
Abstract
Background and purpose
Direct presentation of patients with acute ischemic stroke to a comprehensive stroke center (CSC) reduces time to endovascular treatment (EVT), but may increase time to treatment for intravenous thrombolysis (IVT). This dilemma, however, is not applicable to patients who have a contraindication for IVT. We examined the effect of direct presentation to a CSC on outcomes after EVT in patients not eligible for IVT.
Methods
We used data from the MR CLEAN Registry (2014–2017). We included patients who were not treated with IVT and compared patients directly presented to a CSC to patients transferred from a primary stroke center. Outcomes included treatment times and 90-day modified Rankin Scale scores (mRS) adjusted for potential confounders.
Results
Of the 3637 patients, 680 (19%) did not receive IVT and were included in the analyses. Of these, 389 (57%) were directly presented to a CSC. The most common contraindications for IVT were anticoagulation use (49%) and presentation > 4.5 h after onset (26%). Directly presented patients had lower baseline NIHSS scores (median 16 vs. 17, p = 0.015), higher onset-to-first-door times (median 105 vs. 66 min, p < 0.001), lower first-door-to-groin times (median 93 vs. 150 min; adjusted β = − 51.6, 95% CI: − 64.0 to − 39.2) and lower onset-to-groin times (median 220 vs. 230 min; adjusted β = − 44.0, 95% CI: − 65.5 to − 22.4). The 90-day mRS score did not differ between groups (adjusted OR: 1.23, 95% CI: 0.73–2.08).
Conclusions
In patients who were not eligible for IVT, treatment times for EVT were better for patients directly presented to a CSC, but without a statistically significant effect on clinical outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Intravenous thrombolysis (IVT) is the standard treatment for patients with acute ischemic stroke (AIS) [1]. Patients with a large vessel occlusion (LVO) of the anterior circulation are additionally treated with endovascular treatment (EVT) [2]. In most countries, paramedics transport patients with a suspected AIS to the nearest primary stroke center (PSC) for diagnostic work-up and to initiate IVT. Patients who are eligible for EVT are subsequently transferred to a comprehensive stroke center (CSC). Studies show that this ‘drip-and-ship’ system delays initiation of EVT by 40–106 min and decreases the chance of a good clinical outcome by approximately 10% [3,4,5]. Despite this clear disadvantage, the ‘drip-and-ship’ system is currently the most feasible, because accurately diagnosing an LVO in the prehospital setting is challenging. Directly presenting all patients with suspected AIS to a CSC would overburden these hospitals. In addition, due to longer initial travel times, a centralized model could delay initiation of IVT, and thus negatively impact patient outcome in patients who are not eligible for EVT [5].
Approximately 20% of patients who undergo EVT in routine practice do not receive IVT because of a contraindication for alteplase [6]. Most of these contraindications, such as anticoagulation use and duration of symptoms > 4.5 h, can be easily determined in the ambulance. For patients with such a contraindication for IVT, no valuable time would be lost by bypassing the PSC and going directly to a CSC. In the current study, we analyzed workflow times and clinical outcomes after EVT in patients who were not eligible for IVT, and compared these outcomes between patients who were directly presented to a CSC to those initially presented to a PSC.
Methods
Data will not be made available to other researchers, as no patient approval was obtained for sharing coded data. However, syntax and output files of statistical analyses may be made available on request.
Study design and population
We used data from the MR CLEAN Registry. The MR CLEAN Registry is a nationwide, prospective cohort study, in which all patients who have undergone EVT for AIS in the Netherlands since completion of the MR CLEAN trial (March 2014) until December 2018 have been registered. Permission to carry out this study was granted by the medical ethics committee of the Erasmus University Medical Center in Rotterdam. Detailed methods of the MR CLEAN Registry have previously been reported [6]. For the current study, we used data collected from March 2014 until November 2017 (Registry part I and II). We included patients who had undergone EVT for AIS, and did not receive IVT. In-hospital strokes were excluded.
Definitions and outcomes
EVT was defined as arterial puncture in the angiography suite, with the objective to perform mechanical thrombectomy with a stent retriever and/or thrombus aspiration, with or without local administration of a thrombolytic agent. The actual EVT strategy was at the discretion of the interventionist. Time of stroke onset was defined as the time of witnessed onset of symptoms or, if this was unknown, the moment that the patient was last known to be well.
