
Abstract
Background and objectives
Serum biomarkers are emerging as useful prognostic tools for multiple sclerosis (MS); however, long-term studies are lacking. We aimed to evaluate the long-term prognostic value of the serum levels of neurofilament light chain (NfL), total tau, glial fibrillary acidic protein (GFAP), and chitinase 3-like-1 (CHI3L1) measured close to the time of MS onset.
Methods
In this retrospective, exploratory, observational, case and controls study, patients with relapsing–remitting MS (RRMS) with available baseline serum samples and prospectively follow-up in our MS unit for a long time were selected based on their clinical evolution to form two groups: (1) a benign RRMS (bRRMS) group, defined as patients with an Expanded Disability Status Scale (EDSS) score of ≤ 3 at ≥ 10 years of follow-up; (2) an aggressive RRMS (aRRMS) group, defined as patients with an EDSS score of ≥ 6 at ≤ 15 years of follow-up. An age-matched healthy control (HC) group was selected. NfL, total tau, and GFAP serum levels were quantified using a single-molecule array (SIMOA), and CHI3L1 was quantified using ELISA.
Results
Thirty-one patients with bRRMS, 19 with aRRMS, and 10 HC were included. The median follow-up time from sample collection was 17.74 years (interquartile range, 14.60–20.37). Bivariate and multivariate analyses revealed significantly higher NfL and GFAP levels in the aRRMS group than in the bRRMS group. A receiver operating characteristic curve analysis identified serum NfL level as the most efficient marker for distinguishing aRRMS from bRRMS.
Discussion
This proof-of-concept study comparing benign and aggressive RRMS groups reinforces the potential role of baseline NfL serum levels as a promising long-term disability prognostic marker. In contrast, serum GFAP, total tau, and CHI3L1 levels demonstrated a lower or no ability to differentiate between the long-term outcomes of RRMS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease characterized by multifocal inflammatory demyelination and neurodegeneration of the CNS, resulting in irreversible neurological damage and consequent accumulation of disability [1].
Disability progression shows great heterogeneity among patients, and it is believed that the early use of high-efficacy disease-modifying treatments (DMT) during the course of the disease could delay its irreversible accumulation in patients with high inflammatory activity [2,3,4]. Thus, identifying predictive markers of disability is becoming a priority as it will enable the selection of candidates for this treatment approach. Currently, there are few prognostic markers available, both clinical and radiological, with limited clinical utility [5,6,7,8,9,10,11,12,13], despite being combined in various scoring systems, wherein improving the predictive power involves incorporating variables from the early years of follow-up, which could result in missed opportunities for early treatment [14,15,16].
Accurate and specific biomarkers that targeting specific aspects of the pathological processes underlying MS are potential prognostic markers. The development of ultrasensitive digital immunoassays, such as the single molecule array (SIMOA), has enabled reliable measurement of CNS-relevant biomarkers in serum that were not previously detectable [17]. Neurofilament light chain (NfL), total tau protein, glial fibrillary acidic protein (GFAP), and chitinase 3-like-1 (CHI3L1) are promising prognostic biomarkers for MS. These biomarkers reflect neuronal damage occurring in acute and chronic lesions, astrocytic activation and astrogliosis, and oligodendrocytic activation at different stages of the disease, both in the inflammatory and neurodegenerative processes of MS [18,19,20,21,22]. Multiple studies have analyzed the relationship between disability progression and the baseline levels of NfL [23,24,25,26], GFAP [27,28,29,30,31,32], CHI3L1 [33,34,35], and total tau [36,37,38,39,40,41]. The results are inconsistent across different studies for NfL, GFAP, and total tau. Studies with follow-up periods exceeding 10 years are scarce.
The objective of this study was to investigate the predictive capacity of the serum biomarkers NfL, GFAP, CHI3L1, and total tau measured at the time of initial evaluation for long-term disability in patients with MS. Additionally, we aimed to compare these biomarkers to provide insights for future research.
Methods
Study design, participants, and clinical data collection
We designed an exploratory retrospective, longitudinal, observational, case and control study including patients diagnosed with remitting-relapsing MS (RRMS) according to the McDonald criteria of 2017 [42], who were prospectively followed up in the MS unit of a tertiary hospital with available serum samples at the time of initial patient evaluation. The STROBE guidelines for observational studies were used to conduct this study.
Two groups of patients were defined with distinctive inclusion criteria: a benign RRMS (bRRMS) group, defined as patients with an Expanded Disability Status Scale (EDSS) score of ≤ 3 at ≥ 10 years of follow-up, and an aggressive RRMS (aRRMS) group, defined as patients with an EDSS score of ≥ 6 at ≤ 15 years of follow-up. These inclusion criteria for each patient groups have been applied previously in other published works [43,44,45,46].
A third group of healthy controls (HC) were included, whose inclusion criteria were the absence of neurological diseases and the availability of a stored serum sample. They were selected by age matching to the patient groups.
The exclusion criteria were the presence of neurological comorbidities (peripheral or central nervous system) and relapse within the month before serum sample collection. In both patients and control groups, cases with samples not meeting the technical criteria (presence of particles, lipemia, or hemolyzed samples) were also excluded.
The European Database for Multiple Sclerosis software was used for the prospective collection of clinical data [47]. The variables collected were sex, date of birth, date of onset of MS symptoms, date of serum sampling, date of last relapse before serum sampling, date of last follow-up, total number of relapses during follow-up, EDSS at 10 years of onset for aRRMS, EDSS at 15 years of onset for bRRMS, EDSS at the end of follow-up for all patients, DMT received during follow-up, initiation date of each DMT, progression start date, baseline brain magnetic resonance imaging (MRI) date, presence of gadolinium-enhancing lesions on that MRI, and the presence of new lesions in T2 (in cases where possible, i.e., those with available previous MRI).
