
Abstract
Background
Due to the surge of COVID-19 cases in the US in early March 2020, health care facilities temporarily suspended elective and non-urgent medical procedures such as joint replacement surgeries. The aim of this study was to analyze the impact of the COVID-19 associated shutdown on orthopedic patient care at a specialized orthopedic hospital located at the epicenter of the COVID-19 pandemic.
Methods
Patient volume of outpatient visits and joint replacement surgeries were analyzed and compared for 2019 and 2020. The volumes were further aligned with the timeline of governmental and institutional COVID-19 associated restrictions.
Results
The annual surgery volume was reduced by 20.2% in 2020 and did not make up for the reduction experienced during the shutdown. The total number of patient visits decreased by 25.5% and new patient visits remained 25% lower at the end of 2020. Patient care and surgery volume recovered with declining SARS-CoV-2-cases but did not return to levels prior to the shutdown. During the second quarter of 2020, 28.5% of all patient visits were telehealth appointments. By the end of the year it dropped to 7.6%. There was a shift towards patient appointments at outpatient satellite offices.
Conclusion
Orthopedic providers faced a substantial disruption in outpatient and surgical volume. Telemedicine appointments were crucial for maintaining follow-up patient care and will be an important sector in future patient care. There has been a major push to utilize satellite offices outside the city center.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As reaction to the skyrocketing numbers of SARS-CoV-2 positive cases in the US in early March 2020, the Centers for Medicare & Medicaid Services (CMS) advised health care facilities to postpone all non-urgent medical procedures including elective surgeries [1]. Detailed guidelines were provided by the American College of Surgeons (ACS) on March 24th 2020 [2] and the delay of elective surgeries such as total joint replacements (TJR), was also encouraged by the American Academy of Orthopaedic Surgeons (AAOS). Early in the pandemic, New York State faced high numbers of confirmed COVID-19 cases and COVID-19-related deaths. Consequently, New York hospitals, including specialized orthopedic hospitals, stopped elective patient care to prepare care units for the expected surge of COVID-19 patients.
Once the COVID-19 situation had calmed down, health care facilities aimed to restore patient care cautiously under the guidance of the Governor and in compliance with public health strategies. Strict step-by-step protocols for elective surgeries were established and comprised COVID-19-screening-tools, mandatory COVID-19 testing before admission and limited patient capacity to accommodate physical distancing. Preference was given to high-urgency procedures and low-risk patients. Reopening was strictly subject to the local rates of infection, rates of COVID-19-related hospital admissions and deaths, as well as the availability of personnel and personnel protective equipment (PPE) [3].
One way physicians adapted to the changing environment was by offering telehealth appointments [4, 5]. The pandemic challenged healthcare facilities to quickly develop telehealth platforms and consequently resulted in greater availability and broader acceptance of virtual healthcare [6, 7]. Telemedicine offers decreased risk of exposure and greater flexibility for patients and physicians.
A nationwide Medicare-based analysis reported an initial drop in primary total joint replacements by 92–94% [8] and according to a survey by the American Association of Hip & Knee Surgeons (AAHKS) 70–90% of their questioned members reported a decreased surgery volume [9].
The aim of this study was to quantify the impact of the COVID-19 associated shutdown on orthopedic patient care at the joint replacement service of a specialized orthopedic hospital located at the epicenter of the COVID-19 pandemic. The study assesses the reduction in surgical volume, office visits and its impact on the utilization of telehealth care as well as satellite offices outside the main hospital campus.
Materials and methods
This retrospective study was approved by the Institutional Review Board (IRB). Daily volume data from 2019 and 2020, including hip and knee arthroplasty procedures, outpatient visits, and imaging studies, were pulled and analyzed from a universal electronic medical record system (EPIC) at a single subspecialty orthopedic hospital. For a comparison of different time periods, each year was divided into quarters.
Data analysis was performed in a descriptive manner. The daily number of surgeries (primary and revision hip and knee arthroplasty) was plotted against the number of positive SARS-CoV-2 cases in New York State Area. These numbers were obtained by the website of ‘The COVID-19 Tracking Project’ [10]. Additionally, the mean number of surgeries performed daily (weekend and public holidays excluded) was determined for each quarter and then compared between 2019 and 2020 using Mann–Whitney-U-test as data distribution was non-parametric.
