
Abstract
Transcranial direct current stimulation (tDCS) of the prefrontal cortex might beneficially influence neurocognitive dysfunctions associated with major depressive disorder (MDD). However, previous studies of neurocognitive effects of tDCS have been inconclusive. In the current study, we analyzed longitudinal, neurocognitive data from 101 participants of a randomized controlled multicenter trial (DepressionDC), investigating the efficacy of bifrontal tDCS (2 mA, 30 min/d, for 6 weeks) in patients with MDD and insufficient response to selective serotonin reuptake inhibitors (SSRI). We assessed whether active tDCS compared to sham tDCS elicited beneficial effects across the domains of memory span, working memory, selective attention, sustained attention, executive process, and processing speed, assessed with a validated, digital test battery. Additionally, we explored whether baseline cognitive performance, as a proxy of fronto-parietal-network functioning, predicts the antidepressant effects of active tDCS versus sham tDCS. We found no statistically significant group differences in the change of neurocognitive performance between active and sham tDCS. Furthermore, baseline cognitive performance did not predict the clinical response to tDCS. Our findings indicate no advantage in neurocognition due to active tDCS in MDD. Additional research is required to systematically investigate the effects of tDCS protocols on neurocognitive performance in patients with MDD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Transcranial Direct Current Stimulation (tDCS) is a form of non-invasive brain stimulation (NIBS) that utilizes electrodes on the scalp to create a weak electrical current in order to modulate cortical excitability [1]. In the treatment of major depressive disorder (MDD), anodal tDCS is usually applied over the left dorsolateral prefrontal cortex (DLPFC) [2], a brain area which contributes to frontoparietal network (FPN) function [3]. The FPN plays a central role for several cognitive domains, like attention[4], working memory [5], memory span [6] executive function [7], processing speed[8], and cognitive control [9]. Poor performance in these cognitive domains has also been associated with depressive disorders [10,11,12,13,14]. Therefore, it seems plausible that stimulation of the FPN could influence performance in these domains and that baseline cognitive performance, as a proxy of FPN functioning, could predict the clinical effects of stimulation.
Previous studies have investigated the neurocognitive effects of tDCS when applied to the DLPFC in patients with MDD reporting significant time-dependent improvements in attention/vigilance, working memory, executive functioning, processing speed, and social cognition when compared to placebo [15,16,17,18]. On the other hand, multiple studies report no statistically significant group-by-time interaction effects [19,20,21,22,23,24,25,26,27]. A recent meta-analysis of the cognitive effects of tDCS across multiple disorders revealed that active tDCS elicited improvements in attention/vigilance, and working memory when compared to sham tDCS [28]. This meta-analysis was based on studies that were very heterogeneous in designs, sample sizes, outcomes, and main findings. Thus, a study with a large sample size would be warranted to further test the effects of tDCS on cognition in patients with MDD. To the best of our knowledge, no studies have investigated baseline cognitive testing as a predictor of affective response to tDCS.
In this ancillary analysis of a triple-blind, randomized, sham-controlled multicenter trial, we investigated whether a standard bifrontal tDCS protocol compared to sham tDCS alters cognitive performance across the domains of memory span, working memory, selective attention, sustained attention, executive functioning, and processing speed. Additionally, we explored whether baseline cognitive performance as a proxy of FPN functioning predicts the antidepressant effects of tDCS versus sham tDCS.
