
Abstract
Children involved in car crashes can experience either direct trauma or inertial injuries resulting from interactions with external objects, such as other vehicles, or with the restraint system. Furthermore, improper use of restraint systems can lead to additional severe injuries. Recent reports from international institutions underscored the persistent prevalence of inadequate restraint systems utilization and this widespread issue increases children’s vulnerability and risk of injuries.
The aim of this study is to provide a systematic review of the literature on injuries sustained in children involved in road accidents describing and analyzing elements useful for forensic assessment.
The literature search was performed using PubMed, Scopus and Web of Science from January 1970 to March 2023. Eligible studies have investigated issues of interest to forensic medicine about traffic accidents involving pediatric passengers. A total of 69 studies satisfied the inclusion criteria and were categorized and analyzed according to the anatomical regions of the body affected (head, neck, thoraco-abdominal, and limb injuries), and the assessment of lesions in reconstruction of the accident was examined and discussed.
The review highlights that in motor vehicle accidents involving children, the forensic evaluation of both the cause of death and accident dynamics needs to consider several factors, such as the child’s age, the type of restraint system employed, and the specific passenger seat occupied. Considering the complexity of the factors that can be involved in this road accident, it is crucial that there is a comprehensive exchange of information between the judge and the medical expert.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Road traffic accidents represent a significant public health challenge, imposing substantial economic and social burdens. Despite a reduction in road-related fatalities in developed countries, these accidents continue to contribute to pediatric mortality and morbidities globally [1,2,3,4].
Children involved in car crashes can experience either direct trauma or inertial injuries resulting from interactions with external objects, such as other vehicles, or with the restraint system [5, 6]. Furthermore, improper use of restraint systems can lead to additional severe injuries [7, 8].
The use of restraints, such as car seats and seat belts, must consider the evolving growth and development of the body with age. Infants should be securely buckled in rear-facing car seats, while children aged 9 to 12 no longer require car seats if the seat belt fits them properly and can be worn safely [9,10,11].
Recent reports from international institutions, including the Italian National Institute of Health, the European Road Safety Authority, the National Safety Council Observatory Report, and the Centers for Disease Control and Prevention, have underscored the persistent prevalence of inadequate restraint systems utilization. This widespread issue remains a significant problem, increasing children’s vulnerability and risk of injuries [12,13,14,15].
The complexities inherent in accident dynamics make their reconstruction a challenging task. Typically, the reconstruction of a traffic crash involves interviewing the individuals involved or eyewitnesses, conducting mechanical or engineering examinations, and obtaining recorded images of the accident from digital video sources or event data recorders, but also injuries observed can show distinct and specific characteristics depending on the dynamics of the traffic accident [16,17,18].
A systematic review of studies reporting injuries observed in children involved in motor vehicle accidents was conducted with the aim of describing and analyzing elements that are useful for forensic assessment. This includes features of reported injuries, their role in causing death, and their relevance in reconstructing the dynamics of the accidents.
Materials and methods
An electronic search was performed in 3 databases: PubMed, Scopus, and Web of Science. Keywords related to the study aim and included in the search string were: (car OR motor vehicle) AND (traffic accident OR road traffic OR crash OR prevention) AND (injury OR wound) AND (child OR infant OR pediatric). The Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines were used [19].
The English language and time interval of publication, from January 1970 to March 2023, were applied as filters. All studies that investigate the characteristics of injuries resulting from motor vehicle crashes involving pediatric passengers were included. The following studies were included: (a) studies carried out in the forensic field which involved autopsy of victims; (b) studies performed in clinical settings, involving both living and deceased subjects, from which information on the distribution and production characteristics of injuries could be obtained (c) traffic engineering and public health studies, analysing strategies and technologies for injury prevention in road traffic accidents involving children.
This review did not extract diagnostic or therapeutic implications from the various types of injuries examined.
Titles, abstracts, and full texts were screened for inclusion criteria and examined. References of the selected articles were further screened, and related papers were included as a source of additional data. The following details were collected: authors’ names, article titles, journal names, publication years, article types (such as prospective or retrospective studies, case reports, or original articles), the number of cases, whether the autopsy had been performed and injury localization and mechanism of production.
Results
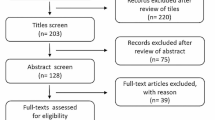
The results of the literature search are summarized in Figure 1. Eighty-six studies met the inclusion criteria and were included in the review. The specific characteristics of each study are summarized in Table 1.

PRISMA flowchart of the present review
A total of 69 studies in the clinical and forensic fields were included in the analysis. Among these, 44 (64%) were retrospective studies, 20 (29%) case reports, 1 (1%) prospective study, and 1 (1%) experimental study. The forensic studies, in which autopsies were carried out, were 20%. The clinical studies, conducted primarily on both living and deceased patients excluding autopsies, were 80% and included the largest number of cases. Abdomen injuries were the most extensively analyzed, appearing in the largest number of studies (50/69), followed by lesions to head (43/69), neck (32/69), chest (37/69), and limbs (13/69). The description of injury features was extracted from each article and thoroughly discussed.
A total of 17 retrospective studies addressing injury prevention strategies and technologies were included.
Discussion
In motor vehicle accidents involving children, injuries can occur in different parts of the body through different mechanisms. Depending on their severity, these injuries may result in the death of the victim and may provide important insights into the dynamics of the accident. The first four paragraphs discuss the characteristics of the injuries, based on a literature review, categorised by the body regions affected (head, neck, thorax-abdomen, and limbs), and the fifth paragraph discusses the evaluation of injury prevention tests and technologies. Given the broad timespan of the literature review (1970–2023), each paragraph shows the chronological arrangement of the cited sources corresponding to the respective topics under discussion.
The final section examines elements critical to forensic assessment, including the role of injuries in causing fatalities and their importance in reconstructing accident dynamics.
Head injuries
Head injuries are identified as the most frequent and fatal consequences of pediatric motor vehicle crashes [3, 7, 9, 36, 52, 59, 67, 70, 76, 78, 92]. The prevailing intracranial lesions observed include cerebral contusions, diffuse axonal damage, subdural or subarachnoid haemorrhage, and basilar skull fracture [59, 76]. Infants are vulnerable to sudden head movements as meningeal bridging veins can be easily stretched and torn leading to subdural haemorrhages. The rupture of those vessels can occur even with minor shaking without substantial contact with any structure or another occupant. On the contrary, in older children, head lesions are often associated with skull fractures and other points of impact within the vehicle [9]. Despite proper restraint usage, children involved in motor vehicle collisions often sustain significant head injuries, and the nature of the trauma reflect the type of restraint [78]. For infants, forward-facing car seat are associated with a higher incidence of skull fractures and intracranial damage [9]. Conversely, rear-facing car safety seats offer optimal support to the head and spine during a crash, as forces are directed from the car safety seat’s back to the infant’s back, which represents their strongest body surface [100]. In older children, typically seated in forward-facing car seat, serious facial or scalp lacerations are more common if lap and shoulder belts were used [9].
