
Abstract
Importance
The prevalence of multiple sclerosis (MS) and aging MS patients is increasing worldwide. There is a need to better understand this MS sub-population, which historically is underrepresented in the literature. This narrative review examines the evolving demographics, disease course, and treatments for older adults with MS (OAMS) to address current knowledge gaps and highlight areas critical for future research.
Observations
OAMS populations require special consideration by clinicians. Older individuals have different care needs than individuals with adult onset MS who are mid-life or younger. Comorbidities, an aging immune system, increasing neurodegeneration, decreasing neurologic reserve, changing benefit/risk relationship for disease modifying therapies (DMTs), and wellness require special attention to provide holistic comprehensive care. Active areas of research include potential cessation of DMTs and novel disease targets.
Conclusions and relevance
This review highlights both the current knowledge and information gaps in the literature that are critical to understanding and properly managing OAMS. The aims are to inform MS clinicians in their current practice, as well as inspire future studies which are critical to providing quality and evidence-based care for OAMS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic central nervous system (CNS) autoimmune disorder with clinical onset typically in young adults ages 20–40. As the world’s population ages and survival increases, there is an increasing number of older adults with MS (OAMS). It is estimated that 2.8 million people are living with MS worldwide, with peak prevalence in the United States (US) ages 55–64 years, followed by ages 65–74 [1, 2]. In the US, it is estimated that approximately 10% of people with MS are over age 65, with that proportion likely to grow [3]. This increasing MS prevalence and recognition in less common populations has seen rise to various MS definitions, including adult onset MS for patients diagnosed between ages 18 and 50, late-onset MS (LOMS), defined as MS diagnosis after age 50, and very late-onset MS (VLOMS) defined as MS diagnosis after age 60 [4].
In addition to these more recent trends, our understanding of MS pathophysiology continues to evolve. Over time, the biology that drives relapses and magnetic resonance imaging (MRI) lesion activity, focal inflammatory demyelination, tends to become less prominent, while the biology that drives progression, diffuse nonresolving compartmentalized inflammation and neurodegeneration, becomes more apparent [5]. This change has implications for MS treatment, particularly in the older MS populations, as the currently available disease modifying treatments (DMTs) are less efficacious with the shift in pathophysiology [6].
Medical comorbidities can further complicate making the correct disease diagnosis in LOMS, as well as influence disease course and treatment. These elements add additional layers of complexity in the OAMS population for the clinician to consider. In this review, we discuss the current evidence regarding demographics, disease course, treatment management, and special considerations for OAMS in comparison to their adult onset counterparts. PubMed was searched using the terms: ‘multiple sclerosis, MS, late-onset, older adults with MS’ with no time or language limitations. The authors independently selected and assessed the eligible articles based on this criteria. References within these articles were additionally evaluated and included as deemed relevant.
Epidemiology of MS in the older age group
The rising prevalence of MS has been noted worldwide, including individually in Canada, New Zealand, and US, among other regions [1, 7,8,9]. One large population cohort study in Manitoba demonstrated rising prevalence with relatively stable incidence of MS, which was interpreted to indicate decreased mortality in an aging population [7]. This is further supported by the observation that in recent decades MS patients’ life expectancy has increased, but still reduced compared to the general population, with suggested average reductions in lifespan of 6–10 years for patients with MS [10]. In other studies, the prevalence of MS patients age 65 and above has been estimated to be 10% in US and 18% in Italy [3, 11]. There is evidence of increasing diagnosis of MS over the age 60, with LOMS estimated to represent approximately 5% of cases [4, 12,13,14]. The reasons for these epidemiologic changes are likely multifactorial, including changes in global life expectancy, increasing access to health care, improved disease awareness and diagnosis, and evolving diagnostic criteria.
Age-related immunosenescence in MS
Immunosenescence, which has been defined as a “multifactorial and dynamic phenomenon that affects both natural and acquired immunity,” is part of the aging phenotype [15]. While a full characterization of molecular underpinnings is beyond the scope of this review, immunosenescence arises when an expansion of abnormal immune cell populations, both innate and adaptive, leads to impaired immune system function and resultant increased risk of infection and cancer [15]. Simultaneously, low-grade, sterile chronic inflammation, termed "inflammaging," emerges [16]. A reduced ability to generate effective immune responses against infections and vaccinations results, despite increased levels of inflammatory cytokines and activity of the innate immune system [15].
People with MS have premature immunosenescence and reduced immune function with accompanying premature aging markers, including telomere length reduction, iron accumulation, and increased oxidative stress [10, 17,18,19]. These markers are associated temporally with neurologic disability progression and are thought to contribute to gradual accrual of disease burden despite decreased frequency of relapses in later life [10]. Recent publications highlight epigenetic age acceleration, specifically in B-cells in people with MS [20]. Senolytics and regenerative strategies targeting these mechanisms may provide novel treatment opportunities [21, 22].
Disease behavior in older adults with MS
Historically, a progressive MS phenotype has been considered the most common presentation of patients with LOMS. However, recent studies highlight that a relapsing course is not uncommon. In one retrospective cohort analysis of 2261 patients with LOMS, primary progressive MS (PPMS) represented 26.7% of all cases, but relapsing remitting MS (RRMS) was still most common phenotype overall (66.4%) [23]. LOMS can continue to exhibit active focal inflammatory lesion activity despite a later onset [24]. CSF profiles, however, have shown less pleocytosis (34% in LOMS compared to 67% in adult onset MS) [25]. These factors should be considered when evaluating an older patient with suspicion of MS, as ultimately the spectrum and phenotype of MS disease in the older population can vary.
Brain volume loss also appears more significant in OAMS and LOMS. Brain tissue damage with parameters of brain parenchyma fraction and gray matter fraction were more advanced in LOMS when compared to an adult onset MS group [26]. This study also found lack of correlation between age and brain atrophy parameters and excluded patients with known vascular comorbidities. Both of these observations suggest that there are significant differences in brain atrophy between adult onset MS and LOMS patients, not solely due to age or comorbid microvascular ischemic disease. Aging MS patients accrue more diffuse brain atrophy, which can be manifested as ventricular expansion [27, 28]. Interestingly, a recent study examining apathy and its relation to caudate volume in OAMS versus controls found that lower caudate volumes were significantly associated with increased apathy in the OAMS group [29].
In terms of disease outcomes, population-based cohort studies have shown an association of later MS diagnosis with greater risk of disability progression [23, 30]. Disease course in LOMS has also shown faster progression to disability [13]. LOMS has been shown to have increased risk of reaching higher Expanded Disability Status Scale (EDSS) milestones. Thus, a better understanding disease course and management in the older age group is paramount [29].
