
Abstract
Introduction
Progressive collapsing foot deformity (PCFD), formally known as “adult-acquired flatfoot deformity” (AAFFD), is a complex foot deformity consisting of multiple components. If surgery is required, joint-preserving procedures, such as a medial displacement calcaneal osteotomy (MDCO), are frequently performed. The aim of this systematic review is to provide a summary of the evidence on the impact of MDCO on foot biomechanics.
Materials and methods
A systematic literature search across two major sources (PubMed and Scopus) without time limitation was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) criteria. Only original research studies reporting on biomechanical changes following a MDCO were included. Exclusion criteria consisted of review articles, case studies, and studies not written in English. 27 studies were included and the methodologic quality graded according to the QUACS scale and the modified Coleman score.
Results
The 27 included studies consisted of 18 cadaveric, 7 studies based on biomechanical models, and 2 clinical studies. The impact of MDCO on the following five major parameters were assessed: plantar fascia (n = 6), medial longitudinal arch (n = 9), hind- and midfoot joint pressures (n = 10), Achilles tendon (n = 5), and gait pattern parameters (n = 3). The quality of the studies was moderate to good with a pooled mean QUACS score of 65% (range 46–92%) for in-vitro and a pooled mean Coleman score of 58 (range 56–65) points for clinical studies.
Conclusion
A thorough knowledge of how MDCO impacts foot function is key in properly understanding the postoperative effects of this commonly performed procedure. According to the evidence, MDCO impacts the function of the plantar fascia and Achilles tendon, the integrity of the medial longitudinal arch, hind- and midfoot joint pressures, and consequently specific gait pattern parameters.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Progressive collapsing foot deformity (PCFD), also known as “adult-acquired flatfoot deformity” (AAFFD), is a complex foot deformity consisting of multiple components: (1) peritalar subluxation resulting in foot deviation in various planes (e.g., hindfoot valgus, talar plantarflexion, forefoot supination); (2) abduction deformity at the level of the midfoot; and (3) forefoot varus with the first ray elevated above the fifth metatarsal [1, 2]. The etiology is still unclear, but generally involves soft tissue degeneration associated with dysfunction of the tibialis posterior tendon (PTT) [3, 4].
If surgery is required, joint-preserving procedures, such as a medial displacement calcaneal osteotomy (MDCO), are frequently performed. Calcaneal osteotomies as part of a bony reconstruction address hindfoot valgus and may also impact midfoot abduction [5,6,7]. The MDCO, first described by Gleich in 1893 [8], involves a medial translation of the entire tuber calcanei. As the lever arm of the Achilles tendon changes, such an osteotomy may have a significant effect on foot function.
Several studies assessed the impact of MDCO on foot biomechanics. Nevertheless, the understanding of MDCO on foot function is currently limited. Therefore, the aims of this systematic review are: (1) to perform a systematic literature search on studies assessing the impact of MDCO on foot biomechanics; (2) to provide an overview of the current knowledge on the effect of MDCO on foot biomechanics; and (3) to grade these studies according to their methodological quality.
Materials and methods
Search strategy and study selection
The original protocol for this systematic literature review was registered on PROSPERO, the international prospective register of systematic reviews (CRD42022270180), after performing a search on the CRD database to find out whether this review was already registered. The electronic MEDLINE database via PubMed and Scopus were systematically searched. The search was performed on the 5th of July 2021, with a final update on the 25th of January 2023. The following search algorithm was used: (calcan* [ALL] AND osteotomy [ALL]) OR (sliding AND calcan*) OR (calcaneus [MeSh] AND osteotomy [MeSh]). There were no limitations on the type of journal or article publication date. Only publications in English were included. The article bibliographies were also reviewed. Bidirectional citation search was used including backward and forward citation search methods [9]. The systematic literature search was conducted independently by three authors (GM, CS and EM) according to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guidelines [10]. Studies were included if they were original research reporting data on biomechanical changes following a MDCO. Exclusion criteria included review articles, case studies, and studies not written in English. The study selection process was performed independently by three observers (EM, GM, CS). In case of a disagreement, a final decision was made by group consensus.
