
Abstract
Brain gray- and white matter changes is well described in alcohol-dependent elderly subjects; however, the effect of lower levels of alcohol consumption on the brain is poorly understood. We investigated the impact of different amounts of weekly alcohol consumption on brain structure in a population-based sample of 70-year-olds living in Gothenburg, Sweden. Cross-sectional data from 676 participants from The Gothenburg H70 Birth Cohort Study 2014–16 were included. Current alcohol consumers were divided into seven groups based on self-reported weekly amounts of alcohol consumption in grams (g) (0–50 g/week, used as reference group, 51–100 g/week, 101–150 g/week, 151–200 g/week, 201–250 g/week, 251–300 g/week, and > 300 g/week). Subcortical volumes and cortical thickness were assessed on T1-weighted structural magnetic resonance images using FreeSurfer 5.3, and white matter integrity assessed on diffusion tensor images, using tract-based statistics in FSL. General linear models were carried out to estimate associations between alcohol consumption and gray- and white matter changes in the brain. Self-reported consumption above 250 g/week was associated with thinning in the bilateral superior frontal gyrus, the right precentral gyrus, and the right lateral occipital cortex, in addition to reduced fractional anisotropy (FA) and increased mean diffusivity (MD) diffusively spread in many tracts all over the brain. No changes were found in subcortical gray matter structures. These results suggest that there is a non-linear relationship between alcohol consumption and structural brain changes, in which loss of cortical thickness only occur in non-demented 70-year-olds who consume more than 250 g/week.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Heavy alcohol consumption is associated with accelerated brain damage [8, 27]. Evidence from multiple structural magnetic resonance imaging (MRI) studies show that reduced gray and white matter volume can be observed in the brains of patients with alcohol-related syndromes [42, 43]. In patients with alcohol use disorders (AUD) without cognitive deficits, findings are more inconsistent. Most studies have found atrophy in the prefrontal cortex (PFC) [5, 13, 23, 28, 37], but other brain regions have been implicated [18, 24, 25, 43]. Moreover, diffusion tensor imaging (DTI) studies have shown reduced white matter integrity in several brain regions among patients with AUD [43]. Some studies found that damage may be more severe in anterior compared to posterior white matter [43].
In contrast to chronic heavy consumption, lower levels of alcohol use have been suggested to be harmless or even beneficial in relation to brain atrophy in older adults. However, several studies have questioned these findings [30, 38] and recent evidence on all-cause mortality has prompted non-use to be the safest level of consumption for all ages [15]. Thus, the current literature on this subject is inconsistent. Few studies have investigated the effect of moderate drinking on brain structure in general, and among older adults in particular [39]. Previous findings include associations between moderate alcohol consumption and reduced total brain and hippocampal volume [38], increased ventricle size [9], reduced gray matter density, and white matter damage [4, 14]. Other studies have found no associations [16], inverse associations [7], or associations only at higher consumption levels [22].
The inconsistencies in previous studies may partly be explained by differences in sample distributions of sex, age, and neurological diseases. Several studies suggest that women are at greater risk for negative consequences of alcohol use [1, 2, 19, 28].
However, reverse findings with more volume loss in men compared with women with AUD have also been reported [31].
Another confounding factor is differences in age between different samples. Aging is associated with structural changes to the brain [32], which may lead to differences among studies with different sample age. Furthermore, beyond cognitive disability induced by alcohol, cognitive status may also reflect a neurodegenerative condition that potentially cause another pattern of brain atrophy and be a confounding effect when investigating the alcohol–brain relationship.
Alcohol use is increasing in recent cohorts of older adults in many countries [3, 6, 17, 26]. Considering the demographic shift with aging populations worldwide, more research is needed to better understand the effects of alcohol on the brain in older adults. While the association between alcohol dependence and brain changes is well described [21], the effect of non-dependent alcohol consumption on the brain is poorly understood. More specifically, few studies have examined the association between alcohol consumption and brain structure in general populations of older adults representing normal aging with true distributions of sex, cognitive status, genetic variants, and alcohol consumption patterns.
The aim of this study is to investigate the association between current alcohol use and brain structure in a large population-based sample of 70-year-olds from the Gothenburg H70 Birth Cohort study.