Our primary clinical outcome measure was good functional outcome at 90 days post-stroke, defined as a score of 0–2 on the modified Rankin Scale (mRS). Other clinical outcome measures were the overall shift in mRS score between groups, occurrence of symptomatic intracranial hemorrhage (sICH) and mortality at 90 days post-stroke. Intracranial hemorrhage was defined as symptomatic if the patient died or deteriorated neurologically (an increase of ≥ 4 points on the National Institutes of Health Stroke Scale [NIHSS]) as a result of the hemorrhage [7]. Successful reperfusion, defined as a score of ≥ 2b on the extended thrombolysis in cerebral infarction (eTICI) scale, was used as a radiological outcome measure.
Workflow-related outcome measures were: time from stroke onset to arterial puncture [onset-to-groin time (OGT)], which was our main secondary outcome measure, and time from arrival at the first hospital to arterial puncture [first-door-to-groin time (FDGT)].
Transferred patients generally live farther away from a CSC than mothership patients, which makes a direct comparison of treatment times inherently biased in favor of patients directly presented to a CSC. To account for this bias, we calculated adjusted OGT and FDGT, in which we corrected for travel time by subtracting estimated ambulance travel times between the PSC and the CSC from the original treatment times, for all transferred patients. These data were provided by the Dutch National Institute for Public Health and the Environment and calculated using their proprietary model, assuming daytime circumstances outside of rush hour and the ambulance driving with the highest level of emergency [8].
Statistical analysis
Patients who were directly presented to a CSC were compared to patients who were transferred from a PSC. We compared baseline characteristics using independent sample t test for normally distributed continuous variables, Mann–Whitney U test for non-normally distributed continuous variables, and χ2 test for categorical variables. For the regression analyses, we imputed missing data using multiple imputation, using the following covariates: age, sex, previous stroke, previous diabetes, previous atrial fibrillation, previous myocardial infarction, pre-stroke mRS score, baseline blood pressure (systolic and diastolic), baseline NIHSS score, location of occlusion, collateral status, onset-to-first-door time, OGT, FDGT, onset-to-reperfusion time, eTICI score after EVT, and mRS score at 90 days post-stroke. To analyze the odds of good functional outcome, defined as mRS 0–2 at 90 days, we used binary logistic regression. Ordinal logistic regression was used to assess the overall shift in mRS score between groups. In both analyses, we adjusted for the following pre-specified prognostic variables: age, pre-stroke mRS, anticoagulation use, baseline NIHSS, location of occlusion, collateral status, and onset-to-first-door time. For our analyses of sICH and mortality, we also used binary logistic regression, adjusting for age, pre-stroke mRS, anticoagulation use, baseline systolic blood pressure, baseline NIHSS, location of occlusion, collateral status and onset-to-first-door time. For analyzing successful reperfusion rate (eTICI ≥ 2b), we used binary logistic regression and adjusted for the following variables: age, location of occlusion and onset-to-first door time. Linear regression was used for the analyses of OGT and FDGT (with and without correction for travel time). In the OGT analysis, we adjusted for age, pre-stroke mRS, baseline blood pressure, baseline NIHSS, location of occlusion and presentation outside the 4.5 h time window. In the FDGT analysis, we adjusted for age, pre-stroke mRS, baseline blood pressure, baseline NIHSS, location of occlusion, and onset-to-first-door time. To explore residual confounding, we performed a secondary analysis in which we stratified for presentation to the first hospital within the 4.5 h time window. In this analysis, we used all clinical, radiological, and workflow-related outcomes named above. All analyses were performed using SPSS (version 25; SPSS Inc., Chicago, IL, USA).
Results
Between March 2014 and November 2017, 3637 patients were included in the MR CLEAN Registry (part I and II). We excluded 2957 patients, either because they were treated with IVT (n = 2640), because it was unknown whether they were treated with IVT (n = 74), or because they had an in-hospital stroke (n = 243). Therefore, 680 patients were included in the analysis (Fig. 1). Of these, 389 (57%) were directly presented to a CSC and 291 (43%) were transferred from a PSC. Patients who were directly presented to a CSC less often had atrial fibrillation (38% vs. 54%, p < 0.001), had lower baseline NIHSS scores (median 16 vs. 17, p = 0.015) and had higher collateral scores on baseline CTA (p = 0.003) compared to transferred patients. Onset-to-first-door times were longer for the direct group [median 105 vs. 66 min, p < 0.001 (Table 1)]. The median estimated ambulance travel time between PSC and CSC for the transferred group was 17 min (IQR: 10–31). Contraindications for IVT are listed in Table 1. Presentation beyond the 4.5 h time window was more common in directly presented patients (35% vs. 15%, p < 0.001). Use of a vitamin K antagonist was less frequent in directly presented patients (32% vs. 45%, p < 0.001), while heparin use (therapeutic dosage) was more common in the direct group (2% vs. 0%, p = 0.040). Other contraindications did not differ between the two groups.

