
Abstract
Background
Atrial fibrillation (AF) detection and treatment are key elements to reduce recurrence risk in cryptogenic stroke (CS) with underlying arrhythmia. The purpose of the present study was to assess the predictors of AF in CS and the utility of existing AF-predicting scores in The Nordic Atrial Fibrillation and Stroke (NOR-FIB) Study.
Method
The NOR-FIB study was an international prospective observational multicenter study designed to detect and quantify AF in CS and cryptogenic transient ischaemic attack (TIA) patients monitored by the insertable cardiac monitor (ICM), and to identify AF-predicting biomarkers. The utility of the following AF-predicting scores was tested: AS5F, Brown ESUS-AF, CHA2DS2-VASc, CHASE-LESS, HATCH, HAVOC, STAF and SURF.
Results
In univariate analyses increasing age, hypertension, left ventricle hypertrophy, dyslipidaemia, antiarrhythmic drugs usage, valvular heart disease, and neuroimaging findings of stroke due to intracranial vessel occlusions and previous ischemic lesions were associated with a higher likelihood of detected AF. In multivariate analysis, age was the only independent predictor of AF. All the AF-predicting scores showed significantly higher score levels for AF than non-AF patients. The STAF and the SURF scores provided the highest sensitivity and negative predictive values, while the AS5F and SURF reached an area under the receiver operating curve (AUC) > 0.7.
Conclusion
Clinical risk scores may guide a personalized evaluation approach in CS patients. Increasing awareness of the usage of available AF-predicting scores may optimize the arrhythmia detection pathway in stroke units.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The potential for diagnosing underlying atrial fibrillation (AF) in cryptogenic stroke (CS) is clinically relevant and may be crucial to the treatment regimen. Current knowledge suggests that one in three CS patients may be diagnosed with AF using prolonged cardiac rhythm monitoring [1, 2]. The duration of monitoring needed to detect paroxysmal arrhythmias seems to be inversely proportional to arrhythmia burden [3], so to properly rule out AF longer monitoring is of interest. Insertable cardiac monitors (ICMs) are the most effective tool revealing AF in up to 58% CS patients [4, 5]. The recent European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin recommends ICMs for the purpose of AF detection [6]. However, as most CS patients do not have underlying arrhythmia, the open clinical question is which patients should be prioritized for screening with ICM when the human and economic resources are not unlimited. Therefore, the selection process to pre-clarify individuals at the highest risk for underlying AF, who would profit the most from early ICM usage, is needed. Such an approach will secure high-risk patients’ faster access to this important investigational modality, as well as assuring proper resource utilization in a health-economic perspective. Furthermore, identifying CS patients with the lowest risk for underlying AF may redirect the search for causes other than arrhythmia.
Various risk factors for occult AF have been identified and several predictive scores have been proposed over time, none of them however being widely used in clinical practice [7]. In this paper, we are discussing the significance of AF predictors evaluated in The Nordic Atrial Fibrillation and Stroke (NOR-FIB) Study and the utility of eligible AF-predicting scores in clinical practice.
Methods
Study design and outcomes
The NOR-FIB study was an international prospective observational multicenter study designed to detect and quantify the burden of AF (≥ 2 min duration) in patients with CS or cryptogenic transient ischaemic attack (TIA) using an ICM (Reveal LINQ®) and to identify biomarkers of incident AF [8]. CS was defined as a non-lacunar brain infarct in the absence of extra- or intracranial atherosclerosis (≥ 50% luminal stenosis in arteries supplying the ischaemic area), high-risk cardiac source (including patent foramen ovale) and any other specific cause of stroke. To avoid bias, clinical TIA cases were included only if an acute lesion on magnetic resonance imaging was detected. The pre-enrolment evaluation and CS diagnosis were assessed by the treating physician. All patients underwent 12-lead ECG and minimum 24-h rhythm monitoring prior to enrolment. Transthoracic echocardiogram was mandatory, while a transesophageal echocardiogram was requested in patients’ ≤ 65 years. Measurements were done according to current guidelines [9,10,11]. Clinical data on vascular and AF risk factors according to predefined case report forms, and blood samples for biomarkers analyses were collected at enrolment and at a 12-month follow-up visit. All patients were monitored with the ICM for 12 months for arrhythmia detection [12].
Between January 2017 and September 2020, 259 finally included patients with CS or cryptogenic TIA from 18 participating centers in Norway, Denmark, and Sweden were monitored. Systematic ICM data evaluation verified paroxysmal AF or atrial flutter (≥ 2 min duration) in 74 (28.6%) patients. Results regarding arrhythmia detection are previously published [13]. For the purpose of AF prediction, differences between several clinical and paraclinical biomarkers in AF vs non-AF patients and the utility of eight existing AF-predicting scores were evaluated. Blood biomarker analyses were performed separately, showing significantly higher levels of cardiac biomarkers of which N-terminal pro-brain natriuretic peptide (NT-proBNP) was the strongest predictor of underlying AF (OR 4.8 [95% CI 1.8–13.0] in age and sex-adjusted model) [14].
Eligible risk scores tested in the NOR-FIB study, chosen due to data availability for each of the score components were as follows (presented predictive values according to original data*):
-
AS5F score calculated as Age × 0.76 + National Institutes of Health Stroke Scale (NIHSS) ≤ 5 (9 points) or > 5 (21 points). The threshold of 67.5 points reflects the AF risk of 5.2% (Number Needed to Screen, NNS ≤ 20). Area under the receiver operating characteristic curve (AUC) 0.75. Online calculator available at www.unimedizin-mainz.de/neurologie/header/as5f.html. [15]
-
Brown ESUS-AF score calculated according to age (65–74 years: 1 point, ≥ 75 years: 2 points) and left atrium (LA) enlargement (moderate or severe: 2 points). Possible total score 0–4. AUC 0.725. For the score of 2 sensitivity 62.9%, specificity 70.6% [16].