The following variables were calculated: age at MS onset, age at the time of serum sampling, total follow-up time, time from MS onset to serum sampling, time from previous relapse to serum sampling, time from baseline cerebral MRI to serum sampling, Multiple Sclerosis Severity Score (MSSS), and age-related Multiple Sclerosis Severity (ARMSS) scores. The DMT variable was analyzed as: “no DMT”; “moderate efficacy DMT” if none of the high efficacy DMT and any of the following was being used at any moment of the follow-up: interferon beta 1a, interferon beta 1b, peginterferon beta 1a, glatiramer acetate, teriflunomide, dimethyl fumarate; and “high efficacy DMT” if any of the following was being used at any moment of the follow-up: fingolimod, natalizumab, alemtuzumab, ocrelizumab, cladribine, rituximab, mitoxantrone.
Serum collection, processing, and laboratory analysis
Patient and healthy control samples were provided by the Biobank HUB-ICO-IDIBELL, funded by the Instituto de Salud Carlos III (PT20/00171) and by Xarxa de Bancs de Tumors de Catalunya, sponsored by the Pla Director d’Oncologia de Catalunya (XBTC).
Serum samples were prospectively collected from patients undergoing blood extraction as part of the usual initial evaluation in the MS unit, using appropriate serum separation tubes. Once obtained, the serum was centrifuged at 3000 rpm for 15 min at room temperature, and the supernatant was collected, aliquoted in volumes of 500 μL, and stored at − 80 °C until analysis. HC samples were obtained from healthy volunteers without neurological disorders at the neurology service, following the same technical procedures.
Serum levels of total tau, GFAP, and NfL were measured in singlicate using NeuroPlex-4B kit (Quanterix, Billerica, MA, USA) and SIMOA technology (Quanterix, Billerica, MA, USA). CHI3L1 serum levels were analyzed using the MicroVue YKL-40 EIA kit from Quidel (Cat no. 8020, Quidel, CA, USA), following the manufacturer's instructions. All samples were analyzed in the same run, and all biomarker values fell within the detection range limits specified by the manufacturer.
In the case of serum neurofilament levels, the web application derived from the study by Benkert et al. was used to obtain scores of standard deviations (SD) relative to normal values of healthy controls. These scores were obtained by correcting only for age, as body mass index (BMI) at the time of sample collection was not available (in these cases, a BMI of 25 is assumed) [48].
Study endpoints
The objectives of this study were to test whether serum NFL, GFAP, total tau, and CHI3L1 levels in the early course of MS were different between the bRRMS and aRRMS groups and to establish their ability to classify cases between the two groups.
Statistical analysis
The distribution of data was assessed using the Shapiro–Wilk test. Data are described as mean ± standard deviation (SD) or as median and interquartile range (IQR) according to their distribution. Categorical variables were described using frequencies. Box plots were used to visualize the distribution of biomarkers across different groups. For the bivariate group comparison analysis, Fisher’s exact test, Mann–Whitney U test, Kruskal–Wallis test, and Poisson or negative binomial regression were applied as appropriate. If the Kruskal–Wallis test was rejected, Dunn’s pairwise multiple comparison test was applied. For multivariate analysis using the MS patient groups, a binary logistic regression model was performed, including all available clinical variables that could act as confounders as independent variables. Diagnostic tests were performed for the regression model to avoid nonlinearity between the predictor variables and the odds logit and collinearity between the predictor variables. For the binomial logistic regression analysis, a logarithmic transformation was applied to the biomarker data to obtain a normal distribution and linearity with the odds ratio logit, as it has been shown that they follow a lognormal distribution. This logarithmic transformation was done according to the equation “ln (X − k)” where “X” is the continuous independent variable and “k” was calculated to achieve a skewness of 0. To assess the biomarker accuracy in classifying patients into benign or aggressive forms, receiver operating characteristic (ROC) curves and the derived area under the curve (AUC) were calculated. Outliers were not excluded from the analysis. The best cutoff value, sensitivity, and specificity were estimated based on the Youden index [49]. And ROC curve standard error calculations, and comparisons were performed using DeLong’s method [50, 51]. All tests were conducted with 95% confidence intervals (CI) and a significance level of 5%. Bonferroni adjustment was used for multiple comparisons in the Dunn test and ROC curve comparison test. In order to maintain the same p value threshold across all test and improve readability, this was done multiplying the resulting p value from each comparison within a multiple comparison by “m”, where “m” is the number of comparisons performed. Statistical analysis and visualization were performed using Stata 18 software (StataCorp LLC, Texas, USA) and GraphPad Prism version 9.5.0 (La Jolla, CA, USA).
Standard protocol approvals, registrations, and patient consents
This study was approved by the Ethics Committee (CEIC) of the Hospital Universitari de Bellvitge (reference number PR257/23). Patient information confidentiality was addressed in accordance with Spanish regulations. All participants provided written informed consent before sample storage in the IDBELL-ICO-HUB Biobank, following the guidelines of Spanish legislation on this matter (Real Decreto 1716/2011) and the approval of the CEIC of Bellvitge University Hospital.
Data availability statement
Anonymized data not published within this article will be made available by request from any qualified investigator.
Results
Study population and groups’ characteristics
Fifty patients with RRMS (31 with bRRMS and 19 with aRRMS) and 10 age-matched HC were included in this study. The baseline demographic characteristics were similar between the two groups of RRMS patients and healthy controls, including age at the time of serum sampling (median of 36 completed years in the bRRMM vs. 43 years in the aRRMS vs. 40.5 years in the HC groups, p = 0.25) and sex ratio (74.2% were female in the bRRMS group vs. 47.4% in aRRMS vs. 50% in HC, p = 0.135).