The improper use of child car seat systems in the front seat, particularly combined with airbags, favours specific injury patterns, explained by the mechanisms associated with airbag trauma [7]. In the case of infants secured in rear-facing car seat systems in the front seat, the airbag strikes the child restraint system and continues to expand, crushing the child’s head. For older children, braking before impact causes them to shift forward, placing them closer to the dashboard. When the airbag deploys, it impacts the face and frontal cranium, inducing violent hyperextension of the cervical spine and subsequent lesions [32]. The lower body mass of children renders them more vulnerable to minor shifts in body position during airbag deployment, resulting in face thermal lesions, abrasions, facial bone fractures, and, in extreme cases, occipitoatlantoaxial disarticulation [31, 34, 39].
In children, irrespective of the seating position inside the vehicle, head and brain injuries are often linked to the inappropriate use of loosely fitting seat belts, as increased head excursion is favoured by inadequate torso restraint. These lesions occur when the child’s head strikes an object in front of her/him, such as the instrument panel without an airbag or the back of the front seats in rear-seated children. The appropriate use of child restraints can help mitigate such injuries by improving torso support and reducing head excursions [8].
In relation to the child’s position within the vehicle during a crash, head damages are more severe in lateral-impact crashes compared to frontal collisions [52]. Lateral impacts can occur between vehicles, fixed objects, such as a wall or road signs, or in rollovers, and often result in severe and potentially lethal craniocerebral injuries [9]. Children are particularly at risk due to their larger head surface area and lower seated height, likely striking the interior door panel or pillars during side-impact crashes [43].
Concerning the temporal distribution of the articles discussed in this paragraph, those addressing the anatomical features of head injuries have all been published from 2000 onwards [3, 7, 9, 36, 52, 59, 67, 70, 76, 78, 92]. Specifically, articles examining head injuries in relation to the child’s seating position and type of crash impacts date back to 10 years ago [9, 52, 78]. Head injuries resulting from the direct impact of airbags have been documented in articles from both the 1990s [31, 32, 34] and the 2000s [7, 39]. Interestingly, there is no mention of such injuries in articles published within the last two decades.
Neck injuries
In infancy, the cervical spine is the neck region most frequently involved in motor vehicle accidents. Children are particularly vulnerable to cervical spine traumatisms in frontal crashes, in which spine hyperflexion distraction may lead to fractures of cervical vertebrae and brainstem damage [52, 80]. On the other hand, rear impacts can cause whiplash injuries due to hyperextension of the neck and secondary lesions from rebound flexion of the head [5]. Pediatric cervical lesions are more common than in adults due to anatomical differences and distinct damage mechanisms. Infants have a relatively wider and heavier head compared to their body, resulting in a higher centre of gravity and fulcrum of movement in the neck. Therefore, the cause of cervical trauma is rapid acceleration and deceleration. Additionally, centres of vertebral ossification and ligamentous structures are laxer and more fragile in children compared to adults [4]. It has been hypothesized that the location and nature of spinal injuries in children shift as a result of anatomical development during the transition from childhood to adolescence. At children age, the lesions tend to occur at inferior vertebral levels, typically at thoracic location [90].
The correct use of children restraint systems does not fully avoid cervical spine traumas. If the child retained in the car seat is seated in the front passenger seat, airbag deployment during an accident can cause hyperextension of the cervical spine due to facial impact [34, 39, 80]. The action of the shoulder belt during the deceleration phenomena can also damage neck structures, which can be directly hurt, resulting in an oblique abrasion corresponding to the position of the shoulder belt, possibly associated with the rupture of the sternocleidomastoid muscle. In severe trauma, tearing of the common carotid artery, below the sternocleidomastoid muscle, can occur as hyperextension and flexion of the neck compressing the vessel between the seat belt and the vertebral column [97, 101]. Although rare, seatbelt action can transect the trachea [38].
In line with the structure of the paragraph discussing head injuries, articles addressing the anatomical features of head injuries have all been published from 2000 onwards [4, 5, 52, 80, 90]. Neck injuries resulting from the direct impact of airbags have been documented in articles from both the 1990s [31, 32, 34] and the 2000s [7, 39]. Thus, also in this type of injuries, there is no mention of such injuries in articles published within the last two decades.
Chest and abdomen injuries
Thoracoabdominal injuries, such as cardiac, pulmonary, splenic or hepatic ruptures, aortic transection, and spine, ribs, or clavicle fractures, are less frequent compared to other body regions. They are usually caused by impact with motor vehicle structures, like protuberances on the door interior [59, 71].
Specifically, children involved in lateral-impact collisions often suffer severe thorax trauma compared to frontal crashes, with a much higher fatal outcomes for those seated on the impact side [9, 52].
Furthermore, the movement of the seat belt during impact can result in a distinct injury pattern, and children are especially vulnerable due to their physical and behavioural characteristics. Children’s abdominal wall and musculature are less developed than adults, and the costal margin does not extend as far down, and even minor trauma can lacerate the spleen and liver.
During deceleration, a child’s body moves rapidly forward, and the immature pelvis cannot properly anchor the lap portion of the belt. Additionally, children tend to slide forward in the seat, flexing their knees at the seat edge, allowing the lap belt to override the anterior superior iliac spines and ride up over the abdomen. Consequently, the child’s upper torso hyperflexes over the lap belt, inducing a sudden increase in internal pressure due to a direct compression between the belt and the spine favouring organ contusions and lacerations. These are easily produced as children have a smaller anteroposterior diameter. Similarly, the thoracic cage of children is more flexible than adults, and compression can easily result in severe internal injuries not necessarily damaging bony structures [37, 40, 45, 102, 103].
Lesions associated with the three-point belt, known as lap-shoulder belt, often involve the chest, with fractures of the sternum, ribs, and clavicle, in addition to lesions to the heart, lungs, brachial plexus, and aorta [104].
A distinctive pattern of injury is associated with the two-point belt, known as lap belt, which was first noted by Garrett and Braunstein and termed the seat belt syndrome [45]. Blunt trauma can cause a traumatic abdominal wall hernia with disruption of muscle and fascia, even without penetration of the skin [30, 73].
