Panagopoulou E, Morgan K, Hackshaw L, Vedhara K (2016) The effects of perceived stress on biological parameters in healthcare professionals: A systematic review. J Health Psychol 21(5):607–618. https://doi.org/10.1177/1359105314532970
Day A, Scott N, Kevin Kelloway E (2010) Information and communication technology: Implications for job stress and employee well-being. In: Perrewé PL, Ganster DC (Eds) New developments in theoretical and conceptual approaches to job stress, vol 8. Research in occupational stress and well-being. Emerald Group Publishing Limited, pp 317–350
Day A, Paquet S, Scott N, Hambley L (2012) Perceived information and communication technology (ICT) demands on employee outcomes: the moderating effect of organizational ICT support. J Occup Health Psychol 17(4):473–491. https://doi.org/10.1037/a0029837
Diebig M, Jungmann F, Müller A, Wulf IC (2018) Inhalts- und prozessbezogene Anforderungen an die Gefährdungsbeurteilung psychischer Belastung im Kontext Industrie 4.0. Zeitschrift Für Arbeits- Und Organisationspsychologie a&o 62(2):53–67. https://doi.org/10.1026/0932-4089/a000265
Dragano N, Lunau T (2020) Technostress at work and mental health: concepts and research results. Curr Opin Psychiatry 33(4):407–413. https://doi.org/10.1097/YCO.0000000000000613
Eguchi H, Shimazu A, Kawakami N, Inoue A, Tsutsumi A (2016) Source-specific workplace social support and high-sensitivity C-reactive protein levels among Japanese workers: A 1-year prospective cohort study. Am J Ind Med 59(8):676–684. https://doi.org/10.1002/ajim.22600
Elovainio M, Ferrie JE, Singh-Manoux A, Gimeno D, de Vogli R, Shipley M, Vahtera J, Brunner E, Marmot MG, Kivimäki M (2010) Organisational justice and markers of inflammation: the Whitehall II study. Occup Environ Med 67(2):78–83. https://doi.org/10.1136/oem.2008.044917
Eppler MJ, Mengis J (2004) The concept of information overload: a review of literature from organization science, accounting, marketing, MIS, and related disciplines. Inf Soc 20(5):325–344. https://doi.org/10.1080/01972240490507974
Field A (2009) Discovering statistics using SPSS: (and sex and drugs and rock “n” roll), 3rd edn. Sage Publ, Los Angeles
Fraga S, Marques-Vidal P, Vollenweider P, Waeber G, Guessous I, Paccaud F, Barros H, Stringhini S (2015) Association of socioeconomic status with inflammatory markers: a two cohort comparison. Prev Med 71:12–19. https://doi.org/10.1016/j.ypmed.2014.11.031
Galluch P, Grover V, Thatcher J (2015) Interrupting the workplace: examining stressors in an information technology context. JAIS 16(1):1–47. https://doi.org/10.17705/1jais.00387
Gimpel H, Lanzl J, Manner-Romberg T, Nüske N (2018) Digitaler Stress in Deutschland: Eine Befragung von Erwerbstätigen zu Belastung und Beanspruchung durch Arbeit mit digitalen Technologien, Düsseldorf
Glaser J, Seubert C (2020) Manual zur deutschen Fassung des Burnout Assessment Tool (BAT-D). Universität Innsbruck, Österreich
Glaser J, Hornung S, Höge T, Strecker C (2020) Das Tätigkeits- und Arbeitsanalyseverfahren (TAA): Screening psychischer Belastungen in der Arbeit. Innsbruck university press
Golz C, Peter KA, Müller TJ, Mutschler J, Zwakhalen SMG, Hahn S (2021) Technostress and digital competence among health professionals in swiss psychiatric hospitals: cross-sectional Study. JMIR Mental Health 8(11):e31408. https://doi.org/10.2196/31408
Guadagnoli E, Velicer WF (1988) Relation of sample size to the stability of component patterns. Psychol Bull 103(2):265–275. https://doi.org/10.1037/0033-2909.103.2.265
Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G (2012) The health paradox of occupational and leisure-time physical activity. Br J Sports Med 46(4):291–295. https://doi.org/10.1136/bjsm.2010.079582
Huth KBS, Chung-Yan GA (2022) Quantifying the evidence for the absence of the job demands and job control interaction on workers’ well-being: A Bayesian meta-analysis. J Appl Psychol. https://doi.org/10.1037/apl0001066
Johnson JV, Hall EM (1988) Job strain, work place social support, and cardiovascular disease: a cross-sectional study of a random sample of the Swedish working population. Am J Public Health 78(10):1336–1342. https://doi.org/10.2105/ajph.78.10.1336
Johnson JV, Hall EM, Theorell T (1989) Combined effects of job strain and social isolation on cardiovascular disease morbidity and mortality in a random sample of the Swedish male working population. Scand J Work Environ Health 15(4):271–279. https://doi.org/10.5271/sjweh.1852