The clinical characteristics and comparison tests between the two groups of patients with RRMS are summarized in Table 1. Globally, 64% of patients were female, and the mean age of MS onset was 36.6 ± 9 years old. They were followed-up for a median of 17.74 years (IQR, 14.60–20.37) out of a total median disease duration of 20.37 years (IQR, 17.97–23.51). Although no statistically significant differences were found in the age at MS onset or sex ratios, a lower proportion of females was observed in the aRRMS group (74.2% in the bRRMS vs. 47.4% in the aRRMS group, p = 0.073). The total follow-up time (median of 18.29 years in bRRMS vs 15.01 in aRRMS, p = 0.03) and disease duration (median of 20.86 years in bRRMS vs 15.89 in aRRMS, p = 0.03) were significantly longer in the bRRMS group. The median EDSS score at the time of serum collection was 1.5 (1 for bRRMS vs. 3 for aRRMS; p < 0.001). The median EDSS at the last follow-up was 1.5 (IQR, 1.5–2) for the bRRMS group and 7.5 (IQR, 7–8) for the aRRMS group, and both MSSS and ARMSS score were significantly higher in aRRMS group (p < 0.001). No differences were found between the two groups in terms of age at the time of sample collection, time from MS onset to sample collection, or time from prior relapse to sample collection.
Baseline cerebral MRI data were available for 48 out of 50 patients (1 missing in each group). The median time between the acquisition of these baseline MRIs and the serum sample collection was 3.35 months (IQR 0.54–23.3), with no statistically significant differences between the two patient groups (median 4.40 months in bRRMS vs. 1.49 in aRRMS, p = 0.073 by Mann–Whitney test). In 8 out of these 48 cases, a previous brain MRI allowed estimating the appearance of new T2 lesions (4 in the bRRMS group and 4 in the aRRMS group); in the other 40 cases, the presence of radiological activity could only be assessed by gadolinium enhancement as it was the first MRI performed. Radiological activity was observed in a total of five baseline MRIs: two in the bRRMS group (two due to gadolinium enhancement and another due to new T2 lesions) and three in the aRRMS group (all due to gadolinium enhancement), with no statistically significant differences between groups (p = 0.349 by Fisher’s test).
Serum biomarkers in aggressive and benign groups
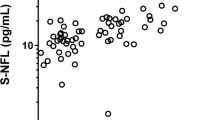
The serum biomarker levels of the three groups and the results of the bivariate contrast tests are summarized in Table 2. Figure 1 shows boxplots of serum biomarker levels. Statistically significant differences in NfL, GFAP, and CHI3L1 serum levels between at least two groups were found in bivariate analysis (p < 0.001, p = 0.002, and p = 0.003, respectively). For serum NfL levels, Dunn’s test confirmed that all groups were significantly different (HC vs. bRRMS, p = 0.0079; HC vs. aRRMS, p < 0.001; and bRRMS vs. aRRMS, p = 0.0066). In the case of GFAP serum levels, the aRRMS group levels were significantly different from those in the HC and bRRMS groups (p < 0.001 and p = 0.047, respectively); however, there were no significant differences between the HC and bRRMS groups (p = 0.072). CHI3L1 levels were significantly different in the HC group from those in both bRRMS and aRRMS patients (p = 0.013 and p = 0.001, respectively); however, there were no differences between the bRRMS and aRRMS patients (p = 0.31).

Distribution boxplots of NfL (A), GFAP (B), CHI3L1 (C), and total Tau (D) levels in the serum of benign and aggressive forms of RRMS patients and control cases using single molecule array (SIMOA) and ELISA technologies. A case scatter plot is represented by dots and outliers by triangles. A logarithmic scale for NFL levels was used in A to improve data visualization. Statistical signification (corrected for multiple comparisons in Dunn test) among groups were set at *p < 0.05, **p < 0.01, ***p < 0.001 and ****p < 0.0001
In the case of neurofilaments, the analysis was repeated using SD scores relative to normal values from a large cohort of healthy subjects [48]. The control, bRRMS and aRRMS groups had a median score in standard deviation of 0.9 (IQR 0.18–1.23), 2.05 (IQR 1.68–2.85), and 2.68 (IQR 2.46–3.09), respectively. Similar to absolute values, the Kruskal–Wallis test (p < 0.001) and pairwise comparisons using the Dunn test confirmed that SD of NfL levels were different among all groups (control vs bRRMS p = 0.004, control vs aRRMS p < 0.001, bRRMS vs aRRMS p = 0.01).
Benign and aggressive multiple sclerosis classification accuracy of serum biomarkers
The ROC curve analysis results assessing the bRRMS vs aRRMS classification power are summarized in Table 3 and Fig. 2. Of note, the only biomarkers with an AUC greater than 0.5 that were statistically significant were NfL and GFAP. When performing multiple comparisons among the biomarker curves, the AUC of NfL and GFAP were significantly higher than those of total tau (p = 0.020 and 0.006, respectively). No significant differences were found between the AUCs of NfL and GFAP (p = 1) or between those of CHI3L1 and total tau (p = 0.1). When conducting the ROC curve analysis to assess the discriminative capacity between bRRMS and aRRMS groups using SD scores for NfL serum levels, the AUC was very similar to that obtained using absolute values, with no statistically significant differences between the two (AUC 0.753 with SD vs 0.766 using absolute values, p = 0.63). The best NfL SD score cut-off value based on Youden index was 2.26.

Receiver operating characteristic (ROC) curves of NfL, GFAP, CHI3L1 and total Tau serum quantification in the differential diagnosis of benign RRMS and aggressive RRMS. AUC values, corresponding to the area under ROC curves
In the multivariate binary logistic regression analysis, age at the time of serum sampling, EDSS score at the time of serum sampling, and time from previous relapse to serum sampling were included as covariables. This association remained statistically significant after multivariate adjustment for NfL. The overall NfL model showed a good fit to the data (LL(M) = − 16.59) and statistical significance (χ2(df = 4) = 31.26, p < 0.001), and the estimated odds ratio for predictor variable NfL was 3.67 (95% confidence interval 1.14–11.87; X2 Wald = 4.71, p = 0.03), indicating that NfL was an independent predictor of the outcome. The remaining biomarkers (GFAP, CHI3L1, and total tau) did not show a significant association in multivariate binary logistic regression analysis.
