
Abstract
Objective
This study investigates the associations between working from home and the presence of MSP during the COVID-19 pandemic. Working from home often involves a lot of sedentary computer screen work and the home working environment might not be optimally equipped, which can lead to health problems, including musculoskeletal pain (MSP).
Methods
Longitudinal data from 16 questionnaire rounds of the Lifelines COVID-19 cohort during the first year of the COVID-19 pandemic (March 2020-February 2021) were used. In total, 40,702 Dutch workers were included. In every round, participants reported whether they worked on location, from home, or hybrid. Logistic Generalized Estimating Equations were used to study the association of work situation with the presence of MSP and the presence of severe MSP.
Results
Working from home was associated with higher risks of having MSP in the lower back (OR: 1.05, 95% CI 1.02–1.08), in the upper back (OR: 1.24, 95% CI 1.18–1.31), and in the neck, shoulder(s) and/or arm(s) (OR: 1.18, 95% CI 1.13–1.22). Hybrid working was associated with higher risks of having pain in the upper back (OR: 1.09, 95% CI 1.02–1.17) and in the neck, shoulder(s) and/or arm(s) (OR: 1.14, 95% CI 1.09–1.20). Both home and hybrid workers had higher risks of severe MSP in the different body areas.
Conclusion
Home workers, and to a smaller extent hybrid workers, had higher risks of having MSP than location workers during the first year of the COVID-19 pandemic. The results indicate the importance of measures to prevent MSP in future policies involving working from home.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
During the COVID-19 pandemic, different containment measures were implemented to control the spread of the SARS-CoV-2 virus, including working from home as much as possible. As a result, working arrangements changed and the number of people that worked from home increased tremendously (Leroy et al. 2021; Lopez-Leon et al. 2020). To illustrate, in The Netherlands before the COVID-19 pandemic in 2019, 37 percent of the workers did work from home sometimes, on average for slightly more than 6 h per week and working completely from home barely happened (Hooftman et al. 2020). By mid-2020, the proportion of people working from home increased to 45 percent with most of them working completely from home, with an average of 29 h per week (Hooftman et al. 2020).
Besides the advantages of working from home (e.g. less commuting and having more flexibility in work hours), working from home brings several constraints (Ipsen et al. 2021). First, working from home often involves a lot of sedentary computer screen work with less active interruptions, for example to walk to meetings or go to the printer, than when working at location. In addition, only one-third of home workers in 2020 and half of home workers in 2021 in the Netherlands had an optimally furnished workplace for a good work posture; an adjustable desk, an adjustable chair, a separate monitor and a separate mouse all together (Hooftman et al. 2020; Oude Hengel et al. 2021). A large group of home workers thus lack an ergonomically sound workplace at home. Furthermore, when ergonomic and adaptable furniture is available, workers do not always install and use the furniture appropriately (van Niekerk et al. 2012). Sitting for many hours behind the screen at workplaces which are not ergonomically installed subsequently creates a risk of musculoskeletal pain (MSP) (van Niekerk et al. 2012; Wahlström 2005). Based on these factors together, one would expect that homeworkers experienced more MSP compared to location workers during the COVID-19 pandemic.
Not much is known yet about the association between working from home and MSP during the COVID-19 pandemic and recently conducted studies showed mixed results. A Turkish case-controlled study showed that pain in the lower back was higher among home workers in comparison with location workers during 3-month lockdown from March 2020 onwards (Toprak Celenay et al. 2020). Results of other European cross-sectional studies comparing MSP during pre- and peri-lockdown indicated no differences (Argus and Pääsuke 2021) or even a decrease (possibly through increased exercise in the study population) in MSP among home workers (Rodríguez-Nogueira et al. 2020). Descriptive results of a Dutch report also showed a decrease of arm, neck or shoulder complaints among homeworkers from 42 percent before the lockdown in 2019 to 38 percent during the lockdown in 2021 (Oude Hengel et al. 2021). This decrease of arm, neck or shoulder complaints was the same for location workers (from 42 percent in 2019 to 36 percent in 2021). However, an ensemble of in-depth studies using appropriate control groups and control variables to study the association between working from home and MSP is not yet available.
