
Abstract
Introduction
In addition to physical and cognitive symptoms, patients with multiple sclerosis (MS) have an increased risk of experiencing mental health problems.
Methods
This narrative review provides an overview of the appearance and epidemiology of affective symptoms in MS such as depression, anxiety, bipolar disorder, euphoria, and pseudobulbar affect. Furthermore, the association between affective symptoms and quality of life and the currently used diagnostic instruments for assessing these symptoms are considered whereby relevant studies published between 2009 and 2021 were included in the review.
Results
Patients with mild and moderate disability more frequently reported severe problems with depression and anxiety than severe mobility problems. Apart from the occurrence of depression, little is known about the association of other affective symptoms such as anxiety, bipolar disorder, euphoria, and pseudobulbar affect and subsyndromal symptoms, which fail to meet the diagnostic criteria but are nevertheless a significant source of distress. Although there are a few recommendations in the research to perform routine screenings for diagnosable affective disorders, a standardized diagnostic procedure to assess subsyndromal symptoms is still lacking. As the applied measurements are diverse and show low accuracy to detect these symptoms, patients who experience affective symptoms are less likely to be identified.
Discussion
In addition to the consideration of definite psychiatric diagnoses, there is an unmet need for a common definition and assessment of disease-related affective symptoms in MS. Future studies should focus on the improvement and standardization of a common diagnostic procedure for subsyndromal affective symptoms in MS to enable integrated and optimal care for patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Apart from physical symptoms, most patients with multiple sclerosis (MS) experience cognitive deficits [1] and affective symptoms which may negatively affect their social and family life, thereby contributing to the burden of the disease [2, 3]. Significantly, patients are found to experience severe affective symptoms at all levels of disease severity and patients with mild and moderate disability (EDSS 0–6.5) reported severe problems with depression and anxiety even more often than severe mobility problems [3].
The lifetime prevalence of affective disorders such as major depression or anxiety disorders in MS can be as high as 50% [4,5,6] and is thus substantially higher than in the general population [7, 8]. Several factors may mediate the occurrence of affective symptoms, including socioeconomic status, age, sex, and the region of residence. Even when these factors are controlled for, there remains a significantly higher annual prevalence risk of affective symptoms in patients with MS when compared to the general population [9]. While the prescription of steroid therapy [10] as well as of some disease modifying treatments is associated with subsequent risks of mood disturbance, such as depressive episodes [11], manic and psychosis [10, 12] the etiology and pathogenesis of these comorbidities are still poorly understood.
There are also indications that affective symptoms become apparent at an early stage of the disease, even before the definite diagnosis of MS [13,14,15], and remain stable for at least 3 years [16]. Support for this assumption comes from a recent retrospective cohort study in which an association between stress-related disorders and an increased risk of subsequent autoimmune diseases was shown [17]. The association between autoimmune disease and affective disorders also indicated an immunological contribution to the development of affective symptoms [18] and hence affective symptoms may comprise the first manifestations of MS [15]. From this, it can be inferred that the presence of neuropsychiatric comorbidities indicates a clear need for intervention as early as possible [14, 19].
Nevertheless, there is evidence suggesting that affective symptoms are still underdiagnosed and undertreated in the clinical standard care of patients with MS [20, 21]. Against this background, in this narrative review, we provide an overview of the incidence and prevalence of affective disorders and symptoms in MS and their impact on quality of life, as well as the current clinical assessment options.
Methods
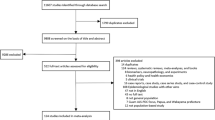
Included in this narrative review were studies with findings on the appearance and epidemiology of affective symptoms and disorders which include depression, anxiety, bipolar disorder, euphoria, and pseudobulbar affect (pathological laughing and crying) in patients with MS. Furthermore, studies focusing on the association between the mentioned affective symptoms or disorders and quality of life were considered, and the findings from the available diagnostic assessment tools are discussed. The literature search was limited to studies that were published between 2009 and 2021, even though a few selective earlier studies were also included if they showed basic insights concerning the covered domains. Case reports were not included. The articles of interest were identified in the ISI Web of Science, ScienceDirect, PubMed, EBSCO Psychology (PsycINFO, PsycARTICLES, PSYNDEXplus), Google Scholar, and Cochrane library.
Results
The 65 analyzed articles for this literature review are displayed in the appendix (Tables 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13), sorted chronologically by year (and alphabetically by author name). The tables contain information about the first author, publication year, investigated symptom or disorder category, total sample size of MS population, age, gender, country of data, included diagnostic assessment tools, main findings, and comments.
Depression
According to cross-national data, major depression represents one of the most common affective disorders with a lifetime prevalence of 20% in the general population [22]. In patients with MS, depression seems to occur more often [23,24,25,26,27] and there is evidence suggesting that patients with MS show a risk of up to 50% of developing major depression in their lifetime [28]. In comparison to the general population, patients with MS have been found to show an elevated point prevalence in depression by 9.3% [8] up to 23.7% [5]. Adjusting for age and sex, the incidence of depression was found to be 71% higher in a group of patients with MS than in a matched healthy control sample [6]. When considering self-reports only, depression rates were even higher. For example, 54% of the patients with MS in the United Kingdom were found to experience depression at some point in their life [29].
