
Abstract
Aims
Impaired vision is an additional risk factor in elderly for falls. We investigated the hypothesis that treadmill (TM) walking affects visual function in both healthy elderly and those with early-moderate visual dysfunction due to glaucoma.
Methods
Thirty healthy controls (HC) aged 64–83 years and 18 glaucoma patients (GLA) aged 62–82 years participated in this cross-sectional study. The impact of TM-walking on visual function was assessed binocularly for (i) best-corrected visual acuity (BCVA) with and without crowding effect, (ii) contrast sensitivity (CS), and (iii) and visual field (mean deviation, VF-MD). Visual function was tested while participants were standing or during TM-walking for 2 speed conditions: (i) fast walking at their preferred speed and (ii) walking at a fixed speed of 3.5 km/h.
Results
GLA, most with early-moderate VF loss, performed equally well as HC. Independent of GROUP, an impact of SPEED on visual functions was statistically evident with large statistical effect size for (i) both types of BCVA with a mean loss of 0.02–0.05 logMAR (η2 = 0.41) and (ii) VF-MD with mean loss of 1 dB (η2 = 0.70), but not for CS.
Conclusions
Here, we introduce a paradigm for the assessment of visual function during walking. We provide proof-of-concept that our approach allows for the identification of walking induced visual function loss, i.e., a deterioration of BCVA and VF-sensitivity during TM-walking in both groups. It is therefore of promise for the investigation of the relation of vision impairment and mobility, ultimately the increased frequency of falls in advanced glaucoma.
Similar content being viewed by others
Avoid common mistakes on your manuscript.

Introduction
Glaucoma is a leading cause of irreversible blindness worldwide [1, 2]. The term glaucoma summarizes etiologically different disease mechanisms pointing to a common finding, i.e. chronic progressive optic neuropathy with loss of the retinal ganglion cells and corresponding visual field defects [3]. In fact, glaucomatous damage not only affects the eye, but also brain structure and function [4, 5] and leads to functional deficits such as impaired visuo-motor coordination [3]. Trivedi et al. also demonstrated impaired sensorimotor brain connectivity in early glaucoma that was correlated with a reduced balance performance [4]. It is plausible that these glaucoma related brain changes lead to impaired postural control and orientation [4, 6, 7], resulting in an increased incidence of falls [8, 9], which is a leading cause of injury-related death in patients [10].
Gait dysfunction and the risk of falling increase with age. For instance, one third of individuals > 65 years and almost half of people > 80 years fall at least once a year [11, 12]. Being a disease of late onset and age-related progression, glaucoma enhances the likelihood of falling, specifically due to risk factors such as impaired peripheral vision, orientation difficulties and the advanced age of affected individuals [10, 13]. Interestingly, visual function has been reported to be reduced during walking even for participants with healthy vision [14, 15], e.g., visual acuities are reduced during treadmill walking at 1.5 m/s in healthy controls [16].
Vision impairment does not only restrict the mobility of the affected individuals and increases the risk of falling, but also reduces quality of life in glaucoma patients [10, 17]. This motivates investigations to unravel the relation of glaucoma and visual function during gait. An important step for this purpose is the investigation of the effect of gait on visual function in both elderly healthy controls and patients with glaucoma.
In this study, we established a TM-walking paradigm to test the hypothesis that readouts of visual function were influenced by TM-walking in both elderly controls and in participants with glaucoma. We examined the effect of treadmill walking (TM-walking) on visual function by comparing best corrected visual acuity (VAS), crowding BCVA (VAC) [18], contrast sensitivity (CS) [19], and visual field sensitivity (VF-MD) between elderly participants (≥ 60 years) with healthy vision and with glaucoma. This might provide visual function parameters that are mostly affected during TM-walking and could be employed as sensitive biomarkers of the interaction of locomotion and visual perception.
Methods
Below included the essential descriptions of methods and for further details, please see supplementary. This study was approved by the Ethics Committee of the Otto-von-Guericke University of Magdeburg, Germany (registration number: 32/18).
Participants
Forty-eight participants [18 glaucoma patients (GLA) and 30 age- and sex-matched healthy controls (HC)] were recruited in this cross-sectional study.
