
Abstract
Background
Cervical dystonia is characterized by a variable pattern of neck muscle involvement. Due to the lack of a diagnostic test, cervical dystonia diagnosis is based on clinical examination and is therefore subjective. The present work was designed to provide practical guidance for clinicians in confirming or refuting suspected cervical dystonia.
Methods
Participants were video recorded according to a standardized protocol to assess 6 main clinical features possibly contributing to cervical dystonia diagnosis: presence of repetitive, patterned head/neck movements/postures inducing head/neck deviation from neutral position (item 1); sensory trick (item 2); and red flags related to conditions mimicking dystonia that should be absent in dystonia (items 3–6). Inter-/intra-rater agreement among three independent raters was assessed by k statistics. To estimate sensitivity and specificity, the gold standard was cervical dystonia diagnosis reviewed at each site by independent senior neurologists.
Results
The validation sample included 43 idiopathic cervical dystonia patients and 41 control subjects (12 normal subjects, 6 patients with isolated head tremor, 4 with chorea, 6 with tics, 4 with head ptosis due to myasthenia or amyotrophic lateral sclerosis, 7 with orthopedic/rheumatologic neck diseases, and 2 with ocular torticollis). The best combination of sensitivity and specificity was observed considering all the items except for an item related to capability to voluntarily suppress spasms (sensitivity: 96.1%; specificity: 81%).
Conclusions
An accurate diagnosis of cervical dystonia can be achieved if, in addition to the core motor features, we also consider some clinical features related to dystonia mimics that should be absent in dystonia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to the most recent consensus update [1], dystonia is defined as a condition characterized by “sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both. Dystonic movements are typically patterned, twisting, and may be tremulous. Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation” [1].
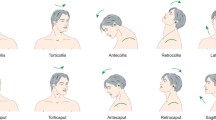
Cervical dystonia (CD), the most frequent form of focal dystonia, is characterized by a variable pattern of neck muscle involvement, leading to clinically heterogeneous directional presentations, such as torticollis, laterocollis, retrocollis, or anterocollis [2]. Patients may also have additional signs and symptoms, including shoulder elevation, neck/shoulder pain, or head tremor, and may benefit from the use of sensory tricks, a highly specific maneuver that may induce transient amelioration of dystonia [3,4,5]. In some patients dystonic activity may also spread to other body parts [6,7,8,9].
Due to the lack of a diagnostic test, CD diagnosis is based on clinical examination and is therefore subjective [10]. As an example, a study on CD incidence in northern California found that up to 65% of patients may be incorrectly diagnosed prior to receiving a correct diagnosis [11]. Further support of a high rate of CD underdiagnosis as a ubiquitous phenomenon also derives from family-based studies from studies assessing diagnostic delay in several geographic areas [12,13,14,15,16]. Diagnostic errors may largely be due to the clinical variability of CD but also to the existence of several related conditions, for example, pseudodystonia mimicking the abnormal movements or postures of CD [17, 18]. In the case of CD, dystonia mimics may include neck chorea producing non-repetitive head movements [19]; neck tics associated with ability to mentally suppress the spasms [20]; orthopedic neck diseases (like atlanto-axial and shoulder subluxation, or fracture of the cervical vertebrae), rheumatologic neck diseases, and posterior fossa tumors, all leading to tonic postures or movement of the head [21]; lower motor neuron disease/myopathy/myasthenia gravis inducing weakness of the neck muscles opposite to the abnormal posture [22, 23]; and ocular torticollis characterized by diplopia caused by the voluntary correction of the abnormal neck posture [24].
According to expert opinion [25], the clinical diagnosis of CD should rely on the core motor features highlighted in the revised definition of dystonia [1], and the exclusion of clinical red flags related to neurological/non-neurological conditions mimicking dystonia (that would be expected to be absent in dystonia) [25]. Whether these key features may help diagnose CD and differentiate the condition from other disorders of the neck that resemble dystonia has never been assessed in terms of diagnostic sensitivity and specificity. The present work was designed in the attempt to minimize sources of diagnostic errors and to provide practical guidance for clinicians in confirming or refuting suspected CD.
