
Abstract
Purpose
The optimal screw placement in arthroscopically assisted fixation of radial head fractures is still an issue and no guiding methods have been evaluated in the recent literature. The study hypothesis was that using a “reference k-wire” percutaneously inserted in and parallel to the radiocapitellar joint would enable to achieve a trajectory more parallel to the radial head articular surface as compared to a free-hand k-wire placement.
Methods
Arthroscopically assisted placement of a k-wire in the radial head was performed in seven fresh-frozen human cadaver specimens by three surgeons. Three different techniques were evaluated: freehand drilling (technique A), placement using a “reference” k-wire in the radiocapitellar joint as a reference without (technique B), and with the AO parallel k-wire guide (technique C). Radiographs from all procedures were obtained and the inclination angle “α” between the k-wire and the articular surface of the radial head was measured and compared among the techniques.
Results
Angles of 84 radiographs were obtained and showed a mean α angle of 30.1° ± 13° for technique A, 5.7° ± 4.5° for technique B, and 5.4° ± 3.7° for technique C. The angle α was significantly higher with technique A as compared to B (p < 0.0001) and C (p < 0.0001). There was no difference between methods B and C (n.s.). No difference was observed among the surgeons for all three methods (p = 0.66).
Conclusion
With the use of an additional “reference” k-wire placed in the radiocapitellar joint, the guiding k-wire for screw drilling can be placed almost parallel to the radial head joint line with limited variability and a good reproducibility during arthroscopically assisted radial head fracture fixation.
Clinical relevance
The here-presented method of an additional, percutaneous introduced “reference” k-wire is easily applicable and helpful to achieve parallel screw placement during arthroscopically assisted radial head fracture fixation.
Level of evidence
IV, biomechanical cadaver study
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The radial head is crucial for the stability and function of the elbow joint [1,2,3]. For the treatment of radial head fractures arthroscopic-assisted techniques for fixation, in specific fracture types, are gaining popularity and present advantages compared to the classic open approach [4,5,6]. Arthroscopy offers potential for better visualization of the articular surface and, with it, improved understanding of the fracture morphology. With this opportunity, a more precise anatomical reduction of the articular surface and the simultaneous treatment of concomitant injuries are potentially possible [5].
Different cadaver studies [7, 8] showed a possible exposure of the whole radial head circumference with standard arthroscopic portals for adequate screw placement. Screw placement is the crucial step in fixation of radial head fractures. As known from traumatology principles, increased primary stability of screws is achieved when they are placed perpendicular to the fracture line [9]. Most radial head fractures type I and II according to the Mason classification [10] modified by Hotchkiss [11] are partial intra-articular fractures: in these cases, axial, valgus, and external rotatory loading at the radiocapitellar joint leads to shearing of the radial head resulting in an intra-articular fracture in which in most cases the fracture line is perpendicular to the radial head articular surface, as described by Gordon et al. [12]. Hereby, the perfect screw inclination would be at an angle of 0° to the radial head articular surface.
Positioning the guide wire can be difficult during elbow arthroscopy since only a two-dimensional view of the radial head is provided and determining the radial longitudinal axis is challenging. Malpositioning of the k-wire can lead to increased surgical time, a higher amount of X-ray radiation to patient and surgeon, and at last improper screw placement. The purpose of this study was to evaluate the performance of two guiding methods and compare them to a free-hand technique of k-wire placement in a cadaveric elbow arthroscopy situation. The study hypothesis was that using a “reference k-wire” inserted in the radiocapitellar joint as a reference for “guide k-wire” placement would enable to achieve a trajectory more parallel to the radial head articular surface as compared to a free-hand k-wire placement. The possible role of an AO parallel k-wire guide in assisting k-wire placement was also evaluated.
Materials and methods
This cadaver study was approved by the institutional review board (21-1118). For the present study, seven fresh-frozen cadaver specimens of upper extremities from human donors were used (females: 57%; right elbows: 57%; median age at death: 76 years). The specimens were evaluated for visible or radiological signs of previous trauma or deformity.