Outpatient visits were characterized by the type of visit (new patient (NP) vs. follow-up (FU) visit, office visit vs. telehealth appointment) and by the location of visit (on-site = main hospital campus vs. satellite-sites = Uniondale/ Long Island, Westchester, Paramus, Stamford). Additionally, we analyzed the number of imaging procedures (MRI, CT, X-ray, ultrasound) and trends in location. To rule out confounding factors, data stemming from surgeons that had been working for less than 2 years (n = 8) or were about to retire (n = 3) were removed. Furthermore, data for the imaging procedures performed either during surgery or at the preoperative holding area were excluded. All analyses were performed in R (version 4.0.3) and Microsoft Office Excel.
Results
Surgical volume
In 2019, a total of 9.734 hip and knee arthroplasty procedures were performed at the author’s institution. In 2020, a total of 7.764 procedures were performed for a volume reduction of 20.2%. In 2019, the median number of hip and knee replacement surgeries performed per weekday (holidays and weekend excluded) was 38. Significantly less surgeries per weekday were performed during the second quarter of 2020, in which the daily surgical volume was reduced by 74.0% to nine surgeries per day (Fig. 1).

compares the average number of surgeries performed per weekday for each quarter between 2019 (light-grey) and 2020 (dark-grey). The daily surgical volume was significantly reduced during the second quarter of 2020 (9.5 [1.0, 26.5] vs 38 [33,43]; p < 0.01*) but not during the first quarter (38 [31, 43.25] vs 36.5 [19.25, 42]; p = 0.13), third quarter (37 [29.5, 44] vs 37 [31,40.75]; p = 0.69) and fourth quarter (38.5 [32.25,44.75] vs 38 [29,42]; p = 0.44)
It was not until the end of July that surgeries returned to a level comparable to 2019. During the remaining year of 2020, the volume increased, however did not exceed the numbers of 2019. Though not significant, there was a slow downward trend for the surgical volume by the end of 2020. This may most likely be attributed to the onset of the second infection wave, as mirrored by the re-rise of the curve of SARS-CoV-2 positive cases starting October 2020 (Fig. 2).

Number of surgeries performed (black line) plotted against the daily increase in positive SARS-CoV-2-cases (dotted line). Left y-axis is the scale for the number of surgeries, the right y-axis is the scale for the daily increase in positive tested SARS-CoV-2-cases in New York State Area. Number of surgeries decreased with the increase of positive SARS-CoV-2 cases
Outpatient visits
Follow-up and new patient visits
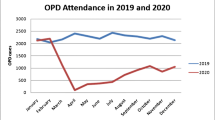
Compared to the year before the COVID-19 pandemic, the number of outpatient visits dropped by 25.5% from 44.526 to 33.177 (Table 1). The greatest difference was reported for the second quarter, during the shutdown. During this time period, only emergencies were treated. Fewer patient visits were observed during the remaining year in 2020. The shortfall of patient visits gradually recovered over time, but numbers did not return to the previously maintained levels of 2019. Follow-up visits had recovered better by the end of 2020, than new patient visits (Fig. 3).

Number of follow-up (light-grey) and new patient visits (dark-grey) performed at offices and using telehealth (dotted lines) over time. Virtual visits were hardly established before the pandemic. Follow-up visits recovered better than new patient visits. By the end of 2020, the number of new patient visits was by 25% lower than in the previous year
Main hospital campus vs satellite sites
There was a push towards patient visits at satellite sites. In 2019, 86.2% of all patient visits took place at the main campus in Manhattan and 13.8% at one of the satellite locations (Long Island, Westchester, Stamford, Paramus) (Table 2). The number of outpatient visits at the main hospital campus during 2020 decreased by more than a third, while the number of outpatient visits at satellite locations decreased by only 3.1%. Orthopedic surgeons were limited to see their patients once a week, with a limit of three patients per hour and preference for physical visits was given to satellite sites. 19.3% of all office visits after the shutdown occurred at one of the satellite locations and the percentage of satellite patient visits continued to increase towards the end of 2020 (Fig. 4).