Discussion
This proof-of-concept study reported an association between serum NfL and GFAP levels measured early in the course of MS and subsequent EDSS progression, showing acceptable predictive power to differentiate two groups of benign and aggressive forms of RRMS in patients with a disease duration of 20 years and an average follow-up period of approximately 18 years.
Baseline serum NfL levels have been associated with worsening of EDSS in the first year, number of relapses, and progression of brain atrophy, as measured by cerebral magnetic resonance imaging (MRI) [52,53,54,55] in short-term prognosis studies. Regarding long-term prognosis, both baseline and longitudinal measures of NfL levels have been linked to greater cerebral MRI-based brain atrophy [25, 53, 56,57,58,59,60]; however, their association with disability progression is inconsistent [23]. In fact, studies with longer clinical follow-up periods found no relationship between baseline NfL levels and disability progression [24, 25]. However, a recent study with a median follow-up of approximately 7 years found an association between baseline NfL levels and a higher risk of confirmed disability progression with an EDSS ≥ 3 during the follow-up period [26]. Additionally, there is a previous study for NfL with a similar design as that of ours, including patients with RRMS, that also demonstrates that baseline sNfL is associated with long term (18.9 years) clinical disease progression and may be a sensitive marker of subsequent poor clinical outcomes [61]. It is worth noting that this study includes clinically isolated syndrome (CIS) and primary progressive MS (PPMS) in addition to RRMS in its cohort, which could have potentially influenced a positive outcome.
Regarding the basal serum GFAP levels, the first study in 2019 failed to demonstrate the prognostic value of GFAP in predicting outcomes [27]. Subsequently, two studies, with median follow-up periods of 3.1 and 4.4 years and smaller cohorts (94 and 115 patients, respectively), found no relationship between GFAP and disability measured using different scales [28, 29]. Two other studies with larger cohorts (257 and 355 patients) and longer follow-up periods (approximately 7 years) found a relationship between GFAP and disease progression [30, 31]. One study demonstrated that GFAP, measured at baseline and longitudinally in subsequent measurements, is a good predictor of disease progression independent of relapse activity (PIRA) [31]. However, a recent study analyzing the prognostic potential of GFAP and PIRA found little or no correlation [32]. Finally, a recent study demonstrated that baseline serum levels of GFAP, either alone or in combination with baseline NfL serum levels, as well as its levels measured after 1 year of follow-up, improved the performance of predictive models that included all known clinical and radiological prognostic variables for EDSS outcomes at 10 years [62].
Our study supports the idea that baseline serum NfL and GFAP levels are predictors of long-term disability progression. The results of the ROC curves also suggest that NfL has a better capacity than GFAP to differentiate between the bRRMS and aRRMS groups and, therefore, has a better prognostic ability, although the AUC comparison test failed to demonstrate a statistically significant difference between both, possibly due to a lack of statistical power. The serum NfL level was probably the most promising biomarker in this study a priori, given that it is a neuronal cytoskeletal component involved in axonal transport and is considered a good surrogate marker of neuronal axonal damage and, therefore, of the lesion burden at the time of its determination, even though it is non-specifically elevated in multiple pathologies [18]. Although it is considered a marker of neuronal damage due to active lesions, a recent study demonstrated that its levels are capable of predicting disability progression independent of relapses in patients undergoing treatment with ocrelizumab [63]. GFAP is the main intermediate filament of human astrocytes and is considered a marker of astrocytic injury and astrogliosis [64]. The idea that GFAP could be a good marker of pure progression has been considered because of its high levels in progressive forms, both in PPMS and secondary progressive MS (SPMS) without recent inflammatory activity [34, 65]. Notably, due to its design, this study does not help clarify whether basal GFAP is related to disability through PIRA, for which contradictory results exist [31, 32].This may explain why previous studies with a shorter follow-up period did not find a relationship between baseline GFAP and prognosis in RRMS patients, unlike those with a longer follow-up period.
In multivariate analysis, NfL association remained statistically significant after accounting for confounding effects such as time between the last relapse and serum collection, and known clinical prognostic markers such as age and EDSS at the moment of serum sampling. An interesting characteristic of our cohort is that being composed of patients with long-term follow-up, serum NfL and GFAP levels were minimally influenced by the early use of high-efficacy treatments as this strategy had not yet been implemented. In fact, at the time of sample collection and initiation of follow-up, only 11 out of 50 patients received moderately effective DMT, and none received highly effective DMT. This is a factor should be considered when interpreting our results as some studies have demonstrated the influence of DMT on serum NfL and GFAP levels, especially in patients on high efficacy DMT [48, 66, 67]. Surprisingly, in our sample, benign forms had a higher proportion of patients under treatment at the time of sample extraction: 10 in bRRMS vs. 1 in aRRMS. From those, 8 were on interferon beta-1a 22ug 3 times per week, 1 on interferon beta-1a 30ug once a week and 1 on glatiramer acetate in the bRRMS group, and 1 was on cyclophosphamide in the aRRMS group. However, the levels of NfL and GFAP in the treated bRRMS group and the untreated bRRMS group were not significantly different (median of 12.44 vs 15.34, p = 0.15). Moreover, when conducting a sensitivity analysis comparing bRRMS and aRRMS by excluding those 11 patients under treatment, the results remained consistent in the bivariate test for both NfL (p = 0.029) and GFAP (p = 0.026), and the ROC curve analysis (AUC = 0.71 for both NfL and GFAP). Another noteworthy characteristic of this cohort is that only two patients from the bRRMS group and three from the aRRMS group exhibited radiological activity on the baseline brain MRI. Therefore, it is unlikely that this activity significantly influenced the mean baseline levels of NfL and GFAP in the groups, thus minimizing bias in the results.
