
Abstract
The aim of this naturalistic observational study was to investigate EEG alterations in patients under olanzapine treatment with a special regard to olanzapine dose and plasma concentration. Twenty-two in-patients of a psychiatric university ward with the monodiagnosis of paranoid schizophrenia (ICD-10: F20.0), who received a monotherapy of olanzapine were included in this study. All patients had a normal alpha-EEG before drug therapy, and did not suffer from brain-organic dysfunctions, as verified by clinical examination and cMRI scans. EEG and olanzapine plasma levels were determined under steady-state conditions (between 18 and 22 days after begin of treatment). In 9 patients (40.9%), pathological EEG changes (one with spike-waves) consecutive to olanzapine treatment were observed. The dose of olanzapine was significantly higher in patients with changes of the EEG than in patients without changes (24.4 mg/day (SD: 8.1) vs. 12.7 mg/day (SD: 4.8); T = −4.3, df = 21, P < 0.001). In patients with EEG changes, the blood plasma concentration of olanzapine (45.6 μg/l (SD: 30.9) vs. 26.3 μg/l (SD: 21.6) tended to be also higher. The sensitivity of olanzapine dosage to predict EEG changes was 66.7%, the specificity 100% (Youden-index: 0.67). EEG abnormalities during olanzapine treatment are common. These are significantly dose dependent. Thus, EEG control recordings should be mandatory during olanzapine treatment with special emphasis on dosages exceeding 20 mg per day, although keeping in mind that EEGs have only a limited predictive power regarding future epileptic seizures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Second-generation antipsychotics (SGA) were introduced due to a smaller amount of adverse drug reactions (ADR), particularly with regard to extrapyramidal syndromes (EPS). However, the generally believed superiority of SGAs in terms of efficacy and safety has been challenged in the last decade [1–3]. Most recently, in a Cochrane review [4], the authors concluded that despite a slightly better efficacy of olanzapine when compared with other SGAs, this has to be weighed against a larger weight gain and its associated metabolic problems.
No significant differences were reported for the risk to develop epileptic seizures when olanzapine was compared with newer atypical antipsychotic drugs such as amisulpiride, quetiapine and risperidone, but seizure risk was lower than under clozapine (RR = 0.15; CI: 0.04–0.58), based on four randomized controlled trials [4]. However, epileptic seizures are a clinically relevant ADR of all antipsychotics. Accordingly, epileptiform EEG abnormalities during treatment with typical and atypical antipsychotics were reported in psychiatric patients with a high variability among SGAs, which was particularly high in patients under clozapine [5] or olanzapine medication [6]. The authors concluded that EEG abnormality risk may vary widely among specific antipsychotics. It was assessed that this risk was particularly high with clozapine and olanzapine, moderate with risperidone and typical antipsychotics, and low with quetiapine. In contrast to this finding, patients treated with quetiapine had significantly more EEG abnormalities, although still rarely observed [7] when compared with patients treated with haloperidol or olanzapine.
For patients under clozapine treatment, therapeutic EEG monitoring was suggested due to frequent EEG abnormalities, [8–11]. However, it may be debatable if a strict EEG monitoring regime is necessary for patients treated with olanzapine, given the rare incidence of seizures for these patients [12].
In addition, it should be taken into account that “EEG changes also vary with serum levels and are as necessary as adequate serum levels for clinical efficacy” [5, 13]. Moreover, co-medication such as benzodiazepine derivates, which are frequently administered in psychotic patients, could have limited the amount of olanzapine treatment-related EEG alterations in prior studies.
Therefore, it was decided to conduct an observational study with a clearly defined patient population (monotherapy and monodiagnoses) to overcome possible biases in other studies (such as inclusion of patients with a benzodiazepine co-medication [6].
Method
Sample
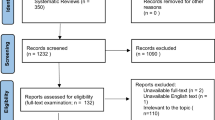
Thirty in-patients of a psychiatric university ward treated with olanzapine were included in the study. Of them, 14 patients (46.7%) were women, and 16 were men (53.3%). The mean age was 44.6 years (range: 18–75 years; SD: 17.0).
All patients with an additional diagnosis other than paranoid schizophrenia (ICD-10: F20.0) or with any additive medication (benzodiazepines, other antipsychotic, or antidepressant medication) were excluded from the analysis. All patients had at least two EEGs readings. For all patients included in the further analysis, the first examination was classified as normal-alpha-EEG. No patient had a history of epilepsy, seizures or seizure-like episodes. An absence of any other neurological disorder was also necessary for inclusion in this study. In addition, patients received a cMRI. Any significant pathologic findings in the cMRI served as exclusion criteria.
Eight screened patients had to be excluded from the analysis because of meeting one or more of the exclusion criteria. Therefore, 22 patients (7 women: 31.8%, 15 men: 68.2%; mean age: 44.8 years, range: 18–69 years, SD: 15.2) remained for the final analysis.
