
Abstract
Timing bone fractures is one of the main tasks of a forensic anthropologist, but still an uncertain diagnostic. In the literature, there are many macroscopic methods to distinguish perimortem from postmortem fractures, based on the distinct structural and mechanical properties of fresh and dry bones. However, this differentiation is still challenging, in particular when the bones are fragmented or still exhibit fresh properties. Although histologic analysis is often used as a complementary diagnostic tool in forensic pathology, its application in the evaluation of bone fractures is uncommon. The aim of this study was to investigate whether fractures of fresh bones reveal a distinct microcracking pattern compared to fractures of dry bones, in order to optimise the fracture timing. To this purpose, we histologically analysed perimortem and postmortem fractures in human humeri. The fresh bones were retrieved from traumatic autopsy cases, and the dry bones from donors which were experimentally fractured. Our results showed that the highest density and length of microcracks (MCKs) were found in the interstitial area of dry fractured bones, which may be considered a marker of postmortem damage. In fresh fractured bones, we generally observed a lower density of MCKs, but a higher proportion of osteonal MCKs, which may be considered a marker of perimortem trauma. In summary, the results of our exploratory study suggest that changes in intrinsic bone factors (mineral/organic components) result in a different microcracking pattern that can be used in fracture timing.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Timing bone injury remains challenging during the assessment of skeletal remains. This analysis implies a distinction between antemortem, perimortem and postmortem [1,2,3,4]. Antemortem trauma occurs prior to death and reveals bone remodelling as a sign of healing. On the contrary, such evidence of healing is not present in both perimortem and postmortem fractures. A reliable distinction between perimortem trauma and postmortem damage is crucial, since the former may allow conclusions on the circumstances of death. Forensic anthropologists use the term perimortem to describe all injuries occurring to wet/fresh bone, when the bone still contains its organic components, despite the fact that somatic death may have already occurred [5]. In contrast, postmortem damage occurs when the bone has lost most of its organic elements, causing it to fracture like a dry bone. It implies the involvement of taphonomic factors such as geological, biological or (un)intentional human alterations [1,2,3,4,5]. The terms ante-, peri- and postmortem are used in a different way in the field of forensic pathology, where they are only used to define the time interval related to somatic death, and not bone degradation [6].
In the literature, there are many methodologies to establish the differential diagnosis between perimortem and postmortem fractures. These methods are based on the distinct structural and mechanical properties of fresh and dry bones. They include macroscopic criteria such as the colour, the smoothness or roughness of the fractured edges [2, 4, 7, 8]. Nevertheless, a reliable differentiation between perimortem trauma and postmortem damage is still challenging and needs further knowledge on distinctive fracture patterns, which may be acquired from complementary methods.
Studies focusing on bone histology to distinguish between perimortem and postmortem bone fractures are very scarce and inconclusive. Hanaue et al. [9] investigated osteon fracture patterns by performing sagittal splitting osteotomy in two fresh human mandibles. The authors observed that fracture lines use to run along the curve of the osteonal lamellae. In contrast, Pechníková et al. [10] analysed undecalcified sections of fracture margins after blunt force trauma in fresh and dry human long bones and found that the fracture line usually crosses the osteons rather than the lamellar systems. Interestingly, they did not find significant differences in the osteon fracture pattern between fresh and dry specimens. Ebacher et al. [11] examined the structure–microcracking relations in human cortical bone tissue following compressive loading. The authors described the presence of a distinct microcracking pattern within the lamellar structure of osteons. They showed that intrinsic factors such as bone composition and microstructure as well as extrinsic factors mainly implying trauma circumstances determine the microcrack (MCK) production and distribution. However, how the different structural levels of cortical bone are involved in the fracture process is still poorly understood.