Diagnosis
MS diagnosis in older populations can utilize the 2017 McDonald criteria, as in the more typical age range. Careful consideration of potential misdiagnosis, however, is of particular importance in the older population given some of the features that can differ in this group. Due to increased prevalence of comorbid conditions in OAMS, vascular risk factors (such as hypertension, hyperlipidemia, diabetes mellitus) leading to stroke and/or microvascular ischemic disease should be strongly considered in the differential of older patients with new neurologic symptoms or abnormal neuroimaging [31]. Spinal spondylosis (contributing to myelopathy), nutritional deficiencies (leading to a variety of manifestations), ophthalmic conditions (producing visual disturbances), and degenerative disorders (contributing to gait impairment or cognitive manifestations) are additional conditions that should be paid particular attention throughout evaluation.
In older MS populations, there is an association between accrual of spinal cord lesions with increasing disability progression [25, 32, 33]. Prevalence of myelopathy is higher in older populations in general, with 9.1% occurring in patients > 70 years of age, compared with 0.6% in patients < 20 years; additionally, recent studies confirm degenerative spine changes are present in most individuals after the 6th decade of life [34]. Spinal stenosis also may impact cord appearance, and a suggested association between segments of the spinal cord with moderate cervical stenosis and segments with MS lesions has been raised, as spinal segments with at least grade 2 stenosis were significantly associated with presence of an MS lesion in the same segment [35]. Careful attention must also be given to spinal cord imaging, as spondylotic myelopathy is one of the most common MS mimics in the aging patient (Fig. 1). Tumor and amyotrophic lateral sclerosis also warrant consideration [36]. An older age should not preclude consideration of a LOMS-related myelopathy if history and imaging are consistent, and conversely a myelopathic picture in an OAMS should not prevent consideration of other causes.

Degenerative disc disease changes co-occur with demyelinating lesions in patients with MS. Note demyelinating-related cord signal changes can arise at levels associated and not associated with structural spinal cord disease
Regarding brain imaging characteristics in the OAMS and LOMS populations, one should expect multifocal supratentorial and infratentorial lesions with similar demyelinating features as seen in other MS populations [25]. The clinician needs to be cognizant of chronic microvascular white matter changes, however, which increase in the older populations, particularly those with vascular risk factors. In a cohort of 338 MS patients, 41 (12%) were misdiagnosed, with cerebrovascular disease being the most common alternate diagnosis [37]. In this study, older age was found to be more common in misdiagnosed patients (odds ratio 1.2, 1.06–1.35, p = 0.003).
Disease therapy in older adults with MS
Most of the clinical trial data serving as the basis for regulatory approval of MS DMTs were obtained in patients younger than age 55 years, limiting generalizability beyond the 6th decade of life [10]. Many trials excluded patients > 45 years or > 50 years [38,39,40,41,42,43,44]. Limited observational data are available for some medications in both OAMS and LOMS. Ultimately, formal prospective studies are needed to ascertain risk/benefit of DMT use in OAMS accurately [45, 46]. Aging also can affect pharmacokinetics and pharmacodynamics of drugs, and, hence, inclusion of OAMS in formal studies of these pharmacologic parameters also are needed in the older population [47].
In addition to inadequate representation in clinical trials, OAMS often experience a progressive MS course, for which few treatment options are available. Targets for neurodegeneration and diffuse nonresolving inflammation that may drive progression are currently under research. The only regulatory-approved option for PPMS currently is ocrelizumab [48]. A number of other agents have been evaluated in PPMS and secondary progressive MS (SPMS), including interferons, glatiramer acetate, mitoxantrone, cladribine, fingolimod, and rituximab. Recommendations specifically for OAMS, whether progressive disease has overlaying inflammatory activity or not, are lacking [49, 50].
Therefore, use of currently available DMTs in OAMS requires balance of likelihood of benefit against risk, such as infection including progressive multifocal leukoencephalopathy (PML). The rate of seroconversion to John Cunningham virus is 10.8% per year and, therefore, risk increases with age [51]. In patients who were new to treatment with natalizumab, age was found to be a risk factor for natalizumab-related PML, as well as prior immunosuppressant use. Those over 50 years of age had a double in hazard ratio for earlier PML onset [52]. This elevated PML risk also might apply to OAMS treated with fingolimod [53].
Role of comorbidities to guide treatment selection
Comorbidities play an important role in MS treatment selection and, despite the paucity of data from RCTs, may be particularly critical when deciding on DMT in OAMS (Table 1) [54,55,56,57,58,59,60,61,62,63, –64]. As discussed below, there is increased risk of disability progression in patients with multiple comorbidities. Simultaneously, multi-drug regimens and DMT side effects could negatively impact this population, creating a paradoxical increased need for DMT given a more aggressive disease course and potential increased risk of deleterious side effects in patients with comorbidities. In one retrospective observational analysis, there was decreased likelihood of DMT initiation in patients with anxiety or ischemic heart disease [65]. There also was decreased likelihood of initiating a DMT as the number of comorbidities increased. Interestingly, there were opposite trends for patients with depression, as this subgroup was found to be 13% more likely to initiate DMT. While comorbidities are not unique to older patients, and a full review of comorbidities and interaction with all DMTs used for MS is beyond the scope of this review, we highlight several key circumstances to consider.
Vascular comorbidities, given their frequency, should be considered prior to DMT initiation. Sphingosine 1-phosphate receptor (S1PR) modulators are associated with cardiovascular adverse events (bradyarrhythmia and atrioventricular conduction slowing) with initiation of treatment and secondary hypertension, both of which may be of increased concern in OAMS [66]. Similarly, abnormal liver function tests, neutropenia, and hypertension were also reported as adverse events with teriflunomide in phase II and III studies [67].
Risk for infection should also be considered on a case-by-case basis and certain medications may increase risk more than others. Natalizumab, along with fingolimod and dimethyl fumarate, was associated with a 59% increased risk of infection related physician claims in a population-based study [68]. When assessed individually in this same study, natalizumab was the only DMT for which the increased infection risk was significant. Alemtuzumab carried higher risk of infection, malignancy, and mortality for patients over 45 years of age [69]. Cladribine has not been shown to be associated with increased risk of adverse events, including lymphopenia, in patients over 50 years compared with younger patients [70]. Intriguingly, when using ocrelizumab, age was not predictive of IgG levels below the lower limit of normal [71]. In an additional retrospective cohort study of 185 MS patients on ocrelizumab, older age was associated with reduced infection risk; 16% of these patients were > 55 years (mean age 43 years, SD 10.6). Younger age, longer MS disease duration, and increased EDSS score were associated with increased odds of antimicrobial use, with younger patients particularly more prone to upper respiratory infections [72].
Discontinuation of therapy
There is uncertainty regarding if and when to discontinue DMTs in OAMS. There is increased risk with DMTs with older age, but the tradeoff of risk versus benefit is not well established in OAMS, particularly with stable disease. Multiple cohort studies have addressed DMT discontinuation in OAMS. In one study, 216 patients were analyzed who discontinued DMT after treatment for at least 6 months, including 81 patients (37.5%) > 55 years old [73]. In the total cohort analysis, 32.9% patients with prior stable disease demonstrated new accumulation of disability after stopping DMT. This study, however, lacked a control group who were continued DMT, and OAMS represented a minority of studied population. In a population-based MS registry study, 132 “stoppers” of DMT for > 3 months and 366 “stayers” with DMT discontinuation < 3 months were analyzed with a median follow-up 6 years [74]. All patients analyzed were > 50 years of age. After propensity matching, there was no difference in risk of relapse or increase in EDSS between the two groups, although progression to EDSS 6.0 was 3.3 times greater in the “stopper” group (adjusted hazard ratio 3.29, 2.22–4.86, p < 0.0001).