Methods and materials
Study population
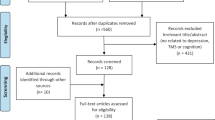
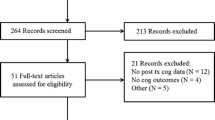
We analyzed data from the DepressionDC trial (trial registration number: NCT02530164); a triple-blind, randomized, sham-controlled clinical trial carried out across eight psychiatric centers in Germany [29]. The study investigated the efficacy and safety of tDCS as a treatment for MDD in patients that did not respond to conventional pharmacological treatment with selective serotonin reuptake inhibitors (SSRIs). Patients were originally randomized to receive 24 sessions within 6 weeks of either active or sham tDCS. The montage employed in tDCS involves placing the anode over F3 and the cathode over F4. Active stimulation consisted of a constant 2 mA direct current that lasted for 30 min. The sham paradigm consisted of a ramp-up and ramp-down sequence to induce similar skin sensations as active tDCS. tDCS was applied using a DC-stimulator (‘Mobile’, neuroConn GmbH, Ilmenau, Germany). Inclusion and exclusion criteria are reported in the supplement. Local ethics committees approved the study at each study site. All participants gave their written informed consent before inclusion in the study. From an initial sample total of 150 patients (intention-to-treat sample), we analyzed the data from 101 patients that had available neuropsychological assessments. Data from 49 patients were missing due to technical errors, organizational difficulties at the local treatment sites, and refusal to participate.
Neurocognitive test battery
Neurocognitive function was assessed longitudinally during the study at baseline, post-treatment (week 6), and at the 6-month follow-up using the EmoCogMeter, a digitalized, validated cognitive test battery developed at the Charite Berlin [30,31,32]. The EmoCogMeter examines the domains of memory span, working memory, selective attention, sustained attention, executive function, and processing speed. Memory span is tested by a digit-span assessment [33]. Working memory was assessed by an n-back task [13]. A variant of the Stroop test and a working memory component were used to assess selective attention and sustained attention, respectively [34]. executive function was measured by both the Trail Making B [35] and Tower of Hanoi tests [36]. Finally, processing speed was measured using a symbol letter modalities test, a variation of the symbol digit modality test. For additional technical information about the tests, please refer to the supplement.
Further outcome measures
The severity of the depressive episode was assessed by trained clinical staff utilizing the Montgomery-Åsberg Depression Rating Scale (MADRS), which was also chosen for the primary outcome of the study [37]. Severity is classified as an absence of symptoms (0–6 points), mild depressive episode (7–19 points), moderate depressive episode (20–34 points), or severe depressive episode (35–60 points). State and trait anxiety were measured utilizing The State-Trait Anxiety Inventory (STAI) [38], with a threshold of 39–40 for identifying clinically significant anxiety symptoms [39].
Statistical analysis
Statistical analyses were conducted in R, version 4.2.1. results [40]. Results were considered significant at α =0.05. We compared baseline characteristics between treatment groups using Pearson's χ2 tests and Wilcoxon-rank-sum tests as appropriate. To reduce the effect of extreme test performances, we identified values below the 1% and above the 99% percentile on each task and set them to the respective percentile values (winsorization).
To assess potential treatment effects of active tDCS on cognitive performance, we fitted linear mixed models using the lme4 package [41] to predict change from baseline to week 6 on each cognitive test. Treatment group (active tDCS versus sham tDCS) was included as a fixed effect while controlling for the respective baseline cognitive test score (formula: change in cognitive performance ~ treatment group + baseline cognitive performance). Sensitivity analyses included additional models with sex, age, and baseline MADRS as covariates.
To assess potential predictive influences of baseline cognitive performance on antidepressant treatment effects of active tDCS, we again fitted linear mixed models to predict change from baseline to week 6 on the MADRS. Treatment group, performance on the respective cognitive domain, and their interaction were included as fixed effects while controlling for baseline MADRS scores (formula: MADRS change ~ treatment group x cognitive performance at baseline + baseline MADRS score).
All models included the treatment site as a random effect (formula: ~ 1| site). Significance of the model factors was determined using omnibus tests (Type III ANOVA) with Satterthwaite approximation to degrees of freedom. We did not use imputation since linear mixed models are able to handle missing data. Standardized effect sizes for regression coefficients were computed using the emmeans::eff_size() approach, with the sigma parameter being directly extracted from the regression model [42]. We corrected for multiple testing across predictors using the false-discovery-rate (FDR) method [43].