Three treatment groups were defined for subsequent comparison (techniques A, B, and C). Technique A consisted in free-hand positioning of a 2.0 mm guide k-wire in the radial head under sole visual arthroscopic control. For technique B, firstly, a “reference k-wire” was positioned percutaneously in the radiocapitellar joint and used as a reference to place the guide k-wire in the radial head. In technique C the “reference k-wire” was positioned percutaneously in the radiocapitellar joint (in the same way as in technique B) and, additionally, the AO parallel k-wire guide was used to drill the guide k-wire in the radial head.
All seven obtained specimens were allocated in a random sequence to each of the three treatment groups so that a sequence of 21 procedures was generated before the study begin. All three procedures were performed in each of the seven specimens.
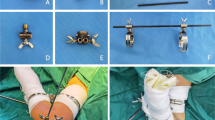
Standard arthroscopy (Synergy, Arthrex, Naples, FL, USA) was performed with the elbow positioned at 90° of flexion, imitating patient positioning in lateral decubitus (Fig. 1). A high posterolateral portal was established for diagnostic arthroscopy. If necessary, an intra-articular debridement with a shaver was performed for better visualization via a standard anterolateral portal. After a single trial of positioning of the guide k-wire with the desired technique, an x-ray with a strict lateral view of the radial head and in the plane of the inserted guide k-wire was obtained with digital fluoroscopy (Fluoroscan Insight-FD Mini, Hologic Medicor GmbH, Kerpen, Germany).

Drilling the guiding k-wire into the radial head without (A) and with an AO parallel k-wire guide (B). Arthroscopic view of the radiocapitellar joint (Ca capitellum; Rh radial head) through a high posterolateral portal (left A, right B) while placing a “reference” k-wire into the radiocapitellar joint from the lateral soft-spot portal
After being instructed on the treatment groups and procedures, three orthopedic surgeons (RSC, DC, KW) performed each of the three techniques on the seven specimens in one sequence of 21 arthroscopies: these procedures were evaluated to assess inter-rater reliability; furthermore, to assess intra-rater reliability of the procedure, the most experienced of the three surgeons (KW) performed a second sequence of 21 arthroscopies 4 h after the first sequence. To avoid repeated perforations of the radial head at the same k-wire insertion point, the elbow was fixed in different pronation and supination positions.
The inclination angle “α” between the guide k-wire and the articular surface of the radial head was determined on digital radiographs with two decimals accuracy using dedicated software (GeoGebra 6.0.620, Hohenwarter et al., http://www.geogebra.org, 2020) (Fig. 2).

Radiographs after placement of the guiding k-wire with the corresponding measurement of the inclination angle α. Radiograph after free-hand placement of the guiding k-wire in the radial head (A) showing an inclination angle of 51° (B), and radiograph after using a reference k-wire in the radiocapitellar joint without parallel k-wire guide (C) and an almost parallel guide k-wire in the radial head (D)
Two examiners blinded to the group allocation of the radiographs (RSC, DC) analyzed all radiographs independently. Before the study, both observers were instructed about the measurement techniques. Two weeks after the initial measurement, one surgeon (RSC) re-measured all inclination angle α to evaluate the intra-observer reliability of the radiographic measurement.
Statistical analysis
Based on the previously published data concerning screw placement in radial head fractures [7], an a priori power analysis was calculated to detect a significant difference between two different angles using the freely available software G*Power 3 (Erdfelder, Faul, Buchner, Lang, HHU Düsseldorf, Düsseldorf, Germany). A sample size of at least 6 elbows with an α = 0.05 for a power of 95% was established to detect a change between two angles (two-sided t-test for two different groups).
Reliability was evaluated using intraclass correlation coefficients (ICCs) and a two-way mixed-effect model assuming a single measurement and absolute agreement.
Calculated means from both readers were then used to analyze and present data. Normal distribution of the data was tested with a Kolmogorov–Smirnov test. Parametric (paired t-test) or non-parametric t-tests (Wilcoxon matched-pairs signed-rank test) were applied to compare the different conditions. To evaluate the differences among the methods one-way analysis of variance (ANOVA) was performed.