Concerning the adjustment of serum NfL levels based on age, as suggested by several studies, for this specific use, the results of the comparative analysis using absolute values and standard deviation scores did not show significant differences between the two, in line with what was suggested by a meta-analysis that supported the notion that this effect is diluted under pathological conditions such as MS [68]. Additionally, age at the time of sample collection was not significantly different between the study groups, and this variable did not influence the results of the multivariable models (data not shown). Regarding the possible influence of previous relapses on the sample extraction over NfL levels [48], the median time between both events was 6.46 months (IQR, 3.71–21.88), with no statistically significant differences between the groups. Furthermore, inclusion in the multivariate model did not significantly affect the results.
In the GFAP model, the introduction of EDSS at the time of extraction rendered the serum GFAP levels insignificant. In our experience, GFAP has not demonstrated the ability to discriminate between patients with benign and aggressive forms of MS after a follow-up period of approximately 18 years. However, in other studies with shorter follow-up periods, GFAP appeared to have some predictive capacity [62].
CHI3L1 and tau levels were not significantly different between the benign and aggressive groups, and their classification power was not deemed acceptable. Therefore, unlike some previous studies, our study failed to demonstrate a relationship between baseline serum CHI3L1 and total tau levels.
There are few studies on the predictive power of basal levels of CHI3L1 for disability prognosis, all of which show positive results but have limited clinical follow-up and, most importantly, CSF samples rather than serum samples [33,34,35]. This fact should be taken into account, as there is evidence that systemic levels of CHI3L1 can increase in a variety of non-neurological pathologies [69].The study with the longer follow-up (median, 11.7 years) in a cohort of 301 patients with RRMS and CIS showed that elevated levels of CHI3L1 at disease onset independently predicted a shorter time to reach irreversible EDSS score of 3 and 6 [34]. An association was also demonstrated between baseline CHI3L1 levels and EDSS at 1 year in a small cohort of patients with PPMS [35]. It is worth mentioning that although progressive forms of MS, especially PPMS, have been associated with elevated levels of CHI3L1 in both CSF and serum [70, 71], this does not necessarily imply that baseline serum levels can be predictive.
Studies on total tau and prognosis in MS, are scarce and have been conducted with short follow-up periods, and the results are inconclusive. Furthermore, in most of these studies, total tau levels were determined in the CSF using ELISA. One study related baseline CSF total tau levels to the MSSS and ARMSS with a 2-year follow-up [36], whereas another study linked these levels to the final EDSS score with a 3-year follow-up [37]. However, several studies have failed to demonstrate this relationship [38,39,40,41]. There are no studies in serum for total tau, and although in this case, the determination was performed using SIMOA, it is noteworthy that the levels are over 100 times higher in CSF [36, 37] than in serum, resulting in a median total tau level in serum of 0.86 pg/mL in the 56 participants of our study, with little variation between groups. Similar to other neurological disorders where total tau in CSF has demonstrated its utility, these results were not replicated in serum [72].
As an exploratory observational study, the rationale behind exclusively including the extremes of the population spectrum regarding disability progression was to maximize sensitivity and, therefore, cost-effectiveness of the study. Regarding the selection criteria for patient groups, the definition criterion for bRRMS is more widely accepted despite multiple definitions and a lack of consensus for aRRMS [43,44,45]. In our study, we chose a previously used criterion that was effective and allowed us to obtain a sufficient sample size [46]. However, this design also implies a series of limitations. The study is not suitable for providing odds ratios (OR) because it does not include the entire cohort of patients; therefore, these are pseudo-odds ratios. Nevertheless, this study provides valuable information regarding the potential of biomarkers, especially their comparative analysis, to guide future studies.
For the same reason, this observed prognostic capacity is undoubtedly overestimated, as the inclusion of an unselected sample will yield more overlapping levels of NfL and GFAP. Consequently, our study did not allow us to assert the usefulness of these biomarkers in clinical practice. In addition to the limitations inherent to observational studies and their designs, two other limitations should be highlighted. The first was the absence of follow-up radiological data, which, although not necessary for the intended purpose of evaluating and comparing the predictive power of the baseline levels of the biomarkers, would have been of great interest. The second stems from its sample size, although considered sufficient to ensure reliable observational results, which restricted the number of covariates that could be included in the multivariable models. The results of our multivariate analysis for NfL support the idea that it is a robust prognostic marker, however, further research including other previously described prognostic markers, both clinical and radiological, and a complete sample of patients will be necessary to confirm their utility and that it is an independent prognostic marker.
In conclusion, this study demonstrated that serum levels of GFAP and especially NfL, measured at the time of initial evaluation have potential to predict long-term disability in patients with MS. However, the roles of total tau and CHI3L1 remain uncertain. Therefore, serum GFAP and NfL levels should be considered candidates for inclusion in scoring systems along with other variables aimed at predicting long-term disability.