Flowchart of patient selection. CSC comprehensive stroke center, IVT intravenous thrombolysis, Registry the multicenter collaboration for endovascular treatment of acute ischemic stroke in the Netherlands (MR CLEAN Registry)
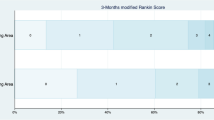
Functional outcome was slightly better in patients who were directly presented to a CSC [mRS 0–2: 36 vs. 28%, OR: 1.51, 95% CI 1.06–2.15 (Table 2; Fig. 2)]. After adjustment, statistical significance was lost (adjusted OR: 1.23, 95% CI 0.73–2.08). When analyzing the shift in overall mRS scores between groups, the results were similar (unadjusted common OR: 1.43, 95% CI 1.07–1.91; adjusted common OR: 1.21, 95% CI 0.80–1.84). Incidence of sICH did not differ between the direct group and the transferred group (5% vs. 5%; adjusted OR: 0.70, 95% CI 0.28–1.75). Other clinical and radiological outcomes also were not different (Table 2).

Functional outcome according to modified Rankin Scale score at 90 days post-stroke. D direct group, T transferred group
Patients directly presented to a CSC had a median OGT of 220 min, compared to 230 min for transferred patients [adjusted β = − 40.0, 95% CI − 61.5 to − 18.5 (Table 3)]. When the increased travel time for transferred patients was taken into account, adjusted OGT was still 18 min shorter for patients directly presented to a CSC, although this was not statistically significant (median 220 vs. 207 min; adjusted β = − 18.1, 95% CI − 39.6 to 3.4). FDGT was also shorter for the direct group (median 93 vs. 150 min; adjusted β = − 51.0, 95% CI − 64.1 to − 37.9), even when corrected for increased travel time (median 93 vs. 127 min, adjusted β = − 28.0, 95% CI − 41.3 to − 14.7).
We stratified the analysis for presentation to the first hospital within the 4.5 h time window. Of 476 patients presented within 4.5 h, 290 (61%) were presented directly to a CSC. Among patients presented outside the 4.5 h time window, direct presentation was more common, with 90/108 patients (83%) being presented directly to a CSC. Baseline characteristics of the two strata are shown in Online Resource 2. Within the 4,5 h time window, patients presented directly to a CSC more often were functionally independent at 90 days [mRS 0–2: 36 vs. 26%, OR: 1.65, 95% CI 1.07–2.56 (Table 4)]. After adjustments for potential confounders, this difference was no longer statistically significant (adjusted OR: 1.28, 95% CI 0.74–2.22). We found similar results for the overall shift in mRS between groups among patients presented within 4.5 h (unadjusted common OR: 1.47, 95% CI 1.04–2.09; adjusted common OR: 1.17, 95% CI 0.76–1.81). Among patients who were presented > 4.5 h after symptom onset there was no difference in functional outcome (adjusted OR: 0.89, 95% CI 0.18–4.29). Other clinical and radiological outcomes also did not differ (Table 4). In patients presented within 4.5 h, the difference in OGT remained statistically significant, in favor of the direct group (median 180 vs. 228 min; adjusted β = − 46.4, 95% CI − 66.1 to − 26.6). In patients presented after > 4.5 h, OGT did not differ between groups (median 457 vs. 455 min; adjusted β = − 8.1, 95% CI − 115.9 to 99.7). The difference in FDGT in favor of the direct group remained statistically significant in both strata (≤ 4.5 h: adjusted β = − 50.8, 95% CI − 65.7 to − 36.2; > 4.5 h: adjusted β = − 47.0, 95% CI − 71.7 to − 22.3). The results of our analyses for both strata of OGT and FDGT corrected for travel time are reported in Online Resource 3.
Discussion
In this nationwide cohort of patients who underwent EVT for AIS, we found that in the subgroup of patients who were not eligible for IVT, treatment times were shorter for patients directly presented to a CSC, compared to patients who were first presented to a PSC. Clinical outcome was also slightly better in directly presented patients, although this was not statistically significant.