DISCOMS was a multicenter, randomized, non-inferiority trial which sought to determine whether risk of disease activity is increased in MS patients age 55 years or older with no recent disease activity (defined as no MS relapse within 5 years or new MRI lesion within 3 years) who discontinue DMT compared to those who remain on DMT [75]. Participants who discontinued DMT were found to have a 7% higher rate of disease activity, either with new lesions on MRI or a relapse within 2 years, compared to those who continued DMT. There was no difference, however, in disability progression (11% in DMT continuation arm versus 12% in DMT discontinuation arm).
Other trials exploring DMT discontinuation are ongoing. While not specific to the OAMS population, DOT-MS (NCT04260711) is a clinical trial investigating discontinuation of DMTs in participants 18 years or older, with clinical and radiographic stability for 5 years. Preliminary data including 89 participants with average age in their early fifties showed that in the discontinuation arm 17.8% had notable new disease activity, 7 of which had signs of substantial MRI activity, defined as three or more new total lesions or two or more new lesions with active inflammation [76]. These findings ultimately lead to trial termination in March 2024, and participants will continue to be followed in an observational matter after restarting their previous DMT. STOP-I-SEP (NCT03653273) evaluates discontinuation of DMT in participants with SPMS age 50 or older and clinical and radiographic stability for 3 or more years.
With the above knowledge in hand, for MS patients who are 55 years of age or older and have been stable for 3–5 or more years on therapy, it is reasonable to discuss discontinuation of DMT, with counseling of associated risks. Despite lack of increased risk of relapse in cohort studies of participants over 60 years, in clinical practice some patients may prefer to remain on DMT. In our experience, the decision of DMT discontinuation must be made on an individualized basis.
Symptomatic treatment
In addition to decisions about DMT, there also is need for concomitant symptomatic management in many patients. There is currently limited research evaluating the benefits, risks, tolerability, and effects on quality of life of commonly used symptomatic treatments in the aging MS population. Despite this knowledge gap, symptomatic treatments remain an important part of management in OAMS. Careful risk/benefit evaluations must be applied when using oral medications, to which risk of drug–drug interactions and side effects may be elevated in the aging population depending on the agent. For instance, use of anticholinergics for detrusor hyperactivity from MS can exacerbate cognitive impairment, which may be of particular detriment in older patient populations given increased likelihood of dementias and MS-related cognitive changes [77]. In addition to medications, physical and occupational therapy are important components of MS care, particularly in older age groups who suffer from multifactorial gait instability or impairment of hand function. Awareness of patient comorbid conditions, for example osteoarthritis or heart failure, may limit some of patient’s capabilities in therapy from an MS standpoint.
Special considerations: comorbidities and the aging process in patients with MS
Comorbidities are relevant to both diagnosis and disease management in older patients. They are common; a study of patients with MS showed 44% of patients had comorbidities (cardiovascular, respiratory, musculoskeletal, diabetes, and others) [78]. Simultaneously, comorbidities may cloud the diagnostic picture. They may lead to delay in diagnosis, particularly in patients with LOMS, if MS plaques are mistaken for age- and comorbidity-related white matter hyperintensities on MRI as a result of microvascular disease, migraine, or if attributed to other CNS diseases when presenting with a neurologic complaint. Studies to validate the 2017 McDonald criteria were performed largely in patients under 50 years of age and, therefore, clinical and imaging manifestations related to comorbidities over the age of 50 were less represented [79]. Diagnostic delay has been shown to increase if obesity, smoking, or physical (vascular, autoimmune, musculoskeletal, gastrointestinal, visual) or mental comorbidities were present, even after stratifying by age of symptom onset (with the oldest category > 40 years) [80].
Further research on the interaction of comorbidities with MS over the lifespan is needed. Systematic review of comorbidities in patients with MS confirms many studies do not include the age distribution of the study population [81]. Other studies on comorbidities include age as a covariate when evaluating the impact of comorbidity on outcome, but do not report its significance or interactions. In general, studies of the impact of early and late-onset comorbidities in the OAMS population are still needed across vascular, musculoskeletal, cognitive, and psychiatric domains, as well as impact of hormonal fluctuations later in life for both male and female patients.
Vascular disease and vascular risk factors
There is an increased risk of ischemic heart disease, congestive heart failure, stroke, and peripheral vascular disease in the MS population compared with overall population [81]. The cause of this increase is not clear—it may be driven by smoking, obesity, low physical activity, or immune abnormalities related to the disease process itself. Conversely, diabetes, hypertension, heart disease, hyperlipidemia, and peripheral vascular disease, when present at any point in the lifespan, are associated with more rapid progression of disability in MS patients [82]. In a population of adults with MS diagnosed at mean age 38.2 (SD 9.5 years), time from diagnosis to ambulatory assistance was median 18.8 years in patients without and 12.8 years in patients with vascular comorbidities. Moreover, synergistic impact of comorbidities has been noted. Depression was associated with increased risk of vascular disease in people with MS, which may further compound risk of increased disability [83]. While further research is required to determine impact of treatment of vascular comorbidities on MS-related disability accrual, recent studies are encouraging. Higher cardiovascular risk as measured by the Framingham risk score is associated with risk of relapse, disability and DMT escalation over a 5-year follow-up [78]. Treatment with statins has been associated with lower all-cause mortality rates, as well as cerebrovascular and macrovascular disease, in people with MS compared with people with MS not taking lipid-lower medications [84].
Musculoskeletal conditions
Musculoskeletal comorbidities may uniquely predict physical ability in some studies. A study of patients with MS and musculoskeletal comorbidity showed a greater decline in physical function over 40 months compared to patients with MS without musculoskeletal comorbidity, controlling for age and MS disease severity [85]. Those with comorbidity were older (mean age 39.3 years, SD 9.6) versus those without (mean age 35.9 years, SD 9.5), though the impact specifically in older patients was not well examined, nor were specific musculoskeletal diagnoses provided.
Comorbidities causing cognitive impairment
Cognitive impairment is common in MS. It is more prevalent in adults with MS than in age-matched peers, and 77.4% of OAMS over the age of 55 years have impairment in more than two cognitive domains [86]. It can occur at any point in the disease and occurs across MS subtypes, including clinically isolated syndrome, relapsing, and progressive forms [87]. Its prevalence is highest in progressive forms of MS, though age and physical disability may mediate this increased risk rather than the disease subtype itself [87, 88]. Specific domains of cognitive dysfunction and their severity vary between patients, but affected domains may include recent memory, sustained attention, verbal fluency, conceptual reasoning, and visuospatial perception [87]. Risk of certain deficits may change with age, as older and middle-aged adults over 40 years of age demonstrate worse visuospatial learning and memory than young adults, while adults over 60 years of age display worse cognitive processing speed than younger and middle-aged adults [89]. Age of MS onset may impact trajectory of cognitive impairment, as patients with LOMS have similar levels of physical disability to patients with adult onset MS but worse cognitive disability, particularly in visual memory, auditory working memory, and memory, even after controlling for disease duration and comorbidities [90].
