
Abstract
Purpose
This study sought to explore whether the experience level of the first assistant surgeon influences perioperative organ injuries (ureteral, bladder, and intestinal injuries) in patients undergoing total laparoscopic hysterectomy (TLH) for benign diseases. We defined an experienced surgeon as a surgeon certified by the Skill Qualification Committee of the Japan Society of Gynecologic and Obstetric Endoscopy and Minimally Invasive Therapy or a surgeon with equivalent surgical skills.
Methods
We reviewed our surgical registry database of TLH for benign indications between 2014 and 2020 and only selected cases performed by an experienced primary surgeon. Patients were divided into two groups based on the experience level of the first assistant. Inverse probability of treatment weighting by propensity score, which was adjusted for patient and procedure characteristics, was used to examine differences in perioperative organ injuries according to the experience level of the first assistant.
Results
Among 1682 patients who underwent TLH, 18 organ injuries were found (0.83%). In the propensity score inverse probability of treatment weighting models, less experience of the first assistant had no significant impact on the occurrence of perioperative organ injuries (p = 0.348).
Conclusion
In TLH for benign indications at our hospital, given an experienced primary surgeon, the inclusion of a less experienced first assistant does not negatively affect the occurrence of perioperative organ injuries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
It is recommended that inexperienced first assistants participate in TLH for training and experience while considering the difficulty of the surgical cases. |
Introduction
Throughout the last three decades, laparoscopic surgery has replaced laparotomy for gynecological surgery [1,2,3]. Hysterectomy is one of the most common gynecologic surgical procedures worldwide, especially for benign conditions [4, 5]. Compared with open surgery, laparoscopic surgery for hysterectomy is regarded as a minimally invasive approach on the basis of decreased blood loss, length of hospital stay, postoperative pain, risk of infection, and shorter overall recovery time [6,7,8]. Because of the obvious advantages of total laparoscopic hysterectomy (TLH), it is imperative that gynecologists receive adequate exposure to this technique to gain experience [9]. Compared with abdominal and vaginal hysterectomies, TLH requires greater surgical expertise [7], a longer time to master, and a longer operating time [7, 10]. As surgeons perform more laparoscopic procedures, it is prudent to consider how many operations an individual surgeon must perform to be considered competent [11]. The number of cases needed to achieve an experienced level of performance of TLH has been reported to range from 21 to 75 [4, 12, 13].
However, primary surgeons cannot successfully perform laparoscopic surgery alone and inevitably require a surgical team that includes assistant surgeons [14]. At our institution, TLH is aided by two assistants. The first assistant holds the laparoscope, while the second assistant moves the uterine manipulator.
In a teaching hospital such as ours, trainees including novices in laparoscopic surgery and residents are continuously rotated for surgical training purposes. The experience of the first assistant is essential for trainees of TLH so that they can acquire the skills of a primary surgeon. Assistants understand the details of the operative procedure, learn effective methods to support the operator, and ensure that their experience is useful for their own future performance of the procedure.
Though TLH has many advantages mentioned above, when serious complications, especially injuries in organs adjacent to the uterus (ureteral, bladder, and intestinal injuries), occur during the surgery, conversion to laparotomy is frequently needed [15], which increases the secondary burden and stress on patients [16].
To find a balance between patient safety and trainee education, the effects on the occurrence of severe complications must be scrutinized. Previous investigations have highlighted the relationship between the experience of primary surgeons and perioperative complications in TLH [9, 17,18,19]. However, to our knowledge, little is known about the impact of the first assistant surgeon’s experience in TLH on the development of complications. Therefore, in the current study, we aim to identify the influence of the first assistant surgeon’s experience on the occurrence of perioperative organ injuries (ureteral, bladder, and intestinal injuries) in TLH for benign diseases.