Methods
Participants
Cross-sectional data were derived from the baseline examination of Birth cohort 1944 in the Gothenburg H70 Birth Cohort study 2014–16 (n = 1203, response rate 72.2%). Participants were systematically selected based on birth dates obtained from the Swedish Tax Agency. The study comprises a one-day general health examination and several additional examinations (e.g., brain imaging). Study procedures have been described in detail elsewhere [33].
A total of 676 participants had a good-quality magnetic resonance imaging (MRI) [34] and available data on alcohol consumption. Out of these, 555 participants were cognitively unimpaired according to the Clinical Dementia Rating (CDR = 0) scale [20], while 121 had CDR > 0. A separate analysis was performed for the cognitively unimpaired subjects.
Ethical permits were obtained from the Swedish Ethical Review Authority (Number 869-13 and by the Radiation Protection Committee Approval number: 13-64). Written informed consents were obtained prior to participation in the study. All methods were carried out in accordance with relevant guidelines and regulations.
Assessment of alcohol consumption
Information on alcohol consumption was assessed in a face-to-face interview during the general health examination. Alcohol variables included weekly consumption of beer, wine, and spirits during the past month. Separate questions for each beverage were used to reduce the risk of underreporting [11]. Total weekly consumption (grams per week [g/week]) was calculated based on amounts reported and categorized into seven subgroups: 0–50 g/week, 51–100 g/week, 101–150 g/week, 151–200 g/week, 201–250 g/week, 251–300 g/week, and above 300 g/week. The 0–50 g/week group was considered as a reference group.
MRI acquisition
The participants were scanned on a 3.0 T Philips Achieva system (Philips Medical Systems), using a 3D T1-weigthed Turbo Field Echo (TFE) sequence (Repetition time (RT) = 7.2 ms, Echo time (TE) = 3.2 ms, flip angle = 9°, matrix size = 250 × 250 mm, field of view = 256 × 256, slice thickness = 1.0 mm) and diffusion-weighted sequence (encoded with 1 b value shell: 800ks/mm2, along with 32 directions and 1 b = 0 image (RT = 7340 ms, ET = 83 ms, flip angle = 90°, matrix size = 112 × 112 mm, field of view = 224 × 224, slice thickness = 3.0 mm).
MRI analysis
Cortical reconstruction and volumetric segmentation of subcortical volumes were performed on the T1 3D images using FreeSurfer’s 5.3 image analysis pipeline, which is documented and freely available for download online (http://surfer.nmr.mgh.harvard.edu/). The technical details of these procedures are described in prior publications, which are listed at https://surfer.nmr.mgh.harvard.edu/fswiki/FreeSurferMethodsCitation. Briefly, the whole-brain T1-weighted images underwent a correction for intensity homogeneity, skull striping, and segmentation into GM and white matter (WM). Cortical thickness was measured as the distance from the gray/white matter boundary to the corresponding pial surface. Subcortical segmentation and assessment of intracranial volume was also performed in FreeSurfer. Reconstructed data sets were visually inspected for accuracy, and segmentation errors were corrected. Quality control was carried out on all MRI data according to previous described procedures [34], and data management and processing were done through our database system [29].
Diffusion-weighted images were analyzed using the FMRIB’s Diffusion Toolbox from FSL (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) (Behrens et al., 2007). First, the data were corrected for distortions caused by eddy currents and head motion using the b0 non-diffusion data as a reference volume (Andersson and Skare, 2002). The resulting images were skull-striped and a diffusion tensor model was fitted at each voxel to determine the preferred diffusion direction as the principal eigenvector of the eigenvalue decomposition (Pierpaoli and Basser, 1996; Song et al., 2002). To provide information on the microstructural organization of the white matter, for each voxel the fractional anisotropy (FA) and mean diffusivity (MD) maps were computed (Beaulieu and Allen, 1994). The FA maps were transformed into MNI space using the tract-based spatial statistics tool. After normalization, FA images were resampled and subsequently merged into a single file to create a mean FA image for all subjects, which was then used to create a mean FA ‘skeleton’. The threshold of the skeleton was set to 0.2 to include the WM tracts that were common to all subjects. Individual FA maps were then projected onto this mean FA skeleton. The transformation matrix of FA obtained in the above steps was applied to MD maps.