Additionally, as patients age, medical comorbidities may increase the risk of cognitive concerns. In a cohort comprised partially of OAMS (mean age 51.2 years), vascular comorbidity was associated with lower cognitive function in OAMS, mediated by changes in brain imaging [91]. Moreover, additional comorbid dementia syndromes (such as vascular dementia or Alzheimer’s disease [AD]) may emerge. In ICD code-based population studies, the risk of vascular dementia was 3.75-fold higher in patients with MS compared with matched controls [92]. Further studies investigating AD and other primary dementia syndromes in patients with MS are needed, though recent studies do emphasize an increased risk of AD in patients with MS [92, 93]. However, it remains unclear whether risk factors for dementia in the non-MS patients, such as ApoE4 alleles, confer similar or higher levels of risk for AD in patients with MS or impact MS disease course. In some studies, ApoE4 has been a prognosticator of a globally more aggressive MS course, including physical disability progression, though not necessarily associated with an increased risk of cognitive dysfunction [94,95,96]. Differentiation of MS-related cognitive changes from other causes is important, and screening for other common causes, including metabolic, infectious, and neurodegenerative conditions is warranted when new-onset cognitive complaints are noted.
Psychiatric comorbidities
At present, evidence-based guidelines do not consider age when screening for or treating psychiatric comorbidities in patients with MS [97]. However, OAMS may be especially at risk for undertreatment beginning in their mid-forties [97]. Depression and anxiety are the most common psychiatric comorbidities, with over 20% of patients affected and lifetime prevalence of 30–40%, depending on the measure used [81, 98,99,100,101]. Depression can occur at any age. When depression symptom scores of patients with MS over age 65 were compared with matched sample of young adults, OAMS reported fewer depressive symptoms than younger adults with MS [102]. However, MS-related helplessness was significantly higher in older compared to younger adults. Notably, in a cohort of patients with mean age of MS onset in their early 30 s, the prevalence of antidepressant use increased from 24.1% in 18–29-year-olds to 32.3% in patients over 60 years [103]. Prevalence of moderate to severe depression was 9.3% in 18- to 29-year-olds and fell to 7.8% in patients over 60.
Of note, psychiatric comorbidities heavily impact cognitive function in patients with MS. When present, severe depression causes changes in working memory, executive function, and reduced information processing speed (similar to those with severe depression without MS). This is particularly true for capacity-demanding tasks, with longer time and increased errors on planning tasks in patients with MS with depression [104, 105].
Anxiety tends to occur in younger patients and has been associated with shorter disease duration, though with notable overlap with depression [106]. Comorbid depression and anxiety lead to consistently low levels of psychological well-being and quality of life [107]. Anxiety has also been shown to impact processing speed [80]. Robust data on prevalence in adult onset MS are lacking.
Practical strategies for addressing psychiatric comorbidities include identifying anxiety, addressing substance use, and promoting increased social support to mitigate the impact of depression and anxiety. Transdiagnostic psychiatric treatment is appropriate when comorbidities are present [106].
Menopause
Approximately 30% of the MS population comprises women who are peri- or menopausal [108]. Age of menopause has not been found to differ in women with MS compared with the general population, with a mean age of around 51 years [108,109,110]. Symptoms of menopause can overlap those of MS, including changes in cognition, mood, bladder function, and sleep [109]. Some studies suggest reduced relapse rate and increased disability progression post-menopause, though systematic review of 28 studies generally did not find difference in disability accumulation pre- and post-menopause [111,112,113].
Little is known about the impact of hormonal replacement therapy (HRT) on MS disease course [108]. In the Comprehensive Longitudinal Investigation of MS at the Brigham and Women's Hospital (CLIMB) study, 16.2% of women had used estrogen HRT, either alone or in combination with progesterone within 5 years of menopause [110]. Use of HRT may be beneficial with regard to quality of life [114]. Smaller studies have shown tolerability of some hormonal therapies, but no large studies have examined risks/benefits in-depth for post-menopausal women with MS [115,116,117]. There are no studies at this time that guide DMT selection specifically with respect to pre- or post-menopausal state.
Wellness and preservation of neurological reserve in older populations
Wellness and preventative care are an important aspect of management in OAMS. These interventions are valuable at all ages, but are particularly relevant in older age.
Smoking is associated with accelerated brain atrophy and disability worsening in patients with RRMS and worsening long-term disability as measured on the Timed-25-Foot Walk and Paced Auditory Serial Addition Test [118]. Following smoking cessation, the rate of motor deterioration slows and eventually matches that in those who never smoked [119]. These observations emphasize the value of smoking cessation.
Exercise is another component to maximal health and has been proposed to be a disease-modifying intervention [120]. In a randomized cross-over trial of progressive resistance training in 35 adults (mean age 43 years), increased cortical thickness and radiographic changes after 24 weeks were noted [121]. While the precise mechanism is not known, physical training interventions in persons with MS improve vascular risk factors and may be considered as a therapeutic strategy for managing vascular comorbidities [122].
Social determinants of health are also critical and may play an increased role with aging. Economic components, including fixed income, race, isolation, transport, living environment, and lack of employment all need to be considered in the context of care for older MS patients [123]. Together, these may contribute to up to 55% of health outcomes.
Conclusion and future directions
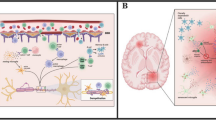
In this review, we highlight key considerations for comprehensive care of people with MS as they age (Fig. 2). Despite the increasing number of OAMS, research in diagnosis and management of this MS population is limited. Gaps in knowledge persist surrounding LOMS diagnosis, OAMS disease behavior, utility of DMTs, and management of comorbidities. Research that includes the impact of comorbidities on disease progression specifically in older patients would be useful, and ideally studies would report age of comorbidity onset, severity, and treatment status to clarify this relationship further. Clinical trials particularly have underrepresentation of the aging MS population. Inclusion of OAMS in future clinical trials should be a priority. Furthermore, efforts into continued MS epidemiologic studies remain paramount in order to better understand factors that influence MS development, pathophysiology, and disease course over time.

Special considerations in the older adult with MS
Data availability
Data availability statement is not applicable as this review article is based exclusively on published work.