When bone is subjected to blunt trauma, it will undergo two mechanisms before a fracture occurs. In the first phase, the bone will undergo elastic deformation. This means that the bone can return to its original dimensions. In the second phase, it will experience plastic deformation, which will deform the bone permanently. The plastic phase will continue until breaking occurs [5]. Fresh bone is moist and contains water and organic components such as lipids and collagen, which make the bone stiff and elastic. Dry bone lacks these organic components, causing the bone to become stiff and brittle [12]. The loss of viscoelasticity in dry bone increases the impact sensitivity, because it makes the bone unable to resist as much strain or elastic deformation as in wet bone. This causes dry bone to fracture immediately after the strength threshold is reached [1, 5]. Due to these distinct properties, the macroscopic fracture patterns in dry and fresh bones are different. Thus, we expect that the analysis of the histological microcracking pattern will also reveal differences.
In this basic and exploratory research, we approach the hypothesis that there is a distinct microcracking pattern related to blunt force trauma in fresh bones that allows us to optimise the distinction between perimortem and postmortem fractures. An enhanced understanding about microcracking patterns in perimortem bone trauma is potentially valuable for timing and reconstructing traumatic events in the forensic context.
Material and methods
Samples
This study used both perimortem (fresh) fractured specimens and healthy unfractured dry bone samples.
To assess the perimortem (fresh) microcracking pattern, five fractured fresh humeri from five traumatic death cases were used with a postmortem time interval (PMI) between 12 and 24 h. All cases presented butterfly fractures of the humeral shaft. The victims were involved in vehicle accidents or falls and came from forensic autopsies at the Institute for Legal Medicine and Forensic Science of Catalonia (IMLCFC), which were removed for complementary medicolegal investigation. In order to correctly compare the autopsy samples with the dry bone samples, only cases with victims aged 55 or older were included in the study.
For experimental purposes, six healthy and unfractured dry humeri were collected from adults (> 60 years) that donated their body to science. The donor bones were provided with a PMI of 15 up to 20 years by the Medical Anatomy Department of the Universitat Autònoma de Barcelona (UAB). This study was approved by the Ethic Commission of Human and Animal Experimental Work (CEEAH) of the UAB, in compliance with the ethical regulations.
Fracture reproduction
The shaft of five out of six dry humeri was experimentally fractured. The experimental fractures were induced using a pendulum impact test machine consisting of a metal frame and a pendulum to which a hammer of 5 kg was attached [13]. A piece of soft rubber was attached to the hammer to avoid direct contact with the bone. The humeri were placed horizontally with the anterior side facing the hammer and attached with tie-wraps to two movable metal holders. The hammer hit perpendicularly the anterior side of the humeral shaft. All of them presented comminuted fracture.
Bone preparation and histological analysis
The resultant dry fractures were histologically compared to the fresh fractures from the autopsy cases. To this purpose, autopsy specimens were previously defleshed and cleaned for a better fracture examination. The samples were cooked in a water detergent solution at 90–100 °C during 2 to5 h. If present, remaining soft tissue was removed using surgical tools and the bones were cleaned with water and left to dry. The dry samples were only cleaned with a soft brush.
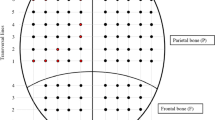
For bone histological examination purpose, specimens were cut with an oscillating saw in blocks of 4 cm including the fractured region. Each block was fixated and dehydrated following the protocol by Ebacher et al. [11] and de Boer et al. [14]. The samples were sequentially kept in a series of ethanol solutions (70%, 80%, 90%, 100%) for 24 h per step. After being left to dry, the bone fragments were embedded in epoxy resin and sectioned in a transverse plane 1 cm below the main fracture line (Fig. 1), ground, polished and mounted on frosted glasses.

Bone fragment of a fractured fresh humerus embedded in epoxy resin and sectioned in a transverse plane 1 cm below the main fracture line. From the inferior side of the resin blocks, ground and polished thin sections of about 100-µm thickness were produced
Thin sections were cut from the fixed bone blocks using a Buehler Isomet saw with a final thickness of 100 µm. Subsequently, the histological sections were put into an alcohol gradient (70%, 96%, 100%) followed by a cleaning agent (Histolemon®) to help fixing the section. Afterwards, DPX (Dibutylphthalate Polystyrene Xylene) was used as a mounting medium to bond the coverslip to the slide until it was polymerised.