Data extraction and quality assessment
The following data from the included studies were extracted: type of study, number of cadaveric specimens / number of biomechanical models / number of feet, age, biomechanical testing method (if appropriate), and the impact on foot biomechanics as primary outcome parameters. In addition, proposed therapeutic and/or surgical consequences were collected as secondary outcome parameters. Data extraction was independently performed by two review authors (GM and EM). The methodological quality of the studies including cadavers was assessed using the QUACS scale (Quality Appraisal for Cadaveric Studies; Table 1) [11]. Two reviewers (GM and CS) independently examined each included study using the checklist consisting of 13 items and reported scores as percentages. These scores were pooled and reported as an average. Clinical studies were graded using the modified Coleman score (Table 2) [12]. The modified Coleman score was applied by two independent reviewers (GM and CS). Each study was assessed for study size, follow-up time, percentage of patients with follow-up, number of interventions, study type, diagnostic certainty, description of surgical method/rehabilitation, outcome criteria/assessment process, and patient selection process.
Statistical analysis
The data were processed descriptively; therefore, no meta-analysis was performed. Patient demographic characteristics (number of patients/ feet, patient age and sex) were summarized. Weighted median scores were calculated for the modified Coleman and QUACS scores. Data analysis was performed using IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA).
Results
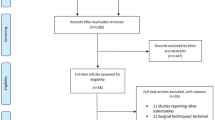
The initial database screening resulted in 1,900 studies. After removing all duplicates and screening of titles and abstracts, 157 studies were eligible for full-text review. After exclusion of 130 studies according to our exclusion criteria (review articles, incomplete data set, no information on foot biomechanics), 27 studies were ultimately included in the final analysis. The selection process was performed according to “Preferred Reporting Items for Systematic Review and Meta-Analyses” (PRISMA) and is shown in Fig. 1 [10].

Flowchart depicting the strategy used to select relevant studies
Study characteristics
The 27 included studies were published between 1995 and 2020 and contained 18 cadaveric studies, 7 studies using biomechanical models, and 2 clinical studies (Table 3). The 18 cadaveric studies included 185 cadavers (188 feet) with a pooled mean age of 65 years (range 43–96 years; age defined in 6 studies), comprised of 13 (50%) female and 13 (50%) male patients (gender defined in 4 studies). Within the 7 studies using biomechanical models, the models were based either on cadavers or MRI / CT scan datasets (including 2 Finite-Element-models). The 2 clinical studies evaluated a total of 93 patients (96 feet) with a pooled mean age of 58 years (range 43–79), comprised of 12 (13%) male and 81 (87%) female patients. Studies including cadavers had a pooled mean QUACS score of 65% (range 46–92%). The pooled mean Coleman score of the clinical studies was 58 (range 56–65) points (Table 3). Within the included studies, 4 were financially supported by different grants.
Impact on the plantar fascia
Within the included studies, 6 assessed the impact of MDCO on the plantar fascia (Table 4). Thordarson et al. showed in a cadaveric study that a transection of the plantar fascia does not affect the corrective potential of MDCO [13]. Iaquinto et al. demonstrated an 80% increase of plantar fascia strain in AAFFD patients, with a significant decrease following MDCO [14]. Similar findings were evident in the studies published by Smith et al. and Spratley et al. [15,16,17]. Horton and colleagues demonstrated that a 1 cm MDCO resulted in an average of 1.2 ± 0.5 mm shortening of the plantar fascia. This finding was confirmed by Sung et al. [18].
Impact on the medial longitudinal arch
The impact of MDCO on the medial longitudinal arch was evaluated in 9 studies (Table 5). Otis et al. analyzed the length of the spring ligament under a load of 100 N in a cadaver study. The length was comparable before and after MDCO [19]. Sung and colleagues confirmed these results in their cadaveric study [18]. Arangio et al. used a 3D biomechanical multisegmental model to analyze the effect of MDCO on the excess forces in the medial longitudinal arch. They demonstrated that MDCO with 10 mm of displacement results in a substantial shift of excess forces toward the lateral side and hereby decreases the load on the medial arch [20]. Hadfield and colleagues confirmed this finding in a cadaver study [21]. In a further study they also showed a 0.5 cm superior translation of the osteotomy to result in a greater load reduction of the first and second metatarsals [22]. Spratley et al. also showed a change in plantar force distribution with a reduce in load of the medial forefoot [17]. Smith et al. proved with patient specific computational models a decrease of plantar fascia, spring ligament, and deltoid ligament sprain loads [15]. Zanolli et al. demonstrated in a cadaveric study that an additional reconstruction of the spring ligament does not change the effect of MDCO [23]. Resnick et al. analyzed the deltoid ligament force under axial loading. Different clinical and surgical conditions were simulated. A decreased force could be detected when MDCO was combined with a triple arthrodesis [24].