Solid viscera, namely liver, pancreas, and the spleen, can be subjected to lacerations and perforations may occur in hollow structures, such as the intestine and stomach [24, 37, 93, 97].
The jejunum is the most common site of small intestine involvement, especially around the ligament of Treitz, where fixation promotes shear stress tears. Another vulnerable fixed site is the ileocecal valve [105].
Although rare, seat belt-related abdominal blunt trauma can lead to aortic injuries such as dissection, rupture, thrombosis, or intimal tears [20, 93, 97]. These lesions are related to forces crushing the vessel between the vertebral column and the seat belt. Additionally, elongation of the aorta from the pressure of the decelerating column of blood and changes in intraluminal pressure may exacerbate the damage [106].
In cases of severe trauma, spine fractures or dislocations can be observed, particularly involving the first and second lumbar vertebrae [21, 37, 54, 93, 97]. Chance fractures, a type of compression injury to the lumbar spine, can also be detected. These fractures consist of rupture of the posterior ligaments and fractures of the spinous process, pedicles, and vertebral bodies. The unique characteristic of the Chance fracture is that the fracture line extends transversely through the spinous process, laminae, transverse processes, pedicles, and into the superior surface of the vertebral body [26, 107].
Concerning the temporal distribution of the articles discussed in this paragraph, all articles covered the range from the 1970s up to the last 10 years, with references uniformly distributed across all the topics addressed. The only topic exclusively covered by sources from the 1990s is the Chance fracture [26, 107].
Limb injuries
Lower extremity injuries are more prevalent, predominantly involving fractures of the femur, pelvis, and patella [76]. Frontal collisions occur when a vehicle abruptly decelerates upon colliding with another vehicle or a stationary object. Consequently, the impact forces are transmitted through the lower limbs of the front-seat occupants, affecting the knee-thigh-hip complex, with the hip joint being particularly susceptible to fractures or dislocations. Conversely, back seat occupants frequently exert force on the front seat using their extended upper limbs, with consequent fractures [9]. If children were secured using forward-facing child car seat systems, injuries below the knee, specifically affecting the tibia or fibula, are notably common. These lesions mainly result from collisions with the vehicle seatback positioned in front of the child’s seating area. Although these bone injuries are typical of frontal impacts, seatback interactions can occur in various other types of crashes [56].
Upper extremity injuries include fractures to the metacarpus, ulna, and radius [76]. These lesions occur in children seated in the front seat due to the action of the airbag compressing the region of the arms, neck, and face. For rear seat occupants, the extended upper limbs may be pushed against the front seat during the deceleration phase typical of frontal collisions [5, 37].
All articles discussed in this paragraph were published within the last 20 and 10 years, spanning from 2001 to 2017 [9, 37, 56, 76].
Injury prevention strategies and technologies
In the last two decades, there has been increasing attention on the development of behavioural and technological prevention strategies to reduce the risk of death or severe injuries in children involved in motor vehicle accidents.
The primary injury prevention strategy highlighted in recent years is the use of child restraint systems. This is not limited to very young children, as studies have shown that children aged 2 through 6 years in child restraint systems experience a 21% reduction in mortality risk compared to those in seat belts alone. Child restraint systems offer significant safety advantages due to biomechanical considerations. They are designed to minimize the risk of ejection during a crash, distribute crash forces through stronger bones, limit crash forces by extending deceleration time, and potentially reduce contact with intruding vehicle structures. Child restraint systems also provide a better fit for restraints in children too small for adult-sized seat belts, offering a mechanical protection advantage [44].
Moreover, the positioning of child restraints on the seat has been observed to have an impact. In frontal motor vehicle crashes, pediatric models in rear-facing configurations generally show lower injury numbers than those in forward configurations, especially recommended up to at least 2 or 4 years of age. This is associated with a better support to the neck and the head, preventing rotational motion of the head [85, 91].
As children grow taller and older, they have a better chance of achieving a good seat belt fit. However, seat belt fit can be influenced by factors such as seat geometry and the locations of seat belt anchorages, independent of the occupant’s height and weight [98]. To optimize the transition from child restraint to seat belt use, the use of booster seats is recommended. Booster seats raise a child to the correct position, and data shows that children aged 6–8 using boosters are less likely to be injured compared to those using vehicle seat belts alone. Boosters adapt the child’s height to the vehicle restraint system, allowing comfortable knee bending and preventing a slouching sitting posture. Optimal protection is achieved when the pelvic bones are tightly coupled early and maintained throughout the event [44, 69, 85, 94].
Regarding seat position, it is strongly recommended to seat the child in the rear seat of the car. Even if the car is equipped with advanced front seat safety systems, including second-generation and modern airbags, it is recommended that all children aged 0–12 years should be seated in the rear rows. In cases of frontal or rear-end crashes, being in the front seat more than doubles the risk of fatality and being unrestrained increases fatality risk fourfold. For teenagers aged 13 and above, the reduction in injuries is not statistically significant, but it is suggested that young teenagers may benefit from rear seating similarly to their preteen counterparts [51, 60, 66].
To facilitate the storage and management of all this information, smartphone apps have been created to communicate child passenger safety. With the increasing interest in mobile health, the use of smartphone apps is considered rational for addressing health problems [84].
Injury prevention technologies have been devised to mitigate injuries in near-side impacts, which carry a high risk of severe or even fatal injuries. In these cases, the principal mechanism of injury is contact with the vehicle interior, mainly associated with intrusion into the occupant compartment at the child’s position, combined with lateral translation of the child’s body. The development of side airbags that protect the head and thorax reduces injury measurements, provided that the airbag properties are designed to consider these occupant sizes [72]. The use of side airbags limits the probability of serious head and trunk injuries, confining them to upper extremity fractures and concussions with brief loss of consciousness [66].
Moreover, air-bag technology has improved with the development of ‘smarter air bags’, with features that include sensors that can identify young passengers based on weight, and child restraint devices with on/off switches [7, 87].
All the articles discussed in this paragraph were uniformly published after the 2000s, with a clear division between those published before 2010 [44, 47, 51, 53, 57, 58, 60, 63, 66] and those published in the subsequent years, extending up to the most recent publications [69, 72, 84, 85, 88, 91, 94, 98].
Forensic evaluation of injury patterns based on accident dynamics
The previous paragraphs have analyzed the primary injuries that may result from road traffic crashes involving children, along with an analysis of prevention strategies and technologies to mitigate them.