-
CHA2DS2-VASc calculated as 1 point each congestive heart failure, hypertension, diabetes, vascular disease, sex (female) and age (65–74), and 2 points for age ≥ 75 years and prior stroke/TIA. Possible score 0–9. C-index 0.62 [17].
-
CHASE-LESS score calculated as coronary artery disease (1 point), heart failure (1 point), age (1 point for every 10 years), stroke severity (1 point for NIHSS 6–13, 4 points for ≥ 14), hyperlipidaemia (− 1 point), diabetes (− 1 point), prior stroke/TIA (-1 point). Possible score 1–15. The likelihood of underlying AF categorized as low (1–3), low intermediate (4–6), high intermediate (7–9), high (≥ 10). C-index 0.730 [18].
-
HATCH score calculated as hypertension (1 point), age > 75 years (1 point), prior stroke/TIA (2 points), chronic obstructive pulmonary disease (1 point), heart failure (2 points). Possible score 0–7. C-index 0.653 [19, 20].
-
HAVOC score calculated as 1 point each for peripheral vascular disease and obesity (body mass index > 30); 2 points each for hypertension, age ≥ 75 years, valvular heart disease, and coronary disease; 4 points for congestive heart failure. Possible score 0–14. Stratifies patients into three risk groups, low (0–4), medium (5–9) and high (10–14) risk. AUC 0.77. For the score ≥ 4 sensitivity 35%, specificity 82.8%, positive predictive value (PPV) 31.8%, negative predictive value (NPV) 84.7% [21, 22].
-
STAF score calculated from the sum of the points for the 4 items: age > 62 years (2 points), NIHSS ≥ 8 (1 point), LA dilatation (2 points), absence of symptomatic extra- or intracranial stenosis ≥ 50% or clinic-radiological lacunar syndrome (3 points). Possible total score 0–8. AUC 0.94. The STAF score ≥ 5 identifies patients with AF with a sensitivity of 89% and a specificity of 88% [23].
-
SURF score calculated as Age × 10 + brain natriuretic peptide (BNP) (ng/l) in the acute phase > 700. CS patients in the NOR-FIB study fulfilled SURF criteria (AF-naive stroke without indication of long-term OAC, no symptomatic atherosclerotic stenosis ≥ 50%, symptomatic arterial dissection or lacunar stroke). AUC 0.842. PPV 47.7%. NPV 96.8% [24].
*The utility of the screening test is usually best expressed by its sensitivity (the percentage of true positive results) and NPV (correctly excluding individuals with no disease), and the AUC or c-index value as the measure of performance.
Cut-off values for the scores were chosen according to the optimal predictive performance from the original papers (AS5F, CHASE-LESS, STAF, SURF), a recommendation from the European Society of Cardiology (Brown ESUS-AF and HAVOC) [25], and comparison between the scores (CHA2DS2-VASc and HATCH) [15, 26].
Statistical analysis
Statistical evaluation was performed using IBM SPSS Statistics 28 software. Data were censored at the study exit, time of death or 12-month follow-up. Missing data on risk factors were registered as not present and included in the analysis. Patient characteristics and biomarker levels are presented as frequencies (%), mean (± standard deviation, SD) or median with interquartile range (IQR, Q1–Q3). Independent sample T-test or Mann–Whitney U-test, according to data distribution, was used to evaluate group differences for continuous variables and Pearson Chi-Square test or Fisher’s exact test for categorical variables. A p value < 0.05 was considered significant. Data analyses for arrhythmia detection and blood biomarker assessment are previously described [13, 14]. Binary logistic regression analyses were fitted to estimate the odds ratio (OR) together with a 95% confidence interval (CI). In a multivariate analysis (standard and stepwise), all relevant risk factors were included as covariates. For each patient, the eight AF-predicting scores were calculated and analyzed. The predictive performance of each score was assessed using receiver operating characteristic (ROC) curves, in addition to sensitivity, specificity, PPV and NPV. In the final evaluation, ROC analyses were performed simultaneously for comparison.
Results
Data from all the 259 were finally included and ICM-monitored patients were evaluated for AF predictors’ detection purpose. Table 1 presents between-group differences in baseline and discharge characteristics indicating potential predictors.
Summarizing, the AF patients were 10 years older and less often smokers, had higher rates of dyslipidaemia and hypertension pre-stroke and were more often using antiarrhythmic drugs compared to patients without AF. Echocardiographic diagnostic revealed more often left ventricle (LV) hypertrophy and valvular heart disease in AF patients, yet there was no significant difference regarding LA enlargement between the two groups. In addition, index stroke due to intracranial vessel occlusions verified on the angiography (27.4% vs 14.8%, p = 0.018) and previous ischaemic lesions on neuroimaging were more often seen in AF patients (51.4% vs 35.7%, p = 0.02).
In the univariate analyses, all the above-mentioned potential biomarkers were associated with the risk of AF event detected by ICM. However, in the multivariate analyses only age was associated with an increased likelihood of detecting AF, increasing the odds near 4 times for the age group 65–74 years, and 5 times for patients’ ≥ 75 years old compared to patients aged < 65 years (Table 2). Current smoking was inversely associated with AF risk, which is in line with previously reported findings [7].