Impact on joints pressure
The impact of MDCO on hind- and midfoot joint pressures was analyzed in 10 studies (Table 6). Fairbank and colleagues analyzed 11 fresh frozen cadaver legs with an axial load of 700 N which quantified the tibiotalar joint contact characteristics. The flatfoot model was associated with a shift of ankle joint pressure laterally and a quantitative alteration of the contact area compared to the normal ankle. MDCO altered the lateral contact pressure. The authors therefore concluded that MDCO might be a useful alternative to the tibiotalar arthrodesis in cases of early tibiotalar arthritis secondary to varus or valgus hindfoot deformity [25]. Havenhill et al. demonstrated similar results comparing an UCBL orthosis and MDCO in flatfoot cadavers [26]. Davitt and colleagues measured the pressure in the tibiotalar and subtalar joints in a cadaveric study after MDCO. Following a 1 cm MDCO, the average center of force shifted medially in both joints [27]. Steffensmeier and colleagues demonstrated in their cadaveric study that a 1 cm MDCO results in a shift of the pressure distribution 1.58 mm medially in the tibiotalar joint. However, the differences in contact area, mean contact stress, and maximum stress in the tibiotalar joint were not different after MDCO. Similar to the study by Davitt and colleagues [27], in this study, a slight anteromedial shift of the subtalar joint center of pressure was measured [28]. Patrick and colleagues also analyzed subtalar joint force, contact area, and peak contact pressure before and after 1 cm MDCO in 4 cadaveric specimens. After MDCO, there was a slight decrease of subtalar joint force from 211.4 N to 168.8 N, a decrease of contact area from 3.5cm2 to 3.1cm2, and a decrease of peak contact pressure from 1810 kPa to 1276 kPa. However, all observed changes were not statistically significant [29]. Arangio et al. demonstrated that pathologically increased force in the talo-navicular joint in a flatfoot model almost normalizes after MDCO. They recommended a MDCO in case of a dysfunction of the PTT [30]. Malik and colleagues confirmed these results and recommended a MDCO as an adjunct procedure in talonavicular arthrodesis for patients with a high risk of nonunion [31]. Iaquinto et al. and Spratley et al. proved in a biomechanical model a normalization of joint pressure in the calcaneo-cuboid joint after MDCO [14, 17]. Scott and colleagues and Smith and colleagues examined the effects of MDCO on joint pressures in the hind- and midfoot combined with a lateral column osteotomy [15, 32]. Scott et al. proved with their cadaveric study an increase of lateral forefoot pressures after lateral column lengthening procedures. The addition of MDCO did not lead to an alteration of plantar pressures [32]. Smith and colleagues demonstrated in 6 biomechanical models that the combination of a MDCO with an Evans Osteotomy and a MDCO with a Z-Osteotomy show the greatest amount of correction for both forefoot abduction and hindfoot valgus in a flatfoot model [15].
Impact on Achilles tendon
The impact of MDCO on the Achilles tendon was analyzed in 5 of the included studies (Table 7). Hadfield and colleagues analyzed the effect of a 1 cm MDCO on Achilles tendon length and plantar foot pressures in 14 cadaveric specimens. The length of the Achilles tendon remained the same after the osteotomy [21]. The same research group analyzed the effect of superior translation of the tuber calcanei with the same parameters. The addition of a 5 mm superior translation did not lead to Achilles tendon lengthening [22]. Nyska and colleagues established an experimental cadaveric AAFFD model by releasing the PTT, spring ligament, and plantar fascia. Applying axial load with a range between 700 and 1400 N substantially aggravated the deformity as confirmed radiographically. Adding a 1 cm MDCO reduced the arch-flattening effect of the Achilles tendon [33]. Arangio et al. proved with their biomechanical model a decreased force provided by the Achilles, flexor hallucis longus (FHL), and flexor digitorum longus (FDL) tendons in AAFFD. Adding a MDCO decreased the force exerted by the Achilles tendon while increasing the force exerted by the peroneus brevis and longus tendons [30]. Sung and colleagues loaded 13 cadaver specimens in a custom testing apparatus. Measurement of PTT force required to achieve early heel rise in an intact foot and were compared to specimens following MDCO and posterior distraction osteotomy. After MDCO, the Achilles force required to achieve the heel rise decreased [18].