The evaluation of the temporal distribution of the various reports allows some considerations. First, articles assessing different injuries have been published throughout the whole timeframe covered by the review (1970–2023), with some peculiarities later discussed. On the other hand, papers on preventive measures are distributed in the last 20 years, in accordance with prevention awareness and the development of new technologies.
In-depth analysis of the temporal trends of head and neck injuries due to airbag direct impact has revealed a significant reduced reporting since the 2000s. This lower incidence can be explained as the application of the prevention strategy to place children in rear seats until their appropriate age.
On the other hand, head lesions associated with lateral impact and chest, abdominal and limb injuries are throughout reported along the entire period covered by the review. As a matter of fact, these lesions typically occur in high-speed road accidents, both lateral and frontal, in which the development of appropriate protective measures, as the integration of side airbags, remains a challenge in the field of engineering.
Analysis of injury patterns provides valuable information about accident dynamics and the type of crash in which children have been involved.
In motor vehicle accidents, child’s injuries can result from direct contact between the body and the internal components of the vehicle. This is particularly prominent in cases of vehicle rollovers and lateral impacts with other vehicles or stationary objects, such as poles and walls. On the other hand, acceleration and deceleration forces experienced in frontal and rear-end collisions can cause injuries through an indirect mechanism involving tissue stretching. In both dynamic scenarios, the primary cause of death is neurogenic shock. This can occur as a result of a direct impact to the head, leading to skull fractures, subdural haemorrhages, and cerebral contusions [3, 9, 59, 76, 92]. The indirect effects of acceleration-deceleration forces result in compressive and shear stresses on the brain and medulla, leading to subdural haemorrhages due to the rupture of meningeal bridging veins [9, 52, 59, 76, 80]. Although this dynamic is not directly related to skull fractures, it can be inferred from the presence of vertebral fractures [52, 80].
In the reported articles, children were correctly restrained in accordance with the specific requirements for their age. This suggests that the correct application of child protective equipment is not sufficient to prevent head injuries, especially in cases of high speed or multiple impacts. Moreover, the use of safety devices such as seat belts can also lead to injuries due to the direct impact of the belt on the body during a collision.
When using a lap-shoulder belt, injuries may include damage to neck and thoracic structures, resulting in sternum, rib, and clavicle fractures, as well as cardiac and aortic lesions [38, 97, 101, 104]. Alternatively, if the child is secured with a lap belt, this can lead to intra-abdominal injuries such as organ lacerations or perforations and aortic dissection [20, 24, 37, 93, 97]. The damages from the seat belt’s action are a result of the pressure exerted on the child’s body, in which muscle and bone structures are not fully developed yet. In such cases, an oblique or transverse abrasion corresponding to the seat belt position is typically observable during external examination.
However, during on-site inspections and the assessment of circumstantial data, it’s crucial to consider that specific injuries can also occur due to the improper use of child safety restraint systems.
The improper use of seat belts that do not correctly accommodate the infant’s body, leading to inadequate torso restraint, raises the risk of increased head movement and a higher likelihood of severe brain injury [8].
Improper placement of car restraints in the front seat can lead to injuries specifically related to airbag action during impact. In fact, standard guidelines for child restraints are based upon age and size. As a child ages, seating progresses to a forward-facing child safety seat to a belt-positioning booster seat with a three-point seat belt. In infants placed in forward-facing car seats, the deployment of airbags can result in facial compression, leading to facial bone and cervical spine fractures due to severe traumatic hyperextension [34, 39, 80]. External examinations may reveal facial thermal lesions or abrasions caused by contact with the airbag. Conversely, for infants positioned in rear-facing car seats, airbag deployment can lead to the child’s head being compressed between the restraint and the upright back of the passenger seat, resulting in skull fractures and brain contusions [32].
The forensic evaluation of injury patterns requires a comprehensive assessment of the child position in the vehicle at the time of the accident, in order to reconstruct the overall dynamics. The specific seat occupied by the child, the type of restraint used, and the adequacy of the restraint in relation to the child’s anthropometric characteristics should be carefully evaluated.
In a medicolegal context, a comprehensive assessment of the cause of injury resulting from a traffic crash requires expertise from multiple disciplines. Traffic crash reconstruction and engineering techniques are employed to evaluate the severity and direction of vehicle forces. Moreover, engineers test the proper functioning of protective devices such as child restraints, air bags, and seat belts. Medical-legal expertise is needed to understand the nature of collision-related injuries and their subsequent developments in non-fatal accidents. Biomechanical methods provide the connection between medically documented injuries and the reconstructed crash forces, and epidemiological approaches are used to properly classify and describe the crash and its outcomes in comparison to similar collisions. In litigation related to traffic accidents, the process of determining the degree to which safety restraint systems non-use contributed to the risk of injury or death is based on a comprehensive analysis of biomechanical, medical, and epidemiological factors [108].
Considering the complexity of the factors that can be involved in this road accident, it is crucial that there is a comprehensive exchange of information between the judge and the medical expert. This should include all relevant circumstantial elements, such as testimonies, accident videos, and kinematic engineering data related to car damage, skid marks, and proper use of safety devices.
Conclusion
The review highlights that in motor vehicle accidents involving children, the forensic evaluation of both the cause of death and accident dynamics needs to consider several factors, such as the child’s age, the type of restraint system employed, and the specific passenger seat occupied. While brain damages remain the most frequently fatal across all age groups, certain specific injuries are linked to the restraint systems or airbag deployment.
When the accident dynamics are known, awareness of the distinct injury patterns can support forensic evaluation of sequence of events. Conversely, when the child location cannot be assumed, such as in case of multiple rollovers, the injuries patterns can provide useful information for the events reconstruction.
Data availability
The data presented in this study are available on request from the corresponding author.