No significant age difference was observed between GLA (mean age ± SEM: 71 ± 1 year) and HC (71 ± 1 year, p = 0.75).
For patient characterization, standard automated perimetry (SAP) was used to assess visual field sensitivities (mean deviation, VF-MD) and optical coherence tomography (OCT) scans were acquired to calculate the average peripapillary retinal nerve fiber layer thickness (pRNFL) and the averaged ganglion cell layer (GCL) and inner plexiform layer (IPL) volume.
Testing the impact of TM-walking on visual function
The primary aim of the study was to investigate visual function during TM-walking. For this purpose, the experimental setup was limited by two main challenges: (i) the use of testing-schemes that are compatible with a TM-walking setting and (ii) the problem of maintaining the viewing distance for vision testing during TM-walking. To overcome these issues, we (i) selected the appropriate soft- and hardware solutions for vision testing, i.e., the FrACT and Ocusweep®, and (ii) used a distance sensor ("Vivior® sensor").
The subsections below provide detailed descriptions of (a) the viewing distance estimation, (b) the general procedures for testing, and specific approaches for vision testing during TM-walking, i.e. for (c) visual acuity and contrast sensitivity testing, and (d) visual field testing.
-
(a)
Viewing distance estimation. Only the distance corrected values VAS/C were analyzed, see supplementary for further details. For the CS and VF measurements, no distance correction was applied due to the unavailability of Vivior readouts.
-
(b)
General procedure for testing (Fig. 1). In order to determine visual function during TM-walking, visual stimuli were presented to participants [1] during standing (S0) or [2] during TM-walking at two speeds: (i) fast walking at a individuals preferred speed (Sself), and (ii) at 3.5 km/h (S3.5). During each of these three conditions, a set of visual function tests were performed after an initial determination of Sself on the treadmill. Subsequent vision testing included two repetitions (ABC-ABC) of BCVA testing with and without crowding and CS testing, followed by one repetition of binocularly performed 24–2 VF testing. Prior to the series of measurements, one standard Ocusweep®-VF testing with a proximity sensor control and acoustic prompt for correction was conducted on the treadmill at rest to obtain a baseline value for binocular VF sensitivity (see supplementary Table 1). Total duration of BCVA, CS and VF testing was about 1:15 h.
-
(c)
Visual acuity and contrast sensitivity. BCVA and CS were determined binocularly for the three different speed conditions at a viewing distance of 5 m using FrACT [20], i.e. 8-alternative forced-choice (AFC), in a dimly-lit room. They were reported as logarithmized minimum angle of resolution (logMAR) and Weber contrast (logCS), respectively. BCVA was tested for two conditions, (i) without (VAS, a single optotype) and (ii) with crowding (VAC, an optotype surrounded by a circle ["©"]). The stimuli were presented on a 28" LED monitor (Samsung U28E590DSL, Dublin, Ireland) and calibrated with Data SpyderX Pro (Datacolor, New Jersey, USA).
-
(d)
Visual field sensitivity. A single repetition of 24–2 binocular VF testing was conducted for each of the three speed conditions with the Ocusweep™ Perimeter (Ocusweep SAP, Ocuspecto Ltd, Turku, Finland). This perimeter enabled testing without head or chin rest under ambient room light at 42.5 cm testing distance controlled via light and proximity sensors, respectively. For the test paradigm, the distance control had to be deactivated to allow for testing during TM-walking. The test stimuli, briefly appearing (100 ms) at different locations across the perimeter, comprised 9 LEDs arranged in a square (5.2 mm = 0.1 log unit smaller than Goldmann IV stimulus) enabling VF testing without refractive correction for near VA > 0.1 logMAR [21, 22]. The participants responded to the stimulus presentations via a remote control. The mean deviation (MD [dB]) was determined for visual field sensitivity assessment. In contrast to the Humphrey Field Analyzer, Ocusweep® uses positive instead of standard negative MD-values to indicate greater visual field loss. For one participant the visual field examination could not be performed for the S3.5 condition.