Methods
Participants were identified from among outpatients attending the movement disorder clinic of the University of Cagliari and Sapienza University of Rome. Inclusion criteria for both case and control subjects were age 18 or older, any sex, and the willingness and mental/physical ability to sign informed consent and participate in the protocol. Case patients were enrolled if they had a diagnosis of focal idiopathic CD made by an experienced movement disorder neurologist [25, 26]. Exclusion criteria were secondary CD and co-existing medical conditions/surgical interventions that could confound assessment of CD. Botulinum neurotoxin (BoNT) treatment was performed at least 12 weeks before the examination. The control group included normal subjects and a group of patients with head/neck impairment that could be confused with CD [18], i.e., isolated head tremor; non-repetitive head movements due to chorea; head tics associated with the ability to mentally suppress spasms; fixed involuntary neck postures due to orthopedic neck diseases (like atlanto-axial and shoulder subluxation or cervical vertebrae fracture), rheumatologic neck diseases, or posterior fossa tumors; focal weakness of the neck muscles opposite the side of abnormal posture due to lower motor neuron disease/myopathy/myasthenia gravis; and diplopia caused by the voluntary correction of abnormal neck posture due to ocular torticollis (Supplemental Table 1).
To assess diagnostic accuracy we focused on the following clinical items: (i) presence of repetitive, patterned head/neck movements/postures inducing head/neck deviation from neutral position (item 1, derived from the 2013 revised definition of dystonia) [1]; (ii) sensory trick (item 2); and (iii) red flags related to conditions mimicking dystonia that would be expected to be absent in dystonia (items 3 to 6). In the latter group, we took into account fixed head/neck deviation from neutral position (item 3, a feature distinguishing dystonia from orthopedic or rheumatologic diseases inducing fixed postures); focal weakness of neck muscles antagonizing the abnormal head/neck posture (item 4, a feature that may prove useful to differentiate lower motor neuron diseases/myopathy from dystonia); diplopia induced by voluntary correction of the abnormal head/neck posture (item 5, a feature that may distinguish CD from ocular torticollis); and ability to voluntarily suppress spasms defined as an inner volitional effort rather than voluntary compensatory frontalis muscle overactivity (item 6, a feature that is potentially useful to distinguish dystonia and tics). Attention was paid to distinguish suppressibility by willpower alone from compensatory movements that often counteract dystonic movements or postures and are also the result of voluntary action. There was no duration requirement for voluntary suppression.
Participants were video recorded according to a standardized protocol in order to assess all the major/distinctive clinical features possibly contributing to CD diagnosis. The video protocol included standard maneuvers triggering involuntary head movements, sensory trick if present, and the strength of neck muscles under voluntary contraction. Patients were asked to demonstrate their trick to the examiner. Tricks were predominantly tactile and included touching the chin, cheek, or neck; in two patients, visual fixation temporarily improved CD. Trick was considered to be effective when it induced complete cessation or at least some decrease in dystonic position. In several patients, sensory trick was effective when applied on the side contralateral to the dystonic movement. In other patients who applied the trick on the same side of the dystonic movement, counterpressure was excluded if the patient employed only a mild force to counteract the dystonic contraction. Subjects were also asked by the examiner about: (i) occurrence of diplopia induced by voluntary correction of the abnormal head/neck posture and (ii) capability to voluntarily suppress involuntary neck movements.