References
Walton C, King R, Rechtman L et al (2020) Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler 26:1816–1821. https://doi.org/10.1177/1352458520970841
Wallin MT, Culpepper WJ, Campbell JD et al (2019) The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology 92:e1029–e1040. https://doi.org/10.1212/WNL.0000000000007035
Minden SL, Frankel D, Hadden LS et al (2004) Disability in elderly people with multiple sclerosis: an analysis of baseline data from the Sonya Slifka longitudinal multiple sclerosis study. NeuroRehabilitation 19:55–67
Naseri A, Nasiri E, Sahraian MA et al (2021) Clinical features of late-onset multiple sclerosis: a systematic review and meta-analysis. Mult Scler Relat Disord 50:102816. https://doi.org/10.1016/j.msard.2021.102816
Lublin FD, Häring DA, Ganjgahi H et al (2022) How patients with multiple sclerosis acquire disability. Brain 145:3147–3161. https://doi.org/10.1093/brain/awac016
Kuhlmann T, Moccia M, Coetzee T et al (2023) Multiple sclerosis progression: time for a new mechanism-driven framework. Lancet Neurol 22:78–88. https://doi.org/10.1016/S1474-4422(22)00289-7
Rotstein DL, Chen H, Wilton AS et al (2018) Temporal trends in multiple sclerosis prevalence and incidence in a large population. Neurology 90:e1435–e1441. https://doi.org/10.1212/WNL.0000000000005331
Alla S, Pearson J, Debernard L et al (2014) The increasing prevalence of multiple sclerosis in New Zealand. Neuroepidemiology 42:154–160. https://doi.org/10.1159/000358174
Dilokthornsakul P, Valuck RJ, Nair KV et al (2016) Multiple sclerosis prevalence in the United States commercially insured population. Neurology 86:1014–1021. https://doi.org/10.1212/WNL.0000000000002469
Vaughn CB, Jakimovski D, Kavak KS et al (2019) Epidemiology and treatment of multiple sclerosis in elderly populations. Nat Rev Neurol 15:329–342. https://doi.org/10.1038/s41582-019-0183-3
Solaro C, Ponzio M, Moran E et al (2015) The changing face of multiple sclerosis: prevalence and incidence in an aging population. Mult Scler 21:1244–1250. https://doi.org/10.1177/1352458514561904
Prosperini L, Lucchini M, Ruggieri S et al (2022) Shift of multiple sclerosis onset towards older age. J Neurol Neurosurg Psychiatry. https://doi.org/10.1136/jnnp-2022-329049
Polliack ML, Barak Y, Achiron A (2001) Late-onset multiple sclerosis. J Am Geriatr Soc 49:168–171. https://doi.org/10.1046/j.1532-5415.2001.49038.x
Tremlett H, Devonshire V (2006) Is late-onset multiple sclerosis associated with a worse outcome? Neurology 67:954–959. https://doi.org/10.1212/01.wnl.0000237475.01655.9d
Santoro A, Bientinesi E, Monti D (2021) Immunosenescence and inflammaging in the aging process: age-related diseases or longevity? Ageing Res Rev 71:101422. https://doi.org/10.1016/j.arr.2021.101422
Franceschi C, Capri M, Monti D et al (2007) Inflammaging and anti-inflammaging: a systemic perspective on aging and longevity emerged from studies in humans. Mech Ageing Dev 128:92–105. https://doi.org/10.1016/j.mad.2006.11.016
Thewissen M, Linsen L, Somers V et al (2005) Premature immunosenescence in rheumatoid arthritis and multiple sclerosis patients. Ann N Y Acad Sci 1051:255–262. https://doi.org/10.1196/ANNALS.1361.066
Stankiewicz JM, Neema M, Ceccarelli A (2014) Iron and multiple sclerosis. Neurobiol Aging 35(Suppl 2):S51–S58. https://doi.org/10.1016/j.neurobiolaging.2014.03.039
Miner AE, Graves JS (2021) What telomeres teach us about MS. Mult Scler Relat Disord 54:103084. https://doi.org/10.1016/j.msard.2021.103084
Maltby V, Xavier A, Ewing E et al (2023) Evaluation of cell-specific epigenetic age acceleration in people with multiple sclerosis. Neurology 101:e679–e689. https://doi.org/10.1212/WNL.0000000000207489
Adamczyk-Sowa M, Nowak-Kiczmer M, Jaroszewicz J, Berger T (2022) Immunosenescence and multiple sclerosis. Neurol Neurochir Pol 56:220–227. https://doi.org/10.5603/PJNNS.a2022.0045
Dema M, Eixarch H, Villar LM et al (2021) Immunosenescence in multiple sclerosis: the identification of new therapeutic targets. Autoimmun Rev 20:102893. https://doi.org/10.1016/j.autrev.2021.102893
Andersen MA, Buron MD, Magyari M (2021) Late-onset MS is associated with an increased rate of reaching disability milestones. J Neurol 268:3352–3360. https://doi.org/10.1007/s00415-021-10490-0
Bermel RA, Rae-Grant AD, Fox RJ (2010) Diagnosing multiple sclerosis at a later age: more than just progressive myelopathy. Mult Scler 16:1335–1340. https://doi.org/10.1177/1352458510377334
Kis B, Rumberg B, Berlit P (2008) Clinical characteristics of patients with late-onset multiple sclerosis. J Neurol 255:697–702. https://doi.org/10.1007/s00415-008-0778-x
Jasek Ł, Śmigielski J, Siger M (2020) Late onset multiple sclerosis—multiparametric MRI characteristics. Neurol Neurochir Pol 54:265–271. https://doi.org/10.5603/PJNNS.a2020.0036
Miller DH, Barkhof F, Frank JA et al (2002) Measurement of atrophy in multiple sclerosis: pathological basis, methodological aspects and clinical relevance. Brain 125:1676–1695. https://doi.org/10.1093/brain/awf177
Jakimovski D, Dujmic D, Hagemeier J et al (2020) Late onset multiple sclerosis is associated with more severe ventricle expansion. Mult Scler Relat Disord 46:102588. https://doi.org/10.1016/j.msard.2020.102588
Cote SE, Wagshul ME, Foley FW et al (2023) Caudate volume and symptoms of apathy in older adults with multiple sclerosis. Mult Scler 29:1266–1274. https://doi.org/10.1177/13524585231188096
Guillemin F, Baumann C, Epstein J et al (2017) Older age at multiple sclerosis onset is an independent factor of poor prognosis: a population-based cohort study. Neuroepidemiology 48:179–187. https://doi.org/10.1159/000479516
Martinelli V, Rodegher M, Moiola L, Comi G (2004) Late onset multiple sclerosis: clinical characteristics, prognostic factors and differential diagnosis. Neurol Sci 25(Suppl 4):S350–S355. https://doi.org/10.1007/s10072-004-0339-8
Tsagkas C, Magon S, Gaetano L et al (2019) Preferential spinal cord volume loss in primary progressive multiple sclerosis. Mult Scler 25:947–957. https://doi.org/10.1177/1352458518775006
Schlaeger R, Papinutto N, Zhu AH et al (2015) Association between thoracic spinal cord gray matter atrophy and disability in multiple sclerosis. JAMA Neurol 72:897–904. https://doi.org/10.1001/jamaneurol.2015.0993
Tetreault L, Goldstein CL, Arnold P et al (2015) Degenerative cervical myelopathy: a spectrum of related disorders affecting the aging spine. Neurosurgery 77(Suppl 4):S51-67. https://doi.org/10.1227/NEU.0000000000000951