As the second step, we tested the utility of eight eligible clinical risk scores for predicting new-onset AF detected after ischaemic stroke or TIA, performing the analyses on the NOR-FIB dataset (Table 3 and Fig. 1). All the analyses showed significantly higher score levels in AF than non-AF patients (p < 0.001) and rates of AF-positive patients due to the increasing score strata (p ≤ 0.003). The STAF score and the SURF score provided the highest sensitivities (88.7% and 92.2%) and the highest NPV (87.3% and 92.4%) respectively. AF detection increased with the STAF ≥ 5 to 33.7% vs 12.7% for the score < 5. For the SURF score > 700 AF detection reached 41.8% vs 7.6% for the score < 700. The AUCs based on the continuous score values were as follows: AS5F 0.741 (95% CI 0.678–0.804); Brown ESUS-AF 0.672 (95% CI 0.596–0.747); CHA2DS2-VASc 0.679 (95% CI 0.606–0.751); CHASE-LESS 0.690 (95% CI 0.619–0.760); HATCH 0.644 (95% CI 0.569–0.719); HAVOC 0.664 (95% CI 0.591–0.736); STAF 0.645 (95% CI 0.566–0.724) and SURF 0.755 (95% CI 0.687–0.824). The AS5F score and the SURF score were the only one considered acceptable reaching AUC > 0.7. AF was detected in 22.6% of patients with the AS5F score < 67.5 and 48.3% of patients with AS5F ≥ 67.5. Performance of the AS5F score was similar compared to validation data, while for the STAF and the SURF score it was lower [15, 26, 27].

Utility of the eight clinical scores in the NOR-FIB study predicting AF in CS and TIA patients. AUC for continuous score values. Similar AUC results were obtained also when corrected for the n difference between score (all scores tested simultaneously): AS5F 0.719, Brown ESUS-AF 0.674, CHA2DS2-VASc 0.674, CHASE-LESS 0.664, HATCH 0.639, HAVOC 0.659, STAF 0.673, SURF 0.736
Cut-off values for the scores chosen according to the optimal predictive performance from the original papers (AS5F, CHASE-LESS, STAF, SURF), recommendation from the European Society of Cardiology [25] (Brown ESUS-AF and HAVOC), and comparison between the scores (CHA2DS2-VASc and HATCH) [15,16,17,18,19,20,21,22,23,24,25,26].
Discussion:
The intention of the current analysis, assessing the performance of the eight eligible AF-predicting scores in the NOR-FIB study, was to better address the work-up of identifying high-risk patients to optimize the arrhythmia detection pathway in CS and TIA patients. All the validated clinical prediction scores that were tested; AS5F, Brown ESUS-AF, CHA2DS2-VASc, CHASE-LESS, HATCH, HAVOC, STAF and SURF demonstrated significantly higher score levels in AF than non-AF patients. The STAF and the SURF score predicted AF with the highest sensitivity and NPV, while the AS5F and the SURF score reached an acceptable AUC > 0.7. The SURF score showed however the best utility expressed by the highest levels of all the three values (Fig. 1).
Although AF was common in our study, revealed in nearly 1 in 3 patients systematically monitored by ICM for 12 months, most patients did not have underlying arrhythmia. Our findings emphasize the advantage of risk-stratifying tools for targeted evaluation of CS patients identifying individuals profiting from the early start of prolonged rhythm monitoring. In addition, implementing scores in the diagnostic approach could cover an important but unmet need—the recognition of patients with the lowest risk of underlying AF, in whom the extended evaluation should rather be redirected towards other causes.
AF predictors in CS
Risk stratification for underlying AF in stroke patients can be attempted by scrutinizing comorbidities predisposing to AF, biomarkers indicating atrial cardiopathy (the substrate for arrhythmia), and neuroimaging lesion patterns indicating embolic stroke [29,30,31,32,33]. Even though increasing age is the most prominent risk factor, burden of comorbidities including hypertension, diabetes mellitus, heart failure, coronary artery disease, chronic kidney disease and obesity significantly contribute to AF development and progression [29]. Several ECG and echocardiographic findings increase the suspicion of atrial disease and AF [34,35,36,37]. Elevated cardiac biomarkers levels [14, 38,39,40] are also reported as a potentially surrogate marker for underlying paroxysmal AF and being incorporated in some of the predictive scores [41, 42]. The latest systematic review and meta-analysis on biomarkers for post-stroke AF detection assessed 69 multimodal markers and identified in all 26 clinical, ECG and blood-based biomarkers [7].
In the NOR-FIB study, several known clinical and paraclinical findings were associated with AF risk in univariate analysis (Table 2). Among the oldest CS patients (≥ 75 years) and those using antiarrhythmic drugs at admission, the likelihood of underlying AF was almost 50%. However, in multivariate analysis, the only independent predictors of AF were increasing age and smoking status. Our findings may be explained by the fact that several of the other AF risk factors are also closely linked, in different overlapping pathologies, to stroke in general. This is further the reason while a single biomarker, including cardiac natriuretic peptides should not be used as a decision-making tool [40], emphasizing the use of scores rather than a stand-alone approach.
