
Abstract
Amyotrophic lateral sclerosis (ALS) is the most common subtype of motor neuron disease (MND). The current gold-standard measure of progression is the ALS Functional Rating Scale—Revised (ALS-FRS(R)), a clinician-administered questionnaire providing a composite score on physical functioning. Technology offers a potential alternative for assessing motor progression in both a clinical and research capacity that is more sensitive to detecting smaller changes in function. We reviewed studies evaluating the utility and suitability of these devices to evaluate motor function and disease progression in people with MND (pwMND). We systematically searched Google Scholar, PubMed and EMBASE applying no language or date restrictions. We extracted information on devices used and additional assessments undertaken. Twenty studies, involving 1275 (median 28 and ranging 6–584) pwMND, were included. Sensor type included accelerometers (n = 9), activity monitors (n = 4), smartphone apps (n = 4), gait (n = 3), kinetic sensors (n = 3), electrical impedance myography (n = 1) and dynamometers (n = 2). Seventeen (85%) of studies used the ALS-FRS(R) to evaluate concurrent validity. Participant feedback on device utility was generally positive, where evaluated in 25% of studies. All studies showed initial feasibility, warranting larger longitudinal studies to compare device sensitivity and validity beyond ALS-FRS(R). Risk of bias in the included studies was high, with a large amount of information to determine study quality unclear. Measurement of motor pathology and progression using technology is an emerging, and promising, area of MND research. Further well-powered longitudinal validation studies are needed.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Amyotrophic lateral sclerosis (ALS) is the most common subtype of motor neuron disease (MND), a neurodegenerative condition characterised by progressive loss of motor function. Only 51.3% of people with MND (pwMND) survive more than 12 months from diagnosis [1]. The only globally licensed disease-modifying treatment for MND, riluzole, has limited efficacy and extends survival by just 2–3 months [2]. There is an urgent clinical need for more effective therapies and many clinical trials are in progress or planned [3]. Accurate measurement of symptom progression in MND is a significant challenge in both clinical and research settings.
The current gold standard for evaluating physical symptom severity and disease progression is the Amyotrophic Lateral Sclerosis Functional Rating Scale—Revised (ALS-FRS(R)), a questionnaire-based assessment, evaluating the presence and resulting disability, of physical symptoms commonly affecting people with MND. However, the ALS-FRS(R) is reliant on clinical judgement, subjective reporting and pwMND’s recollection of symptoms [4]. A sensitive measure of disease trajectory is an essential requirement of clinical trial outcome measures. Instruments such as the ALS-FRS(R) generate composite scores that may not be sensitive to smaller changes in function, necessitating large trial sample sizes, more frequent assessments points and longer duration follow-up, increasing participant burden [5].
Remote monitoring of function may also improve clinical care delivery [6]. Collecting information between appointments may facilitate delivery of more personalised care [6, 7]. The prognostic capacity of devices is an area of active investigation in a range of neurological conditions [8]. Improved ability to predict disease trajectory and early identification of impairment may also help with care planning.
MND is characterised by clinical heterogeneity in site of onset and disease progression [9]. The different types of devices available offer the opportunity to evaluate different body regions, whilst enabling each person to act as their own baseline for detecting change and progression [10].
The potential of greater sensitivity for detecting change with these devices and their implementation as alternative outcome measures may lead to significant reduction in sample size requirements for trials by 30.3% and 44.6% for 18-months trials [10]. Smaller sample size requirements for detecting effects of new medicines reduces trial delivery costs and shortens timelines for trials [10].
Using devices for remote data collection also reduces the need for frequent trial appointments for participants. Decentralised trial delivery offers the opportunity for more frequent assessments, potentially further reducing sample size requirements, for example weekly versus monthly ALS-FRS(R) completion [11, 12]. The opportunity for remote data collection also offers trialists the opportunity to reduce the burden of trial participation on people with MND and optimise retention [13].