Previous post hoc analyses of prospective cohort studies have shown that for patients with an LVO of the anterior circulation, in general, it is beneficial to be directly presented to a CSC, as opposed to being transferred from a PSC. Venema et al., who also used data from the MR CLEAN Registry (part I), found that patients directly presented to a CSC had a 40-min shorter OGT and a 57-min shorter FDGT than transferred patients [3]. The authors also found a negative effect of inter-hospital transfer on the likelihood of functioning independently at 90 days post-stroke (OR: 0.69, 95% CI 0.54–0.89). A post hoc analysis of data from the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke) showed a similar beneficial effect of direct presentation on functional outcome [5]. However, in a subgroup analysis of patients who were not treated with IVT, the authors found that despite the OGT being almost an hour lower, the chance of good functional outcome did not differ between directly presented and transferred patients (56% vs. 50%, p = 0.23). Since previous studies have convincingly shown that earlier initiation of EVT improves clinical outcome, these findings seem discrepant [4, 9,10,11]. However, the authors did not report if and how their subgroup analysis was adjusted for possible confounders, neither were baseline characteristics reported for the subgroup of patients treated with EVT alone.
In the current study, despite adjustment for baseline imbalances, we found the same discrepancy as did the authors of the STRATIS Registry substudy: a beneficial effect of direct presentation on time to treatment, but no statistically significant difference in functional outcome. A potential explanation for this finding is that our sample size was too small to find a difference in functional outcome, but substantial enough to show the larger differences in time to treatment. Another possible explanation could be residual confounding. Although we tried to adjust for factors that, based on baseline characteristics and clinical experience, may have influenced the hospital choice by ambulance paramedics or the choice of referral for EVT by PSC neurologists, there may be other confounding factors that we did not take into account or that we had no data for. For example, patients with severe comorbidity (e.g. active malignancy, renal failure, and congestive heart failure) may be more likely to be directly presented to CSCs, since CSCs are often tertiary care centers. Because data of these severe comorbidities were not available for our study, we could not adjust our analyses for this potential confounder.
There were some baseline imbalances between the direct and the transferred group that warrant mention. First, the transferred group more often had atrial fibrillation. A probable explanation is that this is due to the different distributions of contraindications for IVT over the two groups. Since the transfer group contains relatively few patients in the > 4.5 h time window, other contraindications for IVT are more prevalent in this group. Of these, the most common contraindication is use of anticoagulant medication. Because the indication for anticoagulation use often is atrial fibrillation, this may explain the higher prevalence in this group. Second, the transferred group had higher baseline NIHSS scores. A possible explanation could be that patients with relatively mild neurological deficits were less often referred from a PSC, for instance because the deficits were not considered to be sufficiently severe to warrant EVT. Third, collateral scores were slightly better in directly presented patients. This may be because atrial fibrillation was less common in this group, since this has been associated with worse collaterals [12]. Fourth, time from stroke onset to arrival at the first hospital was significantly longer for directly presented patients. Most likely, this is because ambulance paramedics were inclined to bring patients who were (almost) outside the 4.5 h time window, who were thus only eligible for EVT, directly to a CSC.
We specifically focused on the effects of interhospital transfer in the subgroup of patients not eligible for IVT. We chose to do so, because of the relevance of this subject for routine clinical practice. In approximately 15–20% of patients with AIS, a contraindication for IVT is present [2, 6]. Unlike patients eligible for IVT, in whom direct presentation to a CSC may delay initiation of this treatment, patients ineligible for IVT have no major disadvantage of being presented directly to a CSC. Moreover, the most common contraindications that render patients ineligible for IVT could be identified by ambulance paramedics. For example, anticoagulant use or duration of symptoms could be determined through a patient history. Blood pressure is routinely measured, and an INR could be determined using a point of care test [13]. Further study on this issue is required, for instance to ascertain if determining IVT contraindications negatively influences ambulance response times. However, if such studies do not show any major negative effects, prehospital triage of this patient group could relatively easily be implemented.
Some limitations of our study should also be considered. First of all, the Netherlands, where data collection for this study took place, is a relatively small and densely populated country, where hospitals are located relatively close to one another [14]. Therefore, the differences in time to treatment between directly presented and transferred patients that we found in this study, are likely smaller than they would have been in less densely populated areas [15, 16]. Consequently, our findings should be extrapolated to other countries with caution.