Statistical methods
Structural MRI
Analyses were performed on the total sample (n = 676). Group cortical thickness comparisons were performed using vertex-based GLM (general linear model) in FreeSurfer that included degree of weekly consumption in 50 g intervals and sex as factors and cortical thickness as dependent variable. The Gaussian smoothing kernel was 10 mm. The level of statistical significance was evaluated using a cluster-wise P (CWP) value correction procedure for multiple comparisons based on a Monte Carlo z-field simulation with a cluster forming threshold of p < 0.05 (vertex-z-threshold = 1.3). The association between FreeSurfer segmented subcortical volumes and alcohol consumption was assessed using univariate general linear models (GLM) in Statistica (TIBCO Software Inc. version 13. http://tibco.co), correcting for sex and intracranial volume.
Diffusion tensor imaging
To assess the relationship between alcohol consumption with FA and MD maps, voxel-wise regression analyses were carried out including the alcohol consumption as dependent variable and sex as a confounder. Moreover, group comparisons were carried out assessing the difference in FA and MD between the reference group and other groups with increasing alcohol consumption. All analyses were performed using the randomize tool of FSL with 5000 permutations. The results were corrected for multiple comparisons using threshold-free cluster enhancement corrections (p < 0.05).
Results
Sample characteristics
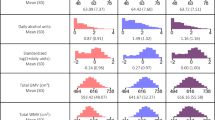
Characteristics of the sample of current drinkers (n = 676) are given in Table 1. The mean (SD) age of the sample at time of MRI scan was 70.5 (0.28), and 47.8% (n = 324) were men. A total of 302 participants (44.6%) were in the 0–50 g/week consumption group, 155 (22.9%) in the 51–100 g/week, 94 (13.9%) in the 101–150 g/week, 56 (8.3%) in the 151–200 g/week, 25 (3.7%) in the 201–250 g/week, 16 (2.4%) in the 251–300 g/week, and 28 (4.1%) in the > 300 g/week group. Only three women consumed more than 300 g pure alcohol per week, which were considered too few to be included in the analysis. Thus, men in the reference group were compared with men in the > 300 g/week-group (n = 25).
APOE Ɛ4 carrier status was not associated with more cortical thinning in subgroups that consumed more alcohol than the reference group. Smoking was not associated with decrease or increase of cortical or subcortical volume and was therefore not included in the model.
The present study comprised 352 women and 324 men. We did, however, not observe any significant interaction (gender*consumption; supplementary Fig. 1) in the analysis we performed. We, therefore, did not perform stratified analysis with men and women separately.
Within the reference group, individuals reporting no alcohol consumption during the past month (n = 80), were less likely to be in a relationship (p < 0.001), were less likely born in Sweden (p < 0.001), and had higher frequency of mild cognitive problems (CDR = 0.5; p = 0.006). There was, however, no significant difference between participants consuming 0 g compared with participants who consumed 1–50 g in brain volume or DTI measures investigated in this study. Therefore 0 g and 1–50 g were merged into one group.
Associations between alcohol consumption and cortical thickness
There were no differences regarding regional cortical thickness between the reference group and consumption groups < 250 g/week (i.e., 51–100 g/week, 101–150 g/week, 151–200 g/week, 201–250 g/week). In participants consuming 251–300 g/week (n = 16), atrophy was observed in the left precentral gyrus left superior frontal and left lateral occipital gyrus, the right postcentral gyrus, right caudal middle frontal gyrus and the right superior frontal gyrus, compared with the reference group (Fig. 1A; Supplementary Table 1).

Cortical thinning in high-consuming participants. A Participants that consumed 0–50 g have thicker cortex than participants who consumed 251–300 g. B Participants who consumed less than 251 g have thicker cortex than participants who consumed more than 250 g. C Participants with CDR = 0, participants who consumed 0–50 g have thicker cortex than participants who consumed 251–300 g. D Men consumed 0–50 g/week have ticker cortex than men that consumed more than 300 g/week. Cortical thinning displayed on the inflated cortical surface. Warmer colors indicate that the reference group have thicker cortex. Images in the upper row display the left hemisphere, the lower column the right hemisphere. Cluster-wise p values < 0.05 are displayed. L left, R right
The results above indicate that cortical thinning may occur in participants who drink > 250 g/week. We, therefore, also compared all participants consuming ≤ 250 g/week (n = 632) with participants consuming > 250 g (n = 44). Participants consuming > 250 g/week displayed cortical thinning in the bilateral superior frontal gyrus, the right caudal middle frontal, precentral and lateral occipital gyrus (Fig. 1B, Fig. 2; supplementary table 2).