Kaiser HF (1970) A second generation little jiffy. Psychometrika 35(4):401–415. https://doi.org/10.1007/BF02291817
Kaiser HF (1974) An index of factorial simplicity. Psychometrika 39(1):31–36. https://doi.org/10.1007/BF02291575
Kaltenegger HC, Becker L, Rohleder N, Nowak D, Weigl M (2020) Association of working conditions including digital technology use and systemic inflammation among employees: study protocol for a systematic review. Syst Rev 9(1):221. https://doi.org/10.1186/s13643-020-01463-x
Kaltenegger HC, Becker L, Rohleder N, Nowak D, Weigl M (2021) Associations of working conditions and chronic low-grade inflammation among employees: a systematic review and meta-analysis. Scand J Work Environ Health 47(8):565–581. https://doi.org/10.5271/sjweh.3982
Kaltenegger HC, Weigl M, Becker L, Rohleder N, Nowak D, Quartucci C (2022) Psychosocial working conditions and chronic low-grade inflammation in geriatric care professionals: A cross-sectional study. PLoS ONE 17(9):e0274202. https://doi.org/10.1371/journal.pone.0274202
Karasek R (1979) Job demands, job decision latitude, and mental strain: implications for job design. Adm Sci Q 24:285–308
Kasemy ZA, Sharif AF, Barakat AM, Abdelmohsen SR, Hassan NH, Hegazy NN, Sharfeldin AY, El-Ma’doul AS, Alsawy KA, Abo Shereda HM, Abdelwanees S (2022) Technostress Creators and Outcomes Among Egyptian Medical Staff and Students: A Multicenter Cross-Sectional Study of Remote Working Environment During COVID-19 Pandemic. Front Public Health 10:796321. https://doi.org/10.3389/fpubh.2022.796321
La Torre G, Esposito A, Sciarra I, Chiappetta M (2019) Definition, symptoms and risk of techno-stress: a systematic review. Int Arch Occup Environ Health 92(1):13–35. https://doi.org/10.1007/s00420-018-1352-1
Lee J, Kim H-R, Jang T-W, Lee D-W, Lee YM, Kang M-Y (2021) Occupational physical activity, not leisure-time physical activity, is associated with increased high-sensitivity C reactive protein levels. Occup Environ Med 78(2):86–91. https://doi.org/10.1136/oemed-2020-106753
LePine JA, Podsakoff NP, LePine MA (2005) A meta-analytic test of the challenge stressor-hindrance stressor framework: an explanation for inconsistent relationships among stressors and performance. AMJ 48(5):764–775. https://doi.org/10.5465/amj.2005.18803921
Liu Y-Z, Wang Y-X, Jiang C-L (2017) Inflammation: The common pathway of stress-related diseases. Front Hum Neurosci 11:316. https://doi.org/10.3389/fnhum.2017.00316
Madsen IEH, Nyberg ST, Magnusson Hanson LL, Ferrie JE, Ahola K, Alfredsson L, Batty GD, Bjorner JB, Borritz M, Burr H, Chastang J-F, de Graaf R, Dragano N, Hamer M, Jokela M, Knutsson A, Koskenvuo M, Koskinen A, Leineweber C, Niedhammer I, Nielsen ML, Nordin M, Oksanen T, Pejtersen JH, Pentti J, Plaisier I, Salo P, Singh-Manoux A, Suominen S, ten Have M, Theorell T, Toppinen-Tanner S, Vahtera J, Väänänen A, Westerholm PJM, Westerlund H, Fransson EI, Heikkilä K, Virtanen M, Rugulies R, Kivimäki M (2017) Job strain as a risk factor for clinical depression: systematic review and meta-analysis with additional individual participant data. Psychol Med 47(8):1342–1356. https://doi.org/10.1017/S003329171600355X
McDade TW, Williams S, Snodgrass JJ (2007) What a drop can do: dried blood spots as a minimally invasive method for integrating biomarkers into population-based research. Demography 44(4):899–925. https://doi.org/10.1353/dem.2007.0038
McEwen BS (1998) Protective and damaging effects of stress mediators. N Engl J Med 338(3):171–179. https://doi.org/10.1056/NEJM199801153380307
McEwen BS, Stellar E (1993) Stress and the individual. Mechanisms leading to disease. Arch Int Med 153(18):2093–2101
Melnick ER, Dyrbye LN, Sinsky CA, Trockel M, West CP, Nedelec L, Tutty MA, Shanafelt T (2020a) The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clin Proc 95(3):476–487. https://doi.org/10.1016/j.mayocp.2019.09.024
Melnick ER, Harry E, Sinsky CA, Dyrbye LN, Wang H, Trockel MT, West CP, Shanafelt T (2020b) Perceived electronic health record usability as a predictor of task load and burnout among US physicians: mediation analysis. J Med Internet Res 22(12):e23382. https://doi.org/10.2196/23382