Activity monitors evaluate changes in participants’ overall capability for engaging in physical activity [11], whilst wearable devices containing an inertial measurement unit (IMU) enable researchers to provide a picture of an individual’s ability to move their limbs [10]. An IMU is contained within a wearable device and used to measure velocity, orientation and gravitational force, which in turn can provide detailed information on the participant’s movements. Within the IMU are an accelerometer, gyroscope and magnetometer sensor. Accelerometers measure acceleration from inertia (movement from a resting baseline), gyroscope measure angular rotation (direction of movement) with the magnetometer improving the accuracy of the gyroscope’s determination of direction [14].
Smartphones are also used to collate passive (automatically collected by the phone itself) and active (entered by participants into specialised apps or web forms) data on function, symptoms and daily activity [13]. Electrical impedance myography devices apply a low-intensity electrical current to a limb, to evaluate an area of muscle and through repeated measurements, we can evaluate changes in the structure and composition of the muscle as it degrades due to disease progression, offering a potential alternative biomarker for people with MND [15]. Dynamometry is also focussed on the muscles, evaluating decline through measuring strength of pressure muscles are capable of, this can be focussed on a specific area of the body (eg hand function and grip strength) or more global decline [16].
In other progressive motor disorders, such as Parkinson’s disease, devices have offered an alternative method of continuous and objective monitoring of motor symptoms in both clinical care and trial delivery [17]. The clinical utility of these devices and their potential suitability as trial outcome measures, in people with MND has steadily gained attention in research. In this study, we will explore the current landscape of research in this area: the devices used, aspects of MND evaluated and directions for future work.
Aim
The aims of this study are to improve understanding of the types of device currently used in research to evaluate motor symptoms in pwMND, and to explore if studies consider the acceptability of devices to participants, and the feasibility their use for routine data collection in MND.
Objectives
The objective of this study is to systematically review previous studies reporting use of devices in people with MND and their suitability to evaluate motor progression in research and clinical care for pwMND.
Hypothesis
We hypothesise that the majority of studies in this area will be exploratory: utilising small sample sizes and shorter lengths of follow-up but encouraging for future exploration in research. In addition, we hypothesise that studies primarily focus on comparing devices to performance on the ALS-FRS(R) questionnaire. We hypothesise that pwMND will find these devices to be acceptable to use.
Methods
Search strategy
We completed a systematic and unbiased literature search on the 13th June 2022, adhering to PRISMA guidelines for conducting and reporting systematic reviews, attached in Appendix 1_PRISMA Guidelines. We searched EMBASE with the terms “amyotrophic lateral sclerosis” OR “motor neuron(e) disease” AND “devices” with the headings expanded to include all relevant sub-headings for devices. We also searched PubMed using (amyotrophic lateral sclerosis [MeSH Terms]) OR (motor neuron disease [MeSH Terms]) AND (devices [MeSH Terms]). In addition, we searched Google Scholar with the search terms “amyotrophic lateral sclerosis” OR “motor neurone disease” AND “wearable devices”, as “devices” alone provided an unmanageable number of results on this database.
Outside of the United Kingdom MND is primarily referred to by its most common subtype, amyotrophic lateral sclerosis (ALS), as a result both terms were included. No language or date restrictions were applied. Reference lists of returned search results were also screened for additional suitable articles.
Screening for eligibility
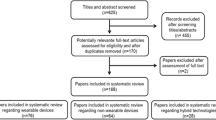
Results were screened for suitability by two independent reviewers, with any disputes resolved by a third reviewer. Full details of inclusion and exclusion criteria used are provided in Table 1 and the number of results included at each stage in the screening process is outlined in Fig. 1.

From Moher et al. [18]. For more information, visit www.prisma-statement.org
Data extraction
Two reviewers extracted information from each search result on the devices used and study participant characteristics. We also noted any additional assessments used to evaluate the devices’ suitability and evaluation of participant feedback on the suitability of these devices.
Risk of bias
Two authors (EB, TF) independently assessed the methodological quality of all included studies using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool for quality assessment questionnaire [19]. Studies were judged to either have high or low risk of bias for each domain based on composite assessment of 13 questions. All studies fitting inclusion criteria were included in the review despite their risk for bias.
Results
An overview of the studies including the specific devices and comparative assessment tools used for concurrent validity is summarised in Table 2 with the full dataset available in Appendix 2_Project Data.