Cortical thinning in participants who are consuming > 250 g/week. The graph displays mean cortical thinning under areas that were reduced in participants who consumed > 250 g/week (areas with significant cortical thinning in Fig. 1B). The x-axis denotes alcohol consumption. The y-axis cortical thickness converted to z-scores
Cognitively unimpaired participants who consumed 251–300 g/week displayed cortical atrophy in the left precentral gyrus as well as the right precentral and caudal middle frontal and superior frontal gyrus compared to the reference group (Fig. 1C, supplementary table 3). No changes were observed in white matter or subcortical volumes.
In men consuming > 300 g/week (n = 25), cortical thinning was observed in many cortical areas (i.e., areas in the bilateral caudal superior and middle frontal gyrus, pre- and postcentral gyrus, entorhinal and fusiform gyrus, posterior cingulate gyrus, paracentral lobule) compared to the men in the reference group (n = 25; Fig. 1D, Supplementary Table 4).
The association between alcohol consumption and subcortical volumes
Subcortical structures did not display reduced volume at any levels of alcohol consumption compared to the reference group.
The association between alcohol consumption and white matter integrity
There were no differences in either FA or MD between reference group and consumption groups ≤ 151 g/week (51–100 g/week and 101–150 g/week). In participants consuming 151–200 g/week (n = 50), reduced FA was found in the body of the corpus callosum and in the superior corona radiata (Fig. 3A, Supplementary Table 5). In participants consuming 251–300 g/week (n = 15), FA was reduced, and MD was increased in a large number of white matter tracts (Fig. 3B, Supplementary Table 5). Men consuming > 300 g/week did not display reduced FA or increased MD in any white matter tract.

The reduction of fractional anisotropy and increase of mean diffusivity in participants who consumed 151–200 g/week and 251–300 g/week. A Reduced FA and in participants who consumed 151–200 g/week compared with participants who consumed 0–50 g/week, B Reduced FA and increased MD in participants who consumed 251–300 g/week compared with participants who consumed 0–50 g/week, Cold colors, areas of significant reduction, darkest blue = p < 0.05 brightest blue = p < 0.005. Warm colors, areas of significant increase, darkest red = p < 0.05 brightest red = p < 0.005
Comparing participants consuming ≤ 250 g/week with participants consuming > 250 g/week (n = 41) we found reduced FA and increased MD in a large number of tracts including anterior thalamic radiation, corticospinal tract, cingulum, forceps major, forceps minor, inferior fronto-occipital fasciculus, inferior longitudinal fasciculus, superior longitudinal fasciculus, uncinate fasciculus, and superior longitudinal fasciculus (Fig. 4, Supplementary table 6).

The reduction of fractional anisotropy and increase of mean diffusivity in participants who consumed > 250 g/week compared with participants who consumed ≤ 250 g/week. Reduced FA and increased MD in participants who consumed > 250 g/week compared with participants who consumed ≤ 250 g/week. Cold colors, areas of significant reduction, darkest blue = p < 0.05 brightest blue = p < 0.005. Warm colors, areas of significant increase, darkest red = p < 0.05 brightest red = p < 0.005
Discussion
In the present study, we aimed to examine the association between current alcohol consumption and brain gray and white matter structure in a large population-based sample of 70-year-olds.
Alcohol consumption of 250 g pure alcohol or more per week was predominantly associated with atrophy of the PFC. These results are in line with a longitudinal study that found increased alcohol-related cortical atrophy rate in frontal > parietal > insular > cingulate and temporal cortex [36]. However, in contrast to Sullivan et al. [35], we also observed thinning in the right occipital cortex. Further, Sullivan et al. (2019) reported that volume loss in the precentral gyrus and the superior frontal gyrus was higher in patients with AUD at 30 years of age, and that the maximal difference in cortical thickness in these regions was found when 70-year-old patients with AUD were compared with 70-year-old controls (ibid). Thus, our results confirm this previous study and indicate that the precentral and superior frontal gyrus may be particularly (and early) affected by alcohol.