In the general population, depressive symptoms are reported to be more frequent in females (12.4%) than in males (6.1%) [8]. However, Théaudin and colleagues [30] did not find any evidence of sex differences concerning depression in MS patients.
Furthermore, compared to patients experiencing depressive symptoms without underlying medical illness, patients with MS showed a comparable clinical presentation of depressive symptomatology. The observed differences between depressive patients and patients with MS were found in specified symptoms: fatigue and irritability were pronounced in patients with MS, while anhedonia and loss of interest were pronounced in patients with a Major Depression [24, 31].
Anxiety
Compared to the lifetime prevalence rates for depression, the reported prevalence rates of an anxiety disorder or anxiety symptoms in MS (general anxiety disorder, social anxiety, agoraphobia, etc.) are more homogeneous, ranging from 20 to 44.5% [32,33,34,35,36]. According to the World Health Organisation (WHO), 8.5% of people in the normal population experience a general anxiety disorder. In contrast, Poder and colleagues (2009) showed that 30.6% of patients with MS were diagnosed with social anxiety disorder, while half of these patients were also diagnosed with general anxiety [37]. Compared to the general population, patients with MS were found to show a higher point prevalence in generalized anxiety disorder by 2.2% [8]. The systematic review by Marrie and colleagues in 2015 also revealed an elevated average point prevalence for anxiety of 21.9% in the MS population [5]. An increased risk of anxiety was found in the pre- and post-diagnostic period of MS, compared to control groups [7, 38]. Female patients with MS and patients with a relapsing–remitting disease course and a worse degree of functional disability showed higher symptoms of anxiety [29, 30].
After adjusting for age and sex, the incidence of an anxiety disorder was still 42% higher in patients with MS than in a matched healthy control sample [6]. In a recent meta-analysis, Boeschoten and colleagues (2017) demonstrated that 22.1% of patients with MS were affected by anxiety [35]. As is the case for depression, when considering self-reports only, anxiety rates were higher as 46.9% of patients with MS in the United Kingdom indicated experiencing anxiety at some point in their life [29].
Interaction of depression and anxiety
With respect to the interaction between depression and anxiety in patients with MS, the results are inconsistent. Some studies indicate that depression and anxiety may be interdependent [33, 39] while more recent findings show that non-somatic symptoms of depression (excessive worry, fear of losing control, inability to relax, etc.) and employment status were risk factors for higher levels of anxiety symptoms in MS [40]. Askari et al. (2014) concluded that depression and the disability level are independent predictors of anxiety [32]. Other studies revealed that the relationship between different aspects of depression and anxiety might change over the course of MS, such that patients may report a stronger link between somatic symptoms of depression with symptoms of anxiety at later disease stages than at earlier stages [40]. Kehler and Hadjistavropoulos (2009) showed that patients with MS and depression had higher levels of health anxiety, the fear or worry about health, compared to an age-matched control group [41]. Nevertheless, although there are no clear correlations between anxious and depressive symptoms in patients with MS the suffering of pressure in the medical history of the affected patients is indisputable.
Bipolar disorder
A further manifestation of affective disorder that should be considered in patients with MS is a bipolar spectrum disorder. Although findings vary from country to country, a large cross-sectional survey across 11 countries found the overall lifetime prevalence of bipolar spectrum disorder to be 2.4% in the general population [42]. There are currently only a few findings concerning the epidemiology, prevalence, and incidence of bipolar disorder in MS patients or correlations between MS and bipolar disorder [12]. Relative to age- and sex-matched controls, Carta and colleagues (2013) reported an odds ratio of 44.4 for experiencing a bipolar disorder together with MS [43]. Marrie et al. (2015) reported a lifetime prevalence of up to 16.2% in patients with MS. An increased lifetime prevalence of bipolar spectrum disorder (bipolar disorders type I and II and cyclothymic disorders) has also been reported for patients with MS when compared to age- and sex-matched controls [5]. After adjusting for age and sex, the incidence of bipolar disorder was 99% higher in MS patients than in the matched healthy population [7].