Impact on gait pattern
The impact on gait pattern was analyzed in 3 studies (Table 8). Marks and colleagues analyzed gait parameters as well as radiographic alignment in 14 patients with MDCO and six patients with lateral lengthening osteotomy of the calcaneus. In both groups, a significant improvement of all gait parameters was observed. The MDCO group demonstrated improved first ray plantarflexion, while the lateral lengthening group presented with better heel inversion [34]. Michelson and colleagues examined the alteration in ankle motion after MDCO. At maximal dorsiflexion, internal rotation and varus motion increased. There was no significant difference in plantar flexion. Therefore, they hypothesized that a MDCO may predispose to premature ankle arthritis as a consequence of the altered ankle mechanics [35]. In a clinical study by Schuh et al., the authors examined 75 feet of 73 patients with posterior tibial tendon dysfunction (PTTD) stage II who underwent an FDL tendon transfer and MDCO. Plantar pressure distribution and American Orthopaedic Foot and Ankle Society (AOFAS) score were analyzed 48 months after surgery. The authors saw statistically significant correlations between the AOFAS score and loading parameters of the medial midfoot [36].
The main biomechanical consequences of the MDCO are summarized in Table 9.
Discussion
27 studies assessing the biomechanical impact of MDCO on foot function were included in the present systematic review. We found evidence that MDCO impacts function of the plantar fascia, integrity of the medial longitudinal arch, alters peritalar joint pressures, and has an influence on Achilles tendon function. Consequently, specific gait pattern parameters were found to be impacted by MDCO.
Interestingly, our analysis showed an increase of plantar fascia strain in the case of AAFFD with a drop following MDCO [14,15,16,17]. In addition, Sung et al. reported a decrease of plantar fascia length after MDCO [18]. Another study showed no impact of a plantar fascia release on the corrective potential following MDCO [13]. Therefore, an additional release of the plantar fascia may not be effective in cases where MDCO is performed.
MDCO does not change spring ligament length, while spring ligament reconstruction may not impact the expected outcome following MDCO [18, 19, 23]. However, a substantial shift of excess forces towards the lateral aspect of the longitudinal arch was found in several studies [17, 20,21,22, 30], reflecting a high strength of evidence. Resnick et al. additionally analyzed deltoid ligament force under axial load and concluded that MDCO in combination with a triple arthrodesis may be a viable treatment option when the hindfoot cannot be positioned properly following fusion procedures [24]. MDCO may not only correct hindfoot valgus deformity, but also offload the medial aspect of the foot and therefore can serve as a solution after hindfoot fusion procedures with non-union.
The studies showed a shift of the average center of force medially in the tibiotalar and subtalar joints following MDCO [27, 28]. Additionally, an overall decrease of subtalar and tibiotalar joint forces, contact area, and peak contact pressures were evident in several studies [29, 30]. These aspects of impact on joint pressure show a high strength of evidence. MDCO can therefore be recommended in case of a tibialis posterior tendon dysfunction or as an additional procedure in talonavicular arthrodesis for patients with a high risk of non-union [30, 31]. In addition, Iaquinto et al. and Spratley et al. showed a normalization of increased joint pressures in the calcaneo-cuboid joint after MDCO [14, 17].
Of note, studies have shown MDCO to not impact Achilles tendon length [21, 22], while a reduction of the arch-flattening effect of the Achilles tendon was evident in two other studies [30, 33]. Additionally, a decrease in force at the level of the Achilles tendon was required to achieve heel rise position after MDCO [18]. Consequently, an additional lengthening of the Achilles tendon when performing MDCO for PCFD reconstruction may not be required in most patients.
Specific gait pattern parameters showed significant improvement after MDCO [34]. However, in a clinical study, Schuh et al. showed that MDCO impairs function of the lesser toes during the stance phase of walking, with an increased load of the forefoot [36]. In addition, Michelson and colleagues hypothesized that MDCO may predispose to premature ankle arthritis as a consequence of altered ankle mechanics [35]. The studies evaluating gait parameters showed a moderate strength of evidence, showing the need for further research in this field. The negative effects on gait pattern parameters must be considered when MDCO is performed. Afterall, the indication for MDCO must be thoroughly evaluated to avoid these postoperative complications. Weightbearing computed tomography as a newer preoperative diagnostic tool, which presents the possibility of imaging in the physiological standing position to assess for forefoot and hindfoot alignment, could reduce the risk of negative effects of MDCO in the future [37,38,39,40,41,42,43].