As a consequence of previous studies using a cross-sectional study design, knowledge is lacking about the presence of MSP over time during the COVID-19 pandemic. For example, it is conceivable that the longer time people work from home in probable sub-optimally equipped workplaces, the more MSP will arise, or that the presence of MSP varies according to different containment measures. To get insight into the association between working from home and the presence of MSP during a longer period, multiple measurements over a longer period are needed. Therefore, the aim of our study was to investigate the longitudinal association between working from home and MSP, with multiple measurements during the first year of the COVID-19 pandemic in a large population of Dutch workers. As working from home, either fully or partly, is expected to remain more common practice, knowledge about the impact on MSP is relevant for future policies involving working from home.
Data and methods
Data
Data from the Lifelines COVID-19 cohort were used (Lifelines 2021). The Lifelines COVID-19 cohort is part of the larger Lifelines population cohort which is a multi-disciplinary prospective population-based cohort study examining in an unique three-generation design the health and health-related behaviors of 167,729 persons living in the North of the Netherlands (provinces Groningen, Friesland and Drenthe). It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioral, physical and psychological factors which contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. During three questionnaire rounds of assessment (1A 2007–2013, 2A 2014–2017, 3A 2019–2023) and additional questionnaires in-between (1B 2011–2014, 1C 2012–2015, 2B 2016–2019) (Sijtsma et al. 2021), participants answered questions including their demographics (e.g., age, sex, educational level) and work-related factors (occupation, occupational status) (Lifelines 2021).
Active participants aged 18 years or older in the Lifelines population cohort were invited to participate in the Lifelines COVID-19 cohort. The aim of the Lifelines COVID-19 cohort was to study the possible causes of developing serious symptoms in response to an infection with SARS-CoV-2 and the impact of the pandemic and quarantine on physical and mental health and socio-economic status in the general population. Data collection started at the beginning of the COVID-19 pandemic in The Netherlands, in March 2020, and participants were invited to fill in a digital questionnaire each round. Starting in round 8 (May 23, 2020), participants were invited only if they had completed at least one previous COVID-19 questionnaire in rounds 1–7. Data of the same participants in different study rounds could be linked to each other by a pseudonymized linking variable which was provided by the Lifelines COVID-19 cohort. Measurements consisted of (bi-)weekly questionnaires and from September 2020 onwards of monthly questionnaires with questions about work situation and physical and mental wellbeing.
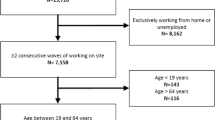
In this study, data of 16 questionnaire rounds (conducted between March 2020-February 2021) of the Lifelines COVID-19 cohort were used, for an overview of the used questionnaire rounds, see Appendix A, Table 4. Participants who completed at least one questionnaire and had a working age (between 18 and 67 years) were included (N = 63,581). As we aimed to include participants who were active workers for the majority of the study, only workers who worked > 75% of the rounds in which they participated were included (N = 48,202). In addition, of the rounds in which they worked, workers needed to work > 75% of the time on location and/or from home (see work situation measure) to be included (N = 43,116). Hereafter, participants were included if they had at least one round of data available on the different types of musculoskeletal pain and complete data on the covariates (N = 40,702 for lower back pain and N = 28,915 for upper back pain and pain in the neck/shoulder(s) and/or arm(s)). See Fig. 1 below for an overview of all selections made.

Flow diagram of the study population
Measurements
Work situation
Work situation was operationalized by a variable with three categories indicating whether a participant was working from home, working on location or working both at home and on location (hybrid) at a specific round. Participants were asked about their daily activity with the following question: ‘What do you currently do in your daily life?’ with the answer categories ‘I am a student’, ‘I work (full-time, part-time, freelance)’, ‘I am on disability’, ‘I am unemployed’, ‘I am retired’, ‘I am on maternity leave’ or ‘other’. Participants who answered their daily activity is work were further asked about their current work situation with multiple answers possible from ‘I work from home’, ‘I am laid off but am still being paid’, ‘I am laid off and am no longer paid’, I continue to work at the usual location (e.g. office, factory, construction site)’, ‘I continue to work at multiple sites for my job’, ‘I am forced to take sick leave or vacation time’ and ‘other’. Participants who answered ‘I work from home’ were categorized as home workers in that specific round. If participants answered ‘I continue to work at the usual location’ or ‘I continue to work at multiple sites for my job’ they were categorized as location workers. When participants answered to work on location as well as from home within one questionnaire round they belonged to the category hybrid workers. This variable was used to visualize the working situation over time and for the GEE analyses.