Results
Sample characteristics
We analyzed data from 101 patients (active tDCS, n = 50; sham tDCS, n = 51). Mean age (active tDCS 39 [SD 14]; sham tDCS 39 [SD 14]; p = 0.76). Sex: active tDCS 40% male; sham tDCS 40% male. Primary baseline and clinical features across the active and sham-tDCS groups were similar (Table 1 and Supplementary Table 1). Winsorized mean test performances and the number of winsorized measurements per cognitive test are reported in supplementary Table 5 and 6.
Treatment effects on neurocognitive test scores
We observed no significant group-by-time interactions between treatment group and memory span, working memory, selective attention, sustained attention, executive function, or processing speed. Pre- and post-treatment performance across neurocognitive tests for active tDCS and sham tDCS is shown in Fig. 1, and Table 2 provides further statistical information. Results for additional models including sex, age and baseline MADRS yielded similar results (supplementary Table 2–4).

Pre- and post-treatment performance across neurocognitive tests for active tDCS and sham tDCS. Note: Error bars indicate mean (SE). Boxplots include the IQR with whiskers indicating 1.5 times IQR. Thin lines represent patient-individual changes
Prediction of clinician-rated depression (MADRS)
We did not detect significant interactions, when predicting MADRS change, between treatment group and memory span, working memory, selective attention, sustained attention, executive function, or processing speed. Table 3 provides the effect size of each neurocognitive test at baseline and Fig. 2 depicts the association between baseline cognitive performance and changes in MADRS scores.

Association between baseline cognitive performance and MADRS change across the trial. MADRS Montgomery-Åsberg Depression Rating Scale
Discussion
In this ancillary analysis of the DepressionDC trial, a randomized, sham-controlled multicenter study assessing the antidepressant efficacy of a prefrontal tDCS as acute treatment in patients with MDD and SSRI treatment, we found no statistically significant group differences between active tDCS and sham tDCS for the change of performance in FPN-associated cognitive domains (i.e. memory span, working memory, selective attention, sustained attention, executive function and processing speed) from baseline to week 6. Furthermore, baseline performance in these domains was not differentially associated with a change in depression severity for active tDCS compared to sham tDCS.
Our results are in contrast to a recent meta-analysis that found significant effects of tDCS on working memory and attention [28]. This meta-analysis was based on studies with sample sizes between n = 18 [15] and n = 127 [26] the number of treatment sessions (one [24] up to 22 [26] and tDCS dosages(0.5 mA [21, 27], 1 mA [15, 20] and 2 mA [16,17,18, 22,23,24,25,26]) was highly heterogeneous. Among single studies included in this meta-analysis, several authors reported an improvement of attention/vigilance, working memory, executive functioning, processing speed, and social cognition [15, 17], spatial working memory [18] or processing speed [16]. However, other studies in this meta-analysis are rather in line with our findings and did not show significant effects of tDCS on performance in neurocognitive domains [20,21,22,23,24,25,26,27]. The ELECT-TDCS trial, a clinical study with identical stimulation parameters and a larger sample size, did not find significant effects on cognition either [26].
There are several potential reasons for these negative findings. First, our multicenter trial tested only one set of tDCS parameters with the aim of reducing depressive symptoms. However, dose–response curves for single domains of neurocognitive performance have not been established. They may be non-linear and could theoretically vary from one domain to another [44, 45] as well as from dose–response curves of antidepressant effects. While being in line with previous studies on antidepressant tDCS, the administered dosage in our trial might have been insufficient to optimally modulate specific prefrontal cognitive functions. Second, the main trial did not show beneficial antidepressant effects of active tDCS over sham tDCS. Thus, the applied tDCS protocol might have also been not potent enough to modulate neuroplasticity changes in general. Third, high levels of arousal, estimated by using the State-Trait Anxiety Inventory (STAI), have been reported to diminish cognitive practice effects elicited by tDCS, [46] underlining the potential role of arousal in shaping responses to neuromodulation. In our study, both groups had high baseline STAI scores, and such high baseline anxiety could have reduced the effects of tDCS on neurocognitive performance. Lastly, several studies have reported that tDCS might only elicit procognitive effects when simultaneously combined with specific cognitive tasks [47,48,49,50,51,52]. Thus, passive stimulation, as administered in our trial, might not be sufficient to enhance cognition in patients with MDD.