To assure that our histological procedure does not produce a significant amount of MCKs, one of the dry humeri without fracture was analysed as a control. The fact that the dry condition makes the bone brittle and more sensitive to trauma allows us to test the effects of the process with a high accuracy. Histological inspection of the cortical bone was performed with a Leica DMD 108 microscope from which micrographs at 4 × magnification of the whole cortical layer were obtained. Subsequently, they were examined with ImageJ v.1.51 in order to calculate the MCK density (MCKs count per mm2) and length (µm). MCKs were divided into two main categories according to their location within the cortex: osteonal or interstitial [15]. In cases that a MCK expands in both areas, the type was defined according to the most affected area.
The MCK density and length were evaluated in several cortical areas of 1 mm2 without overlapping MCKs.
For each area, the number of osteonal and interstitial MCKs was counted (MCKs/mm2) and the length of the MCKs was measured (µm). Furthermore, the proportion of osteonal MCKs in relation to the total MCKs (osteonal and interstitial) was calculated in each area.
Statistical analysis
For descriptive statistics, the mean, median, standard deviation and quartiles were calculated. The normality of the variables was tested using the Shapiro Wilk test. Since none of the variables showed a normal distribution (P < 0.001), the non-parametric Mann–Whitney U test was used for comparative inferential analysis. The intra and inter-rater reliability of the data was analysed using the paired T-test and intraclass correlation coefficient (absolute agreement). For the intra-rater reliability, the observer who performed the data analysis (MWB) performed the MCK count a second time on a subsample. For the inter-rater reliability, this subsample was also analysed by a second observer (XJ). The statistical analyses were performed using Jamovi 1.0.4 and IBM SPSS Statistics v28.0.0. A significance level of 0.05 was set.
Results
The microcracking pattern in both fresh and dry bone samples can be observed in Figs. 2 and 3. Table 1 shows the summary statistics of the MCK variables for the two sample groups of fractured bones.

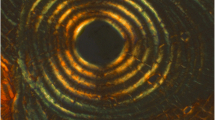
Micrographs of the histological sections of the studied fractured bones showing the microcracking pattern. Interstitial MCKs (white arrowheads). Osteonal MCKs (black arrowheads). A Dry bone with high density and greater length of interstitial MCKs. B Fresh bone with high density of short osteonal MCKs

Micrographs of the histological sections of the studied fractured bones showing the microcracking pattern. MCKs (white arrowheads). Cement line delimiting Haversian systems (black arrowheads). Haversian canal (HC). A. Dry bone with MCKs following the direction of bone lamellas. B. Strongly branched long MCKs in the interstitial area of a dry bone that do not stop at the cement line. C. Short osteonal MCKs running from the Haversian canal to the cement line in a fresh bone. D. Long osteonal MCKs breaking a cement line in a dry bone
MCK density in the osteonal area was higher in the autopsy—fresh—samples (x̅ = 4.25 ± 4.61 MCKs per mm2) than in dry specimens (x̅ = 1.62 ± 2.26 MCKs per mm2). Differences were statistically significant (Mann–Whitney U test; df 1313; P < 0.001). On the contrary to the osteons, the interstitial area of the dry specimens showed a higher MCK density (x̅ = 9.64 ± 9.32 MCKs per mm2) than the fresh samples (x̅ = 3.85 ± 2.86 MCKs per mm2). The differences were statistically significant (Mann–Whitney U test; df 1549; P = 0.004). The highest density of MCKs was found in the interstitial area of the dry bones, whilst the lowest is found in the osteonal zone of the same bones (Fig. 2A). The proportion of osteonal MCKs in relation to the total MCKs (osteonal and interstitial) was higher in the fresh specimens (x̅ = 0.44 ± 0.28) than the dry samples (x̅ = 0.10 ± 0.11) (Fig. 2B). The differences were statistically significant (Mann–Whitney U test; df 710; P < 0.001).