Next to the ‘round-specific work situation’ variable, an ‘overall work situation’ was created. In this overall work situation variable, participants were categorized as home workers if they worked from home and did not work on location in all the available rounds during the year. Participants were categorized as location workers if they worked on location and did not work from home in all the available rounds. Participants were categorized as hybrid workers if they worked from home as well as on location in the available rounds during the year. The overall work situation variable was used in the descriptive statistics of our population, in the flowchart of selections and in the third sensitivity analysis in which continuous working from home was compared to hybrid working during the overall study period.
MSP
MSP was measured by questions that covered different body areas, including the following: lower back, upper back, and pain in the neck, shoulder(s) and/or arm(s). Questions used were derived from the somatization subscale of the Symptom Checklist (SCL-90) (Derogatis et al. 1977; Lifelines 2020). Up to and including the sixth round (March 30, 2020 – May 25, 2020) pain in lower back was assessed by the following question: ‘To what extent have you had the following symptoms in the last 7 days?’ and pain in the lower back followed as one of the symptoms. Respondents could answer on a five-point scale as follows: not at all (0), a little bit (1), somewhat (2), quite a lot (3), or very much (4). From round 7 onwards (May 15, 2020–March 25, 2021) the questionnaire was distributed bi-weekly, so 'the last 7 days' changed to 'the last 14 days’. From round 8 onwards, a question on pain in the upper back and another question on pain in the neck, shoulder(s) and/or arm(s) together were added using a similar question and a five-point answer scale.
Two types of outcome measures were created as follows: presence of pain and presence of severe pain. For the analyses on the presence of pain, the scorings per body area were dichotomized into ‘0 = no pain’ based on the first answer category ‘not at all’ and ‘1 = pain’ consisting of the categories ‘a little bit’ to ‘very much’ combined. In addition, a dichotomous variable ‘total MSP’ was created where 0 means no pain at all in any body area and 1 means the presence of at least a little bit of pain in one or more body areas. For the statistical analyses on severe pain, the scorings per body area if pain occurs were dichotomized into ‘0 = no severe pain’ based on the answer categories ‘not at all’ to ‘somewhat’ and ‘1 = severe pain’ consisting of the categories ‘quite a lot’ and ‘very much’.
Covariates
Several demographic covariates and work-related covariates were included as home workers and location workers are likely to differ with regard to their demographic characteristics and their jobs and corresponding work characteristics, as has been previously shown (Adams-Prassl et al. 2022). In addition, MSP may depend on the type of work and amount of physical strain (Lis et al. 2007). Sex, age (in years), educational attainment (low, middle or high), country of birth (within or outside The Netherlands) and household composition (‘living alone’, ‘living together with adults’, ‘living together with children’, ‘living together with children and adults’ or ‘living together but unknown with whom’) were included as demographic covariates. Occupational class (‘high-skilled white-collar’, ‘low-skilled white-collar’, ‘high-skilled blue collar’ and ‘low-skilled blue-collar’) and type of occupation (Appendix A, Table 5), both based on the International Standard Classification of Occupations (ISCO), and type of contract over the study period (‘exclusively a permanent contract’, ‘both a permanent and non-permanent contract’ and ‘exclusively a non-permanent contract’) were included as work covariates. Last, body mass index (BMI) was included, which may be related to MSP (Aro and Leino 1985; Kortt and Baldry 2002).
Statistical analyses
Descriptive analyses of the round-specific work situation were conducted to determine the amount of home working over the study period. Descriptive analyses separately for the three groups of overall work situation were conducted to get insight into the characteristics of our study population. Then, unadjusted graphs of trend lines were created to observe MSP over time for the different pain types, for the frequencies of the presence of MSP, as well as for the severity of MSP when pain occurs. To study the association between working from home and each dichotomized MSP outcome, data were analyzed with logistic generalized estimating equations (GEE) with an exchangeable correlation structure. For each outcome, we used the following three models: a crude model (model 0), a model adjusted for demographic variables (model 1) and a fully adjusted model (model 2) with additional adjustment for work variables and BMI. In these models, we used the round-specific work situation variable with location workers as reference group.