Gratch D, Do D, Khankhanian P et al (2020) Impact of cervical stenosis on multiple sclerosis lesion distribution in the spinal cord. Mult Scler Relat Disord 45:102415. https://doi.org/10.1016/j.msard.2020.102415
Young WF (2000) Cervical spondylotic myelopathy: a common cause of spinal cord dysfunction in older persons. Am Fam Physician 62(1064–70):1073
Wang Y, Bou Rjeily N, Koshorek J et al (2023) Clinical and radiologic characteristics associated with multiple sclerosis misdiagnosis at a tertiary referral center in the United States. Mult Scler 29:1428–1436. https://doi.org/10.1177/13524585231196795
Kappos L, Radue E-W, O’Connor P et al (2010) A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med 362:387–401. https://doi.org/10.1056/NEJMOA0909494/SUPPL_FILE/NEJMOA0909494_DISCLOSURES.PDF
Polman CH, O’Connor PW, Havrdova E et al (2006) A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med 354:899–910. https://doi.org/10.1056/NEJMOA044397/SUPPL_FILE/NEJM_POLMAN_899SA1.PDF
Hutchinson M, Kappos L, Calabresi PA et al (2009) The efficacy of natalizumab in patients with relapsing multiple sclerosis: subgroup analyses of AFFIRM and SENTINEL. J Neurol 256:405–415. https://doi.org/10.1007/S00415-009-0093-1
Confavreux C, O’Connor P, Comi G et al (2014) Oral teriflunomide for patients with relapsing multiple sclerosis (TOWER): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol 13:247–256. https://doi.org/10.1016/S1474-4422(13)70308-9
Rudick RA, Stuart WH, Calabresi PA et al (2006) Natalizumab plus interferon beta-1a for relapsing multiple sclerosis. N Engl J Med 354:911–923. https://doi.org/10.1056/NEJMOA044396/SUPPL_FILE/NEJM_RUDICK_911SA1.PDF
Devonshire V, Havrdova E, Radue EW et al (2012) Relapse and disability outcomes in patients with multiple sclerosis treated with fingolimod: subgroup analyses of the double-blind, randomised, placebo-controlled FREEDOMS study. Lancet Neurol 11:420–428. https://doi.org/10.1016/S1474-4422(12)70056-X
Bar-Or A, Gold R, Kappos L et al (2013) Clinical efficacy of BG-12 (dimethyl fumarate) in patients with relapsing-remitting multiple sclerosis: subgroup analyses of the DEFINE study. J Neurol 260:2297–2305. https://doi.org/10.1007/S00415-013-6954-7
Patti F, Penaherrera JN, Zieger L, Wicklein E-M (2021) Clinical characteristics of middle-aged and older patients with MS treated with interferon beta-1b: post-hoc analysis of a 2-year, prospective, international, observational study. BMC Neurol 21:324. https://doi.org/10.1186/s12883-021-02347-w
Shirani A, Zhao Y, Petkau J et al (2015) Multiple sclerosis in older adults: the clinical profile and impact of interferon beta treatment. Biomed Res Int. https://doi.org/10.1155/2015/451912
Mangoni AA, Jackson SHD (2004) Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol 57:6–14. https://doi.org/10.1046/j.1365-2125.2003.02007.x
Lin M, Zhang J, Zhang Y et al (2022) Ocrelizumab for multiple sclerosis. Cochrane Database Syst Rev 5:CD013247. https://doi.org/10.1002/14651858.CD013247.pub2
Kappos L, Bar-Or A, Cree BAC et al (2018) Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet 391:1263–1273. https://doi.org/10.1016/S0140-6736(18)30475-6
Macaron G, Cohen JA (2018) Integrating multiple sclerosis guidelines into practice. Lancet Neurol 17:658–660. https://doi.org/10.1016/S1474-4422(18)30248-5
Schwab N, Schneider-Hohendorf T, Hoyt T et al (2018) Anti-JCV serology during natalizumab treatment: review and meta-analysis of 17 independent patient cohorts analyzing anti-John Cunningham polyoma virus sero-conversion rates under natalizumab treatment and differences between technical and biological sero-converters. Mult Scler 24:563–573. https://doi.org/10.1177/1352458517728814
Prosperini L, Scarpazza C, Imberti L et al (2017) Age as a risk factor for early onset of natalizumab-related progressive multifocal leukoencephalopathy. J Neurovirol 23:742–749. https://doi.org/10.1007/s13365-017-0561-9
Berger JR, Cree BA, Greenberg B et al (2018) Progressive multifocal leukoencephalopathy after fingolimod treatment. Neurology 90:e1815–e1821. https://doi.org/10.1212/WNL.0000000000005529
Bayer HealthCare Pharmaceuticals (2024) Betaseron (interferon beta-1b) [package insert]. Bayer Healthcare website. Revised July 2023. Accessed 29 Mar 2024. https://labeling.bayerhealthcare.com/html/products/pi/Betaseron_PI.pdf
TEVA Pharmaceuticals (2024) Copaxone (glatiramer acetate) [package insert]. U.S. Food and drug administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020622s057lbl.pdf. Revised February 2009. Accessed 29 Mar 2024
Sanofi Pharmaceuticals (2024) Aubagio (teriflunomide) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/202992s000lbl.pdf. Revised September 2012. Accessed 28 Mar 2024
Novartis Pharmaceuticals Corporation (2024) Gilenya (fingolimod) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/022527s006lbl.pdf. Revised March 2012. Accessed 28 Mar 2024
Celgene Corporation (2024) Zeposia (ozanimod) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/209899s000lbl.pdf. Revised March 2020. Accessed 29 Mar 2024
Novartis Pharmaceuticals (2024) Mayzent (siponimod) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/209884s000lbl.pdf. Revised March 2019. Accessed 29 Mar 2024
Biogen (2024) Tecfidera (dimethyl fumarate) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/204063lbl.pdf. Revised March 2024. Accessed 29 Mar 2024
Genentech (2024) Ocrevus (ocrelizumab) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761053s012lbl.pdf. Revised November 2018. Accessed 29 Mar, 2024
Biogen (2024) Tysabri (natalizumab) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/125104s283lbl.pdf. Revised December 2009. Accessed 29 Mar 2024
EMD Serono (2024) Mavenclad (cladribine) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/022561s000lbl.pdf. Revised March 2019. Accessed 28 Mar 2024
Genzyme Corporation (2024) Lemtrada (alemtuzumab) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/103948s5182lbl.pdf. Revised April 2021. Accessed 29 Mar 2024
Zhang T, Tremlett H, Leung S et al (2016) Examining the effects of comorbidities on disease-modifying therapy use in multiple sclerosis. Neurology 86:1287. https://doi.org/10.1212/WNL.0000000000002543