AF-risk stratification scores
Clinical risk scores may guide personalized evaluation approach in CS patients and contribute to more optimal access to key diagnostics. However, the criteria used to define patients at risk of underlying AF should be validated, easy to apply in the first days after admission, and commonly available in all units treating stroke patients. Scores with the highest sensitivity and highest NPV correctly identifying patients at the risk have the best utility. Recent systematic review on the use of risk scores for predicting new AF after stroke or TIA highlights seventeen different scores [41]. Age, LA size, hypertension, congestive heart failure, previous stroke/TIA and NIHSS levels are the throughout most common highly relevant components indicating underlying AF. All the scores are potentially eligible for applying during the diagnostic work-up of stroke patients, yet in more complex scores focus on proper clinical assessment covering the actual score components is essential. Five of these seventeen scores have been developed exclusively for CS or ESUS (embolic stroke of undetermined source) patients to predict AF: AF-ESUS, ACTEL, NDAF, Brown ESUS-AF and HAVOC [17, 18, 44,45,46]. The first three scores were not applicable to test in the NOR-FIB study due to the use of different variables (LA measurements more often including volume rather than area, lack of specific data on non-stenotic plaques or tricuspid regurgitation). The last two scores, Brown ESUS-AF [16] and HAVOC score [21] showed lower sensitivity and NPV than the STAF and SURF, and lower AUC values than AS5F and SURF scores which predicted AF best. Even though the Brown-ESUS score is similar to the STAF score, the last also includes stroke severity (NIHSS) and may be used in combination with the D-dimer, increasing its accuracy (sensitivity 95%, specificity 100%) [47]. The more comprehensive HAVOC score, however, may be more relevant for younger or multimorbid CS patients’ population. Nevertheless, Brown ESUS-AF and HAVOC scores have lately been proposed by the European Society of Cardiology for the guidance of further prolonged ECG monitoring in CS [25]. In case of negative initial diagnostics (24 h ECG, echocardiography and hematological evaluation), if Brown ESUS-AF ≥ 2 or HAVOC score ≥ 4 prolonged ECG monitoring with external devices up to first 30 days or ICMs directly is recommended. Recently another AF-predicting score for CS patients monitored by ICM has been proposed, PROACTIA score based on premature atrial beats (PAC/24t), P-wave duration, P-wave morphology, and LA end-systolic volume index [48]. The score enables the identification of patients with low, intermediate and a high risk of subsequent AF detection (AUC 0.79), yet has a complicated formula for which the app-based solution is needed (at the moment unavailable) limiting its usability. Another new score stratifying AF risk in CS, the Graz AF Risk Score includes age, NT-proBNP, supraventricular premature beats, atrial runs, atrial enlargement, left ventricular ejection fraction and brain imaging markers [42]. This score was not applicable for us to test either, as we did not count supraventricular premature beats or atrial runs systematically. The usability of both the newest scores may be limited in stroke units mostly applying in-hospital telemetry instead of Holter monitoring, where atrial runs or premature beats counting is less used in the real-time evaluation assessment.
Proper selection of patients for ICM usage
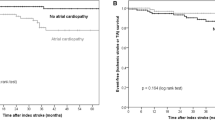
Initial work-up of CS requires wide radiological expertise and good quality of the cardiac and vascular evaluation to determine the probable stroke mechanism. Cardiac investigation focusing on the detection of cardio-aortic sources other than AF (Fig. 2), as well as the atrial cardiopathy signs is crucial in diagnosing cardioembolic stroke [49]. Furthermore, clinical or radiological evidence of multiple vascular territory strokes, cortical or posterior circulation lesions, vessel occlusions and greater stroke severity in the absence of significant stenosis in the ipsilateral artery should also lead the suspicion of potentially underlying cardioembolism and AF, if other cardiac sources excluded [33]. In-hospital ECG monitoring for at least 48 h to rule out AF and reflection on other possible causes of brain ischaemia (i.e., genetic disorders and low-risk cardiac sources) should be completed before the stroke may be classified as cryptogenic [6, 50].

Overview of the cardiac sources of embolism structured after The Stop Stroke TOAST system [49]. AF: atrial fibrillation, PAF: paroxysmal AF, LA: left atrium, LV: left ventricle, MI: myocardial infarction, cMI: chronic myocardial infarction, CHF: congestive heart failure, EF: Left ventricular ejection fraction, TOAST: the Trial of Org 10,172 in Acute Stroke Treatment
For the purpose of prevention, it is realistic to recommend ICM monitoring only to eligible CS patients where underlying AF will affect change in secondary prevention (including those with contraindications to OAC, due to the advent of LA appendage closure procedures). From a socioeconomic perspective, CS patients with short life expectancy (< 1–2 year) or high disability (modified Rankin Scale ≥ 4 due to index stroke or other medical condition with no prospect of recovery), in whom the risk of suffering even a devastating AF-related stroke is less relevant for the outcome should be excluded. Patients with the highest AF suspicion should start prolonged monitoring as early as possible, as recurrent stroke often occurs within the first weeks. The best risk stratification approach is probably using scores combining age (OR 3.26), markers of atrial cardiopathy (OR 2.12–7.79), NIHSS (OR 2.5) and cardiac natriuretic peptides (OR 13.73) which, according to current knowledge, are the strongest predictors of AF (7). The scores that performed best in the present study, the AS5F, STAF and SURF highlight these biomarkers. In a recent study validating AF-predicting scores, the AS5F score demonstrated adequate discrimination (c-index 0.730), being useful in selecting patients for invasive arrhythmia monitoring [27]. The usefulness of the STAF and SURF score is due to its high NPV correctly identifying patients with the lowest AF-risk.