Euphoria
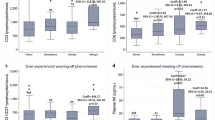
Pathological euphoria as one component of the affective symptoms in MS was first described in the nineteenth century, whereby approximately 10% of the patients were diagnosed to be affected by the pathological expression of euphoria [44]. Given that there was no guidance for a common operationalization of euphoria in patients with MS, different subsequent definitions must be considered. Cottrell and Wilson (1926) provided a classical description of euphoria in which three associated but independent types of euphoria are distinguished [45, 46]: (1) “euphoria sclerotica”: a mental state or mood of cheerfulness and happiness; (2) “eutoniasclerotica”: a feeling of being physically well despite physical deficits; patients in this state are convinced that they can do anything and they are oblivious of their actual physical disability; and (3) “spessclerotica”: a great optimism concerning the future and the prospects of complete recovery from the symptoms [46]. Based on this definition of “euphoria sclerotica,” Paparrigopoulos et al. (2010) described euphoria as a fixed mental state of unusual cheerfulness and optimism about the future despite the presence of a neurological disability. The authors suggested that euphoria should be regarded as a personality change that should be considered distinct from hypomania despite having superficial similarities with it [26]. Duncan et al. (2015) put forward a contemporary definition of euphoria as an “overly optimistic” or “unrealistic optimism” [45]. Using the classical euphoria definition and interviewing method developed by Cottrell and Wilson (1926), Duncan et al. (2016) found high proportions of Cottrell and Wilson’s three types of euphoria (between 63 and 70%, depending on the type of euphoria) in patients with MS. In contrast, using a more contemporary definition and measurement instrument (questions of the Neuropsychiatric Inventory by Cummings (1997) [47]), only 11% of patients with MS were diagnosed as having symptoms of euphoria. The proportions of Cottrell and Wilson’s three types of euphoria in the control group varied between 86 and 94% and thus were significantly higher than the proportions found in the MS group. In contrast, when the Neuropsychiatric Inventory was used, the proportion of persons diagnosed with euphoria in the control group was 4% and thus was lower than the proportion found in the group of patients with MS although the relevant statistical test narrowly missed the conventional criterion of statistical significance [48]. Nevertheless, there are some clear correlations, and patients with symptoms of euphoria were more likely to suffer from a progressive disease form and showed more significant structural pathology [45].
Pseudobulbar affect
A particular type of affective symptom that occurs in patients with MS is pseudobulbar affect. This affective disinhibition syndrome is also known as pathological laughing and crying and is characterized by spontaneous, involuntary, and uncontrollable outbursts of contextually inappropriate laughing or crying that are inconsistent with the patient’s underlying feelings or incongruent with external triggers [49]. Uncontrollable crying seems to be more common than laughing and this mood disturbance has been described in 10% of the MS patients [50]. There are no studies on the prevalence rate of pseudobulbar affect in the general population [49]. A recent study suggests that there may be a relationship between the occurrence of pseudobulbar affect and cognitive impairment in patients with MS. Specifically, deficits in processing speed, visuospatial memory, verbal learning, and fluency in patients with MS have been reported to be associated with pseudobulbar affect [51]. Although more scientific evidence is needed in this area, based on previous indications attention should also be given to pseudobulbar affect in the care of patients with MS.
Association between affective symptoms and quality of life
Affective symptoms such as depression, anxiety, and bipolar disorder are associated with decreased adherence to MS treatment [52], more unfortunate disease progression, cognitive deficits [33], higher suicide risk [53], and reduced quality of life [3, 20, 27]. Depressive symptoms were found to covary with fatigue and reduced cognitive performance, especially concerning information processing speed, attention, working memory, and executive function [54]. Both symptoms of fatigue and reduced cognitive performance may severely affect patients’ quality of life.
Higher levels of health anxiety are associated with greater emotional preoccupation, more use of social support, and reduced use of adaptive coping strategies to manage disabilities in MS [41]. Recent findings show an association between emotional dysregulation and lower health-related quality of life. Maladaptive strategies and difficulties in regulating emotions mediated the associations of depression and anxiety with the quality of life in patients with a progressive course of MS [55].
There seem to be no studies on the possible interactions of euphoria or pseudobulbar affect with important aspects of quality of life such as physical disability or cognitive impairment. The most elaborated studies on quality of life in patients with MS with affective symptoms are available for depression.
Early studies seemed to indicate that greater disease severity and shorter disease duration may be associated with a clinically significant level of depressive symptoms in patients with MS [56]. However, there are also controversial findings concerning the correlation between depression and physical limitations in patients with MS: previous findings provided no evidence of a direct relationship between depression and the Expanded Disability Status Scale [57] as a measure of physical disability in MS [58]. More recent findings showed that patients with MS and comorbid depression had a significantly increased risk of worsening disability [59]. The presence of depression, anxiety, or bipolar disorder was associated with a higher EDSS score in female patients with MS (adjusted for disease duration and progression, age, sex, socioeconomic status, physical comorbidity count, and disease-modifying therapy exposure) [60]. Furthermore, Honarmand et al. (2011) reported a strong association between unemployment and the severity of depression in MS. This work highlighted the need to consider more than physical functioning for the prediction of the employment status as an essential aspect of quality of life [61].
Diagnostic assessment tools
Although there are a few recommendations in the research to perform routine screenings for diagnosable affective disorder in MS, clinicians generally collect information about affect symptoms through unstructured and semi-structured interviews [62,63,64], and a clear diagnostic procedure is still lacking [21, 35].
