
Abstract
Objectives
Positive visual phenomena, although reported in lesions of visual cortex, are often overlooked in patients with acute neurological conditions. Yet, their occurrence without structural abnormalities or other underlying neurological disorders represents a unique observation. This report aims to raise awareness of these phenomena, their implications for understanding visual consciousness and to propose a practical, structured algorithm for the clinical assessment of visual hallucinations related to neurological conditions.
Methods
We describe the clinical presentation and imaging findings in two patients with isolated visual hallucinosis secondary to transitory hypoperfusion.
Results
One patient presented with subocclusion of the right posterior cerebral artery and the other with multifocal arterial abnormalities suggestive of reversible cerebral vasoconstriction syndrome (RCVS). Both presented isolated visual hallucinations and hypoperfusion of the right mesial occipito-temporal cortex. Hallucinated images exhibited peculiarities of certain attributes that were recognized only through guided perceptual analysis performed during their occurrence.
Discussion
Dysfunctions in the visual and attentional networks due to the uneven impact of hypoperfusion on the regions of the mesial occipito-temporal cortex likely contributed to the occurrence of visual hallucinations. The initial impaired awareness of certain image attributes obscured an altered, non-realistic rendering of the hallucinated images. Enhancement of awareness through clinical guidance indicates improved attentional deployment, modulation of visual information processing and hallucination–background integration. These features of the hallucinatory phenomena highlight the critical role of semiological analysis during their occurrence and question the validity of post hoc inquiries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Visual sensory deprivation (e.g. Charles Bonnet syndrome) and several brain disorders, including strokes in visual areas, may induce hallucinations [1,2,3,4,5]. Their underlying mechanisms remain unclear due to several factors. Firstly, these phenomena are particularly complex and likely entail various dysfunctions of specific brain regions and their connections (hodotopic dysfunctions) [6,7,8]. Secondly, the transient and dynamic nature of visual hallucinations makes them difficult to explore, many of the available studies being conducted at a distance from symptom occurrence [5, 9]. Finally, the dogma of localization in clinical neurology focuses on perceptual deficits, negative phenomena that are easier to qualify and quantify, and much less on positive phenomena, which are more subjective and more difficult to assess.
We report two cases with visual hallucinosis and hypoperfusion of the right occipito-temporal cortex, without infarction of the visual cortex, and we propose a practical and structured algorithm for the evaluation of visual hallucinations related to neurological conditions. This algorithm allows an organized exploration of the hallucinatory phenomena and the localization of the involved brain networks. It includes the classification of the hallucinations, the context of their appearance, their chronology, the assessment of insight and of the attributes of the hallucinated images (see Table 1). Since it explores dynamic, often transient, perceptual phenomena, guided analysis is particularly useful when performed while hallucinations are actually occurring and much less so when performed at a distance.
Methods
Case 1
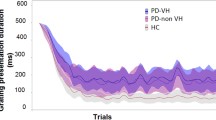
An 85-year-old woman was admitted following transient left hemianopia, manifesting as a “dark veil on the left” that lasted about 10 h. Her medical history included high blood pressure, atrial fibrillation, breast cancer at age 51 and contralateral recurrence at age 78, pulmonary embolism, and bilateral cataract surgery 4 years ago. Her neurological exam was normal. MRI revealed a punctiform area of restricted diffusion in the right ventro-lateral thalamus (motor relay region) and subocclusion of the P2 segment of the right posterior cerebral artery (Fig. 1A, B).

Patient 1 (left): A hyperintensity in the right ventro-lateral thalamus on the diffusion weighted imaging (DWI) sequence corresponding to a punctiform acute ischemic lesion and B significant stenosis of the P2 segment of the right posterior cerebral artery on the time-of-flight (TOF) sequence (white arrow). Patient 2 (right): C, D multiple arterial irregularities (white arrows) on the TOF sequence suggestive of reversible cerebral vasoconstriction syndrome
The following day, while free of other neurological symptoms, she experienced isolated simple and complex visual hallucinations, more often in darkness or dim light. Insight was preserved. A repeat brain MRI revealed hypoperfusion in the right occipito-temporal cortex without new infarction (Fig. 2A, B). EEG during hallucinations, ophthalmological examination and automated perimetry were normal. The hallucinations gradually decreased in frequency ceasing 3 days later. Repeat brain MRI several days later showed resolution of the P2 segment subocclusion.