References
Winston FK, Chen IG, Elliott MR, Arbogast KB, Durbin DR (2004) Recent trends in child restraint practices in the United States. Pediatrics 113(5):e458–e464. https://doi.org/10.1542/peds.113.5.e458
Cunningham RM, Walton MA, Carter PM (2018) The major causes of death in children and adolescents in the United States. The New England J Med 379(25):2468–2475. https://doi.org/10.1056/NEJMsr1804754
Takahashi H, Fujita T, Nakahara S, Sakamoto T (2018) Seating position and patterns of severely injured body parts among child passengers in motor vehicle crashes: Japan as a distinct case. Int J Injury Ctrl Safety Promot 25(4):427–432. https://doi.org/10.1080/17457300.2018.1456469
Platzer P, Jaindl M, Thalhammer G, Dittrich S, Kutscha-Lissberg F, Vecsei V, Gaebler C (2007) Cervical spine injuries in pediatric patients. The J Trauma 62(2):389–396. https://doi.org/10.1097/01.ta.0000221802.83549.46
Eid HO, Abu-Zidan FM (2007) Biomechanics of road traffic collision injuries: a clinician's perspective. Singapore Med J 48(7):693–700
Arbogast KB, Wozniak S, Locey CM, Maltese MR, Zonfrillo MR (2012) Head impact contact points for restrained child occupants. Traffic Injury Prevent 13(2):172–181. https://doi.org/10.1080/15389588.2011.642834
Quiñones-Hinojosa A, Jun P, Manley GT, Knudson MM, Gupta N (2005) Airbag deployment and improperly restrained children: a lethal combination. J Trauma 59(3):729–733
Arbogast KB, Durbin DR, Kallan MJ, Menon RA, Lincoln AE, Winston FK (2002) The role of restraint and seat position in pediatric facial fractures. J Trauma 52(4):693–698. https://doi.org/10.1097/00005373-200204000-00014
Huelke DF (1998) An overview of anatomical considerations of infants and children in the adult world of automobile safety design. Annu Proc Assoc Adv Automot Med 42:93–113
Centers for Disease Control and Prevention (2022) Motor vehicle crashes: a leading cause of death for children. https://www.cdc.gov/transportationsafety/child_passenger_safety/cps-factsheet.html. Accessed 29 June 2023.
National Highway Traffic Safety Administration. Car seats and booster seats. https://www.nhtsa.gov/equipment/car-seats-and-booster-seats. Accessed 23 May 2023.
European Road Safety Observatory (2022) Road safety thematic report – seat belt and child restraint systems. https://road-safety.transport.ec.europa.eu/system/files/2022-01/Road%20Safety%20Thematic%20Report%20-%20Seat%20belt%20and%20child%20restraint%20systems.pdf. Accessed 23 May 2023.
Istituto Superiore di Sanità (2023) Sorveglianza Passi: il 36% degli italiani usa la cintura posteriore, no seggiolino per 2 su 10. https://www.iss.it/en/news/-/asset_publisher/gJ3hFqMQsykM/content/id/9088071. Accessed 27 October 2023.
National safety Council (2023) Child Restraint. https://injuryfacts.nsc.org/motor-vehicle/occupant-protection/child-restraint/. Accessed 27 October 2023.
Centers for Disease Control and Prevention (2023) Child passenger safety: get the facts. https://www.cdc.gov/transportationsafety/child_passenger_safety/cps-factsheet.html#:~:text=Restraint%20status%20was%20known%20for,226%20(36%25)%20were%20unrestrained. Accessed 27 October 2023.
Bolliger MJ, Buck U, Thali MJ, Bolliger SA (2012) Reconstruction and 3D visualisation based on objective real 3D based documentation. Forensic Sci Med Pathol 8(3):208–217. https://doi.org/10.1007/s12024-011-9288-8
Naude C, Serre T, Dubois-Lounis M, Fournier JY, Lechner D, Guilbot M, Ledoux V (2019) Acquisition and analysis of road incidents based on vehicle dynamics. Accid Anal Prev 130:117–124. https://doi.org/10.1016/j.aap.2017.02.021
Giovannini E, Giorgetti A, Pelletti G, Giusti A, Garagnani M, Pascali JP, Pelotti S, Fais P (2021) Importance of dashboard camera (Dash Cam) analysis in fatal vehicle-pedestrian crash reconstruction. Forensic Sci Med Pathol 17(3):379–387. https://doi.org/10.1007/s12024-021-00382-0
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–W64. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
Dajee H, Richardson IW, Iype MO (1979) Seat belt aorta: acute dissection and thrombosis of the abdominal aorta. Surgery 85(3):263–267
Newman KD, Bowman LM, Eichelberger MR, Gotschall CS, Taylor GA, Johnson DL, Thomas M (1990) The lap belt complex: intestinal and lumbar spine injury in children. J Trauma 30(9):1133–1140
Johnson DL, Falci S (1990) The diagnosis and treatment of pediatric lumbar spine injuries caused by rear seat lap belts. Neurosurgery 26(3):434–441. https://doi.org/10.1097/00006123-199003000-00010
Sivit CJ, Taylor GA, Newman KD, Bulas DI, Gotschall CS, Wright CJ, Eichelberger MR (1991) Safety-belt injuries in children with lap-belt ecchymosis: CT findings in 61 patients. AJR. Am J Roentgenol 157(1):111–114. https://doi.org/10.2214/ajr.157.1.2048507
Statter MB, Coran AG (1992) Appendiceal transection in a child associated with a lap belt restraint: case report. J Trauma 33(5):765–766. https://doi.org/10.1097/00005373-199211000-00029
Tso EL, Beaver BL, Haller JA Jr (1993) Abdominal injuries in restrained pediatric passengers. J Pediatr Surg 28(7):915–919. https://doi.org/10.1016/0022-3468(93)90696-i
Sturm PF, Glass RB, Sivit CJ, Eichelberger MR (1995) Lumbar compression fractures secondary to lap-belt use in children. J Pediatr Orthop 15(4):521–523. https://doi.org/10.1097/01241398-199507000-00022
From the Centers for Disease Control and Prevention (1995) Air-bag-associated fatal injuries to infants and children riding in front passenger seats--United States. JAMA 274(22):1752–1753
Kimmins MH, Poenaru D, Kamal I (1996) Traumatic gastric transection: a case report. J Pediatr Surg 31(6):757–758. https://doi.org/10.1016/s0022-3468(96)90124-4
Smith MD 2nd, Camp E 3rd, James H, Kelley HG (1997) Pediatric seat belt injuries. Am Surgeon 63(3):294–298