Regarding the MCK length, in the osteonal area there were no significant differences (Mann–Whitney U test; df 144,519; P = 0.683) between fresh (x̅ = 106.95 ± 92.32 µm) and dry samples (x̅ = 108.02 ± 90.79 µm). In the interstitial area, MCKs were shown to be longer than the osteonal ones (Fig. 3). Additionally, the longest interstitial MCKs were found in the dry specimens (x̅ = 181.23 ± 115.68 µm) (Fig. 3A, B and D) and the shortest in the fresh samples (x̅ = 168.35 ± 115.28 µm) (Fig. 3C). The differences were statistically significant (Mann–Whitney U test; df 898,609; P < 0.001).
The analysis of the control specimen (unfractured dry humerus) revealed that the amount of MCKs (x̅ = 0.21 ± 0.25 osteonal MCKs per mm2 and x̅ = 0.94 ± 0.68 interstitial MCKs per mm2) was significantly lower than in the dry fractured specimens (Table 1) (Mann–Whitney U test; df143; P < 0.001), suggesting that the histological technique was not contributing significantly to MCK propagation.
Table 2 shows the intra and inter-rater reliability analysis. The mean differences in MCKs count between observers (intra and inter) were statistically significant. Nevertheless, the intraclass correlation coefficient in all comparisons was high (ICC > 0.9), indicating very good intra and inter-rater agreement.
Discussion
The current work uses a histological approach to assess whether there are differences in the microcracking pattern between perimortem and postmortem fractures. Specifically, we analysed the microcracking pattern in dry and fresh cortical bone, focusing on the density and the length of the MCKs in the osteonal and interstitial cortical area.
The results of our study showed that in both dry and fresh bone samples, MCKs were mainly located in the interstitial area following the direction of bone lamellas (Figs. 2A and 3A, B and D). This result is concordant with existing literature, which shows that 80–90% of all MCKs occur within interstitial bone or traverse the osteonal cement lines [16, 17]. In accordance with the existing literature, initiation, spreading and even accumulation of MCKs appear to be easier in the broad interstitial area [15, 18]. Jepsen et al. [18] emphasised that whilst the osteons have a rather low mineral content, the interstitial region exhibits enlarged hydroxyapatite crystals due to a lack of remodelling, resulting in an increased brittleness. In this context, brittle bone tissue is commonly known to be more likely to fracture [1,2,3,4,5]. Another variable that has been related to the formation and number of MCKs in the interstitial area is the density of osteocytes. According to Parfitt [19], the interstitial area has a lower density of osteocytes compared to the osteons. Qiu et al. [20] reported that the probability of MCKs in the interstitial region is five times higher than in the osteonal region due to this reduced interstitial osteocyte density. Likewise, Vashishth et al. [21] showed that a reduced osteocyte density is related to the accumulation of MCKs.
In our study, we generally observed a lower density of MCKs in fresh fractured bones (Fig. 2B). In this context, Mello et al. [22] histologically compared femoral bone samples from 20 exhumed individuals with a known period of burial between 6 and 15 years to fresh femurs from routine autopsy cases. They found that the mean osteocyte count was significantly higher in the fresh femurs than in the exhumed bone samples and interpreted the decreased osteocyte number as an indicator for bone degradation due to diagenetic processes. In contrast, collagen bundles were well preserved in exhumed bone and no difference was found compared to the fresh bone specimens. Thus, the assumption that the number of osteocytes limits the number of MCKs may be an explanation for our observation that the highest density and greatest length of MCKs were found in the interstitial area of dry bone. Consequently, our results raise the question of whether theses variables may be a marker to distinguish perimortem trauma from postmortem damage.