1827 search results were identified of which 20 were studies eligible for inclusion (see PRISMA diagram in Fig. 1 for more details).
These 20 studies included 2044 participants (a mean of 102, range 6–584), 1275 (62%) of whom had MND. The remaining individuals were included as healthy controls or as people with other neurological conditions to offer comparison groups. 17 studies (85%) recorded participants’ ALS-FRS(R) scores [20], to evaluate concurrent validity of the devices [12, 13, 16, 21,22,23,24,25,26,27,28,29,30,31,32,33].
Length of follow-up and number of assessment points varied greatly across the studies, from a single time-point of assessment [25] to study duration of 36 months [28]. The median length of follow-up was 6 months, with a mean of 8 months. The number of assessment points, and different tools used, are summarised in Table 2. Devices were used as a part of larger study protocols, such as the Ontario Neurodegenerative Research Initiative (ONDRI), to differentiate presentation and progression across different neurological conditions [28, 34, 35].
Two studies reported on the feasibility of a fully remote research delivery model [12, 30]. Recruitment and informed consent were successfully completed using the internet and electronic transfer of medical records to confirm eligibility. Remote data collection was a more complex issue. Some participants struggled to set up study platforms independently, with up to 28% of participants with MND unable to record a first measurement [30] and only 15% of participants retained to the 9-months time-point (Table 2).
Five of the studies explored a form of participant experience on the suitability of the devices to people with MND. Participants completed questionnaires, reported adverse effects and rated the burden of using devices. In one study, semi-structured interviews were undertaken to provide participants with the opportunity to discuss their experiences [36]. Concerns ranged from the fairly innocuous, limited clothing options and worry of losing regarding the ActiGraph [10], to more serious adverse effects of skin and subcutaneous tissue disorders in 6 of 25 participants, resulting in 2 participants withdrawing from the study [26].
Devices used
Accelerometers were used in nine studies [10, 25,26,27,28, 33, 36,37,38] including those using an accelerometer and additional sensors (gyroscope and magnetometer) in an inertial measurement unit. These sensors were used to evaluate spatio-temporal parameters of gait specifically in three studies [25, 28, 37]. Five studies evaluated lower limb function using accelerometers worn on the waist or ankle during walking tasks [25, 28, 33, 36, 37]; two of which also involved wearing one the wrist to assess upper limb functioning [33, 36]. In addition, two studies used small accelerometers on participants’ fingers to evaluate fine motor skills through measuring typing speed, strength and accuracy [27, 38].
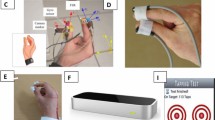
The Microsoft Kinect sensor uses a single camera system to evaluate depth and an individual’s motion, that can be used to capture reachable workspace [39], a clinically relevant measure of upper limb function, providing information on capacity to move the arms and reach within their environment. The Microsoft Kinect sensors were used to evaluate upper limb function, through mapping reachable workspace, in three studies [23, 29, 32]. One study explored the suitability of non-immersive virtual reality tasks as a method of assessing upper limb functionality and cognition, comparing touchscreen laptops, Microsoft Kinect motion sensor and finger motion sensor system Leap Motion Control® [32].
Smartphone applications, such as the Beiwe [13, 22] and ALS AT HOME apps were used [12], offering frequent remote data collection, often using a wide range of endpoints. Smartphone data were categorised as active (directly inputted by participants) and passive (using existing smartphone data such as GPS and call logs), used to calculate activity [13, 22]. Participant-completed ALS-FRS was supplemented with additional questionnaires, motor tests, digital spirometry and cognitive testing.
Six studies evaluated ‘activity monitors’ that collect, and present, data on measurements such as time spent active, sleeping and metabolic equivalent task (MET). MET is a calculation based on body weight to estimate the number of calories burned during an activity or ‘task’ [40]. Monitoring of general activity using wearable devices in studies also enabled researchers to collect data outside of the artificial clinic environment of changes in the participants’ daily functioning, with minimal burden on participants. The Mi Band [12], ActiGraph [10] and Mega Faros sensor [26] were used to evaluate real-world activity levels and heart rate variability during rest and exercise. Activity monitors were combined with additional devices to evaluate respiratory function, such as the AirSmart spirometer [30], and upper limb function, using the Camry digital handgrip dynamometer [12].