Finally, three sensitivity analyses were performed. First, to check if the association between working from home and MSP was confounded by workers’ general health, self-perceived general health was included as covariate in a subsample of the population (N = 33,411) (Hestbaek et al. 2003). General health was measured with the question ‘How would you rate your health, generally speaking?’ and dichotomized into ‘0 = poor general health’ based on the answer categories ‘poor’ and ‘fair’ and ‘1 = good general health’ consisting of the categories ‘good’, ‘very good’, and ‘excellent’. Home workers (95.2%) and hybrid workers (95.9%) reported to have a good general health somewhat less often than location workers (96.4%) (p < 0.05). Second, to test whether the results hold in a group which is relatively more homogeneous considering occupation, we conducted a sensitivity analysis among workers in business economics and administrative occupations (e.g. accountants, policy advisors, administrative officers, N = 9557). Third, in order to test whether the risks of MSP and/or severe MSP are higher when someone worked at home during all available rounds of the study period compared to also having worked occasionally on location, an analysis was performed using the overall working situation variable with overall hybrid working as reference group (N = 40,702 for lower back pain and N = 28,915 for upper back pain and pain in the neck/shoulder(s) and/or arm(s)). The software IBM SPSS 25 was used to conduct the analyses.
Results
Descriptive results of the study population
In the first questionnaire round, 44 percent of the participants worked exclusively from home. The percentage of the participants working from home decreased to 21 percent in September 2020 and increased again to 33 percent at end of the study period. Table 1 shows the characteristics of the workers: 58.7 percent were females, the mean age was 49 years and only a minority had a low educational level (13.0%). The largest differences in demographic variables by work situation were found in educational level (66.4% of home workers and 64.5% of hybrid workers had a high educational level compared to 24.2% of location workers) and occupational class (73.7% of home workers and 72.2% of hybrid workers were employed in high-skilled white-collar occupations compared to 42.7% of location workers).
Presence of MSP and presence of severe MSP during the first year of the pandemic
Figures 2 and 3 show the percentages of pain in the lower back and total MSP over time from March 2020–February 2021 by work situation. The presence of MSP followed a pattern with somewhat lower occurrences in May and August and a slight increase from August onwards to November. This pattern over time was very similar for each work situation. The presence of pain in the upper back and pain in the neck, shoulder(s) and/or arm(s) over time are shown in Figs. 5 and 6 in Appendix B. Similarly, the presence of upper back pain as well as the presence of pain in the neck, shoulder(s) and/or arm(s) showed a slight increase from August onwards to November without large differences between working situations.

Percentages of participants with pain in the lower back during the pandemic from April 2020 until February 2021, by work situation and date. N per round is, respectively, 24,210, 23,811, 23,418, 23,776, 22,286, 20,393, 20,661, 17,244, 16,435, 15,708, 16,564, 16,888, 15,774, 15,807, 14,575, 15,530

Percentages of participants with some MSP during the pandemic from June 2020 until February 2021, by work situation and date. N per round is respectively, 17,211, 16,402, 15,670, 16,537, 16,850, 15,761, 15,786, 14,561, 15,507
Figure 4 shows the severity of the pain in the lower back over time among location, home and hybrid workers reporting any pain (values of zero excluded). From the figure, it can be visually observed that the severity of pain in the lower back was quite stable over time and was quite similar for the three work situation groups, with a mean severity of 1.30 (on scale 1–4) over time. The mean severity of pain over time was 1.30 for those with upper back pain (Fig. 7 in Appendix B) and 1.36 for those with pain in the neck, shoulder(s) and/or arm(s) (Fig. 8 in Appendix B).

Severity of pain in the lower back during the pandemic from April 2020 until February 2021 among workers reporting any pain, by work situation and date. N per round is, respectively, 9645, 9399, 8708, 8386, 7640, 7029, 7316, 6046, 5632, 5655, 5464, 6166, 6312, 6041, 5272, 5693
Association between working from home and MSP
The GEE analyses showed that workers who worked from home had an increased risk of pain in all body areas compared to those working on location (Table 2). Working from home was associated with a higher risk of lower back pain [odds ratio (OR) = 1.05, 95% confidence interval (95% CI) 1.02–1.08], upper back pain (OR = 1.24, 95% CI 1.18–1.31) and pain in the neck, shoulder(s) and/or arm(s) (OR = 1.18, 95% CI 1.13–1.22) compared to working on location. For overall MSP, working from home was associated with a higher risk compared to working on location (OR = 1.12, 95% CI 1.08–1.17). In addition, workers who worked from home had an increased risk of relatively more severe pain in all body areas compared to workers who worked on location with ORs ranging from 1.18 to 1.31.
Except for pain in the lower back, hybrid workers also appeared to have an increased risk of MSP compared to location workers, with ORs varying from 1.09 to 1.14. In addition, workers who worked hybrid during the COVID-19 pandemic had an increased risk of severe pain in all body areas compared to those working on location (ORs varying from 1.12 to 1.32).