Inter-/intra-rater agreement was assessed among three independent raters who did not belong to the centers participating in the project. The number of videos included in the reliability study (64 video recordings of 43 CD patients, 6 normal controls, and 15 disease controls) exceeded that based on recommended subject-to-item ratios (which usually consider the assessment of 5–10 subjects for each item of a new scale) and on the number of items (n = 4) to be assessed by the three observers. Item 5 (diplopia induced by voluntary correction of the abnormal head/neck posture) and item 6 (inability to voluntarily suppress spasms) were not included in the reliability analysis because questions about these items were asked by the site examiner but not captured in the video. Agreement among raters was assessed by k index, which measures the level of agreement beyond chance and ranges from − 1 (perfect disagreement) to + 1 (perfect agreement). A k index > 0.4 (indicating moderate to substantial/almost perfect agreement) was considered to be satisfactory.
To estimate sensitivity and specificity, the gold standard was the diagnosis made at each site by the senior neurologists (GD and AB). Sensitivity was defined as the proportion of subjects who screened positive from among those who had a diagnosis of CD on clinical examination (true positives/true positives + false negatives). Specificity was the proportion of subjects who screened negative from among those who were determined to not have CD on clinical examination (true negatives/false positives + true negatives).
This study was approved by the ethic committee (identification no. PG/2018/7281). Written informed consent was obtained from all participants. A signed patient consent-to-disclose form was obtained for videos of any recognizable patient.
Results
The validation sample included 43 patients with idiopathic CD (age at onset 53.3 ± 9.5 years) and 41 control subjects. The control group included 12 normal subjects, 6 patients with isolated head tremor, 4 with chorea, 6 with tics, 4 with head ptosis due to myasthenia or amyotrophic lateral sclerosis, 7 with orthopedic/rheumatologic neck diseases, and 2 with ocular torticollis. The case and control groups were similar for sex (29 women and 14 men vs. 27 women and 14 men, p = 0.5) and age (60.8 ± 10.7 vs. 59.5 ± 12.7 years, p = 0.4).
Inter-rater agreement was substantial to almost perfect for all four tested items (item 1: k = 0.82, p < 0.0001; item 2: k = 0.87, p < 0.0001; item 3: k = 1.00, p < 0.0001; item 4: k = 0.86, p < 0.0001).
Considering only item 1 (“stereotyped, patterned, involuntary head/neck movements or postures inducing head/neck deviation from neutral position”), the three observers achieved 98% mean sensitivity and 48% mean specificity (Table 1); analyzing item 2 alone (i.e., sensory trick), mean sensitivity was 75% and mean specificity was 84%; finally, mean sensitivity and mean specificity of the red flags group (namely, items 3–6) were 55 and 71%, respectively (Table 1).
Owing to the unsatisfactory levels of sensitivity and specificity, we tested whether combining the selected items would improve diagnostic sensitivity/specificity (Table 2). First, we combined the item that reached the greatest sensitivity, that is item 1, with item 2, or the red flags group (items 3–6): the combination item 1 + item 2 yielded 74% mean sensitivity and 89% mean specificity (Table 2); the combination item 1 + red flags group of items yielded 54% mean sensitivity and 95% mean specificity. Thereafter, we tested the algorithm including all the items and starting with item 1 that reached the greatest sensitivity. The second step was recognition of sensory trick, the item reaching the greatest specificity. In the absence of a sensory trick, including in the algorithm, the red flags group of items yielded the 84% mean sensitivity and 84% mean specificity (Table 2).
Finally, the prior algorithm was further checked by omitting one of the red flags at a time. As reported in Table 3, the best combination of sensitivity and specificity was observed when item 6 (“capability to voluntarily suppress spasms”) was excluded.
Discussion
Among the clinical items herein tested, items 1–4 (i.e., repetitive, patterned head/neck movements/postures inducing head/neck deviation from neutral position; sensory trick; tonic head/neck deviation from neutral position; and focal weakness of neck muscles antagonizing the abnormal head/neck posture) were evaluated for reliability and were found to have almost perfect inter-rater agreement. Items 5 and 6 (i.e., diplopia induced by voluntary correction of the abnormal head/neck posture; and ability to voluntarily suppress spasms) were not tested for reliability because they were assessed by a patient’s answer to a standardized question.