Some studies focussed on devices that specifically aimed to evaluate progression in muscle strength. Electrical impedance myography, which works through the application of low-intensity electrical currents to the muscles, was shown to be potentially suitable to evaluate MND progression [31]. Two studies explored the use of fixed and portable dynamometry devices to assess global and precise muscle strength [16, 21], with hand-held dynamometry devices a common comparison measure to establish the suitability of new exploratory devices [12, 31].
Data analysis
Accelerometer devices collect raw data in three axes from the primary accelerometer sensor. The raw data are analysed using either data visualisation tools and pre-existing algorithms provided by the vendors or devising new data analysis models [26]. Working with the raw data to generate novel scoring thresholds enables investigators to replicate findings in the future studies, compare participants and provide preliminary validity data on the prognostic probability of the devices used.
The data from activity monitors and accelerometers are used to correlate the level of change expected based on standardised tests of disease progression and functionality; in MND studies, this is primarily the ALS-FRS(R). Other studies use raw data from the devices to quantify the individual’s movements when performing a standardised clinical measurement or motor function assessments such as the 6-minute walking test [28], arm raising [29] or typing [27]. Assessments that may be clinically relevant to people with MND may not yet have reliability data on which devices are suitable to evaluate motor functionality during them, a key foundation in considering the suitability of a device to this population.
Risk of bias in included studies
Risk of bias in the included studies is shown in Appendix 3_QUADRAS Data. No study fulfilled all QUADAS-2 criteria for low risk of bias. 31% (126/408) responses were deemed “Unclear” as the information regarding sample decisions, reference and index tests used were not available in the study report meaning the conclusions regarding risk of bias were affected by lack of data availability. However, for all the studies, there was low concern that the index test used, the interpretation of the index test or the participants included, differed from the review question.
Discussion
Digital devices have provided an alternative to traditional questionnaire-based assessment methods to detect progression in clinical trials [41] and research studies [42] in a range of neurological disorders. These devices offer a potential new direction in MND research and clinical care and this review explores the current landscape in this area; the device types used and the suitability and acceptability for pwMND.
Establishing suitability of devices
Studies in this review reported that device outcome measures correlated with the ALS-FRS(R), suggesting that devices have concurrent validity with traditional measures of disease progression [12, 13, 16, 21,22,23,24,25,26,27,28,29,30,31,32,33].
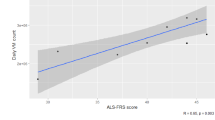
Accelerometer endpoints (average daytime active, percentage of daytime active, total daytime activity score and total 24-h activity score) showed moderate to strong correlations with ALS-FRS(R) scores over a period of 48 weeks [26]. Strong associations between accelerometer endpoints and ALS-FRS(R) scores for up to 21 months and accelerometer data indicated less variability over time [10].
Worsening total ALS-FRS(R) scores, and declining ALS-FRS(R) upper limb sub-scores, were associated with reduced reachable workspace evaluated through Kinect sensors [29]. De Bie et al. [23] also demonstrated the potential utility of device outcome measures, as in their study Kinect sensors were able to detect change in upper limb function when the ALS-FRS(R) did not indicate any significant change over a 1-year period. Scores from activity monitors, specifically the amount of time spent active, correlated with global and motor-specific scores on the ALS-FRS(R), suggesting the potential utility of these devices to evaluate function with low burden to participants [25].
Devices also offered the opportunity to take ALS-FRS(R) data collection out of the clinic, with self-reported ALS-FRS(R) scores correlating highly with clinic-based assessments [13], working towards establishing app-based evaluation and fully remote studies [30] as a potentially suitable alternative to burdensome clinic appointments for people with MND involved in research.
However, the sensitivity of the ALS-FRS(R) to detect smaller changes in functioning is limited [5]. When establishing the suitability of devices for people with MND, concordant validity with existing measures is a helpful starting point, but should not be the only consideration for a devices’ utility in research and clinical evaluation. Responsiveness to change in other physical markers of progression, such as respiratory function and muscle strength, may also be relevant.