Specifically, affective symptoms deserve more attention in patients with MS given that they have a substantial impact on disease progression and quality of life [27]. Mood disturbances may reduce the ability to cope with disabilities in MS [39, 41], cognitive performance [33, 54], and adherence to therapy [52]. However, it is important to note that despite the apparent plausibility, causal interpretations of the typically correlational findings in this domain are not warranted.
An overview of the diagnostic methods used for diagnosing affective disorders and symptoms in MS is provided in Table 1. In clinical contexts, a semi-structured interview is applied to identify DSM-IV diagnoses (SCID) including anxiety and depression [65]. However, this method is time-consuming and thus is seldom used in clinical practice for the care of patients with MS. Typically, self-reporting measures are used instead and a systematic review revealed the need to assess the utility of these measures [66]. The following screening measures for depression were frequently reported: the Beck Depression Inventory-II (BDI-II) [67], the Center for Epidemiologic Studies Depression rating scale (CES-D) [68], and the Chicago Multiscale Depression Inventory (CMDI) [69]. Regarding screening measures for anxiety, the following self-reporting measures are partially validated and usually used in MS: the Beck Anxiety Inventory (BAI) [32], and the Anxiety 7-item and Generalized Anxiety Disorder Scale (GAD-7) [70]. Some measures assessing both depression and anxiety that are used include the 9-item Patient Health Questionnaire (PHQ-9) [71], the Hospital Anxiety and Depression Scale (HADS) [68, 72], and the Patient-Reported Outcome Measurement Information System (PROMIS) [66]. A systematic review confirmed the need for early intervention and treatment of anxiety throughout the course of MS [73]. Therefore, research has already addressed the need for improvement in diagnosing depression [74, 75] and anxiety [70, 72, 75] in MS. The Hospital Anxiety and Depression Scale has become a widely used screening instrument in patients with MS and it can be considered a valid instrument for assessing symptoms of both depression and anxiety [76].
A more specialized instrument for manic and hypomanic symptoms is the Mood Disorder Questionnaire, which is a standardized screening questionnaire [77]. It is the most widely studied screening instrument for bipolar disorder [77] and has been applied in patients with MS [78]. Unfortunately, both the sensitivity and specificity of this instrument are low [77].
To detect and measure the severity of a pseudobulbar affect, the self-reporting method known as the Center for Neurologic Study-Liability Scale (CNS-LS) includes two subscales measuring labile laughter and tearfulness [12]. However, the CNS-LS was not developed for use in MS and a disease-related diagnostic procedure for euphoria does not seem to exist.
A considerable number of studies have revealed that the instruments to measure diagnosable affective symptoms which have been validated in patients with MS show similar characteristics and correlate with each other [65, 79] whereby there was no clear superiority of one instrument over the others. The instruments shared high negative predictive values; therefore, clinicians could exclude the presence of a definite diagnosis of depression or generalized anxiety disorder, although the diagnostic accuracy was low. Consequently, individuals with scores that are elevated but still below the cut-off points may experience subsyndromal symptoms, which are not discovered but also warrant clinical attention. Furthermore, a recent study in this context showed that less obvious symptoms such as social and emotional health problems can be more relevant in identifying mood disturbances in patients with MS than anxiety and depression [80]. This underpins the role of subsyndromal affective symptoms and the need for the identification of individuals with symptoms below the cut-off points of definite diagnostic criteria in the context of MS.
Discussion and conclusion
This narrative review shows a large range of prevalence and incidence rates of affective symptoms in MS such as depression, anxiety, bipolar disorder, euphoria, and pseudobulbar affect. Focusing on individual studies could thus easily lead to an underestimation of the rates at which these affective symptoms occur [21].
One reason for the wide range in prevalence and incidence rates of affective symptoms in MS may be the use of widely varying diagnostic methods. However, even the lower ends of the reported prevalence and incidence rates suggest that a substantial proportion of patients with MS experience affective disorders and symptoms. Affective symptoms may even be the first manifestation of the disease [14, 15, 19]. Although pathological mood expressions such as euphoria and pseudobulbar affect were already identified in the first description of MS [44], investigations concerning symptoms that do not meet the criteria for a diagnosable disorder are still rare.
In addition to a few recommendations to screen patients with MS for definite psychiatric disorders [62,63,64, 81], there are no recommendations concerning how to proceed if symptoms fail to meet diagnostic criteria but are nevertheless a significant source of distress [63]. Such subsyndromal affective symptoms are reported spontaneously by individuals or collected in response to the demand of the clinicians (through interviews, questionnaires, checklists, or severity rating scales) but do not meet the diagnostic criteria (e.g., duration, intensity, and impact of functioning) of definite psychiatric diagnoses [63]. Most of the assessments used focused on single symptoms, which have been partially validated for use in MS patients but not specifically developed for this purpose. A first indication of how relevant subsyndromal symptoms are in dealing with emotional states was derived from a recent study which showed that symptoms such as social and emotional health problems in MS that are less obvious than anxiety and depression are important for the mental health of patients with MS [77]. Neglecting these symptoms would be problematic given that they are negatively associated with the quality of life of MS patients [18, 25, 78]. These deficiencies point to the need for an MS-related assessment tool to also detect subsyndromal affective symptoms in the clinical care of patients with MS.