Technical methods
EEG recordings from 30 psychiatric patients (Department of Psychiatry and Psychotherapy, University of Göttingen, Germany) treated with olanzapine were graded to age, gender, diagnoses, and treatment for type and severity of EEG abnormalities. Dose and clinical factors were evaluated for association with EEG abnormalities. EEG recordings were performed according to the international 10/20 system [14] with 21 electrodes. Plasma olanzapine levels were assessed by high-performance liquid chromatography (HPLC) with low-wavelength ultraviolet absorption detection (253 nm). EEG and plasma levels were determined under steady-state drug conditions (~18–22 days after starting). All EEGs were evaluated by two independent investigators from the Department of Clinical Neurophysiology of the University of Göttingen, who were not involved in the study design, analyses or treatment of the patients. They were also blinded to medication state.
EEG and cMRT were performed according to the standard procedures of the psychiatric university ward in all in-patients. Only the first EEG under olanzapine treatment was considered for analyses. EEGs were classified as normal (alpha-rhythm or variant without pathological alterations), or displaying mild (regional theta activity, pharmacogenic beta-activity), medium (regional theta-delta activity), or severe abnormalities (sharp waves or spikes, periodic patterns, suppression of EEG activity and generalised slowing).
Statistical methods
Normal distribution of age of the patients, dose and blood plasma level of olanzapine was assessed by the Kolmogorov–Smirnov method. Student’s t-test and Pearson correlations were computed to test for statistical associations. Sensitivity and specificity of olanzapine dose and blood plasma level to predict EEG abnormalities were graphically plotted with receiver operating characteristic (ROC) curves. The statistical analysis was performed by calculation of the area under the ROC curve (AUC) with corresponding 95% confidence intervals. The significance level was set at α = 0.05. All statistical tests were two-sided. For the data analyses, the statistical software package SPSS for Windows 16 (SPSS Inc., Chicago, Illinois, USA) was used.
Results
The mean dose of olanzapine was 17.5 mg per day (SD 8.6; range: 5–35 mg). The mean olanzapine blood plasma level was 34.2 μg/l (SD: 26.9; range: 5–111 μg/l). The dose and the plasma level were significantly correlated (Pearson’s correlation coefficient, r = 0.67, P = 0.001).
Per definition, the first EEG was regular in all patients included in the study. The second EEG performed under stable olanzapine medication was unchanged in 13 patients (59.1%, normal EEG with α-rhythm). In 9 patients (40.9%), pathological alterations were observed. Here, in two (9.1%) patients pharmacogenic beta (β) activity, in three patients (13.6%) other mild pathological abnormalities, in three (13.6%) medium severe pathologic abnormalities, and in one patient (4.5%) severe pathologic abnormalities with spike-wave complexes were observed (see Table 1 for a more detailed description of the EEG patterns). No seizures occurred. Neither age (Mann–Whitney-U, Z = −1.2, P = 0.24) nor gender (χ2 = 3.0, df = 1, P = 0.08) were significantly associated with pathological EEG patterns.
The dose of olanzapine was significantly higher in patients with pathological EEG changes than in patients without changes (24.4 mg/day (SD: 8.1) vs. 12.7 mg/day (SD: 4.8); t = −4.3, df = 21, P < 0.001) (Fig. 1). A respective trend was present for the blood concentration of olanzapine (45.6 μg/l (SD: 30.9) vs. 26.3 μg/l (SD: 21.6)), too (Fig. 2). Table 1 displays the demographic parameters (age and sex), blood plasma levels of olanzapine and EEG alterations for each dose of olanzapine.

Association between olanzapine dosage in mg and EEG abnormalities (categorised into three groups). The box length is the interquartile range

Association between blood plasma concentration of olanzapine in μg/l and EEG abnormalities (categorised into three groups). Circle shows a case with more than 1.5 box lengths from the upper or lower edge of the box. The box length is the interquartile range
The ROC curve with EEG alteration as dependent factor and dose as predictor showed an AUC (area under the curve) of 0.88 (95% CI: 0.71–1.00; P = 0.003). The best cut-off value with respect to the best Youden—index was a dose of olanzapine higher than 20 mg/day. The sensitivity was 66.7%, the specificity 100% (Youden-index: 0.67), the positive predictive value 100% and the negative predictive value 81.3% (see Fig. 3).

Receiver operating characteristic (ROC) curve for the detection of EEG abnormalities using the olanzapine dosage
Regarding the blood plasma level of olanzapine, no predictor with a significant AUC in the ROC curve was identified. The best Youden—index would be a cut-off value of above 25 μg/l with a good sensitivity of 88.9%, but poor specificity of 38.5%.