Consistent with previous results, we found predominantly right-sided in high-consuming participants. Many studies have found more alcohol-related cortical atrophy in the right than left hemisphere, which led some authors to propose a “right hemisphere hypothesis” [28]. This hypothesis is further supported by the observation that cognitive functions localized within the right hemisphere are more affected in patients with AUD than functions localized to the left hemisphere [10, 41].
In the present study, 25 men did consume more than 300 g per week. In addition to frontal atrophy these participants further displayed volume loss in regions known to become atrophic in Alzheimer’s disease such as the bilateral medial temporal lobe (the entorhinal and fusiform gyrus), the posterior cingulate, precuneus, in the left superior parietal cortex and bilateral supramarginal gyrus [12]. Thus, our findings indicate that high alcohol consumption (251–300 g/week) is associated with specific frontal and occipital, < right-side pattern of cortical thinning, while very high consumption (> 300 g/week) involves thinning in the frontal, temporal, occipital, and parietal lobes.
In this sample, approximately 18% of participants had mild cognitive problems (CDR = 0.5). Comparing the 251–300 g/week consuming group with the reference group in participants with CDR = 0 revealed cortical thinning in approximately the same regions as in the whole sample (Fig. 1C and Supplementary Table 3).
These findings confirm that we can identify alcohol-related gray matter changes also in participants with no cognitive problems. The lack of associations regarding white matter changes in the higher consuming groups among participants with CDR = 0 may be due to low statistical power.
While high alcohol consumption was linked to a regional specific pattern of cortical gray matter atrophy, the white matter changes were less specific. Instead, it was widely distributed over in many tracts of the brain. Potentially may this be the “signature” of alcohol-related white matter changes in non-demented individuals.
We found no white matter changes in the highest-consuming group (> 300 g/week), while the second highest (251–300 g/week) had changes in many tracts of the brain. It is difficult to explain this finding. Possibly, the splitting of the high consuming group > 250 g into 251–300 g/week vs. > 300 g/week may have reduced our statistical power so that we were not able to detect subtle changes. Such interpretation is supported by the fact that we found significant changes in white matter when the > 250 g/week group was compared with the ≤ 250 g/week group.
One strength of this study is that results are based on data from a systematically selected sample of 70-year-olds from a general population. Obviously, as all participants are 70 years of age, we do not have the confounding effect of age in our results. This is also a limitation as we cannot study whether our results would be generalizable to other age groups. On the other hand, as discussed above, the pattern of alcohol-related cortical thinning is in agreement with some other studies including middle aged or even younger subjects.
One limitation is that alcohol consumption categories are based on past month consumption.
Certainly, in some individuals, the past months may not reflect the average consumption over an extended period of time. Furthermore, current data do not allow us to analyze drinking behavior, e.g., we cannot identify individuals with alcohol addiction among the high consumers of our sample. However, considering the observed thinning in cortical areas of the frontal lobe, we can at least say that these high consumers have a non-healthy consumption pattern.
Another limitation is that while our sample is large, we still suffer from the lack of statistical power when dividing the sample into seven groups. The reason for doing this was that we aimed to find the cutoff value for how much alcohol that can be consumed before structural brain changes in terms of reduced cortical thickness or reduced FA in whiter matter occur. The negative effect of alcohol consumption was found to occur in a non-linear fashion, in which consumption above 250 g per week was linked to significant brain changes.
A final limitation is that we have not assessed comorbid conditions, such as psychiatric disorders, that potential may be associated with brain atrophy. While one previous study indicates that such factors could be interesting to consider [40], we aim to address this in a follow-up study.
Conclusions
In conclusion, we found alcohol-related cortical thinning and white matter changes in 70-year-old men and women consuming more than 250 g pure alcohol per week. Cortical changes were mainly observed in the frontal lobe predominantly in the right hemisphere, while high consumption seems to affect both anterior and posterior white matter tracts in the whole brain. Our findings indicate that there is an increased risk for brain damage also among non-dependent individuals with high weekly consumption.
Data availability
Data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval by the steering group of the studies, and that it is in accordance with rules and regulations from the European Union (e.g. GDPR) and Swedish law.