Patient 1 (left) and Patient 2 (right): A fluid attenuated inversion recovery (FLAIR) and B the corresponding perfusion-weighted imaging (PWI) maps (Olea Sphere®, Olea Medical) showing hypoperfusion in the right mesial occipito-temporal cortex in both patients (black arrows)
Patient's hallucinations were assessed shortly after their first appearance, when they were manifest, and the evolution of the phenomenology was followed daily until its resolution. Simple hallucinations consisted of colored splashes and branching shapes (dendropsias). Her complex hallucinations were clear wall writings, people and plants smaller than real (micropsia), clear and brightly colored. All had neutral emotional impact. Through guided analysis, patient noticed that all hallucinations manifested in her left visual field. The writings were illegible and appeared static. The people and the plants showed depth and lateral shifting without biological movement, resulting in an ellipsoid trajectory, and the transition between the hallucinations and the background was blurred. Noteworthy, lateral component of the translational movement was present during steady fixation and was also influenced by the eye movements (e.g. changes in the perceived trajectory or speed).
Case 2
A 55-year-old woman with history of untreated essential tremor was admitted following a third episode of thunderclap headache. Neurological exam was normal. MRI showed multifocal arterial irregularities suggestive of RCVS (Fig. 1C, D). No precipitating factors were identified and nimodipine was started.
Several hours later, on the evening of the admission day, patient reported isolated simple and complex visual hallucinations with preserved insight. A repeat MRI showed hypoperfusion of the right occipito-temporal cortex without parenchymal lesions (Fig. 2A, B). EEG during hallucinations, ophthalmological exam and automated perimetry were normal. Hallucinations gradually decreased in frequency, ceasing after 2 days. Repeat MRI at one-month follow-up showed resolution of the segmental arterial constrictions, confirming the RCVS, and absent parenchymal lesions.
Patient's hallucinations were assessed soon after their first appearance, when they were manifest, and their progress was monitored daily until they resolved. Simple visual hallucinations included a bright equilateral triangle sliding from the left towards the center of the visual field, replaced several hours later by complex hallucinations of people, animals and plants. Her complex hallucinations were normal-sized, clear, vividly colored, well integrated into background, “moving” and emotionally neutral, except for one reported as a “scary head with holes in its face, large red cheeks and small black eyes”. Through guided visual analysis, patient noted that all hallucinations manifested in the left visual field and that hallucinations of people, animals and plants had in-depth and lateral shifting without biological movement resulting in an ellipsoid trajectory, and a blurred transition with the background. As with the first patient, the lateral component of translational motion was present during steady fixation and was further impacted by eye movements (e.g. changes in the perceived trajectory or speed).
Discussion
The occurrence of visual hallucinations during cerebral hypoperfusion in the ventral visual stream without infarction or underlying neurodegenerative disorder suggests dysfunctions in the visual networks [10, 11]. This is an interesting, and to our knowledge, a previously unreported phenomenon.
While in the first patient, simple and complex hallucinations were intermingled in the course of the hallucinatory phenomena, in the second patient there was a progression from simple to complex hallucinations. Insight was preserved and the hallucinations were spontaneously perceived as real and natural. To emphasize the veracity of the perceived images, patients focused on aspects like the high resolution of certain parts of the image (e.g., animal fur, leafs veins) while disregarding others (e.g., motion patterns, legibility of writing) and the guided analysis performed during the phenomenology pointed out peculiarities of certain attributes (see Table 1).
In our patients, hypoperfusion could have induced an aura-like, cortical spreading depression phenomenon similar to the one described in the penumbra region of ischemic stroke [12,13,14]. Moreover, hypoperfusion likely had an unequal impact on different components of the mesial occipito-temporal cortex inducing variable degrees of dysfunction in the visual hubs. Indeed, the V1 region is more sensitive to hypoxia due to higher cellular density and increased metabolic demand [15]. Therefore, abnormalities of the primary visual cortex may alter the output to higher-order visual areas allowing their spontaneous activation and elaboration of hallucinatory percepts [16]. Hallucinations content reflects the functional specializations of the involved brain regions [16,17,18], and since the regions encoding faces and objects have a right-hemisphere lateralization, this might explain why both reported patients showed hypoperfusion of the right occipitotemporal cortex. It is possible that the text hallucinations in Case 1 originated in areas of the right occipitotemporal cortex involved in the processing of font and handwriting [19, 20], and that guided analysis revealed their lack of semantic content through recruitment of the visual word form area and language-related areas of the left hemisphere [21].