To the best of our knowledge, this is the first study that investigates whether cognition at baseline may be used to predict improvement of depression during a course of tDCS. Our study has multiple strengths. The study followed the highest possible trial design standards by being triple-blinded, placebo-controlled, and multicenter. We applied a tDCS protocol (2 mA, 30 min) established in previous studies which showed a superior antidepressant efficacy of active over sham tDCS, i.e. the SELECT-TDCS [53] and ELECT-TDCS [26] trials, and our data-set is one of the biggest samples in the field to date (n = 101). Furthermore, we used a validated digital assessment battery that has successfully been used in other previous studies [31, 32, 54]. While efforts are being made to digitize previously validated cognitive tests [55, 56], such tools which also reduce documentation errors [57, 58], are still underused.
Limitations
First, there is no uniform consensus on what neurocognitive tests are better used to evaluate the performance in domains associated with FPN function. Our battery included some of the most common tests and slight variations of them. However, other standardized tests could have a higher sensitivity and specificity for detecting neuromodulation effects on cognitive performance [59]. Second, digital tools present a few caveats such as failure of the equipment, corruption of data, and loss of information when retrieving the data. This limited the availability of data in our study. Third, the evaluation of procognitive effects of tDCS and the potential predictive effects of baseline cognition on treatment response were ancillary investigations. Though this data was well balanced across both conditions, there may be latent selection biases making the sample not representative for the whole study population. In addition, the current analysis was likely underpowered to detect small treatment and prediction effects. Lastly, all patients were on a stable SSRI medication for at least 4 weeks prior to inclusion, but not antidepressant-free. Thus, our conclusions regarding the differential effects of SSRI medication and tDCS on performance in distinct neurocognitive domains are limited.
Conclusion
In conclusion, our analysis does not support the notion that acute treatment with active tDCS compared to sham tDCS leads to an improvement in FPN-related neurocognitive functions. In addition, neurocognitive functioning at baseline did not predict the change of MADRS scores over the course of tDCS. Future research should aim at identifying tDCS protocols with optimal dose–response curves for effects on specific neurocognitive domains. Most promising candidates could then be further optimized by adjusting parameters at an individual patient's level.
Data availability
The de-identified individual patient data in this paper will be made accessible after its publication for non-commercial academic projects that have a legitimate research topic and a clearly stated hypothesis. If the application is accepted, researchers will be asked to get the study approved by their institution's ethics board. The authors will subsequently provide the de-identified data sets via a safe data transfer system. You may find the DepressionDC research protocol as well as further extra information at https://osf.io/cpw6f/.
References
Woods AJ et al (2016) A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin Neurophysiol Off J Int Fed Clin Neurophysiol 127(2):1031–1048. https://doi.org/10.1016/j.clinph.2015.11.012
Lefaucheur J-P et al (2017) Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol 128(1):56–92. https://doi.org/10.1016/j.clinph.2016.10.087