References
Agabio R, Pisanu C, Gessa GL, Franconi F (2017) Sex differences in alcohol use disorder. Curr Med Chem 24:2661–2670
Agartz I, Momenan R, Rawlings RR, Kerich MJ, Hommer DW (1999) Hippocampal volume in patients with alcohol dependence. Arch Gen Psychiatry 56:356–363
Ahlner F, Sigström R, Rydberg Sterner T, MellqvistFässberg M, Kern S, Östling S, Waern M, Skoog I (2018) Increased alcohol consumption among swedish 70-year-olds 1976 to 2016: analysis of data from the Gothenburg H70 Birth Cohort studies, Sweden. Alcohol Clin Exp Res 42:2403–2412
Anstey KJ, Jorm AF, Réglade-Meslin C, Maller J, Kumar R, von Sanden C, Windsor TD, Rodgers B, Wen W, Sachdev P (2006) Weekly alcohol consumption, brain atrophy, and white matter hyperintensities in a community-based sample aged 60 to 64 years. Psychosom Med 68:778–785
Bae S, Kang I, Lee BC, Jeon Y, Cho HB, Yoon S, Lim SM, Kim J, Lyoo IK, Kim JE, Choi IG (2016) Prefrontal cortical thickness deficit in detoxified alcohol-dependent patients. Exp Neurobiol 25:333–341
Breslow RA, Castle IP, Chen CM, Graubard BI (2017) Trends in alcohol consumption among older Americans: national health interview surveys, 1997 to 2014. Alcohol Clin Exp Res 41:976–986
de Bruin EA, Hulshoff Pol HE, Schnack HG, Janssen J, Bijl S, Evans AC, Kenemans JL, Kahn RS, Verbaten MN (2005) Focal brain matter differences associated with lifetime alcohol intake and visual attention in male but not in female non-alcohol-dependent drinkers. Neuroimage 26:536–545
Denny CH, Serdula MK, Holtzman D, Nelson DE (2003) Physician advice about smoking and drinking: are U.S. adults being informed? Am J Prev Med 24:71–74
Ding J, Eigenbrodt ML, Mosley TH Jr, Hutchinson RG, Folsom AR, Harris TB, Nieto FJ (2004) Alcohol intake and cerebral abnormalities on magnetic resonance imaging in a community-based population of middle-aged adults: The atherosclerosis risk in communities (ARIC) study. Stroke 35:16–21
Ellis RJ, Oscar-Berman M (1989) Alcoholism, aging, and functional cerebral asymmetries. Psychol Bull 106:128–147
Embree BG, Whitehead PC (1993) Validity and reliability of self-reported drinking behavior: dealing with the problem of response bias. J Stud Alcohol 54:334–344
Fjell AM, McEvoy L, Holland D, Dale AM, Walhovd KB, Alzheimer’s Disease Neuroimaging I (2014) What is normal in normal aging? effects of aging, amyloid and Alzheimer’s disease on the cerebral cortex and the hippocampus. Prog Neurobiol 117:20–40
Fortier CB, Leritz EC, Salat DH, Venne JR, Maksimovskiy AL, Williams V, Milberg WP, McGlinchey RE (2011) Reduced cortical thickness in abstinent alcoholics and association with alcoholic behavior. Alcohol Clin Exp Res 35:2193–2201
Fukuda K, Yuzuriha T, Kinukawa N, Murakawa R, Takashima Y, Uchino A, Ibayashi S, Iida M, Yao H, Hirano M (2009) Alcohol intake and quantitative mri findings among community dwelling Japanese subjects. J Neurol Sci 278:30–34
GBD 2016 Alcohol Collaborators (2018) Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 392(10152):1015–1035
Gu Y, Scarmeas N, Short EE, Luchsinger JA, DeCarli C, Stern Y, Manly JJ, Schupf N, Mayeux R, Brickman AM (2014) Alcohol intake and brain structure in a multiethnic elderly cohort. Clin nutr (Edinburgh, Scotland) 33:662–667
Han BH, Moore AA, Sherman S, Keyes KM, Palamar JJ (2017) Demographic trends of binge alcohol use and alcohol use disorders among older adults in the united states, 2005–2014. Drug Alcohol Depend 170:198–207
Harper J, Malone SM, Wilson S, Hunt RH, Thomas KM, Iacono WG (2021) The effects of alcohol and cannabis use on the cortical thickness of cognitive control and salience brain networks in emerging adulthood: a co-twin control study. Biol Psychiatry 89:1012–1022