The significance level was set at 0.05 and the results are reported as means with standard deviation if not stated otherwise. The statistical analyses were computed using MedCalc Statistical Software version 19.6 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org; 2020).
Results
Angles of 84 radiographs were obtained and analyzed. Inter- and intra-observer reliability of the measurement of the inclination angle α measured with ICC was 0.9855 (95% CI 0.9774–0.9906) and 0.9834 (95% CI 0.9673–0.9907) respectively.
With the technique A, a mean α angle of 30.1° ± SD 13 was obtained by the three surgeons; with the technique B the mean α angle dropped to 5.7° ± SD 4.5° and with the technique C to 5.4° ± 3.7 (Fig. 3). A significant difference was observed when comparing technique A to both technique B (p < 0.0001) and C (p < 0.0001). There was no difference between techniques B and C (p: n.s.). No difference was observed among the three surgeons (n.s.), neither for technique A (n.s.), B (n.s.) or C (n.s.). Inter-observer reliability measured with ICC for method A was 0.6097 (95% CI − 0.07 to 0.92), method B 0.7319 (95% CI 0.08–0.95) and method C 0.7652 (0.29–0.95). Intra-observer reliability for the second sequence of the senior author (KW) showed an ICC of 0.7781 (95% CI 0.46–0.91).

Boxplot of the inclination angle α with the three techniques: A free-hand drilling, B using a “reference” k-wire in the radiocapitellar joint, and C additional AO parallel k-wire guide for the drilling of the guide k-wire
No damage to the radiocapitellar cartilage was observed arthroscopically during the study period.
Discussion
The main finding of this study is that the use of an additional “reference” k-wire in the radiocapitellar joint can support to drilling the definitive guide k-wire for the cannulated screw with less variability and almost parallel to the radial head joint line with good reproducibility during arthroscopic-assisted radial head fracture fixation. A high agreement between surgeons can be achieved either by using the k-wire as a simple reference or with the additional use of the AO parallel k-wire guide.
Arthroscopy of acute elbow trauma is becoming more and more popular and has its role in the fixation of radial head fractures [13]. Arthroscopy allows direct visualization of the fracture and with this perfect reduction of this articular fracture can be verified [14]. Further advantages are reduced surgical trauma to the soft tissue compared to an open approach, the possibility to address other intra-articular soft-tissue lesions, and evacuation of loose bodies in the elbow joint. Clinical results of arthroscopic-assisted osteosynthesis are encouraging [6, 15, 16].
The techniques presented here can help surgeons place the guide wires for cannulated screw in a more parallel trajectory to the radial head articular surface (inclination angle α tend towards zero), herewith potentially enhancing the biomechanical performance of fixation and facilitating arthroscopic-assisted fracture management of radial head fractures. Surgical treatment of radial head fracture is indicated in some Mason type II, type III, and IV fractures while only Mason type II fractures so far allow an arthroscopic-assisted approach. Two-part fractures with the fracture fragment still close to the radial head articular surface are ideal candidates for arthroscopic surgery. Fragments which are dislocated outside the radiocapitellar joint usually are not amenable to being addressed by arthroscopic techniques [17].
In a cadaver study analyzing the inclination angle α of a k-wire introduced by different arthroscopic standard portals, Cucchi et al. [18] showed a mean α angle ranging from 14° to 25° obtained from the medial, 17° from the anterolateral, and − 2.6 for the more distal portal. The authors concluded a more parallel trajectory of the screw about the radial head surface is desirable to achieve superior biomechanical stability. With the here-presented additional “reference k-wire” in the radiocapitellar joint, an α angle very close to 0° (5.7° without and 5.4° with the AO parallel k-wire guide) could be achieved. Notably, the standard deviation documented in the present study using the “reference k-wire” was markedly lower (less than 5°) than the standard deviation reported both without the “reference k-wire” and that documented in the previously cited study (both 13°), suggesting a reduced variability of k-wire placement with the newly proposed technique. The application of this additional k-wire is easy, time-saving, cheap and even for inexperienced arthroscopists easily applicable. Through the soft-spot portal, or wherever the fracture line demands its placement, the k-wire can be introduced and pushed forward to the anterior elbow joint. The correct position of this wire can be assessed arthroscopically and the direction of the wire macroscopically. Care should be taken not to advance this sharp instrument too far anteriorly to avoid damage to the neurovascular structures. Moreover, the surgeon must take care, that the k-wire is not bent by the soft tissues, which would compromise the guiding effect. Further, excessive distalization of the lateral portal should be avoided and pronation of the forearm while cutting/screwing from the lateral is warranted to displace the posterior interosseous nerve medially and thus increase safety.