The lack of a common procedure and sensitive assessment tool for less obvious or subsyndromal affective symptoms can partly explain the reason why the occurrence of affective symptoms is still underestimated and as a result, often remain untreated [21, 65]. Future studies are needed to facilitate better insights into the interaction of these symptoms and the underlying pathophysiology [50]. The elaboration of a common definition of relevant MS-related affective symptoms and mood disturbances, including relevant subsyndromal symptoms, should be focused on in future investigations as a deeper understanding of these issues could improve the care of MS patients. Translating these findings into a definition of a standardized diagnostic procedure is necessary for integrated treatment methods, including essentially the aspects of mental health.
References
Arnett PA, Strober LB (2011) Cognitive and neurobehavioral features in multiple sclerosis. Expert Rev Neurother 11:411–424. https://doi.org/10.1586/ern.11.12
Leonavičius R, Adomaitienė V (2012) Impact of depression on multiple sclerosis patients. Open Med 7:685–690. https://doi.org/10.2478/s11536-012-0032-x
Flachenecker P, Kobelt G, Berg J et al (2017) New insights into the burden and costs of multiple sclerosis in Europe: results for Germany. Mult Scler J 23:78–90. https://doi.org/10.1177/1352458517708141
Fromont A, Binquet C, Rollot F et al (2013) Comorbidities at multiple sclerosis diagnosis. J Neurol 260:2629–2637. https://doi.org/10.1007/s00415-013-7041-9
Marrie RA, Reingold S, Cohen J et al (2015) The incidence and prevalence of psychiatric disorders in multiple sclerosis: a systematic review. Mult Scler J 21:305–317. https://doi.org/10.1177/1352458514564487
Marrie RA, Fisk JD, Tremlett H et al (2015) Differences in the burden of psychiatric comorbidity in MS vs the general population. Neurology 85:1972–1979. https://doi.org/10.1212/WNL.0000000000002174
Marrie RA, Fisk JD, Yu BN et al (2013) Mental comorbidity and multiple sclerosis: validating administrative data to support population-based surveillance. BMC Neurol 13:1–8. https://doi.org/10.1186/1471-2377-13-16
Jacobi F, Höfler M, Strehle J et al (2014) Psychische Störungen in der Allgemeinbevölkerung. Studie zur Gesundheit Erwachsener in Deutschland und ihr Zusatzmodul Psychische Gesundheit (DEGS1-MH). Nervenarzt 85:77–87. https://doi.org/10.1007/s00115-013-3961-y
Marrie RA, Walld R, Bolton JM et al (2017) Estimating annual prevalence of depression and anxiety disorder in multiple sclerosis using administrative data. BMC Res Notes 10:1–6. https://doi.org/10.1186/s13104-017-2958-1
Silveira C, Guedes R, Maia D et al (2019) Neuropsychiatric symptoms of multiple sclerosis: state of the art. Psychiatry Investig 16:877–888. https://doi.org/10.30773/pi.2019.0106
Longinetti E, Frisell T, Englund S et al (2022) Risk of depression in multiple sclerosis across disease-modifying therapies. Mult Scler J 28:632–641. https://doi.org/10.1177/13524585211031128
Murphy R, O’Donoghue S, Counihan T et al (2017) Neuropsychiatric syndromes of multiple sclerosis. J Neurol Neurosurg Psychiatry 88:697–708. https://doi.org/10.1136/jnnp-2016-315367
Roy S, Rodgers J, Drake AS et al (2016) Stable neuropsychiatric status in multiple sclerosis: a 3-year study. Mult Scler J 22:569–574. https://doi.org/10.1177/1352458515597570
Disanto G, Zecca C, MacLachlan S et al (2018) Prodromal symptoms of multiple sclerosis in primary care. Ann Neurol 83:1162–1173. https://doi.org/10.1002/ana.25247
Wijnands JMA, Zhu F, Kingwell E et al (2019) Five years before multiple sclerosis onset: phenotyping the prodrome. Mult Scler J 25:1092–1101. https://doi.org/10.1177/1352458518783662
Caceres F, Vanotti S, Benedict RHB et al (2014) Cognitive and neuropsychiatric disorders among multiple sclerosis patients from Latin America: results of the RELACCEM study. Mult Scler Relat Disord 3:335–340. https://doi.org/10.1016/j.msard.2013.10.007
Song H, Fang F, Tomasson G et al (2018) Association of stress-related disorders with subsequent autoimmune disease. J Am Med Assoc 319:2388–2400. https://doi.org/10.1001/jama.2018.7028
Benros ME, Waltoft BL, Nordentoft M et al (2013) Autoimmune diseases and severe infections as risk factors for mood disorders a nationwide study. JAMA Psychiat 70:812–820. https://doi.org/10.1001/jamapsychiatry.2013.1111
Roy S, Drake A, Fuchs T et al (2018) Longitudinal personality change associated with cognitive decline in multiple sclerosis. Mult Scler J. https://doi.org/10.1177/1352458517753720