The change in the perception of the hallucinations following the guided analysis could be due to several reasons. One possibility is that the hallucinations are intrinsically defective and that the analysis helped the patients become aware of the image flaws. Another possibility is that the hallucinations are inherently real when the patient focuses on them but their perception is altered by the guided redeployment of attention towards a global picture integrating the hallucinations into the environment. Indeed, this last hypothesis is endorsed by the fact that most of the flaws detected in the hallucinated images concerned attributes that interact or are impacted by the visual context, such as the type of movement, the relative size and the interface with the background. In physiological conditions, the detection of image boundaries is paramount in figure–background segregation [22], the segregated images being routed to the lateral occipital cortex and the background to more dorsal occipital areas [23]. Conversely, the detection of boundaries in the already segregated, hallucinated images might prompt their integration into the background and help identify flawed attributes. As altered communication between the canonical attentional control networks seems to be involved in the hallucinatory phenomena regardless of their origin [24, 25], guided analysis may therefore optimize the attentional deployment and, therefore, modulate the visual information processing and hallucination–background integration.
Conclusion
Hallucinated images, although spontaneously reported as “completely natural”, presented structural and kinetic anomalies revealing an altered, non-realistic rendering. Noteworthy, the impaired awareness of peculiarities in the attributes of the hallucinated images questions the accuracy of post hoc inquiries and points to the crucial role of detailed, structured semiological analysis in the acute phase, while visual hallucinations are actually occurring. This should be considered by future studies exploring positive perceptual phenomena.
References
Merabet LB, Maguire D, Warde A et al (2004) Visual hallucinations during prolonged blindfolding in sighted subjects. J Neuro-Ophthalmol 24:109–113. https://doi.org/10.1097/00041327-200406000-00003
Oishi N, Udaka F, Kameyama M et al (2005) Regional cerebral blood flow in Parkinson disease with nonpsychotic visual hallucinations. Neurology 65:1708–1715. https://doi.org/10.1212/01.wnl.0000187116.13370.e0
Ffytche DH (2007) Visual hallucinatory syndromes: past, present, and future. Dialog Clin Neurosci 9:173–189. https://doi.org/10.31887/DCNS.2007.9.2/dffytche
Taylor JP, Firbank MJ, He J et al (2012) Visual cortex in dementia with Lewy bodies: Magnetic resonance imaging study. Br J Psychiatry 200:491–498. https://doi.org/10.1192/bjp.bp.111.099432
Martinelli F, Perez C, Caetta F et al (2020) Neuroanatomic correlates of visual hallucinations in poststroke hemianopic patients. Neurology 94:e1885–e1891. https://doi.org/10.1212/WNL.0000000000009366
Ffytche DH, Catani M (2005) Beyond localization: from hodology to function. Philos Trans R Soc B Biol Sci 360:767–779. https://doi.org/10.1098/rstb.2005.1621
Catani M, Ffytche DH (2005) The rises and falls of disconnection syndromes. Brain 128:2224–2239. https://doi.org/10.1093/brain/awh622
Ffytche DH (2008) The hodology of hallucinations. Cortex 44:1067–1083. https://doi.org/10.1016/j.cortex.2008.04.005
Ffytche DH, Blom JD, Catani M (2010) Disorders of visual perception. J Neurol Neurosurg Psychiatry 81:1280–1287. https://doi.org/10.1136/jnnp.2008.171348
Carrera E, Tononi G (2014) Diaschisis: past, present, future. Brain 137:2408–2422. https://doi.org/10.1093/brain/awu101
Mashour GA, Roelfsema P, Changeux JP, Dehaene S (2020) Conscious processing and the global neuronal workspace hypothesis. Neuron 105:776–798. https://doi.org/10.1016/j.neuron.2020.01.026
Dohmen C, Sakowitz OW, Fabricius M et al (2008) Spreading depolarizations occur in human ischemic stroke with high incidence. Ann Neurol 63:720–728. https://doi.org/10.1002/ana.21390
Liu L, Kearns KN, Eli I et al (2021) Microglial calcium waves during the hyperacute phase of ischemic stroke. Stroke. https://doi.org/10.1161/STROKEAHA.120.032766