Levine JL, Faries PL, Weinberg G (1998) Seat belt injury presenting as bilateral abdominal wall herniations in a child. Pediatr Emergency Care 14(5):352–353
Cooper JT, Balding LE, Jordan FB (1998) Airbag mediated death of a two-year-old child wearing a shoulder/lap belt. J Forensic Sci 43(5):1077–1081
Marshall KW, Koch BL, Egelhoff JC (1998) Air bag-related deaths and serious injuries in children: injury patterns and imaging findings. AJNR. Am J Neuroradiol 19(9):1599–1607
Giguère JF, St-Vil D, Turmel A, Di Lorenzo M, Pothel C, Manseau S, Mercier C (1998) Airbags and children: a spectrum of C-spine injuries. J Pediatr Surg 33(6):811–816. https://doi.org/10.1016/s0022-3468(98)90648-0
Morrison AL, Chute D, Radentz S, Golle M, Troncoso JC, Smialek JE (1998) Air bag-associated injury to a child in the front passenger seat. Am J Forensic Med Pathol 19(3):218–222. https://doi.org/10.1097/00000433-199809000-00003
DeCou JM, Abrams RS, Gauderer MW (1999) Seat-belt transection of the pararenal vena cava in a 5-year-old child: survival with caval ligation. J Pediatr Surg 34(7):1074–1076. https://doi.org/10.1016/s0022-3468(99)90568-7
Tyroch AH, Kaups KL, Sue LP, O'Donnell-Nicol S (2000) Pediatric restraint use in motor vehicle collisions: reduction of deaths without contribution to injury. Arch Surg 135(10):1173–1176. https://doi.org/10.1001/archsurg.135.10.1173
Durbin DR, Arbogast KB, Moll EK (2001) Seat belt syndrome in children: a case report and review of the literature. Pediatr Emergency Care 17(6):474–477. https://doi.org/10.1097/00006565-200112000-00021
Uemura K, Yoshida K (2001) Seat belt induced transection of the trachea in a child on the lap of an adult. J Forensic Sci 46(3):714–716
Lapner PC, McKay M, Howard A, Gardner B, German A, Letts M (2001) Children in crashes: mechanisms of injury and restraint systems. Can J Surg 44(6):445–449
Durbin DR, Kallan M, Elliott M, Arbogast KB, Cornejo RA, Winston FK (2002) Risk of injury to restrained children from passenger airbags. Annual proceedings. Assoc Adv Automotive Med 46:15–25
Nichol PF, Helin M, Zdeblick TA, Hardy SP, Lund DP (2002) Traumatic near-hemicorpectomy caused by a seat belt injury in an 11-year-old girl. J Trauma 53(4):777–779. https://doi.org/10.1097/00005373-200210000-00027
Bockholdt B, Schneider V (2003) The injury pattern to children involved in lethal traffic accidents in Berlin. Legal Med 5(Suppl 1):S390–S392. https://doi.org/10.1016/s1344-6223(02)00139-6
Orzechowski KM, Edgerton EA, Bulas DI, McLaughlin PM, Eichelberger MR (2003) Patterns of injury to restrained children in side impact motor vehicle crashes: the side impact syndrome. J Trauma 54(6):1094–1101. https://doi.org/10.1097/01.TA.0000067288.11456.98
Ebel BE, Koepsell TD, Bennett EE, Rivara FP (2003) Too small for a seatbelt: predictors of booster seat use by child passengers. Pediatrics 111(4 Pt 1):e323–e327. https://doi.org/10.1542/peds.111.4.e323
Prince JS, LoSasso BE, Senac MO Jr (2004) Unusual seat-belt injuries in children. J Trauma 56(2):420–427. https://doi.org/10.1097/01.TA.0000113256.49300.2B
Davies KL (2004) Buckled-up children: understanding the mechanism, injuries, management, and prevention of seat belt related injuries. J Trauma Nursing 11(1):16–24. https://doi.org/10.1097/00043860-200411010-00004
Durbin DR, Chen I, Smith R, Elliott MR, Winston FK (2005) Effects of seating position and appropriate restraint use on the risk of injury to children in motor vehicle crashes. Pediatrics 115(3):e305–e309. https://doi.org/10.1542/peds.2004-1522
Santschi M, Echavé V, Laflamme S, McFadden N, Cyr C (2005) Seat-belt injuries in children involved in motor vehicle crashes. Can J Surg 48(5):373–376
Centers for Disease Control and Prevention (CDC) (2005) Nonfatal motor-vehicle-related backover injuries among children--United States, 2001-2003. MMWR 54(6):144–146
Newgard CD, Lewis RJ (2005) Effects of child age and body size on serious injury from passenger air-bag presence in motor vehicle crashes. Pediatrics 115(6):1579–1585. https://doi.org/10.1542/peds.2004-0555
Arbogast KB, Durbin DR, Kallan MJ, Elliott MR, Winston FK (2005) Injury risk to restrained children exposed to deployed first- and second-generation air bags in frontal crashes. Arch Pediatr Adolesc Med 159(4):342–346. https://doi.org/10.1001/archpedi.159.4.342
Brown JK, Jing Y, Wang S, Ehrlich PF (2006) Patterns of severe injury in pediatric car crash victims: Crash Injury Research Engineering Network database. J Pediatr Surg 41(2):362–367. https://doi.org/10.1016/j.jpedsurg.2005.11.014
Elliott MR, Kallan MJ, Durbin DR, Winston FK (2006) Effectiveness of child safety seats vs seat belts in reducing risk for death in children in passenger vehicle crashes. Arch Pediatr Adolesc Med 160(6):617–621. https://doi.org/10.1001/archpedi.160.6.617
Papavasiliou A, Stanton J, Sinha P, Forder J, Skyrme A (2007) The complexity of seat belt injuries including spinal injury in the pediatric population: a case report of a 6-year-old boy and the literature review. Eur J Emergency Med 14(3):180–183. https://doi.org/10.1097/MEJ.0b013e32801430e2
Achildi O, Betz RR, Grewal H (2007) Lapbelt injuries and the seatbelt syndrome in pediatric spinal cord injury. J Spinal Cord Med 30(Suppl 1(Suppl 1)):S21–S24. https://doi.org/10.1080/10790268.2007.11753964
Jermakian JS, Locey CM, Haughey LJ, Arbogast KB (2007) Lower extremity injuries in children seated in forward facing child restraint systems. Traffic Injury Prevent 8(2):171–179. https://doi.org/10.1080/15389580601175250
Zaloshnja E, Miller TR, Hendrie D (2007) Effectiveness of child safety seats vs safety belts for children aged 2 to 3 years. Arch Pediatr Adolesc Med 161(1):65–68. https://doi.org/10.1001/archpedi.161.1.65
Arbogast KB, Kallan MJ (2007) The exposure of children to deploying side air bags: an initial field assessment. Annu Proc Assoc Adv Automot Med 51:245–259