Within the included studies, 18 (66,67%) make statements about the predictive value or operative consequences of the biomechanical findings, showing that knowledge about the biomechanical consequences of MDCO is important in understanding the effects of the osteotomy on the entire foot.
The presented study has some limitations. First, our findings are limited by the quality of the included studies. However, this is an inevitable limitation of systematic literature reviews and meta-analyses in general. For example, most of the included studies failed to report the educational level of the researchers. Also, most studies did not mention whether the observations were performed by one or more researchers, a possible source of bias. Second, only studies written in English were considered, excluding valuable contributions written in other languages.
Conclusion
A thorough knowledge of how MDCO impacts foot function is key in properly understanding the postoperative effects of this commonly performed procedure. There is evidence that MDCO effects the plantar fascia, medial longitudinal arch, peritalar joint pressures, Achilles tendon, and consequently specific gait pattern parameters. Future research should consider newer diagnostic tools including weightbearing computed tomography.
References
de Cesar Netto C, Deland JT, Ellis SJ (2020) Guest Editorial: Expert Consensus on Adult-Acquired Flatfoot deformity. Foot Ankle Int 41:1269–1271. https://doi.org/10.1177/1071100720950715
Schlickewei C, Barg A (2021) Calcaneal osteotomies in the treatment of Progressive collapsing Foot deformity. What are the restrictions for the Holy Grail? Foot Ankle Clin 26:473–505. https://doi.org/10.1016/j.fcl.2021.05.003
Goldner JL, Keats PK, Bassett FH 3rd, Clippinger FW (1974) Progressive talipes equinovalgus due to trauma or degeneration of the posterior tibial tendon and medial plantar ligaments. Orthop Clin North Am 5:39–51
Johnson KA, Strom DE (1989) Tibialis posterior tendon dysfunction. Clin Orthop Relat Res 196–206
Greenfield S, Cohen B (2017) Calcaneal osteotomies: pearls and pitfalls. Foot Ankle Clin 22:563–571. https://doi.org/10.1016/j.fcl.2017.04.011
de Cesar Netto LCS, Day C, Deland J, Hintermann JT, Johnson B, Myerson JE, Sangeorzan MS, Thordarson BJ, Ellis DB SJ (2020) Consensus for the indication of a Medializing Displacement Calcaneal Osteotomy in the treatment of Progressive collapsing Foot deformity. Foot Ankle Int 41:1282–1285. https://doi.org/10.1177/1071100720950747
Tennant JN, Carmont M, Phisitkul P (2014) Calcaneus osteotomy. Curr Rev Musculoskelet Med 7:271–276. https://doi.org/10.1007/s12178-014-9237-8
A. G (1893) Beitrag Zur Operativen Plattfußbehandlung. Arch Klin Chir 46(1):358–362
Hinde S, Spackman E (2015) Bidirectional citation searching to completion: an exploration of literature searching methods. PharmacoEconomics 33:5–11. https://doi.org/10.1007/s40273-014-0205-3
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Wilke J, Krause F, Niederer D, Engeroff T, Nurnberger F, Vogt L, Banzer W (2015) Appraising the methodological quality of cadaveric studies: validation of the QUACS scale. J Anat 226:440–446. https://doi.org/10.1111/joa.12292
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10:2–11. https://doi.org/10.1034/j.1600-0838.2000.010001002.x
Thordarson DB, Hedman T, Lundquist D, Reisch R (1998) Effect of calcaneal osteotomy and plantar fasciotomy on arch configuration in a flatfoot model. Foot Ankle Int 19:374–378. https://doi.org/10.1177/107110079801900606
Iaquinto JM, Wayne JS (2011) Effects of surgical correction for the treatment of adult acquired flatfoot deformity: a computational investigation. J Orthop Res 29:1047–1054. https://doi.org/10.1002/jor.21379