As a further potential marker for the fracture timing, we found that the proportion of osteonal MCKs in relation to the total MCKs was significantly higher in fresh fractured bones (on average, 44% of MCKs in 1 mm2 are located inside osteons) than in dry fractured bones (10%) (Fig. 2). The protective nature of osteocytes in the propagation of microdamage has been discussed previously. However, it remains unclear why more osteonal MCKs were found in the autopsy-fresh samples than in the dry fractured specimens. Several studies suggest that the osteocytes act as mechanical transductors. By means of the osteocyte canaliculi, they are able to sense their environment and react by inducing bone remodelling following stress or strain [17, 23,24,25,26,27]. Ebacher [11] observed intralamellar cracks and hypothesised that stress accumulation in the numerous canaliculi initiates microcracking as part of early bone damage detection and remodelling process. Since a reduced osteocyte density results in a decreased canaliculi density, their hypothesis is supported by the findings of Busse et al. [28], who described a deficient microdamage detection in older individuals due to a reduced osteocyte lacunar density. It is thus assumed that a reduced osteocyte network leads to failure and delay of remodelling, excessive MCK accumulation and increased bone fragility [11, 28]. Therefore, we suggest that our results in fresh perimortem fractures may be related to the mechanotransductor role of the osteocyte network in vital bone. This is clearly a point of the study that is not well understood and therefore needs more research.
Concerning the length of MCKs, the results showed that interstitial MCKs in fresh and dry bones mainly stop when they encounter a cement line (Fig. 3A). This finding has been experimentally shown by Boyce et al. [29], who observed that interstitial cracks are spreading between cement lines. Since the cement line is an area of reduced mineralisation, it provides a relatively ductile interface with the surrounding bone matrix [30]. According to this author, its elastic properties promote both, slow crack growth but also crack initiation. However, as it has already been reported by Boyce et al. [29], we also observed the longer and strongly branched MCKs do not stop at the cement line. This finding is particularly observed in dry bones (Fig. 3B).
O’Brien et al. [15] have already shown that the length of MCKs is actually the reason for the cement line to either function as a barrier or a weakness. The reason why osteons are stopping microdamage is that bone failure occurs with the propagation of one or two long cracks up to critical lengths and not with the convergence of several small MCKs. These authors reported that short MCKs around 100 µm stop at a cement line and MCKs over 300 µm are capable of crossing it.
Regarding the osteonal MCKs, we observed that they run from the osteonal canals to the cement line (Fig. 3C), and assuming that they initiate at the canal. This assumption would be in line with the hypothesis that void structures such as bone canals provide stress concentration sites for crack initiation, whilst bone lamellae and cement lines minimise the formation of larger cracks [11, 15, 31]. However, particularly in dry specimens, a minority of osteonal MCKs are long enough to break through the cement line (Fig. 3D). Here, the cement line is rather facilitating the crack propagation. These findings may explain why it has been claimed that osteons act as a weakness in bone and enhance crack propagation [32], whilst others reported that they act as barriers to further growth [15, 33].
In summary, this basic and exploratory study provides new insights into the characteristics of microfractures in the cortical tissue of fresh and dry bone as a result of blunt force trauma. Our results indicate a different pattern of microcracks between fresh and dry fractured bones. Specifically, the finding of a higher proportion of osteonal MKCs in fresh bone fractures is a promising finding for future research on histological differences between peri- and postmortem fractures. The reported differential microcracking pattern appears to be an original and important approach to explore differences between perimortem trauma and postmortem damage in the context of forensic anthropology.
Limitations of the study
The small sample size of the study is the main limitation of the present work. As previously mentioned, this is an exploratory approach, and caution should be exercised when it comes to applying these results in the routine forensic fieldwork. Although the intra and inter-rater analysis showed an excellent agreement and indicates that the data are consistent, a better characterisation of the MKCs pattern in a bigger sample size would improve the reliability of the method. Moreover, future studies should take into account more variables such as bone variability and extrinsic factors, particularly those related to taphonomical conditions, as well as the experimental and the histological setting. This area clearly deserves further research in order to get a better understanding about microcrack production and propagation.