Maltese MR, Locey CM, Jermakian JS, Nance ML, Arbogast KB (2007) Injury causation scenarios in belt-restrained nearside child occupants. Stapp Car Crash J 51:299–311. https://doi.org/10.4271/2007-22-0013
Lennon A, Siskind V, Haworth N (2008) Rear seat safer: seating position, restraint use and injuries in children in traffic crashes in Victoria, Australia. Accid Anal Prev 40(2):829–834. https://doi.org/10.1016/j.aap.2007.09.024
Santschi M, Lemoine C, Cyr C (2008) The spectrum of seat belt syndrome among Canadian children: results of a two-year population surveillance study. Paediatr Child Health 13(4):279–283. https://doi.org/10.1093/pch/13.4.279
García-España JF, Durbin DR (2008) Injuries to belted older children in motor vehicle crashes. Accid Anal Prev 40(6):2024–2028. https://doi.org/10.1016/j.aap.2008.08.018
O'Neil J, Daniels DM, Talty JL, Bull MJ (2009) Seat belt misuse among children transported in belt-positioning booster seats. Accid Anal Prev 41(3):425–429. https://doi.org/10.1016/j.aap.2009.01.003
Clarke DD, Ward P, Bartle C, Truman W (2010) Killer crashes: fatal road traffic accidents in the UK. Accid Anal Prev 42(2):764–770. https://doi.org/10.1016/j.aap.2009.11.008
Brown J, Bilston LE (2009) Spinal injury in motor vehicle crashes: elevated risk persists up to 12 years of age. Arch Dis Child 94(7):546–548. https://doi.org/10.1136/adc.2008.138818
Arbogast KB, Kallan MJ, Durbin DR (2009) Front versus rear seat injury risk for child passengers: evaluation of newer model year vehicles. Traffic Inj Prev 10(3):297–301. https://doi.org/10.1080/15389580802677799
Arbogast KB, Locey CM, Zonfrillo MR, Maltese MR (2010) Protection of children restrained in child safety seats in side impact crashes. J Trauma 69(4):913–923. https://doi.org/10.1097/TA.0b013e3181e883f9
Soundappan SS, Holland A, Lam L, Roy G, Evans JB, Adams S, Cass DT (2010) Off-road vehicle trauma in children: a New South Wales perspective. Pediatr Emergency Care 26(12):909–913. https://doi.org/10.1097/PEC.0b013e3181ff0d11
Barraco RD, Cheng JD, Bromberg WJ, Falcone RA, Hammond JS, Lui FY, Sandhu RS, Scaff DW (2010) Child passenger safety workgroup of the EAST Practice Management Guideline Committee. Child passenger safety: an evidence-based review. J Trauma 69(6):1588–1590. https://doi.org/10.1097/TA.0b013e3181fbc69c
Skjerven-Martinsen M, Naess PA, Hansen TB, Rognum TO, Lereim I, Stray-Pedersen A (2011) In-depth evaluation of real-world car collisions: fatal and severe injuries in children are predominantly caused by restraint errors and unstrapped cargo. Traffic Injur Prevent 12(5):491–499. https://doi.org/10.1080/15389588.2011.596868
Töro K, Szilvia F, György D, Pauliukevicius A, Caplinskiene M, Raudys R, Lepik D, Tuusov J, Vali M (2011) Fatal traffic injuries among children and adolescents in three cities (capital Budapest, Vilnius, and Tallinn). J Forensic Sci 56(3):617–620. https://doi.org/10.1111/j.1556-4029.2010.01674.x
Andersson M, Pipkorn B, Lövsund P (2012) Parameter study for child injury mitigation in near-side impacts through FE simulations. Traffic Inj Prev 13(2):182–192. https://doi.org/10.1080/15389588.2011.637411
Moremen JR, Nakayama DK, Ashley DW, Astin M, Nolan TL (2013) Traumatic disruption of the abdominal wall: lap-belt injuries in children. J Pediatr Surg 48(4):e21–e24. https://doi.org/10.1016/j.jpedsurg.2013.02.039
Charyk Stewart T, McClafferty K, Shkrum M, Comeau JL, Gilliland J, Fraser DD (2013) A comparison of injuries, crashes, and outcomes for pediatric rear occupants in traffic motor vehicle collisions. J Trauma Acute Care Surg 74(2):628–633. https://doi.org/10.1097/TA.0b013e31827d606c
Viklund Å, Björnstig J, Larsson M, Björnstig U (2013) Car crash fatalities associated with fire in Sweden. Traffic Injur Prevent 14(8):823–827. https://doi.org/10.1080/15389588.2013.777956
Belwadi AN, Locey CM, Hullfish TJ, Maltese MR, Arbogast KB (2014) Pediatric occupant-vehicle contact maps in rollover motor vehicle crashes. Traffic Injur Prevent 15(Suppl 1):S35–S41. https://doi.org/10.1080/15389588.2014.937485
Zonfrillo MR, Locey CM, Scarfone SR, Arbogast KB (2014) Motor vehicle crash-related injury causation scenarios for spinal injuries in restrained children and adolescents. Traffic Injur Prevent 15(Suppl 1(Suppl 1)):S49–S55. https://doi.org/10.1080/15389588.2014.934959
Stewart CL, Moscariello MA, Hansen KW, Moulton SL (2014) Infant car safety seats and risk of head injury. J Pediatr Surg 49(1):193–197. https://doi.org/10.1016/j.jpedsurg.2013.09.054
Papazoglou KO, Karkos CD, Kalogirou TE, Giagtzidis IT (2015) Endovascular management of lap belt-related abdominal aortic injury in a 9-year-old child. Ann Vasc Surg 29(2):365.e11–365.e3.65E15. https://doi.org/10.1016/j.avsg.2014.09.026
Terranova C (2015) The medico-legal aspects of road traffic deaths in children under 5 years of age. J Forensic Leg Med 36:160–163. https://doi.org/10.1016/j.jflm.2015.09.018
Parrish DW, Barnhorst A, Trebska-McGowan K, Amendola M, Haynes JH (2015) Nonoperative management of pediatric aortic injury with seat belt syndrome. Ann Vasc Surg 29(6):1316.e1–1316.e13166. https://doi.org/10.1016/j.avsg.2015.02.019
Yunus SS, Ngeow WC, Ramli R (2015) Pediatric craniomaxillofacial injuries after road traffic crashes: characteristics of injuries and protective equipment use. Am J Emerg Med 33(9):1253–1257. https://doi.org/10.1016/j.ajem.2015.05.009
Mitchell RJ, Bambach MR, Toson B (2015) Injury risk for matched front and rear seat car passengers by injury severity and crash type: an exploratory study. Accid Anal Prev 82:171–179. https://doi.org/10.1016/j.aap.2015.05.023
Gielen AC, McDonald EM, Omaki E, Shields W, Case J, Aitken M (2015) A smartphone app to communicate child passenger safety: an application of theory to practice. Health Educ Res 30(5):683–692. https://doi.org/10.1093/her/cyv035