Responsiveness to change over time
Only three studies explored the devices at a single time-point [25, 29, 37]. The remaining studies (n = 17) explored change in motor symptoms over time, between 2-week and 36-month study duration.
As when evaluating any progressive disorder, establishing the suitability of these devices to detect change was crucial. Devices were often compared to established measures of disease progression, to establish the ability to detect expected decline and ultimately detect potential treatment effects as biomarkers in clinical trials [31].
The broad range of aspects of functioning which can be evaluated using devices is particularly useful in a condition such as MND with heterogeneous presentation and progression. Devices offer objective measures of both global and precise decline and have been shown by studies in this review to successfully differentiate disease progression [10] and discriminate between neurological conditions [37].
Increasing the length of follow-up, and the number of measurements, to evaluate the reliability of a device across repeated measurements will be a key avenue for future work.
Establishing acceptability of devices
Current data on the acceptability of devices to people with MND were limited, with only five (36%) studies reporting data on participant experience [10, 12, 24, 30, 36]. For the studies that did report on participant experience, feedback was generally positive with participants reporting low burden, an improved sense of control over their condition and minimal impact on their day-to-day activities [10, 12].
The logistical challenge of remote data collection, potential risk to participant safety, and shift in onus on the participant to collect the data, must be carefully managed by clinical and trial teams. Feedback from participants, rates of adverse events and attrition must be closely explored when evaluating the suitability of a potential device for use in this population.
Remote data collection
A key benefit of wearable devices and other health technologies to evaluate disease progression in MND is their portability and suitability for remote data collection. A recruitment, consent and data collection process that was either fully or partially remote would significantly reduce the burden placed on individuals who wish to participate in clinical trials. It would also minimise burden of repeated travel in this vulnerable group, thereby minimising attrition.
Remote data collection using devices presents unique challenges associated with managing and reducing missing data. Studies involving remote data collection reported missing data due to insufficient device charge and participant adherence to protocol of wearing devices. Inability to use the devices and begin data collection may also be problematic, with one study reporting 13% of healthy controls and 28% of pwMND were unable to obtain a first measurement using the technology provided. Only 15% of participants were retained to the 9-month time-point. With only 15% of participants remaining at the 9-month time-point, our ability to draw conclusions from remotely collected data in these studies is limited [12].
Participant-led data collection
The shift to participant-led data collection may be contingent on individuals having a degree of technical knowledge and confidence in their ability to use devices, potentially affecting those who opt to engage [11, 12]. This may bias samples in studies using health technology, for example towards younger individuals, with greater digital literacy and those less affected by upper limb weakness. Clinicians and researchers may pre-emptively address this concern by reducing skills required for people to participate, providing adequate instructions for use, and ongoing technical support. The use of cloud-based data collection methods may also reduce the onus on participants, enabling remote monitoring of adherence and data management from devices.
The inclusion of devices in study design may result in greater participant burden ranging from the intrusion of remembering to wear sensors to attending more remote appointments. It is important that these factors are considered in study design. This burden may also be felt by caregiving relatives and friends as people with MND experiencing motor decline or cognitive impairment may require prompting and physical assistance from a caregiver to adhere to study requirements.
Choice of device
The aim of this study was to systematically review the current landscape of research using devices to explore motor progression in MND. Device suitability is dependent upon the research aims, the intended participant group and project resources but more research into the properties of these devices, and their acceptability to people with MND can help inform future decisions.
A key aspect requiring consideration is the current lack of consensus regarding choices of device for digital data capture. This lack of consensus, linked to the small sample sizes [27] and low quality of existing evidence [29, 37], introduces uncertainty, and may limit uptake in clinical trial design and also patient care.
Prospective studies, with larger sample sizes, longer follow-up durations and direct feedback from device users [43] are required to evaluate the utility of devices and establish which devices are most suitable in MND. The development of strategic guidelines would be beneficial to harmonise approaches and inform future study design and clinical care integration. Many devices contain multiple sensors and investigators must balance the benefits of additional data collection with concerns over decrease battery life and greater data storage requirements. If using accompanying software, the type available for data analysis and data visualisation is relevant in informing design decisions.