Limitations
Our study has some minor limitations. First, functional and structural changes in the LA constituting the substrate for AF might have been even more frequent. As completion of the specified case report form for echo data was optional, some of the valuable information on atrial size was missing in 32 patients. Furthermore, the negative impact of hypertension on AF risk might have been leveled by the usage of antihypertensive drugs [43]. At last, there was no formal test of the performance of the evaluated clinical risk scores, however, in simultaneous ROC analysis scores’ AUC were similar to the AUC for continuous variables of each test. The best performance of the STAF, SURF and AS5F score may be due to a high proportion of patients ≥ 60 years (near 70%), yet the proportion ≥ 70 years was 40%, and ≥ 80 years 12%. However, as increasing age has shown to be one of the strongest predictors of AF in several similar studies evaluating biomarkers, and the risk factor that predicted AF among our patients, the findings are not surprising.
Conclusion
Advanced age and comorbidity scores provided useful information to predict an increased risk of AF in this CS population. Our findings may contribute to a better patient selection for prolonged cardiac rhythm monitoring, by rising awareness on the usage of available AF-predicting scores in optimizing the arrhythmia detection pathway in stroke units. In addition, for patients at the lowest risk of underlying AF the benefit could be an earlier focus on causes other than the arrhythmia. The efforts enhancing the clinical evaluation approach by combining the strongest clinical and paraclinical AF predictors in new scores (or improving the existing) should be prioritized, while new studies and trials should highlight the value of AF prediction as a precision medicine in CS patients.
Data availability
The data that support the findings of this study are available, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request, for details please contact Anne Hege Aamodt (a.h.aamodt@medisin.uio.no).
References:
Yaghi S, Bernstein RA, Passman R, Okin PM, Furie KL (2017) Cryptogenic stroke: research and practice. Circ Res 120(3):527–540. https://doi.org/10.1161/CIRCRESAHA.116.308447
Tsivgoulis G, Triantafyllou S, Palaiodimou L, Grory BM, Deftereos S, Köhrmann M, Dilaveris P, Ricci B, Tsioufis K, Cutting S, Magiorkinis G, Krogias C, Schellinger PD, Dardiotis E, Rodriguez-Campello A, Cuadrado-Godia E, Aguiar de Sousa D, Sharma M, Gladstone DJ, Sanna T, Wachter R, Furie KL, Alexandrov AV, Yaghi S, Katsanos AH (2022) Prolonged cardiac monitoring and stroke recurrence: a meta-analysis. Neurology 98(19):e1942–e1952. https://doi.org/10.1212/WNL.0000000000200227
Sposato LA, Andrade J (2022) Prolonged cardiac monitoring for atrial fibrillation detection after stroke: in search of the elusive sweet spot. Neurology 98(19):781–783. https://doi.org/10.1212/WNL.0000000000200333
Lu Y, Diao SS, Huang SJ, Zhao JJ, Ye MF, Yao FR, Kong Y, Xu Z (2021) Insertable cardiac monitors for detection of atrial fibrillation after cryptogenic stroke: a meta-analysis. Neurol Sci 42(10):4139–4148. https://doi.org/10.1007/s10072-021-05104-6
Cuadrado-Godia E, Benito B, Ois A, Vallès E, Rodríguez-Campello A, Giralt-Steinhauer E, Cabrera S, Alcalde O, Jiménez-López J, Jiménez-Conde J, Martí-Almor J, Roquer J (2020) Ultra-early continuous cardiac monitoring improves atrial fibrillation detection and prognosis of patients with cryptogenic stroke. Eur J Neurol 27(2):244–250. https://doi.org/10.1111/ene.14061
Rubiera M, Aires A, Antonenko K, Lémeret S, Nolte CH, Putaala J, Schnabel RB, Tuladhar AM, Werring DJ, Zeraatkar D, Paciaroni M (2022) European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin. Eur Stroke J 7(3):VI. https://doi.org/10.1177/23969873221099478
Cameron A, Cheng HK, Lee RP, Doherty D, Hall M, Khashayar P, Lip GYH, Quinn T, Abdul-Rahim A, Dawson J (2021) Biomarkers for atrial fibrillation detection after stroke: systematic review and meta-analysis. Neurology 97(18):e1775–e1789. https://doi.org/10.1212/WNL.0000000000012769
Ratajczak-Tretel B, Lambert AT, Johansen H, Halvorsen B, Bjerkeli V, Russell D, Sandset EC, Ihle-Hansen H, Eriksen E, Næss H, Novotny V, Khanevski AN, Truelsen TC, Idicula T, Ægidius KL, Tobro H, Krogseth SB, Ihle-Hansen H, Hagberg G, Kruuse C, Arntzen K, Bakkejord GK, Villseth M, Nakstad I, Eldøen G, Shafiq R, Gulsvik A, Kurz M, Rezai M, Sømark J, Tingvoll SH, Jonassen C, Ingebrigtsen S, Steffensen LH, Kremer C, Atar D, Aamodt AH (2019) Atrial fibrillation in cryptogenic stroke and transient ischaemic attack—the Nordic Atrial Fibrillation and Stroke (NOR-FIB) Study: Rationale and design. Eur Stroke J 4(2):172–180. https://doi.org/10.1177/2396987319837089