References
Galloway A, Zephro L, Wedel VL (2014) Diagnostic criteria for the determination of timing and fracture mechanism. In: Wedel VL, Galloway A (eds) Broken Bones: Anthropological Analysis of Blunt Force Trauma. Charles C Thomas, Springfield, pp 47–58
Christensen AM, Passalacqua NV, Bartelink EJ (2014) Forensic anthropology: current methods and practice. Academic Press, Oxford
Cappella A, Amadasi A, Castoldi E, Mazarelli D, Gaudio D, Cattaneo C (2014) The difficult task of assessing perimortem and postmortem fractures on the skeleton: a blind text on 210 fractures of known origin. J Forensic Sci 59:1598–1601
Symes SA, L’Abbé EN, Stull KE, Lacroix M, Pokines JT (2014) Chapter 13: taphonomy and the timing of bone fractures in trauma analysis. In: Pokines JT, Symes SA (eds) Manual of forensic taphonomy. CRC Press, Florida, pp 341–365
Symes SA, L’Abbé EN, Chapman EN, Wolff I, Dirkmaat DC (2012) Chapter 17: interpreting traumatic injury to bone in medicolegal investigations. In: Dirkmaat DC (ed) A companion to forensic anthropology. Wiley-Blackwell, Oxford, pp 340–388
Cunha E, Pinherio JE (2009) Antemortem trauma. In: Blau S, Ubelaker DH (eds) Handbook of forensic anthropology and archaeology. Left Coast Press, Walnut Creek, CA, pp 246–262
Wieberg DAM, Wescott DJ (2008) Estimating the timing of long bone fractures: correlation between the postmortem interval, bone moisture content, and blunt force trauma fracture characteristics. J Forensic Sci 53:1028–1034
Ortner D (2008) Differential diagnosis of skeletal injuries. In: Kimmerle EH, Baraybar JP (eds) Skeletal trauma. CRC Press, Florida, pp 21–93
Hanaue K, Katakura A, Kasahara K, Kamiyama I, Takaki T, Shibahara T, Abe S, Ide Y (2007) Course of fracture line in sagittal splitting of human mandible. Bull Tokyo Dent Coll 48(4):163–170
Pechníková M, Porta D, Cattaneo C (2011) Distinguishing between perimortem and postmortem fractures: are osteons of any help? Int J Legal Med 125:591–595
Ebacher V, Guy P, Oxland TR, Wang R (2012) Sub-lamellar microcracking and roles of canaliculi in human cortical bone. Acta Biomater 8:1093–10100
Kieser J (2013) Biomechanics of bone and bony trauma. In: Kieser J, Taylor M, Carr D (eds) Forensic biomechanics. Wiley-Blackwell, Oxford, pp 35–70
Scheirs S, Hevink B, Ortega-Sánchez M, Jordana X, McGlynn H, Rodriguez-Baeza A, Malgosa A, Galtés I (2019) Intra vitam trauma pattern. Changing the paradigm of forensic anthropology? Int J Legal Med 133:661–668
De Boer HH, Aarents MJ, Maat GJR (2013) Manual for the preparation and staining of embedded natural dry bone tissue sections for microscopy. Int J Osteoarchaeol 23:83–93
O’Brien FJ, Taylor D, Lee TC (2005) The effect of bone microstructure on the initiation and growth of microcracks. J Orthop Res 23(2):475–480
Schaffler MB, Choi K, Milgrom C (1995) Aging and matrix microdamage accumulation in human compact bone. Bone 17(6):521–525
Robling AG, Castillo AB, Turner CH (2008) Biomechanical and molecular regulation of bone remodeling. Annu Rev Biomed Eng 8:455–498
Jepsen KJ, Akkus OJ, Majeska RJ, Nadeau JH (2003) Hierarchical relationship between bone traits and mechanical properties in inbred mice. Mamm Genome 14(2):97–104
Parfitt AM (2003) New concepts of bone remodeling: A unified spatial and temporal model with physiologic and pathophysiologic implications. In: Agarwal SC, Stout SD (eds) Bone loss and osteoporosis. Springer, Boston, MA
Qiu S, Rao DS, Fyhrie DP, Palnitkar S, Parfitt AM (2005) The morphological association between microcracks and osteocyte lacunae in human cortical bone. Bone 37(1):10–15