Sensitivity analyses on the association between working from home and MSP
First, including general health in the models confirmed the findings that workers who worked from home had an increased risk of pain in all body areas compared to those working on location during the COVID-19 pandemic with ORs varying from 1.04 to 1.22 (Table 3). The effect estimators on severe MSP became slightly smaller when controlling for general health, with only a significant association between working from home and severe pain in the lower back (OR = 1.13, 95% CI 1.04–1.23). Second, the extra sensitivity analysis on the presence of pain and presence of severe pain within the group workers in business economics and administrative occupations generally confirmed the results of the original analyses as well (Appendix C, Table 6). Third, the analyses in which continuous working from home was compared to hybrid working during the overall study period showed that workers who worked from home continuously were somewhat more likely to have MSP (OR = 1.06, 95% CI 1.02–1.11 for pain in the lower back, OR = 1.11, 95% CI 1.03–1.20 for pain in the upper back and OR = 1.09, 95% CI 1.03–1.15 for pain in the neck/shoulder(s) and/or arm(s)) and severe MSP in the lower back (OR = 1.15, 95% CI 1.03–1.29) (Appendix D, Table 7).
Discussion
The aim of the study was to investigate the longitudinal association between working from home during the COVID-19 pandemic and musculoskeletal pain. We studied musculoskeletal pain symptoms over a year period and found that, first, the trends of MSP over time were very similar for each working situation. Second, the results indicate that workers who worked from home during the COVID-19 pandemic had higher risks of having MSP in all body areas compared to workers who worked on location. For hybrid workers, there was some evidence towards having higher risks of MSP in the upper back and MSP in the neck, shoulder(s) and/or arm(s) in this period. Third, the results indicated that both home and hybrid workers have higher risks of relatively severe MSP in different body areas.
The results are in line with a previous study in Turkey which also found an association between working from home and MSP when comparing home workers with location workers (Toprak Celenay et al. 2020), but further studies on this subject appeared to be scarce. The effect estimators in this study were slightly higher for the presence of pain in the upper back and pain in the neck, shoulder(s) and/or arm(s) than for pain in the lower back. Other studies found that office workers with a high computer workload suffer particularly from pain in the upper part of the musculoskeletal system, more than pain in the lower back (Cho et al. 2012), and that inadequate workstation conditions (for example an inappropriate chair height or inadequate arm and back rest) mainly are linked to MSP in upper limbs (Rodrigues et al. 2017).
Controlling for general health did not produce substantial differences in the results, so it is not likely that the association between working from home and the presence of MSP was due to problems with workers’ general health. The odds ratios in the analyses on severe pain did not change in direction. Some odds ratios of severe pain, however, became insignificant when we adjusted for general health. Non-significant relationships may be explained by a smaller study population in this sensitivity analysis and the subsequently wider confidence intervals. The same holds for the second sensitivity analysis within the population of workers in business economics and administrative occupations. As a result, the greater likelihood of severe pain in the neck, shoulder(s) and/or arm(s) for homeworkers was no longer significant within this sensitivity analysis. We also looked at working from home continuously over the study period. The third sensitivity analysis indicated that workers who worked exclusively from home throughout the study period were somewhat more likely to have MSP than those who worked occasionally from home. There is thus some change in presence of MSP as the duration of work from home increases. Here, we made the assumption that workers who reported to work from home during all the questionnaire rounds in which they participated, did not work on location during time when they did not participate.
For future research it would be interesting to investigate whether or not the design of the home workstation is possibly an underlying mechanism which can explain MSP for homeworkers during the COVID-19 period. In the current study there was no information on the design of the home workstation available. In the beginning of the pandemic, workers were unprepared to work from home and the transition from working on location to working from home took place very rapidly because of the urgency of the COVID-19 pandemic. The quick transition to working from home may have resulted in unfavorable workstations and a lack of policies to support healthy home working environments. It is possible that there was too little space in the home for the home worker(s) and that home workers were forced to sit for long times in chairs and behind desks that were ergonomically unsuitable which increased home workers’ MSP. On the other hand, one would expect that improvements to the home office were made during the study period because of the persistent need to work from home (Oude Hengel et al. 2021). In that particular case, MSP would have decreased over time because working conditions at home were improved. However, the trend lines show no remarkable decrease, nor increase, in musculoskeletal pain symptoms over time. Therefore, other mechanisms may as well underlie the association between working from home and MSP. For example, previous studies suggest that home workers had reduced physical activity and prolonged sedentary behavior during the pandemic in comparison with before the pandemic (Fukushima et al. 2021; Loef et al. 2022), which in turn may have contributed to the development of MSP (Kastelic et al. 2018; Lim and Pranata 2021; Søgaard and Sjøgaard 2017). More research is needed to examine the interactions between these factors, and the contributions of these factors to the onset of MSP among home workers.