Smith BA, Adelaar RS, Wayne JS (2017) Patient specific computational models to optimize surgical correction for flatfoot deformity. J Orthop Res 35:1523–1531. https://doi.org/10.1002/jor.23399
Horton GA, Myerson MS, Parks BG, Park YW (1998) Effect of calcaneal osteotomy and lateral column lengthening on the plantar fascia: a biomechanical investigation. Foot Ankle Int 19:370–373. https://doi.org/10.1177/107110079801900605
Spratley EM, Matheis EA, Hayes CW, Adelaar RS, Wayne JS (2015) Effects of Degree of Surgical correction for Flatfoot deformity in patient-specific computational models. Ann Biomed Eng 43:1947–1956. https://doi.org/10.1007/s10439-014-1195-1
Sung IH, Lee S, Otis JC, Deland JT (2002) Posterior tibial tendon force requirement in early heel rise after calcaneal osteotomies. Foot Ankle Int 23:842–849. https://doi.org/10.1177/107110070202300912
Otis JC, Deland JT, Kenneally S, Chang V (1999) Medial arch strain after medial displacement calcaneal osteotomy: an in vitro study. Foot Ankle Int 20:222–226. https://doi.org/10.1177/107110079902000403
Arangio GA, Salathe EP (2001) Medial displacement calcaneal osteotomy reduces the excess forces in the medial longitudinal arch of the flat foot. Clin Biomech (Bristol Avon) 16:535–539 DOI 10.1016/s0268-0033(01)00011 – 0
Hadfield MH, Snyder JW, Liacouras PC, Owen JR, Wayne JS, Adelaar RS (2003) Effects of medializing calcaneal osteotomy on Achilles tendon lengthening and plantar foot pressures. Foot Ankle Int 24:523–529. https://doi.org/10.1177/107110070302400703
Hadfield M, Snyder J, Liacouras P, Owen J, Wayne J, Adelaar R (2005) The effects of a medializing calcaneal osteotomy with and without superior translation on Achilles tendon elongation and plantar foot pressures. Foot Ankle Int 26:365–370. https://doi.org/10.1177/107110070502600504
Zanolli DH, Glisson RR, Nunley JA 2nd, Easley ME (2014) Biomechanical assessment of flexible flatfoot correction: comparison of techniques in a cadaver model. J Bone Joint Surg Am 96:e45. https://doi.org/10.2106/JBJS.L.00258
Resnick RB, Jahss MH, Choueka J, Kummer F, Hersch JC, Okereke E (1995) Deltoid ligament forces after tibialis posterior tendon rupture: effects of triple arthrodesis and calcaneal displacement osteotomies. Foot Ankle Int 16:14–20. https://doi.org/10.1177/107110079501600104
Fairbank A, Myerson MS, Fortin S, Yu-Yahiro J (1995) The effect of calcaneal osteotomy on contact characteristics of the tibiotalar joint. Foot 5:137–142
Havenhill TG, Toolan BC, Draganich LF (2005) Effects of a UCBL orthosis and a calcaneal osteotomy on tibiotalar contact characteristics in a cadaver flatfoot model. Foot Ankle Int 26:607–613. https://doi.org/10.1177/107110070502600806
Davitt JS, Beals TC, Bachus KN (2001) The effects of medial and lateral displacement calcaneal osteotomies on ankle and subtalar joint pressure distribution. Foot Ankle Int 22:885–889. https://doi.org/10.1177/107110070102201105
Steffensmeier SJ, Saltzman CL, Berbaum KS, Brown TD (1996) Effects of medial and lateral displacement calcaneal osteotomies on tibiotalar joint contact stresses. J Orthop Res 14:980–985. https://doi.org/10.1002/jor.1100140619
Patrick N, Lewis GS, Roush EP, Kunselman AR, Cain JD (2016) Effects of Medial Displacement Calcaneal Osteotomy and Calcaneal Z Osteotomy on Subtalar Joint pressures: a cadaveric flatfoot model. J Foot Ankle Surg 55:1175–1179. https://doi.org/10.1053/j.jfas.2016.07.009
Arangio GA, Salathe EP (2009) A biomechanical analysis of posterior tibial tendon dysfunction, medial displacement calcaneal osteotomy and flexor digitorum longus transfer in adult acquired flat foot. Clin Biomech (Bristol Avon) 24:385–390. https://doi.org/10.1016/j.clinbiomech.2009.01.009
Malik A, Grant E, Rhodenizer J (2020) Analysis of Micromotion in a Talonavicular Arthrodesis with and without a calcaneal displacement osteotomy in a Cadaver Model. J Foot Ankle Surg 59:91–94. https://doi.org/10.1053/j.jfas.2018.10.007