Methods
Study design and population
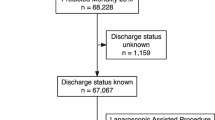
We conducted a retrospective cohort study of 1,682 women who underwent TLH for benign indications between January 1, 2014 and December 31, 2020 at Teine Keijinkai Hospital in Sapporo, Japan. All TLH procedures were performed by fully qualified and experienced primary surgeons. All patients were admitted to the hospital one day before surgery, and they received standard prophylactic antibiotics. A blood test was performed on postoperative day (POD) 2 according to our department’s clinical protocol (Table S1).
Exposure measurements
Data on 12 variables were collected (Table S2), and they included demographic data, comorbidities, preoperative use of gonadotropin-releasing hormone (GnRH) agonists, surgical data, surgical techniques in addition to TLH, and diagnosis. We defined an experienced surgeon, including both the operator and the first assistant, as a surgeon certified by the Skill Qualification Committee of the Japan Society of Gynecologic and Obstetric Endoscopy and Minimally Invasive Therapy or a surgeon with equivalent surgical skills. A surgeon with equivalent surgical skills to those of the certified endoscopic surgeon was defined as a surgeon familiar with TLH who had performed at least 75 TLH surgeries in the past, as mentioned above [4, 12, 13]. To acquire this qualification, applicants are required to perform over 100 gynecologic laparoscopic surgeries over a 2-year period after qualification as a specialist recognized by the Japan Society of Obstetrics and Gynecology; they are also required to pass an examination involving a video of the surgery. We believed that this qualification could only be obtained by a surgeon whose skills had improved after appropriate training and that a technically certified surgeon could be considered an experienced surgeon. Because our hospital is a teaching hospital, many young physicians leave within 6 months to a few years. Therefore, by the aforementioned definition, none of the inexperienced surgeons trained at our hospital became experienced surgeons.
Outcome measurements
To identify patients with organ injuries (ureteral, bladder, and intestinal injuries) related to TLH, medical records were evaluated within 90 days of TLH. Evidence of perioperative organ injuries was determined by review of the operative report, imaging, or a urology and surgery consultation note.
Statistical analysis
Data were reported as medians (interquartile ranges [IQRs]) for continuous variables. Categorical variables were depicted as absolute numbers and proportions and reported as numbers (%). We divided patients into two groups according to whether an experienced first assistant was present during surgery. To identify the risk factors associated with organ injuries during the 90 days after TLH, univariate analyses were performed. To compare each variable between the two groups, the chi-squared test or Fisher’s exact test was used for categorical variables, and the Mann–Whitney U test was used for continuous variables because all continuous variables follow nonparametric distributions.
Propensity score (PS)-based inverse probability of treatment weighting (IPTW) was fitted to confirm the background differences in the two groups in assessing whether the presence or absence of an experienced first assistant affected the morbidity rate of organ injuries. First, the PS for the group with an experienced first assistant was determined by fitting a binary logistic regression model. Patient demographics, comorbidities, preoperative use of a GnRH agonist, surgical data, surgical techniques in addition to TLH, and diagnoses were entered into the final model. Then, an IPTW approach was used to assign the group with an experienced first assistant a weight of 1/PS, and the group without an experienced first assistant, a weight of 1/(1 − PS). The cases in which the PS values were greater than 0.1 were included in the analysis. In the PS-IPTW model, proportional distribution of baseline covariates was assessed by the standardized mean difference (SMD). The two groups were considered to be well balanced when the SMD was less than 0.1. We tested for the differences in organ injury rate between the two groups using Poisson regression. Two-sided p values < 0.05 were considered to show statistical significance. We used the statistical software R 3.6.1 for the statistical analyses [20].
Ethics
This study was approved by the research ethics committee of Teine Keijinkai Hospital (approval no.: 2-020337-00). Informed consent was obtained in the form of opt-out on the website of Teine Keijinkai Hospital.