A limitation of this study is the lack of information about the work situation and MSP before the COVID-19 pandemic. We could not account for the work situation before the COVID-19 pandemic and if workers were already working from home at that time, the work situation before the COVID-19 pandemic may have affected the MSP of those workers during our study period. We also did not have information on baseline MSP measurements prior to the COVID-19 pandemic to see how many and which workers experienced MSP before the COVID-19 pandemic and the change in MSP during the COVID-19 pandemic. The lack of information on MSP before the COVID-19 pandemic may be problematic since previous results suggest that MSP of location and home workers may have declined somewhat during the COVID-19 pandemic (Oude Hengel et al. 2021). In addition, the measures of MSP during the COVID-19 pandemic were self-reported. Because the questions on MSP were about pain in the past 7 days, and later past 14 days, recall bias may exist and may also have increased. Last, we could not account for the number of hours worked, whereas we would expect that the time worked from home per week does matter for MSP. However, a major strength of the current study is its longitudinal design with multiple measurement of work situation and different pain types over almost one year in the COVID-19 pandemic. To our knowledge, the current study is the first study to report a longitudinal association between working from home and MSP.
Knowledge on the association between working from home and MSP during the COVID-19 pandemic may facilitate future policy making with the goal of improving the work situations for many workers who will continue to work from home (at least partly). Policies aimed at reducing MSP are relevant since the prevalence of MSP is associated with sleeping problems, overall fatigue and the mental well-being of workers (Safety et al. 2020). Which prevention measures are suitable does depend on which mechanisms are at play. In case that future research shows that the design of the workstation does matter, prevention measures for employers could for example be diffusion of simple and pragmatic messages on ergonomics and providing financial contributions to equipment (e.g., adjustable chairs) (Bouziri et al. 2020). However, it should also be recognized that appropriate equipment and adaptable furniture alone do not guarantee adequate usage. Workers could for example be trained to optimally set up their furniture or receive technical assistance with the installation (Montreuil and Lippel 2003). In addition, policy-makers could focus on providing simple practical risk assessment tools and guides for workers (Safety et al. 2020). In doing so, it could be of importance that physical activity is promoted and that prolonged sitting is interrupted. For example, the implementation of a software program which encourages workers to take regular breaks can help with the recovery of neck and upper extremity pain (Van den Heuvel et al. 2003). In our study, we adjusted for occupational class. In future studies, it is of importance to take into account job characteristics and psychosocial risk factors more extensively. For example, psychological distress, high workload and little influence over one's own work situation were found as predictors of MSP (Bongers et al. 2006; Eltayeb et al. 2007).
This longitudinal designed study showed that working from home conceivably has negative consequences on the musculoskeletal system. Working from home also has several advantages, for example a reduction in commuting time and improved opportunities to combine work and private life (De Macêdo et al. 2020). Therefore, working from home is expected to become more normal practice for many workers. Future policies should pay attention to the negative effects on workers’ MSP. Furthermore, future studies to the mechanisms are recommended as these can be starting points for measures to prevent MSP of home workers.
Data availability
The datasets analyzed during the current study are available from the Lifelines Cohort study (https://www.lifelines.nl/researcher) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Requests to access these data should be directed to Lifelines Research Office (research@lifelines.nl).