Measurement setup. You can see the treadmill with the safety belt, as well as the mirror through which the test person sees the monitor (on the right wall, here displaying the optotype for crowded VA). The Ocusweep® is attached to the left wall by means of a swivel arm (here 'parked' at the wall, with the back of the device visible). A camera (right) records the measurement
The effect of treadmill walking on systemic vascular parameters, namely the heart rate (pulse), was monitored with a wireless transmitter belt (POLAR Heart RateSensor H9) wrapped around the lower part of the chest coupled with the h/p/cosmos® treadmill setup (h/p/cosmos sports & medical gmbh, Germany). During TM-walking, both groups showed an increase of heart rate during Sself & S3.5 by 11 beats per minute (bpm) in comparison to baseline static (S0) measurements (a mean of 86 bpm), F(1,6, 75,4) = < 0.001.
Analysis and statistics
All statistical analysis and assumptions testing, e.g., normality tests, were performed with SPSS 28 (Statistical Package for the Social Sciences; IBM, Armonk, NY, USA) and included repeated measures analysis of variance (RM-ANOVA) for the within-subject factor SPEED and REPETITION and the between-subject factor GROUP as well as post-hoc analyses. Effect size was determined using eta-squared (η2) value and evaluated after Cohen, i.e., small (0.01), medium (0.06) and large effect (0.14) [23]. The significant p-values reported were corrected for multiple testing using Sidak correction for multiple testing. For further evaluation, the visual acuity loss was calculated by subtracting the results of the S3.5 condition from the S0 condition, e.g., VAS loss [logMAR] = VAS S0 [logMAR]—VAS S3.5 [logMAR].
Results
The sections below describe (a) the effect of TM-walking on viewing distance, a potentially confounding factor for BCVA testing and (b) representative examples for a qualitative overview. This is followed by group analyses of the effect of different TM-walking speeds on (c) the specific vision tests, i.e., VAS/C (corrected for distance variability), CS and VF and (d) visual function loss during TM-walking.
-
(a)
Impact of TM-walking speed on viewing distance. As described in methods, the Vivior® sensor allowed the measurement of the viewing distance during visual function measurements for the different speed conditions. In brief, the observed effects of different TM-walking speeds on viewing distance were small compared to the actual viewing distance, i.e., < 5% (16 cm/500 cm * 100%), see supplementary for further details.
-
(b)
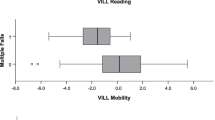
Representative examples. A representative data set of a HC and a GLA participant is given in Fig. 2 as an overview of the results obtained for the different visual function tests at the three speed conditions [S0, SSelf, S3.5]: (i) VAS and (ii) VAC, (iii) CS and (iv) VF. A deterioration of visual function during TM-walking was evident for both groups for VAS, VAC, and VF, but not for CS. This reflects the overall trend of changes induced by different TM-walking speeds on these visual function tests as detailed below.
-
(c)
Impact of TM-walking on visual function tests. TM-walking induced a comparable effect on the visual function in both groups, as shown in the following sections. A detailed listing of the statistical outcomes of the RM-ANOVAs are summarized in Table 1, i.e., specific factors, F-values, η2 and post-hoc tests.

Visual function tests for a HC and GLA for different speed conditions. During TM-walking (Sself & S3.5), BCVA, with (VAC) and without crowding (VAS), and VF-MD deteriorated in comparison to S0. VAS = visual acuity with a single optotype; VAC = visual acuity with crowding; CS = contrast sensitivity; VF-MD = visual field, mean deviation, S0 = static condition, SSelf = individual's tolerated fast TM-walking speed, S3.5 = 3.5 km/h
Visual acuity
Corrected BCVA of both groups deteriorated significantly during Sself (p < 0.001) and S3.5 (p < 0.001) compared to S0 by 0.048 ± 0.01 logMAR and 0.038 ± 0.01 logMAR, respectively. As expected, VAs was better than VAc across all speed conditions (p < 0.001) (Fig. 3A i, ii). There were no differences between groups for these measures that might be attributed to the largely early nature of damage in GLA.