The Pearson’s correlation between blood plasma level and dosage was r = 0.57 (not significant) in patients with a pathologically altered EEG, whereas the correlation coefficient in patients with normal EEG was 0.729 (r = 0.729; P = 0.005).
Discussion
The present study explored the association between olanzapine mediation and pathological alterations of the EEG in a naturalistic patient sample. The results of the present study show that olanzapine causes EEG alterations, and that these alterations are predominantly dose dependent. A suitable cut-off point for the prediction of EEG abnormalities was a daily dose of olanzapine higher than 20 mg, which is in line with the dosage recommended by the manufacturer. Age, sex and blood plasma levels were not significantly associated with EEG alterations. However, for blood plasma level, a respective trend was identified, and lack of significance could be due to the limited statistical power of the study.
The proportion of 40.9% abnormal EEGs in this study is in line with other findings in studies investigating the effects of olanzapine on EEG (proportion of 35% in [7]). It was also observed that EEG abnormalities were statistically significantly increased with dose in the olanzapine group [7]. In another study, a proportion of 44% of patients with EEG abnormalities under olanzapine treatment was described; however, this was based on a small sample size (n = 9 in [15]). The proportion of EEG abnormalities in a study by Centorrino et al. [6] was also comparable (38.5%).
The present study could not confirm a statistical association with the age of the patients, but identified a dose dependency of the effects, which did not occur in the study by Centorinno and co-workers. However, patients in that study were not treated under monotherapy conditions, which may bias the comparability. Haring et al. [5] described an association between EEG abnormalities and blood plasma concentrations of olanzapine. This was not confirmed in the present study, which may be explained by the limited statistical power due to a small sample size. However, a respective trend was observed also in the present study.
Olanzapine is antagonistic (among others) on the dopaminergic receptors D1, D2 and D4 [19] which may impact on the cortico-spinal excitability [19] and may be partly expressed in EEG alterations. The EEG changes seen in the present study are in accordance with a previous report, in which an increase of theta activity by olanzapine in healthy subjects (experimental data including P300) was described [16]. Moreover, it was reported that olanzapine may increase the delta activity in the posterior region [17]. The present results contrast findings by Pillmann et al. [18] that epileptiform activity was not increased under olanzapine treatment.
Wichniak et al. [20] reported that the risk of epileptic seizures under olanzapine treatment can be regarded as low as long as olanzapine is administered as a monotherapy. In addition to this, an excess increase in the dosage of olanzapine should be regarded with caution. Seizures due to olanzapine treatment may be rare, nevertheless a fatal status epilepticus has been described [21].
Strengths of the presented design include the focus on a homogenous patient cohort (only schizophrenia as a monodiagnosis according to ICD-10 F20.0, no relevant pre-existing conditions, no seizure history, regular cMRT without pathological finding in all participants) which has been treated with a monotherapy. In addition, blood plasma levels were recorded and all patients had a regular EEG before treatment. Moreover, all EEGs were rated by two certified investigators, who were not involved in the treatment of the study patients. Furthermore, the raters were blinded regarding the administered olanzapine dose.
The relatively small sample size of this study may be regarded as a limitation. Therefore, other factors which may contribute to a higher proportion of EEG abnormalities in this patient group may have remained undetected due to the limited statistical power. Another relevant limitation is the observational design during a short period of time. No weight-adjusted correlation between blood plasma level and dosage was performed due to missing or unreliable self-reported weight information. It would be interesting to follow up all patients over a period of several years to gain more insight into the relevance of the observed EEG alterations for the manifestation of clinical epileptic seizures. Thus, the current conclusions refer more to EEG abnormalities than to clinical symptoms. In addition, it should be kept in mind that EEG abnormalities may be limited in their power to predict future seizures, at least in certain subpopulations of patients [22, 23]. However, since epileptic seizures are relevant ADRs of antipsychotic drugs, the EEG may help to identify patients at risk. Furthermore, EEG measurements are reported to add information for patients at risk for psychosis [24].
As mentioned above, it would be relevant to estimate the risk of seizures under high-dose olanzapine treatment, and the predictive value of EEG alterations. In order to achieve this goal, a greater sample size, EEG-monitored follow-up studies and observation of cohorts (including different diagnoses and subgroups) may be useful. In addition, implementing an integrated care network in the psychiatric sector [25] for patients under olanzapine treatment may be beneficial. However, a challenge for this will be the treatment practice with benzodiazepine derivates, which on the one hand are administered for seizure prevention and therapy, and on the other hand alter EEG abnormalities.
However, given the results of this and other studies, we conclude that EEG control measurements should be mandatory during olanzapine treatment with special caution if dose levels exceed 20 mg per day, if the patient is treated with concomitant medications, and if there is a history of seizures in the past. However, it should be kept in mind that EEGs have only a limited predictive power regarding the occurrence of epileptic seizures in future. The use of anticonvulsive medication should not be based on the existence of EEG alterations. In addition, a switch to another antipsychotic drug or change of its dosage may be sometimes required.