The high variety and the steep inclination angle obtained with the free-hand k-wire technique underline the necessity for an improved technique. Several factors add to the difficulty of free-hand k-wire placement, like soft-tissue entanglement around the k-wire, blurred vision by fracture hematoma, and resistance to placement by the annular ligament. The annular ligament reaches up to the articular surface of the radial head and is tightly fit around the radial head. To be able to place the k-wire at the correct depth to avoid intra-articular placement, the guiding k-wire must be placed at about 6–8 mm below the radial head surface. Therewith, its entry point can be blocked by the annular ligament. In a conventional technique, the k-wire needs to pull down the annular ligament to gain visibility on the entry point. In the author’s perception, this step mainly adds to misplacement and variability in the α angle. With the described techniques B and C, this step is avoided, as the “reference” k-wire dictates the direction of the guiding k-wire, which can thus be easily placed also through the annular ligament.
Limitations
There are several limitations of this study. First, this is an anatomic cadaver study and all portals were placed by a single, experienced surgeon. In a real surgical setup, the position of the standard portals may differ based on the surgeons’ preferences. Furthermore, the experimental setup did not include the fracture reduction into account. Arthroscopic management in an acute trauma case can be much more difficult and is highly demanding and advanced skills in elbow arthroscopy are needed. Third, there is a high risk of bias by repeated use of the different specimens, and perforating the radial head several times with a 2.0 mm k-wire. To avoid introducing the k-wire in the previous perforation, the elbow was fixed in different pronated and supinated positions. Fourth, the parallelism of osteosynthetic screws to the radial head articular surface is not known to correlate with superior clinical outcomes, nor is this stated by the authors. The authors merely proclaim known biomechanical basics, which offer improved primary stability if screws are placed perpendicular to the fracture line. But even more, the present paper does not focus on the potential superiority of a specific k-wire position but wants to display the feasibility of a simple technique for navigated k-wire placement. This study shows within its limitation that the definitive screw placement can be navigated using simple tools.
Conclusion
With the use of an additional “reference” k-wire placed in and parallel to the radiocapitellar joint, the k-wire for consecutive screw drilling can be navigated, resulting in an almost parallel position about the radial head joint line, with good reproducibility during arthroscopically assisted radial head fracture fixation.