Data analysis and management
A further potential challenge for researchers incorporating devices in trial design, and clinicians integrating devices into care, is how to use device data to evaluate progression. A clear, pre-defined plan for evaluating digitally derived data, correlating with existing validated outcomes and determining thresholds of progression are crucial [44].
As with any outcome measures, the findings from studies using devices can be affected by missing data. Data points may be compromised due to technical issues of erroneous recordings, transferring and storage of data. Studies included in this review reported issues with missing data affecting the ability to draw clinical conclusions from results, due to participants withdrawing early due to adverse effects [24] or being unable to use the technology to collect data [30]. Investigators must manage the risk of missing data, and develop study-specific plans to account for this in data analysis for future studies.
If investigators intend to use raw data for analysis, how the data is stored and organised and the availability of groups with expertise in this type of data analysis must be a crucial consideration. Concerns regarding data security and adherence to privacy regulations may also be a barrier to integrating technologies in study design. Providing detailed data management plans, reviewed by specialists in data security will help to pre-emptively address concerns of prospective participants, regulatory bodies and funders.
Cost of devices
A potential concern for prospective users, regulatory bodies, funders, clinicians and research teams is the cost of providing technologies. Accessibility of these devices may be limited by the cost of providing equipment such as tablets and computers, or purchasing specialist voice recognition or eye gaze software. Approximate costs for devices, where available, are reported in Table 2. Resource is also required for storage and interpretation of data requiring interdisciplinary collaboration with clinicians, data scientists, information governance, and IT security. Ensuring future work is not limited in scope by access to devices, will be difficult to address without additional funding for MND care and research.
Conclusion
Overall, the use of devices for measuring disease progression in MND is a promising direction of research. The reviewed literature was primarily proof-of-concept, exploratory studies with shorter periods of follow-up and smaller sample sizes, limiting the conclusions that can be drawn from the findings. In addition, a large amount of data were unavailable to determine risk of bias accurately, and for the information available, a high risk of bias was indicated. The COVID-19 pandemic has highlighted the importance of implementing remote assessment, using the types of technology discussed in this study, for people with MND [45]. Devices offer the opportunity to decentralise trial delivery and reduce the burden felt by participants previously required to travel to additional appointments.
Future work
Clinicians and trialists designing research to incorporate these devices will face a unique set of considerations and challenges. The body region to be assessed, ease of use, frequency and sensitivity of sampling, reliability, cost to purchase, battery life and storage capacity of devices must be evaluated. The shift towards telemedicine in clinical care may offer valuable insights into delivering effecting remote research opportunities for people with MND [46].
This study indicates a variety of devices are potentially suitable to measure physical symptoms in MND and potentially useful as additional outcome measures in trials. The multi-systemic impact of MND presents multiple potential targets for evaluation as potential technological biomarkers, including speech, motor function, cognition and overall functional ability [47].
As there are a number of potentially suitable devices, the decision on what to use must also consider acceptability to participants, cost, area of function to assess and sensitivity to change. Identifying relevant devices, establishing their suitability and providing clear procedures for integration into health research, specifically for MND, are outlined by Van Eijk et al., who highlight the importance of digital biomarkers [44].
When establishing the responsiveness of a device, future research should evaluate progression of each currently affected area of the body, not just as covariance with total scores from existing measures of progression such as the ALS-FRS(R), which may not be sensitive to detect smaller changes in function. Future work should focus on developing guidelines for clinicians and researchers on available devices, suitability for MND and aspects of functioning measured.
Availability of data and materials
Appendix 2_Project Data.
Code availability
Not applicable.