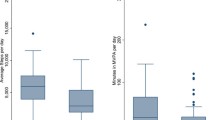
Impact of different TM-walking speeds on visual function tests. A BCVA. (i) & (ii) Effect of TM-walking speeds on BCVA (VAS – without crowding, VAC – with crowding); BCVA was worsened during TM-walking compared to standing. B Contrast sensitivity (CS). (i) Effect of TM-walking speed on CS; the CS did not change during TM-walking and the repetition effect reached only weak significance. (ii) Bland–Altman diagram of test–retest repeatability of the two repetitions for S0 demonstrates good reproducibility over both measurements. C Visual field (VF). (i) Effect of TM-walking on VF; reduced VF-sensitivities were evident during walking. BCVA = best corrected visual acuity, ICC = intraclass coefficient, further abbreviations: see Fig. 2
Contrast sensitivity
Unlike BCVA measures, CS was unaffected by TM-walking. There was a minor repetition effect (p = 0.035, see Fig. 3B i), which was not evident in the post-hoc analysis (p > 0.05). In addition, the relative intra-session reliability was high for both CS measurements repetitions indicated by the respective intraclass correlation coefficients (ICC) (S0: ICC = 0.90, SSelf: ICC = 0.82, S3.5: ICC = 0.87) (for S0: Fig. 3B ii).
Visual field
Similar to BCVA effects, TM-walking had a significant reductive effect on VF sensitivities, which did not differ between HC and GLA; VF-MD was reduced by 0.95 ± 0.08 dB for SSelf and 0.97 ± 0.08 dB for S3.5. As expected, VF-sensitivities were worse for the diseased group, GLA, compared to HC (significant group difference, p = 0.01), which was evident for all speed-conditions, i.e. S0, SSelf, S3.5 (Fig. 3C i).
-
(d)
Visual loss. For a comprehensive assessment of the effect of different TM-walking speeds on vision, one-sample t-tests were performed to assess visual function loss during TM-walking for each test [VAS, VAC, CS, VF] (Fig. 4). Visual loss was calculated by subtracting the test values for S3.5 from those for S0 and tested for the null hypothesis, i.e., no difference. During TM-walking, visual loss was highest for VAs (HC: p = 0.002, GLA: p = 0.001) and VF-MD (HC, GLA: p < 0.001) for both groups; VAS and VF-MD might, therefore, serve as highly sensitive biomarkers to investigate visual performance during TM-walking and consequently as surrogate biomarkers for falls’ tendency. VAc loss was significantly different from 0 only in HC (p = 0.012). There were no significant effects for CS (p > 0.05). Group differences for the visual loss were not evident for none of the tests (VAS, VAC, CS, VF; p > 0.05).
Fig. 4 
Visual loss associated with TM-walking.p-values not italicized: group difference. p-values in italics: difference from no loss, i.e., 0, for each group separately. Significant results are highlighted in bold. A VAS loss. B VAC loss. C CS loss. D VF-MD loss. Significant visual function loss was only evident for VAS, VAC in HC and VF and affected both groups similarly

Discussion
Summary of findings
This study, for the first time, addressed the effect of different TM-walking speeds on visual function of GLA in comparison to age-matched HC. We observed a deterioration of VAS/C and VF-MD during TM-walking compared to standing, but not for CS. Based on our findings, VAS and VF-MD might be potential surrogate biomarkers to identify or assess the risk for falls in GLA and elderly HC. Both HC and GLA demonstrated similar reduction in visual function during TM-walking without group differences, which might be attributed to the early-stage nature of damage in our GLA cohort.
Vision and gait: GLA vs HC
Vision loss, irrespective of the etiology, is a significant risk factor for falls [24, 25]. This risk is further increased due to diseases like glaucoma [26, 27]. However, the magnitude and the exact influence of glaucoma on the tendency to fall are not sufficiently elucidated. In this regard, the present study aimed to disentangle the effects of different TM-walking speeds on visual function in GLA compared to HC. To our knowledge, no previous studies have reported the impact of different TM-walking speeds on visual function in glaucoma, but the effect of TM-walking on BCVA has previously been investigated in healthy controls with the result of deteriorated BCVA with increasing speed [16, 28]. In fact, our finding of a significant decline of -0.05 ± 0.01 logMAR for VAS and -0.02 ± 0.01 logMAR for VAC at 3.5 km/h corresponds well to the results of Verbecque et al. (2018), who reported a visual loss of BCVA in elderly of the 7th (8th) decade during 3 km/h TM-walking of -0.02 (-0.05) logMAR and during 4 km/h of -0.02 (-0.08) logMAR. In addition, we demonstrated a significant decrease in VF-MD during TM-walking at 3.5 km/h by 1.0 ± 0.1 dB. Given that both groups performed equally during our measurements, it seems that elderly HC and those with GLA exhibit comparable visual function loss during TM-walking compared to standing.