Columns portray the percentage of visits provided at the Manhattan Main Campus (dark-grey) vs. at satellite sites (grey) vs telehealth visits (light-grey) out of the total number of visits provided during the respective quarter, for each quarter. Starting June 2020, the number of visits at satellite sites continuously increased over time, while the number of visits at the Main Campus remained at a lower level. Virtual visits peaked after the shutdown and evened out around 7.6%
Telemedicine
In 2019, there were only two telehealth appointments. In 2020, this number increased substantially for new patient and follow-up visits. 12.8% of all patient visits after the shutdown in 2020 were telehealth appointments and the demand for telemedicine reached its peak in the weeks following the COVID-19 shutdown. A new telehealth platform was established by the author’s institution and 28.5% of all visits during the second quarter were virtually provided. The percentage of virtual patient visits stabilized around 7.6% by the end of the year (Fig. 4).
Imaging procedures
The number of imaging procedures (X-rays, MRIs, CT scans, ultrasounds) performed during 2020 reduced by 20.3% compared to 2019. The number of imaging procedures performed at satellite sites increased (Table 3). During 2020, the percentage of imaging examinations performed at one of the satellite locations doubled and by the end of 2020, 10% of all imaging procedures were performed at one of the satellite sites (Fig. 5).

Columns portray the percentage of imaging procedures performed at the Manhattan Main Campus (dark-grey) vs satellite sites (light-grey). Over time, the percentage of imaging procedures performed at satellite sites increase
Discussion
As a result of the COVID-19 shutdown in March 2020, [1, 3] routine orthopedic patient care faced a substantial disruption. Due to the elective nature of hip and knee replacement surgeries, the average number of surgeries performed per day at the author’s institution initially decreased by 90% and remained at a lower level by the end of 2020. A corresponding decrease was observed for patient visits and the changing environment pushed the use of telehealth platforms.
The initial drop in surgical procedures and patient care in early spring 2020 resulted primarily from governmental and institutional restrictions, and the controlled shutdown of routine patient care to preserve resources for COVID-19 and emergency patients. Health care facilities had to adapt their workflows [6] and it took time until PPE and COVID-19 testing was more widespread available to safely resume non-emergent patient care [11]. A “return to normal” in non-emergent patient care required strict protocols for COVID-19-screening and mandatory COVID-19 testing. The author’s healthcare facility only operated at limited capacity and patient selection for surgery was based on medical urgency and the overall health of patients [12].
It was not until the decline of the SARS-CoV-2 infection rate by the end of July 2020, that the volume of surgeries performed at the institution started to recover. During the summer months of 2020, surgical volume regained a comparable level to the previous year, but that volume could not be maintained towards the end of the year. A full recovery was most likely suppressed by the resurgence of SARS-CoV-2-cases in late fall of 2020. These numbers align well with previous reports. According to the results of a Medicare-based analysis [8] and a survey of the AAHKS [9], up to 90% of all members, that completed the survey, reported a substantial reduction of clinic volume for orthopedic care between March and June as well as a persistent reduction in surgery volume [9]. Our data show that the shortfall of hip and knee replacement surgeries was not followed by an excess in the number of surgical procedures to make up for the deferred surgeries. It is unclear if patients sought care in facilities closer to home, in less populated locations, or if there is a backlog of patients who have yet to seek care.
This leaves orthopedic facilities with the potential of a massive backlog and loss of projected revenue [8]. Based on Medicare data, the loss of revenue for the 2 weeks after the shutdown, was estimated to be $236 million. Jain et al. [13] tried to quantify the backlog for total joint replacement surgeries based on the National Inpatient Sample (NIS) of the Agency for Healthcare Research and Quality (AHRQ) [14]. Their scenario assumed that it would take seven months to regain 90% of the previously maintained surgery volume, if surgery numbers had been reconstituted by June 2020.
A recent study investigated patient’s quality of life while waiting for joint replacement surgery during the COVID-19 pandemic [15]. Almost a third of THA patients and a quarter of the TKA patients consider their state of wellbeing as worse than death while waiting for a joint replacement [15]. At the same time, patients may be hesitant to seek medical care to the usual extent out of fear to infect themselves [16]. The fact that new patient visits did not recover to the same extent as follow-up visits did, underlines patient’s hesitancy to consider establishing care and surgeries during the later time in 2020 [17]. To ensure continued patient care, efforts were made to provide virtual health care.