Vashishth D, Verborgt O, Divine G, Schaffler MB, Fyhrie DP (2000) Decline in osteocyte lacunar density in human cortical bone is associated with accumulation of microcracks with age. Bone 26(4):375–380
Mello RB, Silva MRR, Alves MTS, Evison MP, Guimarães MA, Francisco RA, Astolphi RD, Iwamura ESM (2017) Tissue microarray analysis applied to bone diagenesis. Scie Rep 7(1):1–12
Marotti G, Cane V, Palazzini S, PalumboC. (1990) Structure-function relationships in the osteocytes. Ital J Min Elect Metab 4:93–106
Aarden EM, Burger EH, Nijweide PJ (1994) Function of osteocytes in bone. J Cell Biochem 55:287–299
Burger EH, Klein-Nulend J, van der Plas A, Nijweide PJ (1995) Function of osteocytes in bone—their role in mechanotransduction. Am Inst Nutr 22–3166(Suppl. 7):2020S-2023S
Rubin CT, McLeod KJ (1996) Inhibition of osteopenia by biophysical intervention. In: Marcus R, Feldman D, Kelsey J (eds) Osteoporosis. Academic, San Diego, CA, pp 351–371
Turner CH, Pavalko FM (1998) Mechanotransduction and functional response of the skeleton to physical stress: the mechanisms and mechanics of bone adaptation. J Orthop Sci 3(6):346–355
Busse B, Djonic D, Milovanovic P, Hahn M, Püschel K, Ritchie RO, Djuric M, Amling M (2010) Decrease in the osteocyte lacunar density accompanied by hypermineralized lacunar occlusion reveals failure and delay of remodeling in aged human bone. Aging Cell 9:1065–1075
Boyce TM, Fyhrie DP, Glotkowski MC, Radin EL, Schaffler MB (1998) Damage type and strain mode associations in human compact bone bending fatigue. J Orthop Res 16(3):322–329
Burr DB, Schaffler MB, Frederickson RG (1988) Composition of the cement line and its possible mechanical role as a local interface in human compact bone. J Biomech 21(11):939–945
Hazenberg JG, Hentunen TA, Heino TJ, Kurata K, Lee TC, Taylor D (2009) Microdamage detection and repair in bone: fracture mechanics, histology, cell biology. Technol Health Care 17(1):67–75
Ritchie RO, Kinney JH, Kruzic JJ, Nalla RK (2005) A fracture mechanics and mechanistic approach to the failure of cortical bone. Fatigue Fract Eng Mater Struct 28(4):345–371
Frasca P (1981) Scanning-electron microscopy studies of ‘ground substance’in the cement lines, resting lines, hypercalcified rings and reversal lines of human cortical bone. Cells Tissues Organs 109(2):115–121
Acknowledgements
Special thanks go to the technicians, library and personnel staff of the Institute of Legal Medicine and Forensic Sciences of Catalonia (IMLCFC) and the Anatomy department of the Universitat Autònoma de Barcelona (UAB).
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. Research Group in Biological Anthropology (GREAB, AGAUR 2017SGR1630). Proyectos de Generación de Conocimiento, Agencia Estatal de Investigación (PID2021-124112NB-100).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
All autopsy samples are stored in private collection at the IMLCFC, registered as a collection at the Instituto de Salud Carlos III (Reference C.0004241). Dry samples: This study was approved by the Ethic Commission of Human and Animal Experimental Work (CEEAH) of the Universitat Autònoma de Barcelona (UAB), in compliance with the ethical regulations.
Consent to participate
Informed consent was not required for this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Winter-Buchwalder, M., Schwab, N., Galtés, I. et al. Microcracking pattern in fractured bones: new approach for distinguishing between peri- and postmortem fractures. Int J Legal Med 138, 35–42 (2024). https://doi.org/10.1007/s00414-022-02875-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-022-02875-1