Impairment of vision during TM-walking might imply an increased predisposition to falls in both diseased and healthy elderly groups, due to the relevance of vision for balance and navigation. In glaucoma, previous studies indicated the relevance of visual field loss for gait instability and predisposition to falls, e.g., faster rates of visual field loss were significantly associated with an increased incidence of falls in glaucoma [29]. Further, worse VF defects at baseline were associated with a stronger reduction of walking speeds in elderly glaucomatous participants and hence with gait dysfunction at the end of the follow-up period of 3 years [30]. There was a rapid decline of stride velocity per 5 dB decrease in the integrated binocular visual field sensitivity. Elderly individuals might also be prone to falls as the risk is increasing with aging [10, 12]. Accordingly, visual impairments are strongly associated with two or more falls in older adults. This association was previously reported to be related to reduced VA, VF, and impaired CS and presence of cataract in these individuals [27]. Further, in healthy elderly controls, poor visual performance during TM-walking might be attributed to variable gait patterns in comparisons to younger individuals. For instance, elderly individuals might have abnormal gait patterns, e.g., shorter stride length, affecting the head frequency (head movement per time), which might influence of visual function performance while walking [28, 31]. Further, a longitudinal follow-up of healthy elderly participants reported visual, auditory, vestibular, and brain changes that were correlated with gait and balance measures [32].
Outlook, clinical relevance and applications
The overall aim of this research is the evaluation of an multimodal exercise-based intervention program especially for glaucoma patients, similar to training programs that have already been shown to reduce the risk of falls in elderly persons [33, 34]. For this purpose, surrogate biomarkers of the intervention success, including those for visual function recovery, need to be identified. In the present study, we demonstrated that the approach presented is viable and that VAS and VF-MD have the potential to serve as biomarkers. Importantly, we demonstrated that in the range of glaucoma induced visual deficiencies of the present study (binocular MD range: 0 to 10), all patients were able to walk on a treadmill equally well as HC. This proof-of-concept encourages the use of the paradigm in a follow-up study in a cohort with more severe visual function deficits.
Limitations
Glaucoma is widely considered to be an undisputed risk factor for falls, although no greater effect of different TM-walking velocities on GLA compared to elderly HC was observed in the present study. There are several limitations that might have influenced our results. In our study, we mainly tested central vision and included mainly early-moderate stages of glaucoma. In follow-up studies, patients with the loss of the lower VF should be included, as that is considered a specific risk factor for falls [13, 35]. Lack of distance correction of CS and VF measurements is another limitation in this study. While the presented tread-mill-based approach has the benefit to of controlled walking parameters for better comparison amongst participants, it must be noted that the findings of this present study might not reflect physiological changes of visual function during walking indoors and outdoors. Further, we acknowledge that the reported decline of visual function during TM-walking might not be clinically significant, i.e., VF loss of 1 dB or VA loss of 0.02–0.05 logMAR, still it should be noted that the statistical effect size of the reported decline is large (see Methods), η2 = 0.4 and 0.7, respectively. Finally, our GLA cohort included only 18 patients due to recruitment difficulties during the corona pandemic and strict inclusion criteria. In conclusion, the extension of the study to a larger sample including more advanced disease stages would be of promise to uncover the effects of different TM-walking speeds on visual function in glaucoma covering a range of disease states.