References
Leighton DJ et al (2019) Changing epidemiology of motor neurone disease in Scotland. J Neurol 266(4):817–825
Miller RG, Mitchell JD, Moore DH (2012) Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD001447.pub3
Wong C et al (2021) Clinical trials in amyotrophic lateral sclerosis: a systematic review and perspective. Brain Commun 3(4):fcab242
Rooney J et al (2017) What does the ALSFRS-R really measure? A longitudinal and survival analysis of functional dimension subscores in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry 88(5):381–385
van Eijk RP et al (2021) An old friend who has overstayed their welcome: the ALSFRS-R total score as primary endpoint for ALS clinical trials. Amyotroph Lateral Scler Frontotemporal Degener 22(3–4):300–307
Hobson EV et al (2018) The TiM system: developing a novel telehealth service to improve access to specialist care in motor neurone disease using user-centered design. Amyotroph Lateral Scler Frontotemporal Degener 19(5–6):351–361
Hobson EV et al (2016) Using technology to improve access to specialist care in amyotrophic lateral sclerosis: a systematic review. Amyotroph Lateral Scler Frontotemporal Degener 17(5–6):313–324
Cohen AB, Nahed BV, Sheth KN (2013) Mobile medical applications in neurology. Neurology 3(1):52–60
Beghi E et al (2011) The epidemiology and treatment of ALS: focus on the heterogeneity of the disease and critical appraisal of therapeutic trials. Amyotroph Lateral Scler 12(1):1–10
van Eijk RPA et al (2019) Accelerometry for remote monitoring of physical activity in amyotrophic lateral sclerosis: a longitudinal cohort study. J Neurol 266(10):2387–2395
Rutkove S et al (2020) Accelerating clinical therapeutic trials in ALS through frequent at-home data collection. Neurology 94(15):4921
Rutkove SB et al (2020) Improved ALS clinical trials through frequent at-home self-assessment: a proof of concept study. Ann Clin Transl Neurol 7(7):1148–1157
Berry JD et al (2019) Design and results of a smartphone-based digital phenotyping study to quantify ALS progression. Ann Clin Transl Neurol 6(5):873–881
Ahmad N et al (2013) Reviews on various inertial measurement unit (IMU) sensor applications. Int J Signal Process Syst 1(2):256–262
Rutkove SB et al (2012) Electrical impedance myography as a biomarker to assess ALS progression. Amyotroph Lateral Scler 13(5):439–445
Andres PL et al (2017) Fixed dynamometry is more sensitive than vital capacity or ALS rating scale. Muscle Nerve 56(4):710–715
Ossig C et al (2016) Wearable sensor-based objective assessment of motor symptoms in Parkinson’s disease. J Neural Transm (Vienna) 123(1):57–64
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed1000097
Whiting PF et al (2011) QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 155(8):529–536
Cedarbaum JM et al (1999) The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (Phase III). J Neurol Sci 169(1–2):13–21
Bakers JN et al (2021) Portable fixed dynamometry: towards remote muscle strength measurements in patients with motor neuron disease. J Neurol 268(5):1738–1746
Beukenhorst AL et al (2021) Smartphone data during the COVID-19 pandemic can quantify behavioral changes in people with ALS. Muscle Nerve 63(2):258–262
de Bie E et al (2017) Longitudinal evaluation of upper extremity reachable workspace in ALS by Kinect sensor. Amyotroph Lateral Scler Frontotemporal Degener 18(1–2):17–23
Garcia-Gancedo L et al (2019) Objectively monitoring amyotrophic lateral sclerosis patient symptoms during clinical trials with sensors: observational study. JMIR Mhealth Uhealth 7(12):e13433
Geronimo A, Martin AE, Simmons Z (2021) Inertial sensing of step kinematics in ambulatory patients with ALS and related motor neuron diseases. J Med Eng Technol 45(6):486–493
Kelly M et al (2020) The use of biotelemetry to explore disease progression markers in amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener 21(7–8):563–573
Londral A et al (2013) A method to detect keystrokes using accelerometry to quantify typing rate and monitor neurodegenerative progression. In NEUROTECHNIX
Montero-Odasso M et al (2017) Motor phenotype in neurodegenerative disorders: gait and balance platform study design protocol for the Ontario neurodegenerative research initiative (ONDRI). J Alzheimers Dis 59(2):707–721