Results
Of the 1,682 patients, 14 (0.83%) developed organ injuries (ureteral, bladder, and intestinal injuries) during the 90 days after TLH. Five (35.7%) had ureteral injuries, two (14.3%) had bladder injuries, six (42.9%) had intestinal injuries, and one (7.1%) had both bladder and intestinal injuries (Table 1). The result of univariate analysis and baseline characteristics of patients before and after inverse probability weighting in this study are presented in Table 2. In the univariate analysis, in the group with an experienced first assistant, the rates of diabetes mellitus (p value ≤ 0.001) and prior pelvic surgery (p value = 0.038) were significantly lower, whereas the rate of preoperative use of a GnRH agonist was significantly higher (p value ≤ 0.001) than that in the group without an experienced first assistant.
After PS-IPTW, all 12 covariates were well balanced between the two groups (SMD less than 0.1), and no significant difference was observed in the incidence rate of organ injuries between the two groups (p = 0.348). IPTW estimator was 0.52 (95% Confidence interval [− 0.72, 1.75]) (Table 3).
Discussion
In this study, we evaluated the impact of the first assistant’s experience level on the occurrence of perioperative organ injuries. As a result, the involvement of an inexperienced first assistant in TLH for benign diseases was not found to affect the morbidity rate of organ injuries.
Regarding different surgical procedures, several studies determined the complications associated with the experience level of the first assistant. In surgeries for benign diseases, Tarik et al. reported that the training level of the first assistant in bariatric procedures did not negatively affect the occurrence of serious perioperative complications [21]. In surgeries for malignant diseases, comparable results have been reported in laparoscopic sigmoidectomies and laparoscopic hepatectomies [14, 22].
During TLH, the first assistant has several important roles. The skills of the first assistant are an essential part of an effective surgical team because first assistants serve as an integral bridge between primary surgeons and patients [23]. Above all, the surgical camera plays a vital role in the success of any laparoscopic procedure. Techniques that ensure optimal visualization are imperative for first assistants [24]. Moreover, they must identify the dissection plane, grasp tissue, add adequate counter traction, and provide the appropriate surgical field view for primary surgeons [25]. First assistants also provide suitable guidance and second opinions intraoperatively if needed [26, 27].
A primary surgeon may experience stress when working with an inexperienced assistant [14]. Cai et al. described potential reasons why surgery with an inexperienced assistant does not affect the morbidity of complications [22]. First, the lack of experience of the first assistant surgeon could be offset by the rest of the surgical team. If the primary surgeon knows that the first assistant surgeon is less experienced, he or she may consciously verbalize all instructions more clearly to enable better support by the first assistant surgeon. The primary surgeon may also involve more assistants in the surgery for a more even division of tasks. Second, appropriate selection of the surgical assistant based on his or her experience level may occur in consideration of case difficulty and the primary surgeon’s experience. In our study, the group of experienced first assistants had a slightly longer operative time than the group that did not. It may be that experienced first assistants were selected for more difficult cases. Furthermore, Igor et al. stated that primary surgeons may alter their technique based on the experience level of assistant surgeons to ensure surgical safety [27].
The median BMI of the operated women was approximately 22. Compared to patients with normal BMI, the high BMI patients who underwent TLH reported no particular increase in complications [28], which would be unlikely to account for the relatively low rate of organ damage in this study.
One strength of this study is that it included detailed perioperative information from our surgical database. Moreover, all patients received standardized and homogeneous management at our hospital. On the contrary, this study also has several limitations, and the results should be interpreted with caution. First, this study has inherent bias associated with operative factors that may not be referenced from the medical records (e.g., the degree of surgical difficulty and how to handle the organization by the surgeon). Second, our study reflected the experience of a single hospital, and the findings may not be generalizable to other institutions and settings. Lastly, TLH has low rates of perioperative complications and is considered relatively safe. Therefore, it may be difficult to detect significant differences in the rates of perioperative complications between patients in this cohort.
Conclusion
In a population of women who underwent TLH performed by experienced primary surgeons for benign diseases at Teine Keijinkai Hospital, the involvement of an inexperienced first assistant did not affect the morbidity rate of organ injuries. Considering the experience level of the first assistant and the difficulty of surgical cases, the participation of inexperienced first assistants in TLH should, therefore, be encouraged for training and exposure.