Kaiser RH, Andrews-Hanna JR, Wager TD, Pizzagalli DA (2015) Large-Scale Network Dysfunction in Major Depressive Disorder: A Meta-analysis of Resting-State Functional Connectivity. JAMA Psychiat 72(6):603–611. https://doi.org/10.1001/jamapsychiatry.2015.0071
Fischer M, Moscovitch M, Alain C (2021) A systematic review and meta-analysis of memory-guided attention: Frontal and parietal activation suggests involvement of fronto-parietal networks. Wiley Interdiscip Rev Cogn Sci. https://doi.org/10.1002/wcs.1546
Lugtmeijer S, Lammers NA, de Haan EHF, de Leeuw F-E, Kessels RPC (2021) Post-Stroke Working Memory Dysfunction: A Meta-Analysis and Systematic Review. Neuropsychol Rev 31(1):202–219. https://doi.org/10.1007/s11065-020-09462-4
Botdorf M, Riggins T (2018) When less is more: Thinner fronto-parietal cortices are associated with better forward digit span performance during early childhood. Neuropsychologia 121:11–18. https://doi.org/10.1016/j.neuropsychologia.2018.10.020
Sauseng P, Klimesch W, Schabus M, Doppelmayr M (2005) Fronto-parietal EEG coherence in theta and upper alpha reflect central executive functions of working memory. Int J Psychophysiol Off J Int Organ Psychophysiol 57(2):97–103. https://doi.org/10.1016/j.ijpsycho.2005.03.018
Imms P et al (2021) Navigating the link between processing speed and network communication in the human brain. Brain Struct Funct 226(4):1281–1302. https://doi.org/10.1007/s00429-021-02241-8
Swick D, Ashley V, Turken U (2011) Are the neural correlates of stopping and not going identical? Quantitative meta-analysis of two response inhibition tasks. Neuroimage 56(3):1655–1665. https://doi.org/10.1016/j.neuroimage.2011.02.070
Rutherford BR et al (2021) Slowed Processing Speed Disrupts Patient Expectancy in Late Life Depression. Am J Geriatr Psychiatry Off J Am Assoc Geriatr Psychiatry. https://doi.org/10.1016/j.jagp.2020.11.001
Gass CS, Patten B (2020) Depressive symptoms, memory complaints, and memory test performance. J Clin Exp Neuropsychol 42(6):602–610. https://doi.org/10.1080/13803395.2020.1782848
Dotson VM et al (2020) Depression and Cognitive Control across the Lifespan: a Systematic Review and Meta-Analysis. Neuropsychol Rev 30(4):461–476. https://doi.org/10.1007/s11065-020-09436-6
Nikolin S, Tan YY, Schwaab A, Moffa A, Loo CK, Martin D (2021) An investigation of working memory deficits in depression using the n-back task: A systematic review and meta-analysis. J Affect Disord 284:1–8. https://doi.org/10.1016/j.jad.2021.01.084
Woolridge SM, Harrison GW, Best MW, Bowie CR (2021) Attention bias modification in depression: A randomized trial using a novel, reward-based, eye-tracking approach. J Behav Ther Exp Psychiatry. https://doi.org/10.1016/j.jbtep.2020.101621
Fregni F, Boggio PS, Nitsche MA, Rigonatti SP, Pascual-Leone A (2006) Cognitive effects of repeated sessions of transcranial direct current stimulation in patients with depression. Depress Anxiety 23(8):482–484. https://doi.org/10.1002/da.20201
Loo CK, Alonzo A, Martin D, Mitchell PB, Galvez V, Sachdev P (2012) Transcranial direct current stimulation for depression: 3-week, randomised, sham-controlled trial. Br J Psychiatry 200(1):52–59. https://doi.org/10.1192/bjp.bp.111.097634
Boggio PS et al (2007) Go-no-go task performance improvement after anodal transcranial DC stimulation of the left dorsolateral prefrontal cortex in major depression. J Affect Disord 101(1–3):91–98. https://doi.org/10.1016/j.jad.2006.10.026
Salehinejad MA, Ghanavai E, Rostami R, Nejati V (2017) Cognitive control dysfunction in emotion dysregulation and psychopathology of major depression (MD): Evidence from transcranial brain stimulation of the dorsolateral prefrontal cortex (DLPFC). J Affect Disord 210:241–248. https://doi.org/10.1016/j.jad.2016.12.036