References
Adams-Prassl A, Boneva T, Golin M, Rauh C (2022) Work that can be done from home: evidence on variation within and across occupations and industries. Labour Econ 74:102083
Argus M, Pääsuke M (2021) Effects of the COVID-19 lockdown on musculoskeletal pain, physical activity, and work environment in Estonian office workers transitioning to working from home. Work 69(3):741–749. https://doi.org/10.3233/wor-210033
Aro S, Leino P (1985) Overweight and musculoskeletal morbidity: a ten-year follow-up. Int J Obes 9(4):267–275
Bongers P, Ijmker S, Van den Heuvel S, Blatter B (2006) Epidemiology of work related neck and upper limb problems: psychosocial and personal risk factors (part I) and effective interventions from a bio behavioural perspective (part II). J Occup Rehabil 16(3):272–295
Bouziri H, Smith DRM, Descatha A, Dab W, Jean K (2020) Working from home in the time of COVID-19: how to best preserve occupational health? Occup Environ Med 77(7):509–510. https://doi.org/10.1136/oemed-2020-106599
Cho C-Y, Hwang Y-S, Cherng R-J (2012) Musculoskeletal symptoms and associated risk factors among office workers with high workload computer use. J Manipulative Physiol Ther 35(7):534–540
De Macêdo TAM, Cabral E, Silva Castro WR, de Souza Junior CC, da Costa Junior JF, Pedrosa FM, da Silva AB, de Medeiros VRF, de Souza RP, Cabral MAL, Másculo FS (2020) Ergonomics and telework: a systematic review. Work 66(4):777–788. https://doi.org/10.3233/wor-203224
Derogatis LR, Lipman R, Covi L (1977). SCL-90 In Administration, scoring and procedures manual-I for the R (revised) version and other instruments of the Psychopathology Rating Scales Series. Johns Hopkins University School of Medicine. 1–4
Eltayeb S, Staal JB, Kennes J, Lamberts PH, de Bie RA (2007) Prevalence of complaints of arm, neck and shoulder among computer office workers and psychometric evaluation of a risk factor questionnaire. BMC Musculoskelet Disord 8(1):1–11
Fukushima N, Machida M, Kikuchi H, Amagasa S, Hayashi T, Odagiri Y, Takamiya T, Inoue S (2021) Associations of working from home with occupational physical activity and sedentary behavior under the COVID-19 pandemic. J Occup Health 63(1):e12212. https://doi.org/10.1002/1348-9585.12212
Hestbaek L, Leboeuf-Yde C, Manniche C (2003) Is low back pain part of a general health pattern or is it a separate and distinctive entity? A critical literature review of comorbidity with low back pain. J Manipulative Physiol Ther 26(4):243–252
Van den Heuvel SG, de Looze MP, Hildebrandt VH, Thé KH (2003) Effects of software programs stimulating regular breaks and exercises on work-related neck and upper-limb disorders. Scand J Work, Environ Health 29(2):106–116
Hooftman W, Oude Hengel K, Wiezer N, Bouwens L, Zoomer T, De Vroome E (2020) De impact van de COVID-19 crisis op werknemers. Stand van zaken na de eerste golf. TNO Leiden
Ipsen C, van Veldhoven M, Kirchner K, Hansen JP (2021) Six key advantages and disadvantages of working from home in Europe during COVID-19. Int J Environ Res Pub Health 18(4):1826
Kastelic K, Kozinc Ž, Šarabon N (2018) Sitting and low back disorders: an overview of the most commonly suggested harmful mechanisms. Coll Antropol 42(1):73–79
Kortt M, Baldry J (2002) The association between musculoskeletal disorders and obesity. Aust Health Rev 25(6):207–214. https://doi.org/10.1071/ah020207
Leroy S, Schmidt AM, Madjar N (2021) Working from home during COVID-19: A study of the interruption landscape. J Appl Psychol 106(10):1448–1465. https://doi.org/10.1037/apl0000972
Lifelines (2020). Symptoms Checklist SCL-90. Lifelines Wiki. http://wiki-lifelines.web.rug.nl/doku.php?id=symptoms_scl-90. Accessed 7 Dec 2021
Lifelines. (2021). Covid-19 questionnaires (COVQ). Lifelines Wiki. http://wiki-lifelines.web.rug.nl/doku.php?id=covq. Accessed 16 Dec 2021
Lim MA, Pranata R (2021) Sports activities during any pandemic lockdown. Irish J Med Sci 190(1):447–451
Lis AM, Black KM, Korn H, Nordin M (2007) Association between sitting and occupational LBP. Eur Spine J 16(2):283–298
Loef B, van Oostrom SH, van der Noordt M, Proper KI (2022) Working from home during the COVID-19 pandemic and its longitudinal association with physical activity and sedentary behavior. Scandinavian J Work, Environ Health. https://doi.org/10.5271/sjweh.4027
Lopez-Leon S, Forero DA, Ruiz-Díaz P (2020) Recommendations for working from home during the COVID-19 pandemic (and beyond). Work 66(2):371–375. https://doi.org/10.3233/wor-203187
Montreuil S, Lippel K (2003) Telework and occupational health: a Quebec empirical study and regulatory implications. Saf Sci 41(4):339–358