There was a surge in telemedicine appointments after March 2020 [7, 18]. At the author’s institution a HIPAA-compliant telehealth platform was integrated into the electronic health record system, which allowed video calls as well as accurate documentation, and billing of virtual visits. Patients are also able to reach healthcare personnel through a chat function. The current data show that availability of telemedicine was essential for mitigating the disruption of patient care. A recent study by Puzzitiello et al. [19] evaluated patients’ perception and accessibility on orthopedic telehealth services. 85% considered telehealth appointments as appealing and only 36% percent preferred office visits over virtual visits [19]. Patients especially favor the time saving aspect. Nonetheless, despite great technologic advancement, our data show that the utilization of telemedicine has stagnated towards the end of the year. Clinical examinations and injections are a vital part for orthopedic patient care and therefore limitations remain to telehealth care. Detailed virtual examination protocols have been published [5], but in the survey by Puzzitiello et al. [19] about 81% were concerned with the lack of physical examination. Additionally, telehealth platforms must be user-friendly and not all patients have access to or are familiar with digital devices. According to the survey of Puzzitiello et al., only 8.5% of the consulted population was over 60 years old. One can therefore presume that most patients were capable to use digital devices and overall healthier [19]. Lam et al. [20] reported that 72% of the elderly are unready for the use of telemedicine because of impaired vision or hearing disability. Virtual patient care may play a bigger role for the younger patient population, as well as for FU appointments more than for new patient visits, as mutual trust between the attending physician and the patient has already been created. Furthermore, there are other innovative platforms that play a growing role and allow remote patient monitoring easily. One of the authors has his patients report on pain, ROM, walking ability and other measurable outcomes daily and is thereby constantly aware of the postoperative rehabilitation progress, or the lack thereof. Remote patient monitoring is a growing topic and if patients are doing well after surgery, remote monitoring will help physicians decide whether an in-person FU visit is necessary.
Outpatient centers for surgical procedures have already become more common over the last several years and one can expect the outpatient sector to grow further. There was a push towards satellite sites for patient visits observed. In 2020, primary total knee and hip arthroplasties were removed from the “inpatient-only” list [21] as improved care for patients receiving joint replacement surgery has enabled the emergence of same-day-surgeries and outpatient arthroplasties [22]. This may help to make up for the expected backlog in orthopedic surgeries but will require appropriate efforts in resource (re-)allocation, uniform patient care protocols, patient selection criteria and ambulatory aftercare for surgical patients [23].
The current study has following limitations: (1) the data do not extend beyond the end of 2020 and cannot foresee if lost volume will be recovered in 2022. Assessing the impact of the COVID vaccine rollout in the United Sates will be of great interest at a later stage (2) this study only includes providers on EPIC and does not provide information for all surgeons on staff at Hospital for Special Surgery.
Conclusion
Orthopedic patient care faced a substantial disruption and the shortfall in surgeries and outpatient visits was not fully made up, potentially leaving a significant backlog at the end of 2020. While it appears that the increased utilization of offsite satellite offices will continue throughout 2022, the role of telehealth appointments has decreased in the second half of 2020. Nonetheless, telehealth and remote patient monitoring is a growing sector and health care facilities will have to invest into its use to keep up with up-to-date patient care on the long term.
Change history
05 August 2022
A Correction to this paper has been published: https://doi.org/10.1007/s00402-022-04567-2
References
(CMS) CfMMS (2020) Non-emergent, elective medical services, and treatment recommendations. https://www.cms.gov/files/document/cms-non-emergent-elective-medical-recommendations.pdf
(ACS) ACoS (2020) COVID-19 guidelines for triage of orthopaedic patients. https://www.facs.org/for-medical-professionals/covid-19/clinical-guidance/elective-case/orthopaedics/
(AAOS) AAoOS (2020) AAOS guidelines for elective surgery during the COVID-19 pandemic. https://www.aaos.org/about/covid-19-information-for-our-members/aaos-guidelines-for-elective-surgery/