Hitzemann R, Bergeson SE, Berman AE, Bubier JA, Chesler EJ, Finn DA, Hein M, Hoffman P, Holmes A, Kisby BR, Lockwood D, Lodowski KH, McManus M, Owen JA, Ozburn AR, Panthagani P, Ponomarev I, Saba L, Tabakoff B, Walchale A, Williams RW, Phillips TJ (2022) Sex differences in the brain transcriptome related to alcohol effects and alcohol use disorder. Biol Psychiatry 91:43–52
Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL (1982) A new clinical scale for the staging of dementia. The Br J psychiatry : J mental sci 140:566–572
Kril JJ, Halliday GM (1999) Brain shrinkage in alcoholics: A decade on and what have we learned? Prog Neurobiol 58:381–387
Kubota M, Nakazaki S, Hirai S, Saeki N, Yamaura A, Kusaka T (2001) Alcohol consumption and frontal lobe shrinkage: Study of 1432 non-alcoholic subjects. J Neurol Neurosurg Psychiatry 71:104–106
Li J, Wang Y, Xu Z, Liu T, Zang X, Li M, Ma L (2019) Whole-brain morphometric studies in alcohol addicts by voxel-based morphometry. Ann Transl Med 7:635
Mackey S, Allgaier N, Chaarani B, Spechler P, Orr C, Bunn J, Allen NB, Alia-Klein N, Batalla A, Blaine S, Brooks S, Caparelli E, Chye YY, Cousijn J, Dagher A, Desrivieres S, Feldstein-Ewing S, Foxe JJ, Goldstein RZ, Goudriaan AE, Heitzeg MM, Hester R, Hutchison K, Korucuoglu O, Li CR, London E, Lorenzetti V, Luijten M, Martin-Santos R, May A, Momenan R, Morales A, Paulus MP, Pearlson G, Rousseau ME, Salmeron BJ, Schluter R, Schmaal L, Schumann G, Sjoerds Z, Stein DJ, Stein EA, Sinha R, Solowij N, Tapert S, Uhlmann A, Veltman D, van Holst R, Whittle S, Wright MJ, Yucel M, Zhang S, Yurgelun-Todd D, Hibar DP, Jahanshad N, Evans A, Thompson PM, Glahn DC, Conrod P, Garavan H, Group EAW (2019) Mega-analysis of gray matter volume in substance dependence: general and substance-specific regional effects. Am J Psychiatry 176:119–128
Maksimovskiy AL, Fortier CB, Milberg WP, McGlinchey RE (2019) A structural mri study of differential neuromorphometric characteristics of binge and heavy drinking. Addict Behav Rep 9:100168
Marmet S, Rehm J, Gmel G (2016) The importance of age groups in estimates of alcohol-attributable mortality: impact on trends in Switzerland between 1997 and 2011. Addiction (Abingdon, England) 111:255–262
Miller JW, Naimi TS, Brewer RD, Jones SE (2007) Binge drinking and associated health risk behaviors among high school students. Pediatrics 119:76–85
Momenan R, Steckler LE, Saad ZS, van Rafelghem S, Kerich MJ, Hommer DW (2012) Effects of alcohol dependence on cortical thickness as determined by magnetic resonance imaging. Psychiatry Res 204:101–111
Muehlboeck JS, Westman E, Simmons A (2014) Thehivedb image data management and analysis framework. Front Neuroinform 7:49
Paul CA, Au R, Fredman L, Massaro JM, Seshadri S, Decarli C, Wolf PA (2008) Association of alcohol consumption with brain volume in the Framingham study. Arch Neurol 65:1363–1367
Pfefferbaum A, Rosenbloom M, Deshmukh A, Sullivan E (2001) Sex differences in the effects of alcohol on brain structure. Am J Psychiatry 158:188–197
Raz N, Gunning-Dixon F, Head D, Rodrigue KM, Williamson A, Acker JD (2004) Aging, sexual dimorphism, and hemispheric asymmetry of the cerebral cortex: replicability of regional differences in volume. Neurobiol Aging 25:377–396
Rydberg Sterner T, Ahlner F, Blennow K, Dahlin-Ivanoff S, Falk H, Havstam Johansson L, Hoff M, Holm M, Horder H, Jacobsson T, Johansson B, Johansson L, Kern J, Kern S, Machado A, MellqvistFassberg M, Nilsson J, Ribbe M, Rothenberg E, Ryden L, Sadeghi A, Sacuiu S, Samuelsson J, Sigstrom R, Skoog J, Thorvaldsson V, Waern M, Westman E, Wetterberg H, Zetterberg H, Zetterberg M, Zettergren A, Ostling S, Skoog I (2019) The gothenburg h70 birth cohort study 2014–16: design, methods and study population. Eur J Epidemiol 34:191–209