Marrie RA, Patten SB, Berrigan LI et al (2018) Diagnoses of depression and anxiety versus current symptoms and quality of life in multiple sclerosis. Int J MS Care 20:76–84. https://doi.org/10.7224/1537-2073.2016-110
Marrie RA, Horwitz R, Cutter G et al (2009) The burden of mental comorbidity in multiple sclerosis: frequent, underdiagnosed, and undertreated. Mult Scler 15:385–392. https://doi.org/10.1177/1352458508099477
Kessler RC, Bromet EJ (2013) The epidemiology of depression across cultures. Annu Rev Public Health 34:119–138. https://doi.org/10.1146/annurev-publhealth-031912-114409
Simpson RJ, McLean G, Guthrie B et al (2014) Physical and mental health comorbidity is common in people with multiple sclerosis: nationally representative cross-sectional population database analysis. BMC Neurol 14:1–8. https://doi.org/10.1186/1471-2377-14-128
Brokate B, Reimer J, Hildebrandt H (2017) Charakteristik depressiver Symptome bei psychischen Erkrankungen und Multipler Sklerose – eine retrospektive Datenanalyse. Zeitschrift für Neuropsychol 28:197–205. https://doi.org/10.1024/1016-264X/a000203
Ozdemir PG, Milanlioglu A, Boysan M et al (2015) Relations between mood characteristics, circadian preferences, and functionality in multiple sclerosis. Int J Psychiatry Clin Pract 19:148–154. https://doi.org/10.3109/13651501.2014.980831
Paparrigopoulos T, Ferentinos P, Kouzoupis A et al (2010) The neuropsychiatry of multiple sclerosis: focus on disorders of mood, affect and behaviour. Int Rev Psychiatry 22:14–21. https://doi.org/10.3109/09540261003589323
Feinstein A, Magalhaes S, Richard JF et al (2014) The link between multiple sclerosis and depression. Nat Rev Neurol 10:507–517. https://doi.org/10.1038/nrneurol.2014.139
Patten SB, Marrie RA, Carta MG (2017) Depression in multiple sclerosis. Int Rev Psychiatry 29:463–472
Jones KH, Ford DV, Jones PA et al (2012) A large-scale study of anxiety and depression in people with multiple sclerosis: a survey via the web portal of the UK MS Register. PLoS One 7:e41910. https://doi.org/10.1371/journal.pone.0041910
Théaudin M, Romero K, Feinstein A (2016) In multiple sclerosis anxiety, not depression, is related to gender. Mult Scler J 22:239–244. https://doi.org/10.1177/1352458515588582
Hasselmann H, Bellmann-Strobl J, Ricken R et al (2016) Characterizing the phenotype of multiple sclerosis-associated depression in comparison with idiopathic major depression. Mult Scler 22:1476–1484. https://doi.org/10.1177/1352458515622826
Askari F, Ghajarzadeh M, Mohammadifar M et al (2014) Anxiety in patients with multiple sclerosis: association with disability, depression, disease type and sex. Acta Med Iran 52:889–892
Goretti B, Viterbo RG, Portaccio E et al (2014) Anxiety state affects information processing speed in patients with multiple sclerosis. Neurol Sci 35:559–563. https://doi.org/10.1007/s10072-013-1544-0
Leonavičius R, Adomaitienė V (2013) Anxiety and social activities in multiple sclerosis patients. Cent Eur J Med 8:56–61. https://doi.org/10.2478/s11536-012-0072-2
Boeschoten RE, Braamse AMJ, Beekman ATF et al (2017) Prevalence of depression and anxiety in multiple sclerosis: a systematic review and meta-analysis. J Neurol Sci 372:331–341. https://doi.org/10.1016/j.jns.2016.11.067
Wood B, van der Mei I, Ponsonby A-L et al (2012) Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosis. Muliple Scler J 19:217–224. https://doi.org/10.1177/1352458512450351
Poder K, Ghatavi K, Fisk J et al (2009) Social anxiety in a multiple sclerosis clinic population. Mult Scler 15:393–398. https://doi.org/10.1177/1352458508099143
Hoang H, Laursen B, Stenager EN, Stenager E (2016) Psychiatric co-morbidity in multiple sclerosis: the risk of depression and anxiety before and after MS diagnosis. Mult Scler J 22:347–353. https://doi.org/10.1177/1352458515588973
Brown RF, Valpiani EM, Tennant CC et al (2009) Longitudinal assessment of anxiety, depression, and fatigue in people with multiple sclerosis. Psychol Psychother Theory Res Pract 82:41–56. https://doi.org/10.1348/147608308X345614
Hartoonian N, Terrill AL, Beier ML et al (2015) Predictors of anxiety in multiple sclerosis. Rehabil Psychol 60:91–98. https://doi.org/10.1037/rep0000019
Kehler MD, Hadjistavropoulos HD (2009) Is health anxiety a significant problem for individuals with multiple sclerosis? J Behav Med 32:150–161. https://doi.org/10.1007/s10865-008-9186-z