Moore GC, Benbasat I (1991) Development of an instrument to measure the perceptions of adopting an information technology innovation. Inf Syst Res 2(3):192–222. https://doi.org/10.1287/isre.2.3.192
Morey JN, Boggero IA, Scott AB, Segerstrom SC (2015) Current directions in stress and human immune function. Curr Opin Psychol 5:13–17. https://doi.org/10.1016/j.copsyc.2015.03.007
Naczenski LM, de Vries JD, van Hooff MLM, Kompier MAJ (2017) Systematic review of the association between physical activity and burnout. J Occup Health 59(6):477–494. https://doi.org/10.1539/joh.17-0050-RA
Nakata A (2012) Psychosocial job stress and immunity: a systematic review. Methods Mol Biol (clifton, N.J.) 934:39–75. https://doi.org/10.1007/978-1-62703-071-7_3
Ninaus K, Diehl S, Terlutter R, Chan K, Huang A (2015) Benefits and stressors - Perceived effects of ICT use on employee health and work stress: An exploratory study from Austria and Hong Kong. Int J Qual Stud Health Well Being 10:28838. https://doi.org/10.3402/qhw.v10.28838
Parker SK, Grote G (2022) Automation, algorithms, and beyond: why work design matters more than ever in a digital world. Appl Psychol 71(4):1171–1204. https://doi.org/10.1111/apps.12241
Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO, Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC, Taubert K, Tracy RP, Vinicor F (2003) Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for disease control and prevention and the american heart association. Circulation 107(3):499–511. https://doi.org/10.1161/01.CIR.0000052939.59093.45
Piecha A, Hacker W (2020) Informationsflut am Arbeitsplatz - Umgang mit großen Informationsmengen vermittelt durch elektronische Medien: Forschungsbericht zu Projekt F2373, Dortmund
Podsakoff NP, LePine JA, LePine MA (2007) Differential challenge stressor-hindrance stressor relationships with job attitudes, turnover intentions, turnover, and withdrawal behavior: a meta-analysis. J Appl Psychol 92(2):438–454. https://doi.org/10.1037/0021-9010.92.2.438
Ragu-Nathan TS, Tarafdar M, Ragu-Nathan BS, Tu Q (2008) The consequences of technostress for end users in organizations: conceptual development and empirical validation. Inf Syst Res 19(4):417–433. https://doi.org/10.1287/isre.1070.0165
Reinecke L, Aufenanger S, Beutel ME, Dreier M, Quiring O, Stark B, Wölfling K, Müller KW (2017) Digital stress over the life span: the effects of communication load and internet multitasking on perceived stress and psychological health impairments in a german probability sample. Media Psychol 20(1):90–115. https://doi.org/10.1080/15213269.2015.1121832
Riedl R (2012) On the biology of technostress. SIGMIS Database 44(1):18–55. https://doi.org/10.1145/2436239.2436242
Riedl R, Kindermann H, Auinger A, Javor A (2012) Technostress from a neurobiological perspective. Bus Inf Syst Eng 4(2):61–69. https://doi.org/10.1007/s12599-012-0207-7
Riedl R, Kindermann H, Auinger A, Javor A (2013) Computer breakdown as a stress factor during task completion under time pressure: identifying gender differences based on skin conductance. Adv Hum Comp Interact 2013:1–8. https://doi.org/10.1155/2013/420169
Rohleder N (2019) Stress and inflammation - The need to address the gap in the transition between acute and chronic stress effects. Psychoneuroendocrinology 105:164–171. https://doi.org/10.1016/j.psyneuen.2019.02.021
Rohwer E, Flöther J-C, Harth V, Mache S (2022) Overcoming the “Dark Side” of technology-a scoping review on preventing and coping with work-related technostress. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph19063625
Schaufeli WB, de Witte H, Desart S (2019) Manual Burnout Assessment Tool (BAT). Unpublished internal report, KU Leuven, Belgium
Schaufeli WB, Desart S, de Witte H (2020) Burnout assessment tool (BAT)-development, validity, and reliability. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph17249495
Segerstrom SC, Miller GE (2004) Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull 130(4):601–630. https://doi.org/10.1037/0033-2909.130.4.601
Semmer NK, Zapf D, Dunckel H (1999) Instrument zur streßbezogenen Tätigkeitsanalyse ISTA. In: Dunckel H (ed) Handbuch psychologischer Arbeitsanalyseverfahren. VdF Hochschulverlag, Zürich, pp 179–204
Semmer NK, Grebner S, Elfering A (2003) Beyond self-report: using observational, physiological, and situation-based measures in research on occupational stress. In: Emotional and Physiological Processes and Positive Intervention Strategies, vol 3. Research in Occupational Stress and Well-being. Emerald (MCB UP), Bingley, pp 205–263