Zhao Z, Lv Y, Gu Z-C et al (2021) Risk for cardiovascular adverse events associated with sphingosine-1-phosphate receptor modulators in patients with multiple sclerosis: insights from a pooled analysis of 15 randomised controlled trials. Front Immunol 12:795574. https://doi.org/10.3389/fimmu.2021.795574
Miller AE (2015) Teriflunomide: a once-daily oral medication for the treatment of relapsing forms of multiple sclerosis. Clin Ther 37:2366–2380. https://doi.org/10.1016/j.clinthera.2015.08.003
Wijnands JMA, Zhu F, Kingwell E et al (2018) Disease-modifying drugs for multiple sclerosis and infection risk: a cohort study. J Neurol Neurosurg Psychiatry 89:1050–1056. https://doi.org/10.1136/jnnp-2017-317493
Bass AD, Arroyo R, Boster AL et al (2021) Alemtuzumab outcomes by age: post hoc analysis from the randomized CARE-MS studies over 8 years. Mult Scler Relat Disord 49:102717. https://doi.org/10.1016/j.msard.2020.102717
Disanto G, Moccia M, Sacco R et al (2022) Monitoring of safety and effectiveness of cladribine in multiple sclerosis patients over 50 years. Mult Scler Relat Disord. https://doi.org/10.1016/J.MSARD.2022.103490
Hauser SL, Kappos L, Montalban X et al (2021) Safety of ocrelizumab in patients with relapsing and primary progressive multiple sclerosis. Neurology 97:e1546–e1559. https://doi.org/10.1212/WNL.0000000000012700
Seery N, Sharmin S, Li V et al (2021) Predicting infection risk in multiple sclerosis patients treated with ocrelizumab: a retrospective cohort study. CNS Drugs 35:907–918. https://doi.org/10.1007/s40263-021-00810-3
Jakimovski D, Kavak KS, Vaughn CB et al (2022) Discontinuation of disease modifying therapies is associated with disability progression regardless of prior stable disease and age. Mult Scler Relat Disord 57:103406. https://doi.org/10.1016/j.msard.2021.103406
Kaminsky A-L, Omorou AY, Soudant M et al (2020) Discontinuation of disease-modifying treatments for multiple sclerosis in patients aged over 50 with disease inactivity. J Neurol 267:3518–3527. https://doi.org/10.1007/s00415-020-10029-9
Corboy JR, Fox RJ, Kister I et al (2023) Risk of new disease activity in patients with multiple sclerosis who continue or discontinue disease-modifying therapies (DISCOMS): a multicentre, randomised, single-blind, phase 4, non-inferiority trial. Lancet Neurol 22:568–577. https://doi.org/10.1016/S1474-4422(23)00154-0
Coerver EFWBJ et al (2024) Patient-reported outcomes in discontinuation of first-line disease-modifying therapy in stable multiple sclerosis (DOT-MS): results of a multicenter randomized controlled trial. Presented at: ECTRIMS Milan; October 11–13 2023, Milan, Italy
Risacher SL, McDonald BC, Tallman EF et al (2016) Association between anticholinergic medication use and cognition, brain metabolism, and brain atrophy in cognitively normal older adults. JAMA Neurol 73:721–732. https://doi.org/10.1001/jamaneurol.2016.0580
Petruzzo M, Reia A, Maniscalco GT et al (2021) The Framingham cardiovascular risk score and 5-year progression of multiple sclerosis. Eur J Neurol 28:893–900. https://doi.org/10.1111/ene.14608
Thompson AJ, Banwell BL, Barkhof F et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17:162–173. https://doi.org/10.1016/S1474-4422(17)30470-2
Marrie RA, Horwitz R, Cutter G et al (2009) Comorbidity delays diagnosis and increases disability at diagnosis in MS. Neurology 72:117–124. https://doi.org/10.1212/01.wnl.0000333252.78173.5f
Marrie RA, Cohen J, Stuve O et al (2015) A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: overview. Mult Scler 21:263–281. https://doi.org/10.1177/1352458514564491
Marrie RA, Rudick R, Horwitz R et al (2010) Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology 74:1041–1047. https://doi.org/10.1212/WNL.0b013e3181d6b125
Palladino R, Chataway J, Majeed A, Marrie RA (2021) Interface of multiple sclerosis, depression, vascular disease, and mortality: a population-based matched cohort study. Neurology 97:E1322–E1333. https://doi.org/10.1212/WNL.0000000000012610
Palladino R, Marrie RA, Majeed A, Chataway J (2020) Evaluating the risk of macrovascular events and mortality among people with multiple sclerosis in England. JAMA Neurol 77:820–828. https://doi.org/10.1001/JAMANEUROL.2020.0664
Dallmeijer AJ, Beckerman H, de Groot V et al (2009) Long-term effect of comorbidity on the course of physical functioning in patients after stroke and with multiple sclerosis. J Rehabil Med 41:322–326. https://doi.org/10.2340/16501977-0335
Branco M, Ruano L, Portaccio E et al (2019) Aging with multiple sclerosis: prevalence and profile of cognitive impairment. Neurol Sci 40:1651–1657. https://doi.org/10.1007/s10072-019-03875-7
Rao SM, Leo GJ, Bernardin L, Unverzagt F (1991) Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology 41:685–691. https://doi.org/10.1212/WNL.41.5.685
Ruano L, Portaccio E, Goretti B et al (2017) Age and disability drive cognitive impairment in multiple sclerosis across disease subtypes. Mult Scler 23:1258–1267. https://doi.org/10.1177/1352458516674367
Baird JF, Cederberg KLJ, Morghen Sikes E et al (2019) Changes in cognitive performance with age in adults with multiple sclerosis. Cogn Behav Neurol 32:201–207. https://doi.org/10.1097/WNN.0000000000000200
Butler Pagnotti R, Hua LH, Miller JB (2022) Cognition and disease characteristics in adult onset versus late onset multiple sclerosis. Mult Scler J 28:933–941. https://doi.org/10.1177/13524585211039112
Marrie RA, Patel R, Figley CR et al (2022) Effects of vascular comorbidity on cognition in multiple sclerosis are partially mediated by changes in brain structure. Front Neurol 13:910014. https://doi.org/10.3389/fneur.2022.910014
Bin CE, Jung SY, Jung JH et al (2023) The risk of dementia in multiple sclerosis and neuromyelitis optica spectrum disorder. Front Neurosci 17:1214652. https://doi.org/10.3389/FNINS.2023.1214652/FULL
Luczynski P, Laule C, Hsiung G-YR et al (2019) Coexistence of multiple sclerosis and Alzheimer’s disease: a review. Mult Scler Relat Disord 27:232–238. https://doi.org/10.1016/j.msard.2018.10.109
Masterman T, Zhang Z, Hellgren D et al (2002) APOE genotypes and disease severity in multiple sclerosis. Mult Scler 8:98–103. https://doi.org/10.1191/1352458502ms787oa
Ghaffar O, Reis M, Pennell N et al (2010) APOE epsilon4 and the cognitive genetics of multiple sclerosis. Neurology 74:1611–1618. https://doi.org/10.1212/WNL.0b013e3181e074a7
Engel S, Graetz C, Salmen A et al (2020) Is APOE ε4 associated with cognitive performance in early MS? Neurol(R) Neuroimmunol Neuroinflamm 7:e278. https://doi.org/10.1212/NXI.0000000000000728