Conclusion
In this study, we have found TM-walking to impair visual function for both GLA and HC. In both groups, the effect of TM-walking speed was most pronounced for VAS and VF-MD. Consequently, visual acuity and visual field sensitivity appear to be the most sensitive biomarkers to assess visual performance during locomotion, potentially gait control, and ultimately the risk of falls. At the individual level, these biomarkers might serve to identify persons with enhanced visual function loss during locomotion and thus increased risk of falls. In combination with interventions that address visual impairment related falls, these biomarkers promise readouts of intervention success. Intervention studies might benefit from the application of the TM-walking paradigm introduced in the present study in order to assess the impact of interventions, such as mobility training, on visual perception during locomotion and provide a quantitative readout of the success of therapy.
References
Jiang M-M, Zhou Q, Liu X-Y, Shi C-Z, Chen J, Huang X-H (2017) Structural and functional brain changes in early- and mid-stage primary open-angle glaucoma using voxel-based morphometry and functional magnetic resonance imaging. Medicine (Baltimore) 96(9):e6139
Haykal S, Jansonius NM, Cornelissen FW (2021) Progression of visual pathway degeneration in primary open-angle glaucoma: a longitudinal study. Front Hum Neurosci 15:630898
Zwierko T, Jedziniak W, Lesiakowski P, Śliwiak M, Kirkiewicz M, Lubiński W (2019) Eye-hand coordination impairment in glaucoma patients. Int J Environ Res Public Health 16(22):4332
Trivedi V, Bang JW, Parra C, Colbert MK, O’Connell C, Arshad A et al (2019) Widespread brain reorganization perturbs visuomotor coordination in early glaucoma. Sci Rep 9(1):14168
Williams AL, Lackey J, Wizov SS, Chia TMT, Gatla S, Moster ML et al (2013) Evidence for widespread structural brain changes in glaucoma: a preliminary voxel-based MRI study. Invest Ophthalmol Vis Sci 54(8):5880–5887
Dai H, Morelli JN, Ai F, Yin D, Hu C, Xu D et al (2013) Resting-state functional MRI: functional connectivity analysis of the visual cortex in primary open-angle glaucoma patients. Hum Brain Mapp 34(10):2455–2463
Demaria G, Invernizzi A, Ombelet D, Carvalho JC, Renken RJ, Cornelissen FW (2021) Binocular integrated visual field deficits are associated with changes in local network function in primary open-angle glaucoma: a resting-state fMRI study. Front Aging Neurosci 13:744139
Shabana N, Cornilleau-Pérès V, Droulez J, Goh JCH, Lee GSM, Chew PTK (2005) Postural stability in primary open angle glaucoma. Clin Exp Ophthalmol 33(3):264–273
de Luna RA, Mihailovic A, Nguyen AM, Friedman DS, Gitlin LN, Ramulu PY (2017) The association of glaucomatous visual field loss and balance. Transl Vis Sci Technol 6(3):8
Lee A, Lee K-W, Khang P (2013) Preventing falls in the geriatric population. Perm J 17(4):37–39
Patino CM, McKean-Cowdin R, Azen SP, Allison JC, Choudhury F, Varma R (2010) Central and peripheral visual impairment and the risk of falls and falls with injury. Ophthalmology 117(2):199-206.e1
Robert Koch-Institut. Gesundheit und Krankheit im Alter. Berlin; 2009. (Beiträge zur Gesundheitsberichterstattung des Bundes). Available from: URL: http://nbn-resolving.de/urn:nbn:de:0257-1002569
Dhital A, Pey T, Stanford MR (2010) Visual loss and falls: A review. Eye (Lond) 24(9):1437–1446
Peters BT, Mulavara AP, Cohen HS, Sangi-Haghpeykar H, Bloomberg JJ (2012) Dynamic visual acuity testing for screening patients with vestibular impairments. VES 22(2):145–151
Koyama S, Tanabe S, Hirakawa Y, Sakurai H, Kanada Y (2015) Effects of walking on bilateral differences in spatial attention control: a cross-over design. Arch Physiother 5:12
Deshpande N, Tourtillott BM, Peters BT, Bloomberg JJ (2013) Dynamic visual acuity (DVA) during locomotion for targets at near and far distances: effects of aging, walking speed and head-trunk coupling. J Vestib Res 23(4–5):195–201