Merikangas KR, Jin R, He JP et al (2011) Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry 68:241–251
Carta MG, Moro MF, Lorefice L et al (2013) The risk of bipolar disorders in multiple sclerosis. J Affect Disord 155:255–260. https://doi.org/10.1016/j.jad.2013.11.008
Charcot JM (1881) Lectures on the diseases of the nervous system: delivered at la salpêtrière, Vol. 2. New Sydenham Society
Duncan A, Malcolm-Smith S, Ameen O, Solms M (2015) Changing definitions of euphoria in multiple sclerosis: a short report. Mult Scler J 21:776–779. https://doi.org/10.1177/1352458514549400
Cottrell SS, Kinnier Wilson SA (1926) The affective symptomatology of disseminated sclerosis. A study of 100 cases. J Neurol Neurosurg Psychiatry S1–S7:1–30. https://doi.org/10.1136/jnnp.s1-7.25.1
Cummings JL (1997) The Neuropsychiatric Inventory: assessing psychopathology in dementia patients. Neurology 48:10S-16S. https://doi.org/10.1212/WNL.48.5_Suppl_6.10S
Duncan A, Malcolm-Smith S, Ameen O, Solms M (2016) The incidence of euphoria in multiple sclerosis : artefact of measure. Mult Scler Int 2016:5738425. https://doi.org/10.1155/2016/5738425
Iacovides A, Andreoulakis E (2011) Bipolar disorder and resembling special psychopathological manifestations in multiple sclerosis: a review. Curr Opin Psychiatry 24:336–340. https://doi.org/10.1097/YCO.0b013e328347341d
Haussleiter IS, Brüne M, Juckel G (2009) Psychopathology in multiple sclerosis: diagnosis, prevalence and treatment. Ther Adv Neurol Disord 2:13–29. https://doi.org/10.1177/1756285608100325
Hanna J, Feinstein A, Morrow SA (2016) The association of pathological laughing and crying and cognitive impairment in multiple sclerosis. J Neurol Sci 361:200–203. https://doi.org/10.1016/j.jns.2016.01.002
Tarrants M, Oleen-Burkey M, Castelli-Haley J, Lage MJ (2011) The impact of comorbid depression on adherence to therapy for multiple sclerosis. Mult Scler Int 2011:1–10. https://doi.org/10.1155/2011/271321
Erlangsen A, Stenager E, Conwell Y et al (2020) Association between neurological disorders and death by Suicide in Denmark. J Am Med Assoc 323:444–454. https://doi.org/10.1001/jama.2019.21834
Fidao A, De Livera A, Nag N et al (2021) Depression mediates the relationship between fatigue and mental health-related quality of life in multiple sclerosis. Mult Scler Relat Disord 47:102620. https://doi.org/10.1016/j.msard.2020.102620
Prakash RS, Schirda B, Valentine TR et al (2019) Emotion dysregulation in multiple sclerosis: impact on symptoms of depression and anxiety. Mult Scler Relat Disord 36:101399. https://doi.org/10.1016/j.msard.2019.101399
Da Silva AM, Vilhena E, Lopes A et al (2011) Depression and anxiety in a Portuguese MS population: associations with physical disability and severity of disease. J Neurol Sci 306:66–70. https://doi.org/10.1016/j.jns.2011.03.042
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33:1444–1452. https://doi.org/10.1212/wnl.33.11.1444
Mrabet S, Ben Ali N, Kchaou M, Belal S (2014) Depression in multiple sclerosis. Rev Neurol (Paris) 170:700–702. https://doi.org/10.1016/j.neurol.2014.07.017
Binzer S, McKay KA, Brenner P et al (2019) Disability worsening among persons with multiple sclerosis and depression: a Swedish cohort study. Neurology 93:E2216–E2223. https://doi.org/10.1212/WNL.0000000000008617
McKay KA, Tremlett H, Fisk JD et al (2018) Psychiatric comorbidity is associated with disability progression in multiple sclerosis. Neurology 90:e1316–e1323. https://doi.org/10.1212/WNL.0000000000005302
Honarmand K, Akbar N, Kou N, Feinstein A (2011) Predicting employment status in multiple sclerosis patients: the utility of the MS functional composite. J Neurol 258:244–249. https://doi.org/10.1007/s00415-010-5736-8
Thielscher C, Thielscher S, Kostev K (2013) The risk of developing depression when suffering from neurological diseases. GMS Ger Med Sci 11:1–7. https://doi.org/10.3205/000170
Minden SL, Feinstein A, Kalb RC et al (2014) Evidence-based guideline: assessment and management of psychiatric disorders in individuals with MS Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 82:174–181. https://doi.org/10.1212/WNL.0000000000000013
Fragoso YD, Adoni T, Anacleto A et al (2014) Recommendations on diagnosis and treatment of depression in patients with multiple sclerosis. Pract Neurol 14:206–209. https://doi.org/10.1136/practneurol-2013-000735