Simmons A, Westman E, Muehlboeck S, Mecocci P, Vellas B, Tsolaki M, Kloszewska I, Wahlund LO, Soininen H, Lovestone S, Evans A, Spenger C (2011) The AddNeuroMed framework for multi-centre MRI assessment of Alzheimer’s disease: experience from the first 24 months. Int J Geriatr Psychiatry 26:75–82
Sullivan EV, Pfefferbaum A (2019) Brain-behavior relations and effects of aging and common comorbidities in alcohol use disorder: a review. Neuropsychology 33:760–780
Sullivan EV, Zahr NM, Sassoon SA, Thompson WK, Kwon D, Pohl KM, Pfefferbaum A (2018) The role of aging, drug dependence, and hepatitis c comorbidity in alcoholism cortical compromise. JAMA Psychiat 75:474–483
Tomasi DG, Wiers CE, Shokri-Kojori E, Zehra A, Ramirez V, Freeman C, Burns J, Kure Liu C, Manza P, Kim SW, Wang GJ, Volkow ND (2019) Association between reduced brain glucose metabolism and cortical thickness in alcoholics: evidence of neurotoxicity. Int J Neuropsychopharmacol 22:548–559
Topiwala A, Allan CL, Valkanova V, Zsoldos E, Filippini N, Sexton C, Mahmood A, Fooks P, Singh-Manoux A, Mackay CE, Kivimäki M, Ebmeier KP (2017) Moderate alcohol consumption as risk factor for adverse brain outcomes and cognitive decline: longitudinal cohort study. BMJ (Clin Res ed) 357:j2353
Topiwala A, Ebmeier KP (2018) Effects of drinking on late-life brain and cognition. Evid Based Ment Health 21:12–15
Uhlmann A, Bandelow B, Stein DJ, Bloch S, Engel KR, Havemann-Reinecke U, Wedekind D (2019) Grey matter structural differences in alcohol-dependent individuals with and without comorbid depression/anxiety-an MRI study. Eur Arch Psychiatry Clin Neurosci 269:285–294
Yoon HW, Chung JY, Oh JH, Min HK, Kim DJ, Cheon Y, Joe KH, Kim YB, Cho ZH (2009) Differential activation of face memory encoding tasks in alcohol-dependent patients compared to healthy subjects: an fMRI study. Neurosci Lett 450:311–316
Zahr NM, Kaufman KL, Harper CG (2011) Clinical and pathological features of alcohol-related brain damage. Nat Rev Neurol 7:284–294
Zahr NM, Pfefferbaum A (2017) Alcohol’s effects on the brain: Neuroimaging results in humans and animal models. Alcohol Res 38:183–206
Acknowledgements
The study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (ALF965812, ALF 716681), the Swedish Research Council (2012-5041, 2015-02830, 2013-8717, 2017-00639, 2019-01096, 2022-00882), Swedish Research Council for Health, Working Life and Wellfare (2013-1202, 2018-00471, AGECAP 2013-2300, 2013-2496, 2018-00471), Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse, Hjärnfonden (FO2014-0207, FO2016-0214, FO2018-0214, FO2019-0163, FO2020-0235), Alzheimerfonden (AF-554461, AF-647651, AF-743701, AF-844671, AF-930868, AF-940139, AF-968441), Eivind och Elsa K:son Sylvans stiftelse,
The Alcohol Research Council of the Swedish Alcohol Retailing Monopoly (no 2017-0051, 2016-0059, FO 2019-0077, FO2021-0067), Systembolagets alkoholforskningsråd (CAN), Swedish Research Council for Health, Working Life and Wellfare (2017-1604)
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lindberg, O., Ahlner, F., Tsevis, T. et al. Effects of current alcohol use on brain volume among older adults in the Gothenburg H70 Birth Cohort study 2014–16. Eur Arch Psychiatry Clin Neurosci 274, 363–373 (2024). https://doi.org/10.1007/s00406-023-01691-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-023-01691-x