References
Reich DS, Lucchinetti CF, Calabresi PA (2018) Multiple sclerosis. N Engl J Med 378(2):169–180. https://doi.org/10.1056/NEJMra1401483
Weideman AM, Tapia-Maltos MA, Johnson K, Greenwood M, Bielekova B (2017) Meta-analysis of the age-dependent efficacy of multiple sclerosis treatments. Front Neurol. https://doi.org/10.3389/FNEUR.2017.00577
Ontaneda D, Tallantyre E, Kalincik T, Planchon SM, Evangelou N (2019) Early highly effective versus escalation treatment approaches in relapsing multiple sclerosis. Lancet Neurol 18:973–980. https://doi.org/10.1016/S1474-4422(19)30151-6
Harding K et al (2019) Clinical outcomes of escalation vs early intensive disease-modifying therapy in patients with multiple sclerosis. JAMA Neurol 76(5):536–541. https://doi.org/10.1001/JAMANEUROL.2018.4905
Paul A, Comabella M, Gandhi R (2019) Biomarkers in multiple sclerosis. Cold Spring Harb Perspect Med. https://doi.org/10.1101/CSHPERSPECT.A029058
Tintore M et al (2015) Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain 138(Pt 7):1863–1874. https://doi.org/10.1093/BRAIN/AWV105
D’Amico E, Patti F, Leone C, Lo Fermo S, Zappia M (2016) Negative prognostic impact of MRI spinal lesions in the early stages of relapsing–remitting multiple sclerosis. Mult Scler J Exp Transl Clin 2:1–7. https://doi.org/10.1177/2055217316631565
Fisniku LK et al (2008) Disability and T 2 MRI lesions: a 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain 131(3):808–817. https://doi.org/10.1093/brain/awm329
Swanton JK et al (2009) Early MRI in optic neuritis: the risk for disability. Neurology 72(6):542–550. https://doi.org/10.1212/01.wnl.0000341935.41852.82
Minneboo A, Barkhof F, Polman CH, Uitdehaag BMJ, Knol DL, Castelijns JA (2004) Infratentorial lesions predict long-term disability in patients with initial findings suggestive of multiple sclerosis. Arch Neurol 61(2):217–221. https://doi.org/10.1001/archneur.61.2.217
Malpas CB et al (2020) Early clinical markers of aggressive multiple sclerosis. Brain 143(5):1400–1413. https://doi.org/10.1093/brain/awaa081
Jokubaitis VG et al (2016) Predictors of long-term disability accrual in relapse-onset multiple sclerosis. Ann Neurol 80(1):89–100. https://doi.org/10.1002/ana.24682
Dekker I et al (2020) Infratentorial and spinal cord lesions: cumulative predictors of long-term disability? Mult Scler J 26(11):1381–1391. https://doi.org/10.1177/1352458519864933
Pisani AI, Scalfari A, Crescenzo F, Romualdi C, Calabrese M (2021) A novel prognostic score to assess the risk of progression in relapsing−remitting multiple sclerosis patients. Eur J Neurol 28(8):2503–2512. https://doi.org/10.1111/ene.14859
Gasperini C et al (2021) Scoring the 10-year risk of ambulatory disability in multiple sclerosis: the RoAD score. Eur J Neurol 28(8):2533–2542. https://doi.org/10.1111/ene.14845
Sormani MP et al (2013) Scoring treatment response in patients with relapsing multiple sclerosis. Mult Scler J 19(5):605–612. https://doi.org/10.1177/1352458512460605
Comabella M, Sastre-Garriga J, Montalban X (2016) Precision medicine in multiple sclerosis: biomarkers for diagnosis, prognosis, and treatment response. Curr Opin Neurol 29(3):254–262. https://doi.org/10.1097/WCO.0000000000000336
Gafson AR et al (2020) Neurofilaments: neurobiological foundations for biomarker applications. Brain 143(7):1975–1998. https://doi.org/10.1093/BRAIN/AWAA098
Abdelhak A et al (2022) Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat Rev Neurol 18(3):158–172. https://doi.org/10.1038/s41582-021-00616-3
Bonneh-Barkay D, Wang G, Starkey A, Hamilton RL, Wiley CA (2010) In vivo CHI3L1 (YKL-40) expression in astrocytes in acute and chronic neurological diseases. J Neuroinflamm 7:34. https://doi.org/10.1186/1742-2094-7-34
Starossom SC et al (2019) Chi3l3 induces oligodendrogenesis in an experimental model of autoimmune neuroinflammation. Nat Commun. https://doi.org/10.1038/s41467-018-08140-7
Hampel H, Blennow K, Shaw LM, Hoessler YC, Zetterberg H, Trojanowski JQ (2010) Total and phosphorylated tau protein as biological markers of Alzheimer’s disease. Exp Gerontol 45(1):30–40. https://doi.org/10.1016/j.exger.2009.10.010
Manouchehrinia A et al (2020) Plasma neurofilament light levels are associated with risk of disability in multiple sclerosis. Neurology 94(23):E2457–E2467. https://doi.org/10.1212/WNL.0000000000009571
Aloizou AM et al (2022) Baseline neurofilament levels in cerebrospinal fluid do not correlate with long-term prognosis in multiple sclerosis. Mult Scler Relat Disord. https://doi.org/10.1016/j.msard.2022.103940
Cantó E et al (2019) Association between serum neurofilament light chain levels and long-term disease course among patients with multiple sclerosis followed up for 12 years. JAMA Neurol 76(11):1359–1366. https://doi.org/10.1001/JAMANEUROL.2019.2137
Monreal E et al (2023) Association of serum neurofilament light chain levels at disease onset with disability worsening in patients with a first demyelinating multiple sclerosis event not treated with high-efficacy drugs. JAMA Neurol. https://doi.org/10.1001/jamaneurol.2023.0010
Watanabe M et al (2019) Serum GFAP and neurofilament light as biomarkers of disease activity and disability in NMOSD. Neurology 93(13):E1299–E1311. https://doi.org/10.1212/WNL.0000000000008160
Barro C et al (2022) Serum NfL but not GFAP predicts cognitive decline in active progressive multiple sclerosis patients. Mult Scler J 29(2):206–211. https://doi.org/10.1177/13524585221137697