Marrie RA, Zhang L, Lix LM et al (2018) The validity and reliability of screening measures for depression and anxiety disorders in multiple sclerosis. Mult Scler Relat Disord 20:9–15. https://doi.org/10.1016/j.msard.2017.12.007
Hind D, Kaklamanou D, Beever D et al (2016) The assessment of depression in people with multiple sclerosis: a systematic review of psychometric validation studies. BMC Psychiatry. https://doi.org/10.1186/s12888-016-0931-5
Hautzinger M, Keller F, Kühner C (2009) BDI-II beck depressions-inventar revision, 2nd edn. Pearson Assessment & Information GmbH. PsychCorp., Frankfurt
Patten SB, Burton JM, Fiest KM et al (2015) Validity of four screening scales for major depression in MS. Mult Scler J 21:1064–1071. https://doi.org/10.1177/1352458514559297
Strober LB, Arnett PA (2015) Depression in multiple sclerosis: the utility of common self-report instruments and development of a disease-specific measure. J Clin Exp Neuropsychol 37:722–732. https://doi.org/10.1080/13803395.2015.1063591
Terrill AL, Hartoonian N, Beier M et al (2014) The 7-item generalized anxiety disorder scale as a tool for measuring generalized anxiety in multiple sclerosis. Int J MS Care 17:49–56. https://doi.org/10.7224/1537-2073.2014-008
Patrick S, Connick P (2019) Psychometric properties of the PHQ-9 depression scale in people with multiple sclerosis: a systematic review. PLoS ONE 14:1–12. https://doi.org/10.1371/journal.pone.0197943
Watson TM, Ford E, Worthington E, Lincoln NB (2014) Validation of mood measures for people with multiple sclerosis. Int J MS Care 16:105–109. https://doi.org/10.7224/1537-2073.2013-013
Butler E, Matcham F, Chalder T (2016) A systematic review of anxiety amongst people with multiple sclerosis. Mult Scler Relat Disord 10:145–168. https://doi.org/10.1016/j.msard.2016.10.003
Fischer A, Fischer M, Nicholls RA et al (2015) Diagnostic accuracy for major depression in multiple sclerosis using self-report questionnaires. Brain Behav 5:1–8. https://doi.org/10.1002/brb3.365
Honarmand K, Feinstein A (2009) Validation of the Hospital Anxiety and Depression Scale for use with multiple sclerosis patients. Mult Scler 15:1518–1524. https://doi.org/10.1177/1352458509347150
Litster B, Fiest KM, Patten SB et al (2016) Screening tools for anxiety in people with multiple sclerosis: a systematic review. Int J MS Care 18:273–281. https://doi.org/10.7224/1537-2073.2016-004
Zimmerman M, Galione JN (2011) Screening for bipolar disorder with the mood disorders questionnaire: a review. Harv Rev Psychiatry 19:219–228. https://doi.org/10.3109/10673229.2011.614101
Carta MG, Moro MF, Lorefice L et al (2014) Multiple sclerosis and bipolar disorders: the burden of comorbidity and its consequences on quality of life. J Affect Disord 167:192–197
Sparaco M, Lavorgna L, Bonavita S (2019) Psychiatric disorders in multiple sclerosis. J Neurol 268(1):45–60
Filser M, Baetge SJ, Balloff C et al (2021) Mental symptoms in MS (MeSyMS): development and validation of a new assessment. Mult Scler Relat Disord 49:102744. https://doi.org/10.1016/j.msard.2021.102744
Schiffer RB, Arnett P, Ben-Zacharia A et al (2005) The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 11:328–337. https://doi.org/10.1191/1352458505ms1162oa
Funding
Open access funding provided by University of Bern. This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Melanie Filser has no conflict of interest. Axel Buchner has no conflict of interest. Gereon R. Fink has no conflict of interest. Stefan M. Gold: Honoraria/speaker fees from Mylan, Almirall, and Celgene. Research grants from Biogen and kind support from the GAIA Group. Iris-Katharina Penner: Honoraria/speaker fees from Adamas Pharma, Almirall, Bayer Pharma, Biogen, BMS, Celgene, Desitin, Genzyme, Janssen, Merck, Roche, Novartis, and Teva. Research support from the German MS Society, Celgene, Teva, Roche, and Novartis. All listed potential conflicts of interest are outside the context of this article’s research, authorship, and publication.
Appendix: Tables with included and reviewed research articles
Appendix: Tables with included and reviewed research articles
Tables 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Filser, M., Buchner, A., Fink, G.R. et al. The manifestation of affective symptoms in multiple sclerosis and discussion of the currently available diagnostic assessment tools. J Neurol 270, 171–207 (2023). https://doi.org/10.1007/s00415-022-11359-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-022-11359-6