Zhao HT, Tuohy MC, Chow D et al (2021) Neurovascular dynamics of repeated cortical spreading depolarizations after acute brain injury. Cell Rep 37:109794. https://doi.org/10.1016/j.celrep.2021.109794
Huang BY, Castillo M (2008) Hypoxic-Ischemic brain injury: imaging findings from birth to adulthood. Radiographics 28:417–439. https://doi.org/10.1148/rg.282075066
Ffytche DH, Howard RJ, Brammer MJ et al (1998) The anatomy of conscious vision: an fMRI study of visual hallucinations. Nat Neurosci 1:738–742. https://doi.org/10.1038/3738
Mégevand P, Groppe DM, Goldfinger MS et al (2014) Seeing scenes: topographic visual hallucinations evoked by direct electrical stimulation of the parahippocampal place area. J Neurosci 34:5399–5405. https://doi.org/10.1523/JNEUROSCI.5202-13.2014
Lanfranco RC, Rivera-Rei Á, Huepe D et al (2021) Beyond imagination: Hypnotic visual hallucination induces greater lateralised brain activity than visual mental imagery. Neuroimage 239:118282. https://doi.org/10.1016/j.neuroimage.2021.118282
Qiao E, Vinckier F, Szwed M et al (2010) Unconsciously deciphering handwriting: subliminal invariance for handwritten words in the visual word form area. Neuroimage 49:1786–1799. https://doi.org/10.1016/j.neuroimage.2009.09.034
Hills CS, Pancaroglu R, Duchaine B, Barton JJS (2015) Word and text processing in acquired prosopagnosia. Ann Neurol 78:258–271. https://doi.org/10.1002/ana.24437
Bouhali F, de Schotten MT, Pinel P et al (2014) Anatomical connections of the visual word form area. J Neurosci 34:15402–15414. https://doi.org/10.1523/JNEUROSCI.4918-13.2014
Poort J, Raudies F, Wannig A et al (2012) The role of attention in figure-ground segregation in areas V1 and V4 of the visual cortex. Neuron 75:143–156. https://doi.org/10.1016/j.neuron.2012.04.032
Appelbaum LG, Wade AR, Vildavski VY et al (2006) Cue-invariant networks for figure and background processing in human visual cortex. J Neurosci 26:11695–11708. https://doi.org/10.1523/JNEUROSCI.2741-06.2006
Shine JM, O’Callaghan C, Halliday GM, Lewis SJG (2014) Tricks of the mind: Visual hallucinations as disorders of attention. Prog Neurobiol 116:58–65. https://doi.org/10.1016/j.pneurobio.2014.01.004
D’Antonio F, Boccia M, Di Vita A et al (2022) Visual hallucinations in Lewy body disease: pathophysiological insights from phenomenology. J Neurol 269:3636–3652. https://doi.org/10.1007/s00415-022-10983-6
Safran AB, Sanda N (2015) Color synesthesia. Insight into perception, emotion, and consciousness. Curr Opin Neurol 28:36–44. https://doi.org/10.1097/WCO.0000000000000169
Blanke O, Landis T, Spinelli L, Seeck M (2004) Out-of-body experience and autoscopy of neurological origin. Brain 127:243–258. https://doi.org/10.1093/brain/awh040
Montagnese M, Vignando M, Collerton D et al (2022) Cognition, hallucination severity and hallucination-specific insight in neurodegenerative disorders and eye disease. Cogn Neuropsychiatry 27:105–121. https://doi.org/10.1080/13546805.2021.1960812
Jonas J, Descoins M, Koessler L et al (2012) Focal electrical intracerebral stimulation of a face-sensitive area causes transient prosopagnosia. Neuroscience 222:281–288. https://doi.org/10.1016/j.neuroscience.2012.07.021
Parvizi J, Jacques C, Foster BL et al (2012) Electrical stimulation of Human Fusiform face-selective regions distorts face perception. J Neurosci 32:14915–14920. https://doi.org/10.1523/JNEUROSCI.2609-12.2012
Funding
Open access funding provided by University of Geneva.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical standard statement
The ethical principles were in line with the Helsinki Declaration. The data of all described patients are anonymized and all of the involved persons have consented to their data being published in anonymized form.
Consent to participate
The data of all described patients are anonymized, and all of the involved subjects have consented to their data being published in anonymized form.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sanda, N., Escribano Paredes, J.B. & Ferastraoaru, V. Visual hallucinosis during hypoperfusion of the right occipito-temporal cortex. J Neurol 269, 6627–6633 (2022). https://doi.org/10.1007/s00415-022-11346-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-022-11346-x