Pauwels A et al (2022) Plasma glial fibrillary acidic protein and neurofilament light chain in relation to disability worsening in multiple sclerosis. Mult Scler 28(11):1685–1696. https://doi.org/10.1177/13524585221094224
Barro C et al (2022) Serum GFAP and NfL levels differentiate subsequent progression and disease activity in patients with progressive multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. https://doi.org/10.1212/NXI.0000000000200052
Meier S et al (2023) Serum glial fibrillary acidic protein compared with neurofilament light chain as a biomarker for disease progression in multiple sclerosis. JAMA Neurol. https://doi.org/10.1001/jamaneurol.2022.5250
Jiang X et al (2023) Glial fibrillary acidic protein and multiple sclerosis progression independent of acute inflammation. Mult Scler J. https://doi.org/10.1177/13524585231176732
Lucchini M et al (2023) CSF CXCL13 and chitinase 3-like-1 levels predict disease course in relapsing multiple sclerosis. Mol Neurobiol 60(1):36–50. https://doi.org/10.1007/S12035-022-03060-6
Martínez MAM et al (2015) Glial and neuronal markers in cerebrospinal fluid predict progression in multiple sclerosis. Mult Scler J 21(5):550–561. https://doi.org/10.1177/1352458514549397
Pérez-Miralles F et al (2020) CSF chitinase 3-like-1 association with disability of primary progressive MS. Neurol Neuroimmunol Neuroinflamm. https://doi.org/10.1212/NXI.0000000000000815
Virgilio E et al (2021) Cerebrospinal tau levels as a predictor of early disability in multiple sclerosis. Mult Scler Relat Disord. https://doi.org/10.1016/j.msard.2021.103231
Martínez-Yélamos A, Saiz A, Bas J, Hernandez JJ, Graus F, Arbizu T (2004) Tau protein in cerebrospinal fluid: a possible marker of poor outcome in patients with early relapsing-remitting multiple sclerosis. Neurosci Lett 363(1):14–17. https://doi.org/10.1016/j.neulet.2004.03.039
Brettschneider J et al (2005) Tau protein level in cerebrospinal fluid is increased in patients with early multiple sclerosis. Mult Scler 11(3):261–265. https://doi.org/10.1191/1352458505MS1159OA
Guimarães J, Cardoso MJ, Sá MJ (2006) Tau protein seems not to be a useful routine clinical marker of axonal damage in multiple sclerosis. Mult Scler 12(3):354–356. https://doi.org/10.1191/1352458506MS1288SR
HeinNéeMaier K et al (2008) Biological markers for axonal degeneration in CSF and blood of patients with the first event indicative for multiple sclerosis. Neurosci Lett 436(1):72–76. https://doi.org/10.1016/J.NEULET.2008.02.064
Terzi M, Birinci A, Çetinkaya E, Onar MK (2007) Cerebrospinal fluid total tau protein levels in patients with multiple sclerosis. Acta Neurol Scand 115(5):325–330. https://doi.org/10.1111/J.1600-0404.2007.00782.X
Thompson AJ et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17(2):162–173. https://doi.org/10.1016/S1474-4422(17)30470-2
Iacobaeus E et al (2020) Aggressive multiple sclerosis (1): towards a definition of the phenotype. Mult Scler J 26(9):1031–1044. https://doi.org/10.1177/1352458520925369
Glad SB, Aarseth JH, Nyland H, Riise T, Myhr KM (2010) Benign multiple sclerosis: a need for a consensus. Acta Neurol Scand 122(SUPPL. 190):44–50. https://doi.org/10.1111/j.1600-0404.2010.01375.x
Arroyo-Pereiro P et al (2023) Kappa free light chains index in multiple sclerosis very long-term prognosis. Front Immunol. https://doi.org/10.3389/fimmu.2023.1223514
Tintore M et al (2020) The long-term outcomes of CIS patients in the Barcelona inception cohort: looking back to recognize aggressive MS. Mult Scler J 26(13):1658–1669. https://doi.org/10.1177/1352458519877810
Confavreux C, Compston DAS, Hommes OR, McDonald WI, Thompson AJ (1992) EDMUS, a European database for multiple sclerosis. J Neurol Neurosurg Psychiatry 55(8):671–676. https://doi.org/10.1136/JNNP.55.8.671
Benkert P et al (2022) Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurol 21(3):246–257. https://doi.org/10.1016/S1474-4422(22)00009-6
Hughes G (2015) Youden’s index and the weight of evidence revisited. Methods Inf Med 54(6):576–577. https://doi.org/10.3414/ME15-04-0007
Zhang DD, Zhou XH, Freeman DH, Freeman JL (2002) A non-parametric method for the comparison of partial areas under ROC curves and its application to large health care data sets. Stat Med 21(5):701–715. https://doi.org/10.1002/sim.1011
Bantis LE et al (2023) Statistical assessment of the prognostic and the predictive value of biomarkers—a biomarker assessment framework with applications to traumatic brain injury biomarker studies. Res Methods Med Health Sci 4(1):34–48. https://doi.org/10.1177/26320843221141056
Disanto G et al (2017) Serum neurofilament light: a biomarker of neuronal damage in multiple sclerosis. Ann Neurol 81(6):857–870. https://doi.org/10.1002/ANA.24954
Barro C et al (2018) Serum neurofilament as a predictor of disease worsening and brain and spinal cord atrophy in multiple sclerosis. Brain 141(8):2382–2391. https://doi.org/10.1093/BRAIN/AWY154
Calabresi PA et al (2021) Temporal profile of serum neurofilament light in multiple sclerosis: implications for patient monitoring. Mult Scler 27(10):1497–1505. https://doi.org/10.1177/1352458520972573
Thebault S et al (2022) High or increasing serum NfL is predictive of impending multiple sclerosis relapses. Mult Scler Relat Disord 59:103535. https://doi.org/10.1016/J.MSARD.2022.103535
Kuhle J et al (2017) Serum neurofilament is associated with progression of brain atrophy and disability in early MS from Neurologic Clinic and Policlinic. Neurology 88:826–831. https://doi.org/10.1212/WNL.0000000000003653