Minden SL, Feinstein A, Kalb RC et al (2014) Evidence-based guideline: assessment and management of psychiatric disorders in individuals with MS: report of the guideline development subcommittee of the American academy of neurology. Neurology 82:174–181. https://doi.org/10.1212/WNL.0000000000000013
Marrie RA, Fisk JD, Tremlett H et al (2015) Differences in the burden of psychiatric comorbidity in MS vs the general population. Neurology 85:1972–1979. https://doi.org/10.1212/WNL.0000000000002174
Marrie RA, Patten SB, Tremlett H et al (2016) Sex differences in comorbidity at diagnosis of multiple sclerosis: a population-based study. Neurology 86:1279–1286. https://doi.org/10.1212/WNL.0000000000002481
Boeschoten RE, Braamse AMJ, Beekman ATF et al (2017) Prevalence of depression and anxiety in multiple sclerosis: a systematic review and meta-analysis. J Neurol Sci 372:331–341. https://doi.org/10.1016/j.jns.2016.11.067
Patten SB, Marrie RA, Carta MG (2017) Depression in multiple sclerosis. Int Rev Psychiatry 29:463–472. https://doi.org/10.1080/09540261.2017.1322555
Kneebone II, Dunmore EC, Evans E (2003) Symptoms of depression in older adults with multiple sclerosis (MS): comparison with a matched sample of younger adults. Aging Ment Health 7:182–185. https://doi.org/10.1080/1360786031000101148
Chan CK, Tian F, Pimentel Maldonado D et al (2021) Depression in multiple sclerosis across the adult lifespan. Mult Scler 27:1771–1780. https://doi.org/10.1177/1352458520979304
Arnett PA, Higginson CI, Randolph JJ (2001) Depression in multiple sclerosis: relationship to planning ability. J Int Neuropsychol Soc 7:665–674. https://doi.org/10.1017/s1355617701766027
Arnett PA, Higginson CI, Voss WD et al (1999) Depressed mood in multiple sclerosis: relationship to capacity-demanding memory and attentional functioning. Neuropsychology 13:434–446. https://doi.org/10.1037//0894-4105.13.3.434
Hanna M, Strober LB (2020) Anxiety and depression in multiple sclerosis (MS): antecedents, consequences, and differential impact on well-being and quality of life. Mult Scler Relat Disord 44:102261. https://doi.org/10.1016/j.msard.2020.102261
Beiske AG, Svensson E, Sandanger I et al (2008) Depression and anxiety amongst multiple sclerosis patients. Eur J Neurol 15:239–245. https://doi.org/10.1111/j.1468-1331.2007.02041.x
Bove R, Okai A, Houtchens M et al (2021) Effects of menopause in women with multiple sclerosis: an evidence-based review. Front Neurol 12:554375. https://doi.org/10.3389/fneur.2021.554375
Bove R, Healy BC, Secor E et al (2015) Patients report worse MS symptoms after menopause: findings from an online cohort. Mult Scler Relat Disord 4:18–24. https://doi.org/10.1016/j.msard.2014.11.009
Bove R, Healy BC, Musallam A et al (2016) Exploration of changes in disability after menopause in a longitudinal multiple sclerosis cohort. Mult Scler 22:935–943. https://doi.org/10.1177/1352458515606211
Ladeira F, Salavisa M, Caetano A et al (2018) The influence of menopause in multiple sclerosis course: a longitudinal cohort study. Eur Neurol 80:223–227. https://doi.org/10.1159/000496374
Baroncini D, Annovazzi PO, De Rossi N et al (2019) Impact of natural menopause on multiple sclerosis: a multicentre study. J Neurol Neurosurg Psychiatry 90:1201–1206. https://doi.org/10.1136/jnnp-2019-320587
Karageorgiou V, Lambrinoudaki I, Goulis DG (2020) Menopause in women with multiple sclerosis: a systematic review. Maturitas 135:68–73. https://doi.org/10.1016/j.maturitas.2020.03.001
Bove R, White CC, Fitzgerald KC et al (2016) Hormone therapy use and physical quality of life in postmenopausal women with multiple sclerosis. Neurology 87:1457–1463. https://doi.org/10.1212/WNL.0000000000003176
Bove R, Anderson A, Rowles W et al (2022) A hormonal therapy for menopausal women with MS: a phase Ib/IIa randomized controlled trial. Mult Scler Relat Disord 61:103747. https://doi.org/10.1016/j.msard.2022.103747
Pozzilli C, De Giglio L, Barletta VT et al (2015) Oral contraceptives combined with interferon β in multiple sclerosis. Neurol(R) Neuroimmunol Neuroinflamm 2:e120. https://doi.org/10.1212/NXI.0000000000000120
Voskuhl R, Patti F (2016) Hormone replacement in menopausal women with multiple sclerosis: looking back, thinking forward. Neurology 87:1430–1431. https://doi.org/10.1212/WNL.0000000000003189
Lie IA, Wesnes K, Kvistad SS et al (2022) The effect of smoking on long-term gray matter atrophy and clinical disability in patients with relapsing-remitting multiple sclerosis. Neurol(R) Neuroimmunol Neuroinflamm. https://doi.org/10.1212/NXI.0000000000200008
Rodgers J, Friede T, Vonberg FW et al (2022) The impact of smoking cessation on multiple sclerosis disease progression. Brain 145:1368–1378. https://doi.org/10.1093/brain/awab385
Dalgas U, Stenager E (2012) Exercise and disease progression in multiple sclerosis: can exercise slow down the progression of multiple sclerosis? Ther Adv Neurol Disord 5:81–95. https://doi.org/10.1177/1756285611430719
Kjølhede T, Siemonsen S, Wenzel D et al (2018) Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult Scler 24:1356–1365. https://doi.org/10.1177/1352458517722645
Ewanchuk BW, Gharagozloo M, Peelen E, Pilutti LA (2018) Exploring the role of physical activity and exercise for managing vascular comorbidities in people with multiple sclerosis: a scoping review. Mult Scler Relat Disord 26:19–32. https://doi.org/10.1016/j.msard.2018.08.022
Dobson R, Rice DR, D’hooghe M et al (2022) Social determinants of health in multiple sclerosis. Nat Rev Neurol 18:723–734. https://doi.org/10.1038/s41582-022-00735-5
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Kimberly DiMauro has no conflicts to report. Dr. Carol Swetlik has no conflicts to report. Dr. Jeffrey Cohen received personal compensation for consulting for Astoria, Bristol-Myers Squibb, Convelo, EMD Serono, FiND Therapeutics, INMune, and Sandoz; and serving as an Editor of Multiple Sclerosis Journal.
Ethical approval
An ethics statement is not applicable because this article is based on published literature.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
DiMauro, K.A., Swetlik, C. & Cohen, J.A. Management of multiple sclerosis in older adults: review of current evidence and future perspectives. J Neurol 271, 3794–3805 (2024). https://doi.org/10.1007/s00415-024-12384-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-024-12384-3