Scott AT, Hendry TM, Iaquinto JM, Owen JR, Wayne JS, Adelaar RS (2007) Plantar pressure analysis in cadaver feet after bony procedures commonly used in the treatment of stage II posterior tibial tendon insufficiency. Foot Ankle Int 28:1143–1153. https://doi.org/10.3113/FAI.2007.1143
Nyska M, Parks BG, Chu IT, Myerson MS (2001) The contribution of the medial calcaneal osteotomy to the correction of flatfoot deformities. Foot Ankle Int 22:278–282. https://doi.org/10.1177/107110070102200402
Marks RM, Long JT, Ness ME, Khazzam M, Harris GF (2009) Surgical reconstruction of posterior tibial tendon dysfunction: prospective comparison of flexor digitorum longus substitution combined with lateral column lengthening or medial displacement calcaneal osteotomy. Gait Posture 29:17–22. https://doi.org/10.1016/j.gaitpost.2008.05.012
Michelson JD, Mizel M, Jay P, Schmidt G (1998) Effect of medial displacement calcaneal osteotomy on ankle kinematics in a cadaver model. Foot Ankle Int 19:132–136. https://doi.org/10.1177/107110079801900303
Schuh R, Gruber F, Wanivenhaus A, Hartig N, Windhager R, Trnka HJ (2013) Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for the treatment of stage II posterior tibial tendon dysfunction: kinematic and functional results of fifty one feet. Int Orthop 37:1815–1820. https://doi.org/10.1007/s00264-013-2071-6
Barg A, Bailey T, Richter M, de Cesar Netto C, Lintz F, Burssens A, Phisitkul P, Hanrahan CJ, Saltzman CL (2018) Weightbearing Computed Tomography of the Foot and Ankle: Emerging Technology Topical Review. Foot Ankle Int 39:376–386. https://doi.org/10.1177/1071100717740330
Lintz F, de Cesar Netto C, Barg A, Burssens A, Richter M, Weight Bearing CTISG (2018) Weight-bearing cone beam CT scans in the foot and ankle. EFORT Open Rev 3:278–286. https://doi.org/10.1302/2058-5241.3.170066
Richter M, Lintz F, de Cesar Netto C, Barg A, Burssens A (2020) Results of more than 11,000 scans with weightbearing CT - impact on costs, radiation exposure, and procedure time. Foot Ankle Surg 26:518–522. https://doi.org/10.1016/j.fas.2019.05.019
Burssens A, Barg A, van Ovost E, Van Oevelen A, Leenders T, Peiffer M, Bodere I, Weightbearing CTISG, Audenaert E, Victor J (2019) The hind- and midfoot alignment computed after a medializing calcaneal osteotomy using a 3D weightbearing CT. Int J Comput Assist Radiol Surg 14:1439–1447. https://doi.org/10.1007/s11548-019-01949-7
Peiffer M, Belvedere C, Clockaerts S, Leenders T, Leardini A, Audenaert E, Victor J, Burssens A, Wbct ISG (2020) Three-dimensional displacement after a medializing calcaneal osteotomy in relation to the osteotomy angle and hindfoot alignment. Foot Ankle Surg 26:78–84. https://doi.org/10.1016/j.fas.2018.11.015
Krahenbuhl N, Kvarda P, Susdorf R, Burssens A, Ruiz R, Barg A, Hintermann B (2022) Assessment of Progressive collapsing Foot Deformity using semiautomated 3D measurements derived from weightbearing CT scans. Foot Ankle Int 43:363–370. https://doi.org/10.1177/10711007211049754
Kvarda P, Krahenbuhl N, Susdorf R, Burssens A, Ruiz R, Barg A, Hintermann B (2022) High reliability for semiautomated 3D measurements based on Weightbearing CT scans. Foot Ankle Int 43:91–95. https://doi.org/10.1177/10711007211034522
Funding
No funding received.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No conflicts.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mueller, G., Frosch, KH., Barg, A. et al. Impact of the medial displacement calcaneal osteotomy on foot biomechanics: a systematic literature review. Arch Orthop Trauma Surg 144, 1955–1967 (2024). https://doi.org/10.1007/s00402-024-05267-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-024-05267-9