Chitnis T et al (2018) Neurofilament light chain serum levels correlate with 10-year MRI outcomes in multiple sclerosis. Ann Clin Transl Neurol 5(12):1478–1491. https://doi.org/10.1002/ACN3.638
Jakimovski D et al (2019) Serum neurofilament light chain levels associations with gray matter pathology: a 5-year longitudinal study. Ann Clin Transl Neurol 6(9):1757–1770. https://doi.org/10.1002/ACN3.50872
Srpova B et al (2021) Serum neurofilament light chain reflects inflammation-driven neurodegeneration and predicts delayed brain volume loss in early stage of multiple sclerosis. Mult Scler J 27(1):52–60. https://doi.org/10.1177/1352458519901272
Buchmann A et al (2023) High serum neurofilament light chain levels correlate with brain atrophy and physical disability in multiple sclerosis. Eur J Neurol. https://doi.org/10.1111/ENE.15742
Thebault S, Abdoli M, Fereshtehnejad SM, Tessier D, Tabard-Cossa V, Freedman MS (2020) Serum neurofilament light chain predicts long term clinical outcomes in multiple sclerosis. Sci Rep 10(1):10381. https://doi.org/10.1038/S41598-020-67504-6
Bose G et al (2023) Early neurofilament light and glial fibrillary acidic protein levels improve predictive models of multiple sclerosis outcomes. Mult Scler Relat Disord. https://doi.org/10.1016/j.msard.2023.104695
Bar-Or A et al (2023) Blood neurofilament light levels predict non-relapsing progression following anti-CD20 therapy in relapsing and primary progressive multiple sclerosis: findings from the ocrelizumab randomised, double-blind phase 3 clinical trials. EBioMedicine. https://doi.org/10.1016/J.EBIOM.2023.104662
Eng LF, Ghirnikar RS, Lee YL (2000) Glial fibrillary acidic protein: GFAP-thirty-one years (1969–2000). Neurochem Res 25(9–10):1439–1451. https://doi.org/10.1023/A:1007677003387
Norgren N, Sundström P, Svenningsson A, Rosengren L, Stigbrand T, Gunnarsson M (2004) Neurofilament and glial fibrillary acidic protein in multiple sclerosis. Neurology 63(9):1586–1590. https://doi.org/10.1212/01.WNL.0000142988.49341.D1
Delcoigne B et al (2020) Blood neurofilament light levels segregate treatment effects in multiple sclerosis. Neurology 94(11):e1201–e1212. https://doi.org/10.1212/WNL.0000000000009097
Högel H et al (2020) Serum glial fibrillary acidic protein correlates with multiple sclerosis disease severity. Mult Scler 26(2):210–219. https://doi.org/10.1177/1352458518819380
Bridel C et al (2019) Diagnostic value of cerebrospinal fluid neurofilament light protein in neurology: a systematic review and meta-analysis. JAMA Neurol 76(9):1035–1048. https://doi.org/10.1001/JAMANEUROL.2019.1534
Pinteac R, Montalban X, Comabella M (2020) Chitinases and chitinase-like proteins as biomarkers in neurologic disorders. Neurol Neuroimmunol Neuroinflamm 8(1):e921.https://doi.org/10.1212/NXI.0000000000000921
Mañé-Martínez MA et al (2016) Glial and neuronal markers in cerebrospinal fluid in different types of multiple sclerosis. J Neuroimmunol 299:112–117. https://doi.org/10.1016/j.jneuroim.2016.08.004
Cantó E et al (2011) Chitinase 3-like 1 plasma levels are increased in patients with progressive forms of multiple sclerosis. Mult Scler 18(7):983–990. https://doi.org/10.1177/1352458511433063
Illán-Gala I et al (2021) Plasma tau and neurofilament light in frontotemporal lobar degeneration and Alzheimer disease. Neurology 96(5):e671–e683. https://doi.org/10.1212/WNL.0000000000011226
Acknowledgements
The authors thank Susana Pobla (Multiple Sclerosis Unit Secretary) for providing the technical support. We would also like to thank all the patients who participated in this study. This study was supported by the Instituto de Salud Carlos III (PT20/00171) and Xarxa de Bancs de Tumors de Catalunya, sponsored by the Pla Director d’Oncologia de Catalunya (XBTC). We thank the CERCA Programme/Generalitat de Catalunya for their institutional support.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Contributions
I-L, L-B, L-RP and E-M contributed to sample and data collection. P-AB analyzed plasma samples for the studied analytes. P-AP contributed to the analysis, and interpretation of the data and writing of the report. A-MV contributed to the writing of the report. A-MY, S-MY and P-AB contributed to the study design, analysis and interpretation of the data, and report correction. All the authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
Pablo Arroyo-Pereiro, Albert Muñoz-Vendrell, Isabel León, Antonio Martínez-Yélamos and Sergio Martínez-Yélamos received honoraria for participating on advisory boards and for collaborations as consultants and scientific communications; they also received research support as well as funding for travel and congress expenses from Roche, Biogen Idec, Novartis, TEVA, Merck, Genzyme, Sanofi, Bayer, Almirall, and Celgene. Pol Andrés-Benito received research support funding from Biogen Iberica S.L.
Ethical approval
This study was approved by the Hospital Universitari de Bellvitge Research Ethics Committee, with reference PR257/23. Patients signed informed consent forms, and data were collected anonymously. Patient information confidentiality was handled in accordance with Spanish regulations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Arroyo Pereiro, P., Muñoz-Vendrell, A., León Moreno, I. et al. Baseline serum neurofilament light chain levels differentiate aggressive from benign forms of relapsing–remitting multiple sclerosis: a 20-year follow-up cohort. J Neurol 271, 1599–1609 (2024). https://doi.org/10.1007/s00415-023-12135-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-12135-w