References
Hackl M, Wegmann K, Kahmann SL, Heinze N, Staat M, Neiss WF, Scaal M, Müller LP (2017) Radial shortening osteotomy reduces radiocapitellar contact pressures while preserving valgus stability of the elbow. Knee Surg Sport Traumatol Arthrosc 25(7):2280–2288
Orbay JL, Mijares MR, Berriz CG (2016) The transverse force experienced by the radial head during axial loading of the forearm: a cadaveric study. Clin Biomech 31:117–122
Hilgersom NFJ, Eygendaal D, van den Bekerom MPJ (2017) Disadvantages of having a shortening of the proximal radius. Knee Surg Sport Traumatol Arthrosc 25:3326–3327
Atesok K, Doral NN, Whipple T, Mann G, Mei-Dan O, Atay AA, Beer Y, Lowe J, Soudry M, Schemitsch EH (2011) Arthroscopy-assisted fracture fixation. Knee Surg Sport Traumatol Arthrosc 19(2):320–329
Haasters F, Helfen T, Böcker W et al (2019) The value of elbow arthroscopy in diagnosing and treatment of radial head fractures. BMC Musculoskelet Disord 20:343. https://doi.org/10.1186/s12891-019-2726-6
Michels F, Pouliart N, Handelberg F (2007) Arthroscopic management of Mason type 2 radial head fractures. Knee Surg Sport Traumatol Arthrosc 15(10):1244–1250
Cucchi D, Guerra E, Luceri F, Lenich A, Nicoletti S, Randelli P, Wirtz DC, Eygendaal D, Arrigoni P (2019) A combination of an anteromedial, anterolateral and midlateral portals is sufficient for 360° exposure of the radial head for arthroscopic fracture fixation. Knee Surg Sport Traumatol Arthrosc 27(1):319–325
Hodax JD, Blood TD, Kleinhenz DT, Gorman M, Biercevicz A, DaSilva M (2017) An anatomic evaluation of arthroscopic access to the radial head. Arthrosc J Arthrosc Relat Surg 33(5):953–958
Ruedi TP, Buckley R, Moran C (2007) AO principles of fracture management. Georg Thieme Verlag, Stuttgart
Mason ML (1954) Some observations on fractures of the head of the radius with a review of one hundred cases. Br J Surg 42:123–132
Hotchkiss (1997) Displaced fractures of the radial head: internal fixation or excision? J Am Acad Orthop Surg 5(1):1–10
Gordon KD, Duck TR, King GJW, Johnson JA (2003) Mechanical properties of subchondral cancellous bone of the radial head. J Orthop Trauma 17(4):285–289
van Tongel A, Macdonald P, van Riet R, Dubberley J (2012) Elbow arthroscopy in acute injuries. Knee Surg Sport Traumatol Arthrosc 20:2542–2548
Rolla PR, Surace MF, Bini A, Pilato G (2006) Arthroscopic treatment of fractures of the radial head. Arthrosc J Arthrosc Relat Surg 22(2):233.e1-233.e6
Wang J, Qi W, Shen X, Tao S, Liu Y (2018) Results of arthroscopic fixation of Mason type II radial head fractures using Kirschner wires. Med 97(12):201
Wang J, Liu Y, Zhongli L, Wang Z, Wei M (2012) Arthroscopic poking reduction and internal fixation of radial head fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 26(2):208–211
Thès A, Hardy P (2016) Elbow fractures treatment. In: Randelli P, Dejour D, van Dijk CN et al (eds) Arthroscopy. Springer Berlin Heidelberg, Berlin, pp 725–732
Cucchi D, Arrigoni P, Luceri F, Menon A, Guerra E, Müller LP, Burger C, Eygendaal D, Wegmann K (2019) Modified anteromedial and anterolateral elbow arthroscopy portals show superiority to standard portals in guiding arthroscopic radial head screw fixation. Knee Surg Sport Traumatol Arthrosc 27(10):3276–3283
Acknowledgements
We would like to thank Jutta Knifka (Department of Orthopedic and Trauma Surgery, University of Cologne, Cologne, Germany) for her help and technical assistance with the experimental setup.
Funding
Open access funding provided by University of Zurich. Not applicable, no financial bias exists for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There were no conflict of interest for RSC, TL, DC and MH. LPM and KW have an advisory contract and receives consultant payments from Medartis, Arthrex and Tornier, which are not related to the subject of this work. There was no outside funding or grants received that assisted in this study.
Ethical approval
Institutional review board approval was obtained from the Ethics Committee of the University of Cologne, Cologne, Germany (Reference number 21-118).
Informed consent
Informed consent was given by all donors who have willed their body to science during their lifetime.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Camenzind, R.S., Cucchi, D., Leschinger, T. et al. Screw placement in arthroscopically assisted osteosynthesis of radial head fractures using a reference k-wire in the radiocapitellar joint: a cadaveric study. Arch Orthop Trauma Surg 143, 4111–4116 (2023). https://doi.org/10.1007/s00402-022-04605-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-022-04605-z