Oude Hengel K, In der Maur M, Bouwens L, De Vroome E, Hooftman W (2021) De impact van de COVID-19 pandemie op werknemers. Eind 2021. TNO Leiden
Rodrigues MSA, Leite RDV, Lelis CM, Chaves TC (2017) Differences in ergonomic and workstation factors between computer office workers with and without reported musculoskeletal pain. Work 57(4):563–572
Rodríguez-Nogueira Ó, Leirós-Rodríguez R, Benítez-Andrades JA, Álvarez-Álvarez MJ, Marqués-Sánchez P, Pinto-Carral A (2020) Musculoskeletal Pain and Teleworking in Times of the COVID-19: Analysis of the Impact on the Workers at Two Spanish Universities. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph18010031
Safety EAF, Work HA, Kok J, Vroonhof P, Snijders J, Roullis G, Clarke M, Peereboom K, Dorst P, Isusi I (2020) Work-related musculoskeletal disorders : prevalence, costs and demographics in the EU. Publ off. https://doi.org/10.2802/66947
Sijtsma A, Rienks J, van der Harst P, Navis G, Rosmalen JGM, Dotinga A (2021) Cohort Profile Update: Lifelines, a three-generation cohort study and biobank. Int J Epidemiol. https://doi.org/10.1093/ije/dyab257
Søgaard K, Sjøgaard G (2017) Physical activity as cause and cure of muscular pain: evidence of underlying mechanisms. Exerc Sport Sci Rev 45(3):136
Toprak Celenay S, Karaaslan Y, Mete O, Ozer Kaya D (2020) Coronaphobia, musculoskeletal pain, and sleep quality in stay-at home and continued-working persons during the 3-month Covid-19 pandemic lockdown in Turkey. Chronobiol Int 37(12):1778–1785. https://doi.org/10.1080/07420528.2020.1815759
Van Niekerk SM, Louw QA, Hillier S (2012) The effectiveness of a chair intervention in the workplace to reduce musculoskeletal symptoms. A Sys Rev BMC Musculoskelet Disord 13:145. https://doi.org/10.1186/1471-2474-13-145
Wahlström J (2005) Ergonomics, musculoskeletal disorders and computer work. Occup Med (lond) 55(3):168–176. https://doi.org/10.1093/occmed/kqi083
Acknowledgements
The authors wish to acknowledge the services of the Lifelines Cohort study, the contributing research centers delivering data to Lifelines, and all the study participants. The Lifelines initiative has been made possible by subsidy from the Dutch Ministry of Health, Welfare and Sport, the Dutch Ministry of Economic Affairs, the University Medical Center Groningen (UMCG), Groningen University, and the provinces in the north of the Netherlands (Drenthe, Friesland, Groningen).
Funding
This study was funded by the COVID-19 program of the Dutch Ministry of Health, Welfare and Sport that was conducted by the Dutch National Institute for Public Health and the Environment. The funding bodies had no role in the study design, the collection, analysis, and interpretation of data, the writing of the manuscript, and the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Data analyses were performed by EB and BL. The first draft of the manuscript was written by EB and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no conflicts of interest.
Protection of research participants
Approval of the Lifelines Cohort study was obtained from the Medical Ethics Committee of the University Medical Center Groningen, The Netherlands. Informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix A
Appendix B

Percentages of participants with pain in the upper back during the pandemic from June 2020 until February 2021, by work situation and date. N per round is respectively: 17,223, 16,409, 15,677, 16,547, 16,861, 15,770, 15,799, 14,574, 15,515

Percentages of participants with pain in the neck, shoulder(s) and/or arm(s) during the pandemic from June 2020 until February 2021, by work situation and date. N per round is respectively: 17,228, 16,421, 15,686, 16,552, 16,870, 15,771, 15,800, 14,575, 15,527

Severity of pain in the upper back during the pandemic from June 2020 until February 2021 among workers reporting any pain, by work situation and date. N per round is respectively: 1846, 1808, 1853, 1722, 2060, 2307, 2354, 2243, 2398

Severity of pain in the neck, shoulder(s) and/or arm(s) during the pandemic from June 2020 until February 2021 among workers reporting any pain, by work situation and date. N per round is respectively: 5349, 4982, 4924, 4789, 5406, 5889, 5855, 5145, 5557
Appendix C
See Table 6.
Appendix D
See Table 7
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bosma, E., Loef, B., van Oostrom, S.H. et al. The longitudinal association between working from home and musculoskeletal pain during the COVID-19 pandemic. Int Arch Occup Environ Health 96, 521–535 (2023). https://doi.org/10.1007/s00420-022-01946-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-022-01946-5