Ong SR, Crowston JG, Loprinzi PD, Ramulu PY (2018) Physical activity, visual impairment, and eye disease. Eye (Lond) 32(8):1296–1303
Ogata NG, Boer ER, Daga FB, Jammal AA, Stringham JM, Medeiros FA (2019) Visual crowding in Glaucoma. Invest Ophthalmol Vis Sci 60(2):538–543
Bach M, Wesemann W, Kolling G, Bühren J, Krastel H, Schiefer U. Photopisches Kontrastsehen. Ortliche Kontrastempfindlichkeit. Der Ophthalmologe 2008; 105(1):46–8, 50–9
Bach M (1996) The freiburg visual acuity test-automatic measurement of visual acuity. Optom Vis Sci 73:49–53
Tigchelaar I, Leinonen MT. Reaction Time Perimetry in older glaucoma patients. Invest Ophthalmol Vis Sci 2020 [cited 2023 Apr 12]. Available from: https://iovs.arvojournals.org/article.aspx?articleid=2769129
Tigchelaar I, de Waard D, Jansonius NM, Leinonen MT (2022) Exploring the effect of glaucomatous visual field defects of current drivers on a neuropsychological test battery. Acta Ophthalmol 100(2):e463–e469
Cohen J (1988) Statistical power analysis for the behavioral sciences. Taylor and Francis, Hoboken. NJ
Hardwood RH (2001) Visual problems and falls. Age and Aging 30:13–18
Legood R, Scuffham P, Cryer C (2002) Are we blind to injuries in the visually impaired? A review of the literature. Inj Prev 8(2):155–160
Dolinis J, Harrison JE, Andrews GR (1997) Factors associated with falling in older Adelaide residents. Aust N Z J Public Health 21(5):462–468
Ivers RQ, Cumming RG, Mitchell P, Attebo K (1998) Visual impairment and falls in older adults: the Blue Mountains Eye Study. J Am Geriatr Soc 46(1):58–64
Verbecque E, van Criekinge T, Vanloot D, Coeckelbergh T, van de Heyning P, Hallemans A et al (2018) Dynamic Visual Acuity test while walking or running on treadmill: Reliability and normative data. Gait Posture 65:137–142
Baig S, Diniz-Filho A, Wu Z, Abe RY, Gracitelli CPB, Cabezas E et al (2016) Association of fast visual field loss with risk of falling in patients with Glaucoma. JAMA Ophthalmol 134(8):880–886
Jian-Yu E, Mihailovic A, Garzon C, Schrack JA, Li T, West SK et al (2021) Association between visual field damage and gait dysfunction in patients with Glaucoma. JAMA Ophthalmol 139(10):1053–1060
Guinand N, Pijnenburg M, Janssen M, Kingma H (2012) Visual acuity while walking and oscillopsia severity in healthy subjects and patients with unilateral and bilateral vestibular function loss. Arch Otolaryngol Head Neck Surg 138(3):301–306
Baloh RW, Ying SH, Jacobson KM (2003) A longitudinal study of gait and balance dysfunction in normal older people. Arch Neurol 60(6):835–839
Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH (2009) Interventions for preventing falls in elderly people. Cochrane Database Syst Rev (2):CD000340. https://doi.org/10.1002/14651858.CD000340.pub2
Tinetti ME (2003) Clinical practice. Preventing falls in elderly persons. N Engl J Med 348(1):42–9
Black AA, Wood JM, Lovie-Kitchin JE (2011) Inferior field loss increases rate of falls in older adults with glaucoma. Optom Vis Sci 88(11):1275–1282
Acknowledgements
We thank the study participants for their support of the study and DFG support.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was funded by German Research Foundation (DFG; Project: 423926179; HO-2002/20–1 & SCHE 1584/5–1. There was no rule of the funders in planning, conducting or reporting the current study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed involving human participants were in accordance with the ethical standards of the (Ethics Committee of the Otto-von-Guericke University of Magdeburg, Germany (registration number: 32/18) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consents were obtained from all participants.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Beyer, R., Al-Nosairy, K.O., Freitag, C. et al. Treadmill-walking impairs visual function in early glaucoma and elderly controls. Graefes Arch Clin Exp Ophthalmol (2024). https://doi.org/10.1007/s00417-024-06530-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00417-024-06530-w