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT, Sutton M, Stewart W, American Society of Echocardiography’s Nomenclature and Standards Committee; Task Force on Chamber Quantification; American College of Cardiology Echocardiography Committee; American Heart Association; European Association of Echocardiography, European Society of Cardiology. Recommendations for chamber quantification (2006) Recommendations for chamber quantification. Eur J Echocardiogr 7(2):79–108. https://doi.org/10.1016/j.euje.2005.12.014
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28(1):1-39.e14. https://doi.org/10.1016/j.echo.2014.10.003
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group (2016) 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37(27):2129–2200. https://doi.org/10.1093/eurheartj/ehw128
Tomson TT, Passman R (2015) The Reveal LINQ insertable cardiac monitor. Expert Rev Med Devices 12(1):7–18. https://doi.org/10.1586/17434440.2014.953059
Ratajczak-Tretel B, Tancin Lambert A, Al-Ani R, Arntzen K, Bakkejord GK, Bekkeseth HMO, Bjerkeli V, Eldøen G, Gulsvik A, Halvorsen B, Høie GA, Ihle-Hansen H, Ihle-Hansen H, Ingebrigtsen S, Johansen H, Kremer C, Krogseth SB, Kruuse C, Kurz M, Nakstad I, Novotny V, Naess H, Qazi R, Rezai MK, Rørholt DM, Steffensen LH, Sømark J, Tobro H, Truelsen TC, Wassvik L, Ægidius KL, Atar D, Aamodt AH, NOR-FIB study Group (2022) Atrial fibrillation in cryptogenic stroke and TIA patients in The Nordic Atrial Fibrillation and Stroke Study (NOR-FIB) Study: main results. Eur Stroke J. https://doi.org/10.1177/23969873221123122
Tancin Lambert A, Ratajczak-Tretel B, Al-Ani R, Arntzen K, Bakkejord GK, Bekkeseth HMO, Bjerkeli V, Eldøen G, Gulsvik AK, Halvorsen B, Høie GA, Ihle-Hansen H, Ihle-Hansen H, Ingebrigtsen S, Johansen H, Kremer C, Krogseth SB, Kruuse C, Kurz M, Nakstad I, Novotny V, Naess H, Qazi R, Rezai MK, Rørholt DM, Steffensen LH, Sømark J, Tobro H, Truelsen TC, Wassvik L, Ægidius KL, Pesonen M, de Melis M, Atar D, Aamodt AH, NOR-FIB study Group (2023) Biomarkers predictive of atrial fibrillation in patients with cryptogenic stroke. Insights from The Nordic Atrial Fibrillation and Stroke (NOR-FIB) Study. Eur J Neurol. https://doi.org/10.1111/ene.15746
Uphaus T, Weber-Krüger M, Grond M, Toenges G, Jahn-Eimermacher A, Jauss M, Kirchhof P, Wachter R, Gröschel K (2019) Development and validation of a score to detect paroxysmal atrial fibrillation after stroke. Neurology 92(2):e115–e124. https://doi.org/10.1212/WNL.0000000000006727
Ricci B, Chang AD, Hemendinger M, Dakay K, Cutting S, Burton T, Mac Grory B, Narwal P, Song C, Chu A, Mehanna E, McTaggart R, Jayaraman M, Furie K, Yaghi S (2018) A simple score that predicts paroxysmal atrial fibrillation on outpatient cardiac monitoring after embolic stroke of unknown source. J Stroke Cerebrovasc Dis 27(6):1692–1696. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.01.028
Liu R, Yang X, Li S, Jiang Y, Wang Y, Wang Y (2018) Modified CHADS2 and CHA2DS2-VASc scores to predict atrial fibrillation in acute ischemic stroke patients. J Clin Neurosci 51:35–38. https://doi.org/10.1016/j.jocn.2018.02.016
Hsieh CY, Lee CH, Sung SF (2020) Development of a novel score to predict newly diagnosed atrial fibrillation after ischemic stroke: the CHASE-LESS score. Atherosclerosis 295:1–7. https://doi.org/10.1016/j.atherosclerosis.2020.01.003
Tischer TS, Schneider R, Lauschke J, Diedrich D, Kundt G, Bänsch D (2015) Prevalence of atrial fibrillation and the HATCH score: Intensified monitoring of patients with high HATCH score. Herz 40(5):803–808. https://doi.org/10.1007/s00059-015-4305-4
Hsieh CY, Lee CH, Wu DP, Sung SF (2018) Prediction of new-onset atrial fibrillation after first-ever ischemic stroke: a comparison of CHADS2, CHA2DS2-VASc and HATCH scores and the added value of stroke severity. Atherosclerosis 272:73–79. https://doi.org/10.1016/j.atherosclerosis.2018.03.024
Kwong C, Ling AY, Crawford MH, Zhao SX, Shah NH (2017) A clinical score for predicting atrial fibrillation in patients with cryptogenic stroke or transient ischemic attack. Cardiology 138(3):133–140. https://doi.org/10.1159/000476030
Zhao SX, Ziegler PD, Crawford MH, Kwong C, Koehler JL, Passman RS (2019) Evaluation of a clinical score for predicting atrial fibrillation in cryptogenic stroke patients with insertable cardiac monitors: results from the CRYSTAL AF study. Ther Adv Neurol Disord 11(12):1756286419842698. https://doi.org/10.1177/1756286419842698
Suissa L, Bertora D, Lachaud S, Mahagne MH (2009) Score for the targeting of atrial fibrillation (STAF): a new approach to the detection of atrial fibrillation in the secondary prevention of ischemic stroke. Stroke 40(8):2866–2868. https://doi.org/10.1161/STROKEAHA.109.552679
Suissa L, Bertora D, Kalle R, Bruno C, Romero G, Mahagne MH (2019) SURF (stroke with underlying risk of atrial fibrillation): proposals for a definition. Clin Neurol Neurosurg 182:43–48. https://doi.org/10.1016/j.clineuro.2019.04.028