Boggio PS et al (2008) A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. Int J Neuropsychopharmacol 11(2):249–254. https://doi.org/10.1017/S1461145707007833
Loo CK et al (2010) A double-blind, sham-controlled trial of transcranial direct current stimulation for the treatment of depression. Int J Neuropsychopharmacol 13(01):61. https://doi.org/10.1017/S1461145709990411
Palm U et al (2012) Transcranial direct current stimulation in treatment resistant depression: A randomized double-blind, placebo-controlled study. Brain Stimulat 5(3):242–251. https://doi.org/10.1016/j.brs.2011.08.005
Segrave RA, Arnold S, Hoy K, Fitzgerald PB (2014) Concurrent Cognitive Control Training Augments the Antidepressant Efficacy of tDCS: A Pilot Study. Brain Stimulat 7(2):325–331. https://doi.org/10.1016/j.brs.2013.12.008
Bennabi D et al (2015) Pilot study of feasibility of the effect of treatment with tDCS in patients suffering from treatment-resistant depression treated with escitalopram. Clin Neurophysiol Off J Int Fed Clin Neurophysiol 126(6):1185–1189. https://doi.org/10.1016/j.clinph.2014.09.026
Moreno ML et al (2015) Effects of acute transcranial direct current stimulation in hot and cold working memory tasks in healthy and depressed subjects. Neurosci Lett 591:126–131. https://doi.org/10.1016/j.neulet.2015.02.036
Brunoni AR, Tortella G, Benseñor IM, Lotufo PA, Carvalho AF, Fregni F (2016) Cognitive effects of transcranial direct current stimulation in depression: Results from the SELECT-TDCS trial and insights for further clinical trials. J Affect Disord 202:46–52. https://doi.org/10.1016/j.jad.2016.03.066
Brunoni AR et al (2017) Trial of Electrical Direct-Current Therapy versus Escitalopram for Depression. N Engl J Med 376(26):2523–2533. https://doi.org/10.1056/NEJMoa1612999
Pavlova EL et al (2018) Transcranial direct current stimulation of 20- and 30-minutes combined with sertraline for the treatment of depression. Prog Neuropsychopharmacol Biol Psychiatry 82:31–38. https://doi.org/10.1016/j.pnpbp.2017.12.004
Begemann MJ, Brand BA, Ćurčić-Blake B, Aleman A, Sommer IE (2020) Efficacy of non-invasive brain stimulation on cognitive functioning in brain disorders: a meta-analysis. Psychol Med 50(15):2465–2486. https://doi.org/10.1017/S0033291720003670
Burkhardt G et al (2023) Transcranial direct current stimulation as an additional treatment to selective serotonin reuptake inhibitors in adults with major depressive disorder in Germany (DepressionDC): a triple-blind, randomised, sham-controlled, multicentre trial. Lancet Lond Engl. https://doi.org/10.1016/S0140-6736(23)00640-2
Fuge P et al (2014) Assessment of Age-related Changes in Cognitive Functions Using EmoCogMeter, a Novel Tablet-computer Based Approach. J Vis Exp JoVE 84:50942. https://doi.org/10.3791/50942
Fuge P et al (2014) Interaction of Early Life Stress and Corticotropin-Releasing Hormone Receptor Gene: Effects on Working Memory. Biol Psychiatry 76(11):888–894. https://doi.org/10.1016/j.biopsych.2014.04.016
Grimm S et al (2015) Variation in the corticotropin-releasing hormone receptor 1 (CRHR1) gene modulates age effects on working memory. J Psychiatr Res 61:57–63. https://doi.org/10.1016/j.jpsychires.2014.12.001
Schroeder RW, Twumasi-Ankrah P, Baade LE, Marshall PS (2012) Reliable Digit Span: A Systematic Review and Cross-Validation Study. Assessment 19(1):21–30. https://doi.org/10.1177/1073191111428764
Epp AM, Dobson KS, Dozois DJA, Frewen PA (2012) A systematic meta-analysis of the Stroop task in depression. Clin Psychol Rev 32(4):316–328. https://doi.org/10.1016/j.cpr.2012.02.005
Bowie CR, Harvey PD (2006) Administration and interpretation of the Trail Making Test. Nat Protoc 1(5):2277–2281. https://doi.org/10.1038/nprot.2006.390
Simon HA (1975) The functional equivalence of problem solving skills. Cognit Psychol 7(2):268–288. https://doi.org/10.1016/0010-0285(75)90012-2