With regard to accuracy, the item “patterned, repetitive head/neck movements/postures inducing head deviation from neutral position” achieved very high sensitivity (98% on average), thus confirming the suggestion present in the 2013 definition of dystonia that assigns a crucial role to this item in diagnosing and differentiating CD from other neck movement disorders, like chorea and tremor [1]. Nevertheless, the 49% specificity indicated a high risk of misclassifying several cases. Neither sensory trick nor red flags alone provided satisfactory sensitivity and specificity.
Since these accuracy estimates were unsatisfactory, we tested whether combining the selected items improved diagnostic sensitivity/specificity. We observed that combining item 1 (the item that reached the greatest sensitivity) and sensory trick (the item that reached the greatest specificity) increased specificity to 89% but decreased sensitivity to 73%. This was probably because sensory trick is a feature largely specific for dystonia but is not present in about 20% of CD patients [4, 5]. It should be noticed that among control subjects, 4 patients with tic, 3 patients with myasthenia, and 1 patient with ocular torticollis reported that touching the neck was a sensory trick. In tic patients, we could not be sure that this was a true trick or the result of the voluntary spasm suppression characteristic of tics [20]. In the other controls, tactile stimulation/local compression of the muscle may have led to the alleviation of muscle weakness and improvement in neck position.
In the absence of a sensory trick, active exclusion of the red flags (items 3–6) yielded 84% mean sensitivity and 84% mean specificity. Finally, we tested shorter versions of the algorithm by excluding one of the red flags at a time. The best combination of sensitivity and specificity was obtained when the item “ability to mentally suppress spasms” was omitted. This is a feature that is potentially useful in distinguishing dystonia and tics, because tics are voluntarily suppressible while dystonia is not. The lack of utility of this item may be because voluntary suppressibility can be difficult to ascertain, and the result may depend closely on how the question is asked [27]. Some patients with CD may interpret the ability to voluntarily suppress symptoms in different ways. They may believe that “voluntary” includes compensatory movements that counteract dystonic movements or postures or they may believe that suppressibility can be partial. In fact, several CD patients reported voluntary suppressibility, which may reflect these differences of interpretation. Regardless of the explanation, the average 96% sensitivity and 81% specificity obtained with this algorithm (Fig. 1) means that it can correctly diagnose CD in more than 9/10 patients who have the condition and correctly identify 8/10 subjects who do not have the condition (Fig. 1).

Proposed algorithm for the diagnosis of cervical dystonia
Our study has several strengths. First, the validation procedure included patients with CD (whose demographic and clinical characteristics resembled those of patients reported in other published series), healthy controls, and subjects with a variety of neck disorders mimicking CD. Second, the standardized videotape protocol reproduced all major features seen during clinical examination. However, the present study also has some limitations. We did not evaluate whether incorporating the proposed guideline was better than providing only brief training without specific criteria to the raters. Nevertheless, there are several lines of evidence indicating that, in the absence of specific criteria, there is variability in the diagnostic approach of physicians, regardless of their expertise [28, 29]. Our aim was to provide a valid and practical guideline capable of reducing variability among physicians. There may also be variability in the interpretation of patients to answer standardized questions on video examination. Probably a live examination would provide better outcome than video examination. Likewise, specificity will probably be better in real life than in this sample where the number of mimics closely matched the number of cases. Finally, since all patients and evaluating physicians involved in this study were from the same country, the results of this study need to be confirmed in different patient and physician populations.
Despite these limitations, this study demonstrates two relevant points. First, an accurate diagnosis of CD is not possible if we refer only to the core clinical feature of CD as proposed in the 2013 revised classification of dystonia [1], i.e., “patterned and repetitive movements/postures in the head/neck” as well as to the combination of this item and sensory trick. Second, a higher diagnostic accuracy can be achieved if we also consider clinical features related to dystonia mimics that should be absent in dystonia. The diagnostic algorithm without the item “ability to voluntarily suppress spasms” was sensitive and specific enough to be proposed as a guideline for presumptive diagnosis of CD, though it needs to be further expanded and validated in a larger international sample.