References
Varghese A, Doglioli M, Fader AN (2019) Updates and controversies of robotic-assisted surgery in gynecologic surgery. Clin Obstet Gynecol 62:733–748. https://doi.org/10.1097/GRF.0000000000000489
Šimičević M, Juras J, LovrićGršić H et al (2021) Comparison of laparoscopic and laparotomic approach in lymphadenectomy in women with gynaecological cancer. J Inst Obstet Gynaecol 41:329–330. https://doi.org/10.1080/01443615.2020.1716312
Vitale SG, Ludwin A, Vilos GA et al (2020) From hysteroscopy to laparoendoscopic surgery: what is the best surgical approach for symptomatic isthmocele? A systematic review and meta-analysis. Arch Gynecol Obstet 301:33–52. https://doi.org/10.1007/s00404-020-05438-0
Terzi H, Biler A, Demirtas O et al (2016) Total laparoscopic hysterectomy: analysis of the surgical learning curve in benign conditions. Int J Surg Lond Engl 35:51–57. https://doi.org/10.1016/j.ijsu.2016.09.010
Albright BB, Witte T, Tofte AN et al (2016) Robotic versus laparoscopic hysterectomy for benign disease: a systematic review and meta-analysis of randomized trials. J Minim Invasive Gynecol 23:18–27. https://doi.org/10.1016/j.jmig.2015.08.003
Farquhar CM, Steiner CA (2002) Hysterectomy rates in the United States 1990–1997. Obstet Gynecol 99:229–234
Aarts JW, Nieboer TE, Johnson N et al (2015) Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD003677.pub5
Meikle SF, Nugent EW, Orleans M (1997) Complications and recovery from laparoscopy-assisted vaginal hysterectomy compared with abdominal and vaginal hysterectomy. Obstet Gynecol 89:304–311. https://doi.org/10.1016/S0029-7844(96)00315-8
Igwe E, Hernandez E, Rose S, Uppal S (2014) Resident participation in laparoscopic hysterectomy: impact of trainee involvement on operative times and surgical outcomes. Am J Obstet Gynecol 211:484.e1–7. https://doi.org/10.1016/j.ajog.2014.06.024
Johnson N, Barlow D, Lethaby A et al (2005) Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials. BMJ 330:1478
Mavrova R, Radosa JC, Wagenpfeil G et al (2016) Learning curves for laparoscopic hysterectomy after implementation of minimally invasive surgery. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet 134:225–230. https://doi.org/10.1016/j.ijgo.2016.01.017
Mäkinen J, Johansson J, Tomás C et al (2001) Morbidity of 10 110 hysterectomies by type of approach. Hum Reprod Oxf Engl 16:1473–1478. https://doi.org/10.1093/humrep/16.7.1473
Donnez O, Donnez J (2010) A series of 400 laparoscopic hysterectomies for benign disease: a single centre, single surgeon prospective study of complications confirming previous retrospective study. BJOG Int J Obstet Gynaecol 117:752–755. https://doi.org/10.1111/j.1471-0528.2010.02520.x
Kim YW, Min BS, Kim NK et al (2010) The impact of incorporating of a novice assistant into a laparoscopic team on operative outcomes in laparoscopic sigmoidectomy: a prospective study. Surg Laparosc Endosc Percutan Tech 20:36–41. https://doi.org/10.1097/SLE.0b013e3181cdb762
Api M, Boza A, Kayataş S, Boza B (2017) Laparoscopic repair of ureter damaged during laparoscopic hysterectomy: presentation of two cases. Turk J Obstet Gynecol 14:191–194. https://doi.org/10.4274/tjod.34270
İnan AH, Budak A, Beyan E, Kanmaz AG (2019) The incidence, causes, and management of lower urinary tract injury during total laparoscopic hysterectomy. J Gynecol Obstet Hum Reprod 48:45–49. https://doi.org/10.1016/j.jogoh.2018.10.009