Montgomery SA, Asberg M (1979) A new depression scale designed to be sensitive to change. Br J Psychiatry J Ment Sci 134:382–389. https://doi.org/10.1192/bjp.134.4.382
Julian LJ (2011) Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. https://doi.org/10.1002/acr.20561
Knight RG, Waal-Manning HJ, Spears GF (1983) Some norms and reliability data for the State-Trait Anxiety Inventory and the Zung Self-Rating Depression scale. Br J Clin Psychol 22(Pt 4):245–249. https://doi.org/10.1111/j.2044-8260.1983.tb00610.x
“R: a language and environment for statistical computing.” Accessed: Jul. 10, 2023. [Online]. Available: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing
Bates D, Mächler M, Bolker B, Walker S (2015) Fitting Linear Mixed-Effects Models Using lme4. J Stat Softw 67:1–48. https://doi.org/10.18637/jss.v067.i01
R Lenth (2016) Least-Squares Means: The R Package lsmeans, J Stat Softw https://doi.org/10.18637/jss.v069.i01
Benjamini Y, Hochberg Y (1995) Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J R Stat Soc Ser B Methodol 57(1):289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
Ehrhardt SE, Filmer HL, Wards Y, Mattingley JB, Dux PE (2021) The influence of tDCS intensity on decision-making training and transfer outcomes. J Neurophysiol 125(2):385–397. https://doi.org/10.1152/jn.00423.2020
Ehrhardt SE, Ballard T, Wards Y, Dux PE, Filmer HL (2022) tDCS augments decision-making efficiency in an intensity dependent manner: A training study. Neuropsychologia 176:108397. https://doi.org/10.1016/j.neuropsychologia.2022.108397
Esposito M, Ferrari C, Fracassi C, Miniussi C, Brignani D (2022) Responsiveness to left-prefrontal tDCS varies according to arousal levels. Eur J Neurosci 55(3):762–777. https://doi.org/10.1111/ejn.15584
Schneider N et al (2021) Combining transcranial direct current stimulation with a motor-cognitive task: the impact on dual-task walking costs in older adults. J Neuroengineering Rehabil 18(1):23. https://doi.org/10.1186/s12984-021-00826-2
Lo KYH et al (2022) Concurrent anodal transcranial direct current stimulation (tDCS) with cognitive training to improve cognition in schizophrenia. Schizophr Res 241:184–186. https://doi.org/10.1016/j.schres.2022.01.026
Filmer HL, Lyons M, Mattingley JB, Dux PE (2017) Anodal tDCS applied during multitasking training leads to transferable performance gains. Sci Rep 7(1):12988. https://doi.org/10.1038/s41598-017-13075-y
Oldrati V, Colombo B, Antonietti A (2018) Combination of a short cognitive training and tDCS to enhance visuospatial skills: A comparison between online and offline neuromodulation. Brain Res 1678:32–39. https://doi.org/10.1016/j.brainres.2017.10.002
Han YMY et al (2022) Neurophysiological and behavioral effects of multisession prefrontal tDCS and concurrent cognitive remediation training in patients with autism spectrum disorder (ASD): A double-blind, randomized controlled fNIRS study. Brain Stimulat 15(2):414–425. https://doi.org/10.1016/j.brs.2022.02.004
Weller S, Nitsche MA, Plewnia C (2020) Enhancing cognitive control training with transcranial direct current stimulation: a systematic parameter study. Brain Stimulat 13(5):1358–1369. https://doi.org/10.1016/j.brs.2020.07.006
Brunoni AR et al (2013) The Sertraline vs Electrical Current Therapy for Treating Depression Clinical Study: Results From a Factorial, Randomized, Controlled Trial. JAMA Psychiat 70(4):383–391. https://doi.org/10.1001/2013.jamapsychiatry.32
Aust S et al (2022) Efficacy of Augmentation of Cognitive Behavioral Therapy With Transcranial Direct Current Stimulation for Depression: A Randomized Clinical Trial. JAMA Psychiat 79(6):528–537. https://doi.org/10.1001/jamapsychiatry.2022.0696