Data availability
Data are available upon reasonable request.
References
Albanese A, Bhatia K, Bressman SB et al (2013) Phenomenology and classification of dystonia: A consensus update. Mov Disord 28:863–873. https://doi.org/10.1002/mds.25475
Jinnah HA (2019) The Dystonias. CONTINUUM: Lifelong Learn Neurol 25:976–1000. https://doi.org/10.1212/CON.0000000000000747
Di Biasio F, Marchese R, Abbruzzese G et al (2020) Motor and sensory features of cervical dystonia subtypes: data from the italian dystonia registry. Front Neurol 11:1–7. https://doi.org/10.3389/fneur.2020.00906
Tinazzi M, Erro R, Mascia MM et al (2020) Demographic and clinical determinants of neck pain in idiopathic cervical dystonia. J Neural Transm 127:1435–1439. https://doi.org/10.1007/s00702-020-02245-4
Ramos VFML, Karp BI, Hallett M (2014) Tricks in dystonia: ordering the complexity. J Neurol Neurosurg Psychiatry 85:987–993. https://doi.org/10.1136/jnnp-2013-306971
Berman BD, Groth CL, Sillau SH et al (2019) Risk of spread in adult-onset isolated focal dystonia: a prospective international cohort study. J Neurol, Neurosurg and Psychiatry. https://doi.org/10.1136/jnnp-2019-321794
Abbruzzese G, Berardelli A, Girlanda P et al (2008) Long-term assessment of the risk of spread in primary late-onset focal dystonia. J Neurol Neurosurg Psychiatry 79:392–396. https://doi.org/10.1136/jnnp.2007.124594
Ercoli T, Erro R, Fabbrini G et al (2021) Spread of segmental/multifocal idiopathic adult-onset dystonia to a third body site. Parkinsonism Relat Disord 87:70–74. https://doi.org/10.1016/j.parkreldis.2021.04.022
Defazio G, Ercoli T, Erro R et al (2020) Idiopathic non-task-specific upper limb dystonia, a neglected form of dystonia. Mov Disord 35:2038–2045. https://doi.org/10.1002/mds.28199
Kilic-Berkmen G, Pirio Richardson S, Perlmutter JS et al (2022) Current guidelines for classifying and diagnosing cervical dystonia: empirical evidence and recommendations. Movement Disorders Clinical Practice 9:183–190. https://doi.org/10.1002/mdc3.13376
LaHue SC, Albers K, Goldman S et al (2020) Cervical dystonia incidence and diagnostic delay in a multiethnic population. Mov Disord 35:450–456. https://doi.org/10.1002/mds.27927
Martino D, Aniello MS, Masi G et al (2004) Validity of family history data on primary adult-onset dystonia. Arch Neurol 61:1569–1573. https://doi.org/10.1001/archneur.61.10.1569
Macerollo A, Superbo M, Gigante AF et al (2015) Diagnostic delay in adult-onset dystonia: data from an Italian movement disorder center. J Clin Neurosci 22:608–610. https://doi.org/10.1016/j.jocn.2014.09.014
Bidewell JW, Powell AT, Walker AC (1995) Diagnosing idiopathic dystonia: must it take so long? Aus Health Rev 18:120–131. https://doi.org/10.3316/ielapa.960302911
Jog M, Chouinard S, Hobson D et al (2011) Causes for treatment delays in dystonia and hemifacial spasm: a Canadian survey. Can J Neurol Sci 38:704–711. https://doi.org/10.1017/S0317167100012270
Tiderington E, Goodman EM, Rosen AR et al (2013) How long does it take to diagnose cervical dystonia? J Neurol Sci 335:72–74. https://doi.org/10.1016/j.jns.2013.08.028
Raju S, Ravi A, Prashanth LK (2019) Cervical dystonia mimics: a case series and review of the literature. Tremor Other Hyperkinetic Movements (New York, NY) 9:1–11. https://doi.org/10.7916/tohm.v0.707