Weatherwax M, Coddington J, Ahmed A, Richards EA (2016) Child passenger safety policy and guidelines: why change is imperative. J Pediatr Health Care 30(2):160–164. https://doi.org/10.1016/j.pedhc.2015.09.006
Meral O, Aktaş EÖ, Ersel M (2018) Examination of morbidity and mortality of cases according to intra-vehicle position and accident mechanism. Turkish J Trauma Emergency Surg 24(3):216–223. https://doi.org/10.5505/tjtes.2017.34662
O'Donovan S, van den Huevel C, Baldock M, Byard RW (2018) Factors involved in the assessment of paediatric traffic injuries and deaths. Med Sci Law 58(4):210–215. https://doi.org/10.1177/0025802418790857
Davis NL, Shah N (2018) Use of car beds for infant travel: a review of the literature. J Perinatol 38(10):1287–1294. https://doi.org/10.1038/s41372-018-0195-7
Savenkova EN, Efimov AA (2019) Vliianie nekotorykh faktorov na osobennosti povrezhdeniĭ, voznikaiushchikh v usloviiakh avtomobil'noĭ travmy u deteĭ-passazhirov [The influence of certain factors on the specific features of the injuries inflicted to the children involved in the motor vehicle traffic accidents]. Sud Med Ekspert 62(1):4–7. https://doi.org/10.17116/sudmed2019620114
Mallory A, Stammen J, Zhu M (2019) Cervical and thoracic spine injury in pediatric motor vehicle crash passengers. Traffic Injur Prevent 20(1):84–92. https://doi.org/10.1080/15389588.2018.1529412
Belwadi A, Sarfare S, Tushak S, Maheshwari J, Menon S (2019) Responses of the scaled pediatric human body model in the rear- and forward-facing child seats in simulated frontal motor vehicle crashes. Traffic Inj Prev 20(sup2):S143–S144. https://doi.org/10.1080/15389588.2019.1661684
Alghnam S, Jastaniah E, Alwahaibi W, Albabtain IT, Alqublan S, Bajwaiber M, Alzahrani S, Alghamdi A (2020) The prevalence of head and facial injuries among children in Saudi Arabia following road traffic crashes. Ann Saudi Med 40(5):417–424. https://doi.org/10.5144/0256-4947.2020.417
Jammeh ML, Ohman JW, Reed NR, English SJ, Jim J, Geraghty PJ (2020) Management of seat belt-type blunt abdominal aortic trauma and associated injuries in pediatric patients. Ann Vasc Surg 69:447.e9–447.e16. https://doi.org/10.1016/j.avsg.2020.07.024
Bohman K, Östh J, Jakobsson L, Stockman I, Wimmerstedt M, Wallin H (2020) Booster cushion design effects on child occupant kinematics and loading assessed using the PIPER 6-year-old HBM and the Q10 ATD in frontal impacts. Traffic Inj Prev 12(21(sup1)):S25–S30. https://doi.org/10.1080/15389588.2020.1795148
Sarwahi V, Atlas AM, Galina J, Satin A, Dowling TJ 3rd, Hasan S, Amaral TD, Lo Y, Christopherson N, Prince J (2021) Seatbelts save lives, and spines, in motor vehicle accidents: a review of the National Trauma Data Bank in the pediatric population. Spine 46(23):1637–1644. https://doi.org/10.1097/BRS.0000000000004072
Laureano ICC, Palitot TFT, Cavalcanti AFC, Cavalcanti AL (2021) Craniofacial trauma in Brazilian child victims of traffic accidents: a single-trauma center analysis. Dental Med Problems 58(4):441–445. https://doi.org/10.17219/dmp/127668
Riches KJ, James RA, Gilbert JD, Byard RW (2002) Fatal childhood vascular injuries associated with seat belt use. Am J Forensic Med Pathol 23(1):45–47. https://doi.org/10.1097/00000433-200203000-00009
Parab A, Whyte T, Albanese B, Bilston L, Koppel S, Charlton JL, Olivier J, Keay L, Brown J (2022) Can age or height define appropriate thresholds for transition to adult seat belts? An analysis of observed seat belt fit in children aged 7-12 years. Int J Environ Res Public Health 19(3):1524. https://doi.org/10.3390/ijerph19031524
Spering C, Müller G, Füzesi L, Bouillon B, Rüther H, Lehmann W, Lefering R, Section of Injury Prevention DGOU, & and TraumaRegister DGU (2022) Prevention of severe injuries of child passengers in motor vehicle accidents: is re-boarding sufficient? Eur J Trauma Emerg Surg 48(5):3989–3996. https://doi.org/10.1007/s00068-022-01917-y
Weber K (2000) Crash protection for child passengers. UMTRI Res Rev 31(3):1
McConnell EJ, Macbeth GA (1997) Common carotid artery and tracheal injury from shoulder strap seat belt. J Trauma 43(1):150–152. https://doi.org/10.1097/00005373-199707000-00038
Tepas JJ (1996) Pediatric trauma. Appleton & Lange, pp 879–898
Asbun HJ, Irani H, Roe EJ, Bloch JH (1990) Intra-abdominal seatbelt injury. J Trauma 30(2):189–193
May AK, Chan B, Daniel TM, Young JS (1995) Anterior lung herniation: another aspect of the seatbelt syndrome. J Trauma 38(4):587–589. https://doi.org/10.1097/00005373-199504000-00021
Bruny JL, Bensard DD (2004) Hollow viscous injury in the pediatric patient. Sem Pediatr Surg 13(2):112–118. https://doi.org/10.1053/j.sempedsurg.2004.01.007
Freni L, Barbetta I, Mazzaccaro D, Settembrini AM, Dallatana R, Tassinari L, Settembrini PG (2013) Seat belt injuries of the abdominal aorta in adults--case report and literature review. Vasc Endovasc Surg 47(2):138–147. https://doi.org/10.1177/1538574412469446
Chance GQ (1948) Note on a type of flexion fracture of the spine. British J Radiol 21(249):452. https://doi.org/10.1259/0007-1285-21-249-452
Freeman MD (2021) Principles and methods for evidence-based quantification of the effect of seat belt non-use in crash-related litigation. Int JEnviron Res Public Health 18(18):9455. https://doi.org/10.3390/ijerph18189455
Funding
Open access funding provided by Alma Mater Studiorum - Università di Bologna within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giovannini, E., Santelli, S., Pelletti, G. et al. Pediatric motor vehicle crashes injuries: A systematic review for forensic evaluation. Int J Legal Med 138, 1329–1341 (2024). https://doi.org/10.1007/s00414-024-03174-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-024-03174-7