Shirom A, Toker S, Berliner S, Shapira I (2008) The job demand-control-support model and stress-related low-grade inflammatory responses among healthy employees: a longitudinal study. Work Stress 22(2):138–152. https://doi.org/10.1080/02678370802180830
Stadin M, Nordin M, Fransson EI, Broström A (2020) Healthcare managers’ experiences of technostress and the actions they take to handle it - a critical incident analysis. BMC Med Inform Decis Mak 20(1):244. https://doi.org/10.1186/s12911-020-01261-4
Tams S, Grover V, Thatcher J (2014) Modern information technology in an old workforce: Toward a strategic research agenda. J Strateg Inf Syst 23(4):284–304. https://doi.org/10.1016/j.jsis.2014.10.001
Tarafdar M, Tu Q, Ragu-Nathan BS, Ragu-Nathan TS (2007) The impact of technostress on role stress and productivity. J Manag Inf Syst 24(1):301–328. https://doi.org/10.2753/MIS0742-1222240109
Tarafdar M, Cooper CL, Stich J-F (2019) The technostress trifecta - techno eustress, techno distress and design: Theoretical directions and an agenda for research. Info Syst J 29(1):6–42. https://doi.org/10.1111/isj.12169
Taris TW, Kompier MAJ (2014) Cause and effect: optimizing the designs of longitudinal studies in occupational health psychology. Work Stress 28(1):1–8. https://doi.org/10.1080/02678373.2014.878494
Ulrich-Lai YM, Herman JP (2009) Neural regulation of endocrine and autonomic stress responses. Nat Rev Neurosci 10(6):397–409. https://doi.org/10.1038/nrn2647
van der Doef M, Maes S (1999) The job demand-control (-support) model and psychological well-being: a review of 20 years of empirical research. Work Stress 13(2):87–114. https://doi.org/10.1080/026783799296084
Weigl M (2022) Physician burnout undermines safe healthcare. BMJ (clinical Res Ed). https://doi.org/10.1136/bmj.o2157
West CP, Dyrbye LN, Shanafelt TD (2018) Physician burnout: contributors, consequences and solutions. J Intern Med 283(6):516–529. https://doi.org/10.1111/joim.12752
Wright BJ, Eddy PJ, Kent S (2020) Work Stress, Immune, and Inflammatory Markers. In: Theorell T (ed) Handbook of Socioeconomic Determinants of Occupational Health. Springer International Publishing, Cham, pp 1–19
Funding
Open Access funding enabled and organized by Projekt DEAL. This work is part of the research project “Identifikation biomedizinischer und gesundheitlicher Wirkweisen von positiven und negativen Auswirkungen von digitalem Stress und dessen Bewältigung” [‘Identification of biomedical and health-related modes of action of positive and negative effects of digital stress and coping with it’] which is part of the Bavarian Research Association on Healthy Use of Digital Technologies and Media (ForDigitHealth), funded by the Bavarian Ministry of Science and Arts. HK, MW and DN have been partly funded by the Munich Centre for Health Sciences (MC-Health). The funders were not involved in the study design, the collection, analysis and interpretation of the data, the writing of the report, and the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Conceptualization: Helena C. Kaltenegger, Linda Becker, Nicolas Rohleder, Dennis Nowak, Caroline Quartucci, Matthias Weigl. Data curation: Helena C. Kaltenegger, Matthias Weigl. Formal analysis: Helena C. Kaltenegger, Matthias Weigl. Investigation: Helena C. Kaltenegger, Caroline Quartucci. Methodology: Helena C. Kaltenegger, Linda Becker, Nicolas Rohleder, Dennis. Nowak, Matthias Weigl. Project administration: Matthias Weigl, Helena C. Kaltenegger. Supervision: Matthias Weigl. Writing – original draft: Helena C. Kaltenegger. Writing – review & editing: Helena C. Kaltenegger, Linda Becker, Nicolas Rohleder, Dennis Nowak, Caroline Quartucci, Matthias Weigl.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee at the Medical Faculty of Ludwig Maximilian University (LMU) Munich (November 23th 2020/ 20–0914). Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaltenegger, H.C., Becker, L., Rohleder, N. et al. Associations of technostressors at work with burnout symptoms and chronic low-grade inflammation: a cross-sectional analysis in hospital employees. Int Arch Occup Environ Health 96, 839–856 (2023). https://doi.org/10.1007/s00420-023-01967-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-023-01967-8