Dilaveris PE, Antoniou CK, Caiani EG, Casado-Arroyo R, Climent AΜ, Cluitmans M, Cowie MR, Doehner W, Guerra F, Jensen MT, Kalarus Z, Locati ET, Platonov P, Simova I, Schnabel RB, Schuuring M, Tsivgoulis G, Lumens J (2022) ESC Working Group on e-Cardiology Position Paper: accuracy and reliability of electrocardiogram monitoring in the detection of atrial fibrillation in cryptogenic stroke patients : In collaboration with the Council on Stroke, the European Heart Rhythm Association, and the Digital Health Committee. Eur Heart J Digit Health 3(3):341–358. https://doi.org/10.1093/ehjdh/ztac026. (PMID:36712155;PMCID:PMC9707962)
Suissa L, Mahagne MH, Lachaud S (2011) Score for the targeting of atrial fibrillation: a new approach to diagnosing paroxysmal atrial fibrillation. Cerebrovasc Dis 31(5):442–447. https://doi.org/10.1159/000323852
Hsieh CY, Kao HM, Sung KL, Sposato LA, Sung SF, Lin SJ (2022) Validation of risk scores for predicting atrial fibrillation detected after stroke based on an electronic medical record algorithm: a registry-claims-electronic medical record linked data study. Front Cardiovasc Med. 9:888240. https://doi.org/10.3389/fcvm.2022.888240
Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, Kamel H, Kernan WN, Kittner SJ, Leira EC, Lennon O, Meschia JF, Nguyen TN, Pollak PM, Santangeli P, Sharrief AZ, Smith SC Jr, Turan TN, Williams LS (2021) 2021 Guideline for the Prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 52(7):e364–e467. https://doi.org/10.1161/STR.0000000000000375. (Epub 2021 May 24. Erratum in: Stroke. 2021 Jul;52(7):e483-e484)
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, Fauchier L, Filippatos G, Kalman JM, La Meir M, Lane DA, Lebeau JP, Lettino M, Lip GYH, Pinto FJ, Thomas GN, Valgimigli M, Van Gelder IC, Van Putte BP, Watkins CL, ESC Scientific Document Group (2021) 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 42(5):373–498. https://doi.org/10.1093/eurheartj/ehaa612
Delgado V, Di Biase L, Leung M, Romero J, Tops LF, Casadei B, Marrouche N, Bax JJ (2017) Structure and function of the left atrium and left atrial appendage: AF and stroke implications. J Am Coll Cardiol 70(25):3157–3172. https://doi.org/10.1016/j.jacc.2017.10.063
Blum S, Meyre P, Aeschbacher S, Berger S, Auberson C, Briel M, Osswald S, Conen D (2019) Incidence and predictors of atrial fibrillation progression: a systematic review and meta-analysis. Heart Rhythm 16(4):502–510. https://doi.org/10.1016/j.hrthm.2018.10.022
Kato Y, Takahashi S (2022) Atrial cardiopathy and cryptogenic stroke. Front Neurol 13:839398. https://doi.org/10.3389/fneur.2022.839398
Sharobeam A, Churilov L, Parsons M, Donnan GA, Davis SM, Yan B (2020) Patterns of infarction on MRI in patients with acute ischemic stroke and cardio-embolism: a systematic review and meta-analysis. Front Neurol 11:606521. https://doi.org/10.3389/fneur.2020.606521
German DM, Kabir MM, Dewland TA et al (2016) Atrial fibrillation predictors: importance of the electrocardiogram. Ann Noninvasive Electrocardiol 21(1):20–29. https://doi.org/10.1111/anec
Guichard JB, Guasch E, Roche F, Da Costa A, Mont L (2022) Premature atrial contractions: a predictor of atrial fibrillation and a relevant marker of atrial cardiomyopathy. Front Physiol 13:971691. https://doi.org/10.3389/fphys.2022.971691
Ma J, Chen Q, Ma S (2021) Left atrial fibrosis in atrial fibrillation: mechanisms, clinical evaluation and management. J Cell Mol Med 25(6):2764–2775. https://doi.org/10.1111/jcmm.16350
Suwa Y, Miyasaka Y, Taniguchi N, Harada S, Nakai E, Shiojima I (2022) Atrial fibrillation and stroke: importance of left atrium as assessed by echocardiography. J Echocardiogr 20(2):69–76. https://doi.org/10.1007/s12574-021-00561-6
Fonseca AC, Coelho P (2021) Update on biomarkers associated to cardioembolic stroke: a narrative review. Life (Basel) 11(5):448. https://doi.org/10.3390/life11050448
Harpaz D, Bajpai R, Ng GJL, Soljak M, Marks RS, Cheung C, Arumugam TV, Quek AML, Tok AIY, Seet RCS (2021) Blood biomarkers to detect new-onset atrial fibrillation and cardioembolism in ischemic stroke patients. Heart Rhythm 18(6):855–861. https://doi.org/10.1016/j.hrthm.2021.01.032
Zhang K, Kamtchum-Tatuene J, Li M, Jickling GC (2021) Cardiac natriuretic peptides for diagnosis of covert atrial fibrillation after acute ischaemic stroke: a meta-analysis of diagnostic accuracy studies. Stroke Vasc Neurol 6(1):128–132. https://doi.org/10.1136/svn-2020-000440
Kishore AK, Hossain MJ, Cameron A, Dawson J, Vail A, Smith CJ (2022) Use of risk scores for predicting new atrial fibrillation after ischemic stroke or transient ischemic attack—a systematic review. Int J Stroke 17(6):608–617. https://doi.org/10.1177/17474930211045880
Kneihsl M, Bisping E, Scherr D, Mangge H, Fandler-Höfler S, Colonna I, Haidegger M, Eppinger S, Hofer E, Fazekas F, Enzinger C, Gattringer T (2022) Predicting atrial fibrillation after cryptogenic stroke via a clinical risk score-a prospective observational study. Eur J Neurol 29(1):149–157. https://doi.org/10.1111/ene.15102