Paul KD, Levitt E, McGwin G, Brabston EW 3rd, Gilbert SR, Ponce BA, Momaya AM (2021) COVID-19 impact on orthopedic surgeons: elective procedures, telehealth, and income. South Med J 114(5):311
Tanaka MJ, Oh LS, Martin SD, Berkson EM (2020) Telemedicine in the era of COVID-19: the virtual orthopaedic examination. J Bone Jt Surg Am 102(12):e57
Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS (2020) Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg 28(11):e469
Rao SS, Loeb AE, Amin RM, Golladay GJ, Levin AS, Thakkar SC (2020) Establishing telemedicine in an academic total joint arthroplasty practice: needs and opportunities highlighted by the COVID-19 pandemic. Arthroplasty Today 6(3):617
Barnes CL, Zhang X, Stronach BM, Haas DA (2021) The initial impact of COVID-19 on total hip and knee arthroplasty. J Arthroplasty 36:56–61
Stambough JB, Deen JT, Walton SL, Kerr JM, Zarski MJ, Yates AJ Jr, Andrawis JP (2021) Arthroplasty during COVID-19: surveillance of AAHKS members in the first year of the pandemic. Arthroplasty Today 7:209
The Atlantic (2020) The COVID tracking project. https://covidtracking.com/
Ranney ML, Griffeth V, Jha AK (2020) Critical supply shortages—the need for ventilators and personal protective equipment during the Covid-19 Pandemic. N Engl J Med 382(18):e41
Boettner F, Bostrom MP, Figgie M, Gonzalez Della Valle A, Haas S, Mayman D, Padgett D (2020) Timeline and procedures on restarting non-emergent arthroplasty care in the US epicenter of the COVID-19 pandemic. HSS J 16(Suppl 1):1
Jain A, Jain P, Aggarwal S (2020) SARS-CoV-2 impact on elective orthopaedic surgery: implications for post-pandemic recovery. J Bone Jt Surg Am 102(13):e68
Wilson JM, Schwartz AM, Farley KX, Roberson JR, Bradbury TL, Guild GN 3rd (2020) Quantifying the backlog of total hip and knee arthroplasty cases: predicting the impact of COVID-19. HSS J 16(Suppl 1):1
Clement ND, Scott CEH, Murray JRD, Howie CR, Deehan DJ (2021) The number of patients “worse than death” while waiting for a hip or knee arthroplasty has nearly doubled during the COVID-19 pandemic. Bone Jt J 103(4):672
Czeisler M, Marynak K, Clarke KEN, Salah Z, Shakya I, Thierry JM, Ali N, McMillan H, Wiley JF, Weaver MD, Czeisler CA, Rajaratnam SMW, Howard ME (2020) Delay or avoidance of medical care because of COVID-19-related concerns—United States, June 2020. MMWR Morb Mortal Wkly Rep 69(36):1250
Moverman MA, Puzzitiello RN, Pagani NR, Barnes CL, Jawa A, Menendez ME (2021) Public perceptions of resuming elective surgery during the COVID-19 pandemic. J Arthroplasty 36(2):397
Mann DM, Chen J, Chunara R, Testa PA, Nov O (2020) COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inf Assoc 27(7):1132
Puzzitiello RN, Moverman MA, Pagani NR, Ryan SP, Salzler MJ, Jawa A, Menendez ME (2021) Public perceptions and disparities in access to telehealth orthopaedic services in the COVID-19 era. J Natl Med Assoc 25:56
Lam K, Lu AD, Shi Y, Covinsky KE (2020) Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Intern Med 180(10):1389
(CMS-1717-FC) CMhoPpsaAsCpsfR (2020). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Hospital-Outpatient-Regulations-and-Notices-Items/CMS-1717-FC
Edwards PK, Milles JL, Stambough JB, Barnes CL, Mears SC (2019) Inpatient versus outpatient total knee arthroplasty. J Knee Surg 32(8):730
Meneghini RM (2020) Resource reallocation during the COVID-19 pandemic in a suburban hospital system: implications for outpatient hip and knee arthroplasty. J Arthroplasty 35(7s):S15
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the designing the study. The manuscript was drafted by CH and edited by AJ and SD. Data analysis was performed by CH. The project was supervised by FB and SJ. All authors reviewed the manuscript and contributed to its final version.
Corresponding author
Ethics declarations
Conflicts of interest
FB is consultant for Smith & Nephew, OrthoDevelopment, DePuy and Medtronic and receives Royalties from Smith & Nephew and OrthoDevelopment. SJ receives Royalties and Research Support from Stryker, is a paid consultant for Stryker and has stock options in the company Imagen. None of the COIs are related to this research project. Remaining authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethics approval
The study was approved by the local Institutional Review Board of the senior author’s institution.
Informed consent
Due to the study design, it was not necessary to obtain informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The given name and last names of the authors were swapped.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hanreich, C., Boettner, F., DeNegre, S. et al. The impact of the COVID-19 associated shutdown on orthopedic patient care. Arch Orthop Trauma Surg 143, 2885–2892 (2023). https://doi.org/10.1007/s00402-022-04466-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-022-04466-6