Second, it is likely that our data were affected by selection bias. In the MR CLEAN Registry, patients with an LVO who were ultimately deemed ineligible for EVT for whatever reason, were not included. As a consequence, we have no data of patients that could not receive EVT because of time lost by primary transportation to a PSC causing the time window for EVT to exceed [17]. Therefore, the negative effects of inter-hospital transfer may be larger than shown in this study. Additionally, selection bias is inherent to the manner of hospital selection by ambulance paramedics. Even though the protocol in the Netherlands is to bring patients with a suspected stroke to the nearest stroke center, ambulance paramedics may nonetheless decide to bypass a PSC and bring a patient directly to a CSC. In a similar way, factors affecting the decision of PSC neurologists whether or not to refer a patient for EVT may have influenced our data. By adjusting our analyses for potential confounders, based on clinical experience and baseline imbalances, we have tried to minimize the impact of this issue on our results.
Finally, for some variables we had relatively high numbers of missing values, the most important of which were onset-to-first-door time (14%), FDGT (14%), and mRS score at 90 days post-stroke (8%). We tried to minimize the impact of the missing data on our analyses using multiple imputation, as described in the methods section.
Further research should focus on finding a triage instrument for prehospital selection of patients eligible for EVT, so that these patients can be brought directly to a CSC, without overburdening these hospitals with patients who can be treated in a PSC. Results of other research toward optimization of prehospital stroke logistics are expected in the coming years: a randomized controlled trial in Spain [Direct Transfer to an Endovascular Center Compared to Transfer to the Closest Stroke Centre in Acute Stroke Patients With Suspected Large Vessel Occlusion (RACECAT), Clinicaltrials.gov number: NCT02795962] is comparing direct presentation to transfer to a CSC in patients with a high likelihood of an LVO. Until then, directly presenting patients with a suspected stroke and a contraindication for IVT to a CSC may be considered, since there is no obvious disadvantage in bypassing the PSC in this patient population. Implementing this would, however, result in a higher patient load for CSCs. Other studies have shown that approximately 10% of suspected stroke patients have an LVO [18], and in our cohort, 19% of patients with an LVO had a contraindication for IVT. Assuming that the proportion of patients with a contraindication for IVT is also 19% in the entire population of patients with a suspected AIS, routing these patients directly to a CSC would mean that for every patient with an LVO and a contraindication for IVT, approximately nine patients without an LVO and with a contraindication for IVT would be presented to a CSC. In addition to the higher patient load, unnecessary transportation of these patients to a CSC may also be a burden on the patients and their families, because it may involve admission to a hospital further from home. To reduce the number of unnecessary direct presentations to a CSC, a triage method applied by paramedics, such as a clinical LVO-detection scale, may be useful.
In conclusion, we showed that in patients with an LVO who were not eligible for IVT, direct presentation to a CSC decreased time to EVT, compared to initial presentation to a PSC. Direct presentation was also associated with a slightly better clinical outcome that was not statistically significant. Since there is no obvious disadvantage in bypassing the PSC in this patient population, directly presenting patients with a suspected stroke and a contraindication for IVT to a CSC, if logistically feasible, may be considered.
References
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K et al (2018) 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 49:e46–e110
Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM et al, HERMES Collaborators (2016) Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 387:1723–1731
Venema E, Groot AE, Lingsma HF, Hinsenveld W, Treurniet KM, Chalos V et al (2019) Effect of interhospital transfer on endovascular treatment for acute ischemic stroke. Stroke 50:923–930
Saver JL, Goyal M, van der Lugt A, Menon BK, Majoie CB, Dippel DW et al, HERMES Collaborators (2016) Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA 316:1279–1288
Froehler MT, Saver JL, Zaidat OO, Jahan R, Aziz-Sultan MA, Klucznik RP, STRATIS Investigators et al (2017) Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke). Circulation 136:2311–2321
Jansen IGH, Mulder MJHL, Goldhoorn RB, Registry Investigators MRCLEAN (2018) Endovascular treatment for acute ischaemic stroke in routine clinical practice: prospective, observational cohort study (MR CLEAN Registry). BMJ 360:k949
Von Kummer R, Broderick JP, Campbell BC, Demchuk A, Goyal M, Hill MD et al (2015) The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke 46:2981–2986
Kommer GJ, Zwakhals SL, Over E, Dutch National Institute for Public Health and the Environment (2017) Models for the National Ambulance Plan 2016. https://www.rivm.nl/publicaties/modellen-referentiekader-ambulancezorg-2016-ontwikkeling-modellen-voor-dam-b-vervoer-en. Accessed 20 Apr 2017.