Vermeent S, Dotsch R, Schmand B, Klaming L, Miller JB, van Elswijk G (2020) Evidence of Validity for a Newly Developed Digital Cognitive Test Battery. Front Psychol 11:770. https://doi.org/10.3389/fpsyg.2020.00770
Chan JYC et al (2022) Evaluation of Digital Drawing Tests and Paper-and-Pencil Drawing Tests for the Screening of Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-analysis of Diagnostic Studies. Neuropsychol Rev 32(3):566–576. https://doi.org/10.1007/s11065-021-09523-2
Håkansson I, Lundström M, Stenevi U, Ehinger B (2001) Data reliability and structure in the Swedish National Cataract Register. Acta Ophthalmol Scand 79(5):518–523. https://doi.org/10.1034/j.1600-0420.2001.790519.x
Point S, Baruch Y (2023) (Re)thinking transcription strategies: Current challenges and future research directions. Scand J Manag 39(2):101272. https://doi.org/10.1016/j.scaman.2023.101272
Parkinson WL, Rehman Y, Rathbone M, Upadhye S (2020) Performances on individual neurocognitive tests by people experiencing a current major depression episode: A systematic review and meta-analysis. J Affect Disord 276:249–259. https://doi.org/10.1016/j.jad.2020.07.036
Funding
Open Access funding enabled and organized by Projekt DEAL. The DepressionDC trial was a project of the German Center for Brain Stimulation (GCBS) research consortium, funded by the German Federal Ministry of Education and Research (BMBF; grant number FKZ 01EE1403G). GB has received an internal grant for young researchers from the Medical Faculty of the Ludwig Maximilian University Munich (grant number: FOEFOLE 1127).
Author information
Authors and Affiliations
Contributions
Conceptualization: AS, GB, UV; Formal Analysis: GB, SG; Funding Acquisition: FP, AJF; Investigation: AS, UV, GB, LF, CN; Methodology: AS. GB, SA; Project Administration: FP; Resources: FP, AJF, CP, SA; Supervision: GB, FP, AJF, CP, SA; Visualization: GB; Writing – Original Draft Preparation: AS; Writing – Review & Editing: GB, FP, UV, GV, LF, AJF, CSL, SG, SA, CP, CN, LF, PZ, TK, MB.
Corresponding author
Ethics declarations
Conflict of interest
FP has received consulting fees from Brainsway Inc. (Jerusalem, Israel) as a member of the European Scientific. Advisory Board and from Sooma (Helsinki, Finland) as a member of the International Scientific. Advisory Board; honoraria for workshops from Mag&More GmbH (Munich, Germany); and honoraria for lectures from neuroCare Group (Munich, Germany) and Brainsway Inc. (Jerusalem, Israel); and has received equipment from Mag&More GmbH (Munich, Germany), neuroCare Group (Munich, Germany), and Brainsway Inc. (Jerusalem, Israel). BL received honoraria for consultancy and speakers’ fees from ANM, AstraZeneca, Autifony Therapeutics, Decibel Therapeutics, Desyncra, Gerson Lehmanns Group, Lundbeck, Merz, MagVenture, Medical Tribune, Neurolite, Neuromod, Novartis, Pfizer, Rovi, Schwabe, Sea Pharma, Servier, Sonova and Sound Therapeutics; research funding from the Tinnitus Research Initiative, Bayhost, the German Research Foundation, the German Federal Ministry of Education and Research, the American Tinnitus Association, AstraZeneca, cerbomed, Neuromod and the European Union; and has received equipment from MagVenture and Deymed Diagnostic. CP is managing partner of PsyKit GmbH, Tübingen, Germany. AS, UV, GV, LF, AJF, GB, CSL, SG, SA, CP, CN, LF, PZ, TK, and MB declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Soldini, A., Vogelmann, U., Aust, S. et al. Neurocognitive function as outcome and predictor for prefrontal transcranial direct current stimulation in major depressive disorder: an analysis from the DepressionDC trial. Eur Arch Psychiatry Clin Neurosci (2024). https://doi.org/10.1007/s00406-024-01759-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00406-024-01759-2