Berlot R, Bhatia KP, Kojović M (2019) Pseudodystonia: a new perspective on an old phenomenon. Parkinsonism Relat Disord 62:44–50. https://doi.org/10.1016/j.parkreldis.2019.02.008
Cardoso F, Seppi K, Mair KJ et al (2006) Seminar on choreas. Lancet Neurol 5:589–602. https://doi.org/10.1016/S1474-4422(06)70494-X
Ganos C, Münchau A, Bhatia KP (2014) The Semiology of tics, tourette’s, and their associations. Movement Disord Clin Pract 1:145–153. https://doi.org/10.1002/mdc3.12043
Martinez-Lage JF, Martinez Perez M, Fernandez Cornejo V, Poza M (2001) Atlanto-axial rotatory subluxation in children: early management. Acta Neurochir 143:1223–1228. https://doi.org/10.1007/s007010100018
Antelmi E, Plazzi G, Erro R et al (2016) Intermittent head drops: the differential spectrum. J Neurol Neurosurg Psychiatry 87:414–419. https://doi.org/10.1136/jnnp-2015-310864
Cauchi M, Marsh E (2016) A practical approach to the patient presenting with dropped head. Pract Neurol 16:445–451. https://doi.org/10.1136/practneurol-2016-001450
Mitchell PR (1999) Ocular torticollis. Trans Am Ophthalmol Soc 97:697–769
Defazio G, Albanese A, Pellicciari R et al (2019) Expert recommendations for diagnosing cervical, oromandibular, and limb dystonia. Neurol Sci 40:89–95. https://doi.org/10.1007/s10072-018-3586-9
Romano M, Bagnato S, Altavista MC et al (2022) Diagnostic and therapeutic recommendations in adult dystonia: a joint document by the Italian Society of Neurology, the Italian Academy for the Study of Parkinson’s disease and movement disorders, and the Italian Network on Botulinum Toxin. Neurol Sci. https://doi.org/10.1007/s10072-022-06424-x
Koller WC, Biary NM (1989) Volitional control of involuntary movements. Movement Disord: Off J Movement Disord Soc 4:153–156. https://doi.org/10.1002/mds.870040207
Logroscino G, Livrea P, Anaclerio D et al (2003) Agreement among neurologists on the clinical diagnosis of dystonia at different body sites. J Neurol Neurosurg Psychiatry 74:348–350. https://doi.org/10.1136/jnnp.74.3.348
Defazio G, Jinnah HA, Berardelli A et al (2021) Diagnostic criteria for blepharospasm: a multicenter international study. Parkinsonism Relat Disord 91:109–114. https://doi.org/10.1016/j.parkreldis.2021.09.004
Funding
Open access funding provided by Università degli Studi di Cagliari within the CRUI-CARE Agreement. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest relevant to this work.
Ethical approval
This study was approved by the ethic committee (identification no. PG/2018/7281). All patients were informed about the nature of the study and gave their written consent to participate. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Supplementary Information
Below is the link to the electronic supplementary material.
415_2023_11585_MOESM2_ESM.png
Supplementary file2 Receiver operating characteristic curve displaying sensitivity and specificity and area under the curve for the diagnostic algorithm displayed in Figure 1. The arrow indicates the best combination of sensitivity and specificity discriminating patients with cervical dystonia from controls (PNG 150 KB)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Defazio, G., Belvisi, D., Comella, C. et al. Validation of a guideline to reduce variability in diagnosing cervical dystonia. J Neurol 270, 2606–2612 (2023). https://doi.org/10.1007/s00415-023-11585-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-11585-6