Dzeshka MS, Shantsila A, Shantsila E, Lip GYH (2017) Atrial fibrillation and hypertension. Hypertension 70(5):854–861. https://doi.org/10.1161/HYPERTENSIONAHA.117.08934
Bugnicourt JM, Flament M, Guillaumont MP, Chillon JM, Leclercq C, Canaple S, Lamy C, Godefroy O (2013) Predictors of newly diagnosed atrial fibrillation in cryptogenic stroke: a cohort study. Eur J Neurol 20(10):1352–1359. https://doi.org/10.1111/ene.12017
Ntaios G, Perlepe K, Lambrou D, Sirimarco G, Strambo D, Eskandari A, Karagkiozi E, Vemmou A, Korompoki E, Manios E, Makaritsis K, Vemmos K, Michel P (2021) Identification of patients with embolic stroke of undetermined source and low risk of new incident atrial fibrillation: the AF-ESUS score. Int J Stroke 16(1):29–38. https://doi.org/10.1177/1747493020925281
Muscari A, Barone P, Faccioli L, Ghinelli M, Pastore Trossello M, Puddu GM, Spinardi L, Zoli M (2020) Usefulness of the ACTEL score to predict atrial fibrillation in patients with cryptogenic stroke. Cardiology 145(3):168–177. https://doi.org/10.1159/000505262
Liu LB, Guo YD, Xu AD, Zhong JX, Zhuo WY (2018) Diagnostic value of STAF score in combination with D-dimer in cardioembolism. PLoS ONE 13(10):e0204838. https://doi.org/10.1371/journal.pone.0204838
Skrebelyte-Strøm L, Rønning OM, Dahl FA, Steine K, Kjekshus H (2022) Prediction of occult atrial fibrillation in patients after cryptogenic stroke and transient ischaemic attack: PROACTIA. Europace 24(12):1881–1888. https://doi.org/10.1093/europace/euac092
Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ (2005) An evidence-based causative classification system for acute ischemic stroke. Ann Neurol 58(5):688–697. https://doi.org/10.1002/ana.20617
Bersano A, Kraemer M, Burlina A, Mancuso M, Finsterer J, Sacco S, Salvarani C, Caputi L, Chabriat H, Oberstein SL, Federico A, Lasserve ET, Hunt D, Dichgans M, Arnold M, Debette S, Markus HS (2021) Heritable and non-heritable uncommon causes of stroke. J Neurol 268(8):2780–2807. https://doi.org/10.1007/s00415-020-09836-x
Acknowledgements
We would like to thank Maiju Pesonen and Thomas von Lueder for their assistance and guidance in this research, and all participating stroke units in Norway, Denmark, and Sweden for their contribution. We gratefully honour the late Professor David Russell for his leadership in this research.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital). NOR-FIB is an investigator-driven academic study, supported by Oslo University Hospital, Norwegian Health Association, South-Eastern Norway Regional Health Authority (BRT and ATL PhD fellowship) and Østfold Hospital Trust. Devices were partly provided by Medtronic.
Author information
Authors and Affiliations
Consortia
Contributions
AHA, DR, DA researched the literature and conceived the NOR-FIB study. BRT, ATL, DR, DA, AHA were involved in protocol development. BRT, ATL, KA, GKB, HMOB, GE, AG, HIH, HIH, SI, HJ, CK, SBK, CK, MK, IN, VN, KN, RQ, MKR, DMR, LHS, JS, HT, TCT, LW, KLÆ, AHA were involved in patient recruitment and follow-up. RAA, GAH, DA, ATL, BRT were responsible for ECG evaluations. BRT wrote the first manuscript draft and was responsible for the statistical evaluation of the data consulting with a statistician. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
AHA has received travel support, and honoraria for advice or lecturing from Bayer, Boehringer Ingelheim, BMS, Abbvie, Teva, Novartis, Roche, Pfizer, and Teva, research grant from Boehringer Ingelheim. DA has received honoraria and consultation fees from Actelion, Amgen, AstraZeneca, BMS/Pfizer, Bayer, Boehringer-Ingelheim, MSD, Novartis, Pharmacosmos, Roche Diagnostics, Sanofi, Takeda, and Vifor Pharma, and research funding (to the institution) from BMS/Pfizer, Bayer, Roche Diagnostics and Medtronic. BRT and ATL have received travel funding from Medtronic.
Ethical approval
The study was performed according to Helsinki Declaration and was approved by the Norwegian Regional Committee for Medical and Health Research Ethics (REK 2013/2371) and local ethics committees in Denmark and Sweden. Written consent was obtained from all participants. Patients´ data were collected through the European Cerebrovascular Research Infrastructure (ECRI) and stored in the Services for Sensitive Data (TSD) at the University of Oslo. Study is registered at ClinicalTrials.gov (NCT02937077).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ratajczak-Tretel, B., Lambert, A.T., Al-Ani, R. et al. Prediction of underlying atrial fibrillation in patients with a cryptogenic stroke: results from the NOR-FIB Study. J Neurol 270, 4049–4059 (2023). https://doi.org/10.1007/s00415-023-11680-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-11680-8