References
Jones PB, Barnes TR, Davies L et al (2006) Randomized controlled trial of the effect on quality of life of second- vs. first-generation antipsychotic drugs in schizophrenia: cost utility of the latest antipsychotic drugs in schizophrenia study (CUtLASS 1). Arch Gen Psychiatry 63:1079–1087
Lieberman JA, Stroup TS, McEvoy JP et al (2005) Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 353:1209–1223
Leucht S, Corves C, Arbter D et al (2009) Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet 373:31–41
Komossa K, Rummel-Kluge C, Hunger H, et al (2009) Olanzapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev CD006654
Haring C, Neudorfer C, Schwitzer J et al (1994) EEG alterations in patients treated with clozapine in relation to plasma levels. Psychopharmacology (Berl) 114:97–100
Centorrino F, Price BH, Tuttle M et al (2002) EEG abnormalities during treatment with typical and atypical antipsychotics. Am J Psychiatry 159:109–115
Amann BL, Pogarell O, Mergl R et al (2003) EEG abnormalities associated with antipsychotics: a comparison of quetiapine, olanzapine, haloperidol and healthy subjects. Hum Psychopharmacol 18:641–646
Freudenreich O, Weiner RD, McEvoy JP (1997) Clozapine-induced electroencephalogram changes as a function of clozapine serum levels. Biol Psychiatry 42:132–137
Gross A, Joutsiniemi SL, Rimon R, Appelberg B (2004) Clozapine-induced QEEG changes correlate with clinical response in schizophrenic patients: a prospective, longitudinal study. Pharmacopsychiatry 37:119–122
Silvestri RC, Bromfield EB, Khoshbin S (1998) Clozapine-induced seizures and EEG abnormalities in ambulatory psychiatric patients. Ann Pharmacother 32:1147–1151
Welch J, Manschreck T, Redmond D (1994) Clozapine-induced seizures and EEG changes. J Neuropsychiatry Clin Neurosci 6:250–256
Beasley CM Jr, Tollefson GD, Tran PV (1997) Safety of olanzapine. J Clin Psychiatry 58(Suppl 10):13–17
Fink M (2002) EEG changes with antipsychotic drugs. Am J Psychiatry 159:1439 (discussion 1439)
Jasper H (1958) Progress and problems in brain research. J Mt Sinai Hosp NY 25:244–253
Schuld A, Kuhn M, Haack M et al (2000) A comparison of the effects of clozapine and olanzapine on the EEG in patients with schizophrenia. Pharmacopsychiatry 33:109–111
Hubl D, Kleinlogel H, Frolich L et al (2001) Multilead quantitative electroencephalogram profile and cognitive evoked potentials (P300) in healthy subjects after a single dose of olanzapine. Psychopharmacology (Berl) 158:281–288
Yamada K, Isotani T, Irisawa S et al (2004) EEG Global field power spectrum changes after a single dose of atypical antipsychotics in healthy volunteers. Brain Topogr 16:281–285
Pillmann F, Schlote K, Broich K, Marneros A (2000) Electroencephalogram alterations during treatment with olanzapine. Psychopharmacology (Berl) 150:216–219
Nitsche MA, Monte-Silva K, Kuo MF, Paulus W (2010) Dopaminergic impact on cortical excitability in humans. Rev Neurosci 21:289–298
Wichniak A, Szafranski T, Wierzbicka A, Waliniowska E, Jernajczyk W (2006) Electroencephalogram slowing, sleepiness and treatment response in patients with schizophrenia during olanzapine treatment. J Psychopharmacol 20:80–85
Wyderski RJ, Starrett WG, Abou-Saif A (1999) Fatal status epilepticus associated with olanzapine therapy. Ann Pharmacother 33:787–789
Fountain NB, Freeman JM (2006) EEG is an essential clinical tool: pro and con. Epilepsia 47(Suppl 1):23–25
Kim HL, Donnelly JH, Tournay AE, Book TM, Filipek P (2006) Absence of seizures despite high prevalence of epileptiform EEG abnormalities in children with autism monitored in a tertiary care center. Epilepsia 47:394–398
Gschwandtner U, Pflueger MO, Semenin V et al (2009) EEG: a helpful tool in the prediction of psychosis. Eur Arch Psychiatry Clin Neurosci 259:257–262
Brocheler A, Bergmann F, Schneider F (2009) Models of mental health care in psychiatry across sectoral borders. Eur Arch Psychiatry Clin Neurosci 259(Suppl 2):S227–S232
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Degner, D., Nitsche, M.A., Bias, F. et al. EEG alterations during treatment with olanzapine. Eur Arch Psychiatry Clin Neurosci 261, 483–488 (2011). https://doi.org/10.1007/s00406-011-0208-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-011-0208-4