Hildebrandt T, Emir S, Boosz A et al (2018) Total laparoscopic hysterectomy: how does training for surgeons in a standardized operation affect hospitals and patients? Arch Gynecol Obstet 298:763–771. https://doi.org/10.1007/s00404-018-4869-3
Barber EL, Harris B, Gehrig PA (2016) Trainee participation and perioperative complications in benign hysterectomy: the effect of route of surgery. Am J Obstet Gynecol 215:215.e1–7. https://doi.org/10.1016/j.ajog.2016.02.022
Jokinen E, Brummer T, Jalkanen J et al (2015) Hysterectomies in Finland in 1990–2012: comparison of outcomes between trainees and specialists. Acta Obstet Gynecol Scand 94:701–707. https://doi.org/10.1111/aogs.12654
Ihaka R, Gentleman R (1996) R: a language for data analysis and graphics. J Comput Graph Stat 5:299–314. https://doi.org/10.1080/10618600.1996.10474713
Yuce TK, Holmstrom A, Soper NJ et al (2020) Complications and readmissions associated with first assistant training level following elective bariatric surgery. J Gastrointest Surg Off J Soc Surg Aliment Tract. https://doi.org/10.1007/s11605-020-04787-0
Cai M, Syn NLX, Koh Y-X et al (2020) Impact of first assistant surgeon experience on the perioperative outcomes of laparoscopic hepatectomies. J Laparoendosc Adv Surg Tech A 30:423–428. https://doi.org/10.1089/lap.2019.0701
Yuh B (2013) The bedside assistant in robotic surgery–keys to success. Urol Nurs 33:29–32
Chiu A, Bowne WB, Sookraj KA et al (2008) The role of the assistant in laparoscopic surgery: important considerations for the apprentice-in-training. Surg Innov 15:229–236. https://doi.org/10.1177/1553350608323061
Johnston WK, Low RK, Das S (2003) Image converter eliminates mirror imaging during laparoscopy. J Endourol 17:327–331. https://doi.org/10.1089/089277903322145521
Abu-Ghanem Y, Erlich T, Ramon J et al (2017) Robot assisted laparoscopic radical prostatectomy: assistant’s seniority has no influence on perioperative course. J Robot Surg 11:305–309. https://doi.org/10.1007/s11701-016-0655-z
Sorokin I, Nelson J, Canvasser NE (2018) Re: robot-assisted laparoscopic radical prostatectomy: assistant’s seniority has no influence on perioperative course. J Robot Surg 12:389–390. https://doi.org/10.1007/s11701-018-0836-z
O’Hanlan KA, Emeney PL, Frank MI et al (2021) Total laparoscopic hysterectomy: making it safe and successful for obese patients. JSLS 25(e2020):00087. https://doi.org/10.4293/JSLS.2020.00087
Acknowledgements
We thank the surgeons who conducted TLH reported in this study, including C. Sato, MD; T. Matsuda, MD; A. Nakajima, MD; H. Ota, MD; K. Imai, MD; T. Higa, MD; Y. Yamamoto, MD; T. Suzuki, MD; Y. Suzuki, MD; K. Minowa, MD; R. Tsunematsu, MD; K. Takimoto, MD; M. Yamamoto, MD; Y. Ohara, MD; M. Nishimura, MD; S. Matsumoto, MD; T. Cho, MD; T. Shimabukuro, MD; and S. Asai, MD. We also thank Ms. Y. Kawabata for constructing the databases used in this study.
Funding
The authors have no relevant financial or non-financial interests to disclose.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Data collection was performed by YT. Data analysis was performed by YT and ST. The first draft of the manuscript was written by YT and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsuzuki, Y., Hirata, T., Tsuzuki, S. et al. Does the experience of the first assistant affect organ injuries in laparoscopic hysterectomy for benign diseases?. Arch Gynecol Obstet 307, 453–458 (2023). https://doi.org/10.1007/s00404-022-06745-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-022-06745-4