Oskarsson B et al (2016) Upper extremity 3-dimensional reachable workspace assessment in amyotrophic lateral sclerosis by Kinect sensor. Muscle Nerve 53(2):234–241
Rutkove SB et al (2019) ALS longitudinal studies with frequent data collection at home: study design and baseline data. Amyotroph Lateral Scler Frontotemporal Degener 20(1–2):61–67
Shefner JM et al (2018) Reducing sample size requirements for future ALS clinical trials with a dedicated electrical impedance myography system. Amyotroph Lateral Scler Frontotemporal Degener 19(7–8):555–561
Trevizan IL et al (2018) Efficacy of different interaction devices using non-immersive virtual tasks in individuals with Amyotrophic Lateral Sclerosis: a cross-sectional randomized trial. BMC Neurol 18(1):1–10
Vieira FG et al (2022) A machine-learning based objective measure for ALS disease severity. NPJ Digit Med 5(1):1–9
Farhan SMK et al (2017) The Ontario neurodegenerative disease research initiative (ONDRI). Can J Neurol Sci 44(2):196–202
Vert A et al (2022) Detecting accelerometer non-wear periods using change in acceleration combined with rate-of-change in temperature. BMC Med Res Methodol 22(1):147–147
Godkin FE et al (2022) Feasibility of a continuous, multi-sensor remote health monitoring approach in persons living with neurodegenerative disease. J Neurol 269(5):2673–2686. https://doi.org/10.1007/s00415-021-10831-z
Esser P et al (2011) Assessment of spatio-temporal gait parameters using inertial measurement units in neurological populations. Gait Posture 34(4):558–560
Londral A, Pinto S, de Carvalho M (2016) Markers for upper limb dysfunction in Amyotrophic Lateral Sclerosis using analysis of typing activity. Clin Neurophysiol 127(1):925–931
Kurillo G et al (2013) Evaluation of upper extremity reachable workspace using Kinect camera. Technol Health Care 21(6):641–656
Canosa A et al (2020) Lifetime sport practice and brain metabolism in Amyotrophic Lateral Sclerosis. Neuroimage 27:102312
Capecci M et al (2019) Clinical effects of robot-assisted gait training and treadmill training for Parkinson’s disease. A randomized controlled trial. Ann Phys Rehabil Med 62(5):303–312
Gijbels D et al (2010) Predicting habitual walking performance in multiple sclerosis: relevance of capacity and self-report measures. Mult Scler J 16(5):618–626
van Eijk RP et al (2019) Refining eligibility criteria for amyotrophic lateral sclerosis clinical trials. Neurology 92(5):e451–e460
van Eijk RPA et al (2021) A road map for remote digital health technology for motor neuron disease. J Med Internet Res 23(9):e28766
Bombaci A et al (2021) Telemedicine for management of patients with amyotrophic lateral sclerosis through COVID-19 tail. Neurol Sci 42(1):9–13
Pugliese R et al (2022) Emerging technologies for management of patients with amyotrophic lateral sclerosis: from telehealth to assistive robotics and neural interfaces. J Neurol 269(6):2910–2921
Ramanarayanan V et al (2022) Speech as a biomarker: opportunities, interpretability, and challenges. Perspect ASHA Special Interest Groups 7(1):276–283
Funding
The Euan MacDonald Centre for Motor Neuron Disease Research. SC is supported by the UK Dementia Research Institute (DRI), which receives its funding from UK DRI Ltd, funded by the MRC, Alzheimer’s Society and Alzheimer’s Research UK.
Author information
Authors and Affiliations
Contributions
SP and EB contributed to the conception of the project. EB, TF, and SP carried out the literature searches and data acquisition, interpretation and analysis. EB, TF, SP, DF, RD, JN, SA, SC and DP drafted the manuscript. The manuscript was reviewed and approved for publication by all the authors.
Corresponding author
Ethics declarations
Conflicts of interest
Professor Carson is a paid editor at Journal of Neurology, Neurosurgery and Psychiatry, and gives independent testimony in Court on a range of neuropsychiatric topics.
Ethical standard statement
The authors confirm that this article complies with ethical standards.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Beswick, E., Fawcett, T., Hassan, Z. et al. A systematic review of digital technology to evaluate motor function and disease progression in motor neuron disease. J Neurol 269, 6254–6268 (2022). https://doi.org/10.1007/s00415-022-11312-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-022-11312-7