Mulder MJHL, Jansen IGH, Goldhoorn RB, Venema E, Chalos V, Compagne KCJ, MR CLEAN Registry Investigators et al (2018) Time to endovascular treatment and outcome in acute ischemic stroke: MR CLEAN Registry results. Circulation 138:232–240
Fransen PS, Berkhemer OA, Lingsma HF, Beumer D, van den Berg LA, Yoo AJ, Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands Investigators et al (2016) Time to reperfusion and treatment effect for acute ischemic stroke: a randomized clinical trial. JAMA Neurol 73:190–196
Nogueira RG, Smith WS, Sung G, Duckwiler G, Walker G, Roberts R et al (2011) Effect of time to reperfusion on clinical outcome of anterior circulation strokes treated with thrombectomy: pooled analysis of the MERCI and Multi MERCI trials. Stroke 42:3144–3149
Guglielmi V, LeCouffe NE, Zinkstok SM, Compagne KCJ, Eker R, Treurniet KM, MR CLEAN Registry Investigators et al (2019) Collateral circulation and outcome in atherosclerotic versus cardioembolic cerebral large vessel occlusion. Stroke 50:3360–3368
Beynon C, Erk AG, Potzy A, Mohr S, Popp E (2015) Point of care coagulometry in prehospital emergency care: an observational study. Scand J Trauma Resusc Emerg Med 23:58
Kommer GJ, van den Broek I, de Bruin-Kooistra M, Deuning C; Dutch National Institute for Public Health and the Environment (2017) Supply and accessibility of emergency hospital care in the Netherlands 2017: analysis of the geographical accessibility of hospitals. https://www.rivm.nl/publicaties/aanbod-en-bereikbaarheid-van-spoedeisende-ziekenhuiszorg-in-nederland-2017-analyse. Accessed 9 Nov 2017.
Adeoye O, Albright KC, Carr BG, Wolff C, Mullen MT, Abruzzo T et al (2014) Geographic access to acute stroke care in the United States. Stroke 45:3019–3024
Albright KC, Branas CC, Meyer BC, Matherne-Meyer BCM, Zivin JA, Lyden PD et al (2010) ACCESS: acute cerebrovascular care in emergency stroke systems. Arch Neurol 67:1210–1218
Prabhakaran S, Ward E, John S, Lopes DK, Chen M, Temes RE et al (2011) Transfer delay is a major factor limiting the use of intra-arterial treatment in acute ischemic stroke. Stroke 42:1626–1630
Helwig SA, Ragoschke-Schumm A, Schwindling L, Kettner M, Roumia S, Kulikovski J et al (2019) Prehospital stroke management optimized by use of clinical scoring vs mobile stroke unit for triage of patients with stroke: a randomized clinical trial. JAMA Neurol. https://doi.org/10.1001/jamaneurol.2019.2829
Funding
The MR CLEAN Registry was funded and carried out by Erasmus University Medical Center, Amsterdam UMC, and Maastricht University Medical Center. The study was additionally funded by the Applied Scientific Institute for Neuromodulation (Toegepast Wetenschappelijk Instituut voor Neuromodulatie), which played no role in trial design and patient enrollment, nor in data collection, analysis, or writing of the article.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analyses were performed by LM, AG, and JC. The first draft of the manuscript was written by LM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Majoie reports grants from CVON/Dutch Heart Foundation, European Commission, TWIN Foundation and Stryker, outside the submitted work (paid to institution). In addition, Dr. Majoie is shareholder of Nico.lab, a company that focuses on the use of artificial intelligence for medical image analysis. Dr. Roos reports stockholdings from Nico.lab outside the submitted work. Dr. Coutinho reports grants from Medtronic outside the submitted work. Dr. Majoie, Dr. Roos, and Dr. Coutinho are (co-)investigators of the MR-CLEAN-NO IV trial (ISRCTN80619088). The other authors report no conflicts.
Ethical standards
Permission to carry out the MR CLEAN Registry study was granted by the medical ethics committee of the Erasmus University Medical Center in Rotterdam. This study was carried out in accordance with the Declaration of Helsinki.
Additional information
MR CLEAN Registry Investigators-group authors: please see Online Resource 1.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van Meenen, L.C.C., Groot, A.E., Venema, E. et al. Interhospital transfer vs. direct presentation of patients with a large vessel occlusion not eligible for IV thrombolysis. J Neurol 267, 2142–2150 (2020). https://doi.org/10.1007/s00415-020-09812-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-020-09812-5