
Abstract
Introduction
There is still a lack of evidence concerning the patellar fixation of the medial patellofemoral ligament (MPFL) graft in selected patient with recurrent instability. The purpose of the present study was to investigate and compare clinical outcomes and further complications of isolated MPFL reconstruction via suture anchors versus tunnel techniques for recurrent patellofemoral instability.
Materials and methods
This systematic review of the literature was conducted according to the PRISMA guidelines. In September 2019, the main databases were accessed. All the clinical trials performing isolated MPFL reconstruction in patients with recurrent patellofemoral instability were included in the present study. Only articles fixing the MPFL graft through suture anchors and/ or patellar tunnel techniques were included in the analysis.
Results
Data from 46 papers (1712 patients) were recorded. The mean follow-up was 40 ± 18 months. No differences were found in Kujala, Lysholm and Tegner score, International Knee Documentation Committee, visual analogic scale, range of motion and re-dislocation rate. The suture anchors fixation group detected reduced rate of apprehension test (OR: 0.6; p = 0.03), revision surgeries (OR: 0.4; p = 0.02) and anterior knee pain (OR: 0.05; p < 0.0001) and reduced not-classified complications (OR: 0.18; p < 0.0001).
Conclusion
Both the suture anchors and the bone-tunnels are a feasible option for isolated MPFL reconstruction in patients with recurrent patellofemoral instability. Patellar fixation via suture anchors evidenced a reduced rate of anterior knee pain, revision surgeries, apprehension test and an overall reduced complication compared to the bone-tunnel technique.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patellofemoral instability is a common disorder, especially among young and active patients [1]. Patellofemoral instability is a multifactorial disorder [2]. Several pathoanatomical risk factors that predispose to instability has been described: patella alta, mal-alignment syndromes, axial deformation, patellar dysplasia [3,4,5]. Most of the patients reported a combination of two or more risk factors that contribute to developing instability [6]. After the first patellar dislocation, tears of medial-patellofemoral ligament (MPFL) occur in approximately in all the patients [7]. Despite the multifactorial etiology, the isolated MPFL reconstruction yields comparable results to the older realignment procedures, with lesser postoperative morbidity and increased patient satisfaction [8]. The role of the MPFL has been extensively investigated in the past decades. However, there is still lack of evidence concerning the patellar fixation of the MPFL graft. Typically, the MPFL reconstruction was performed via bone tunnel techniques. No differences were found in strength between the native MPFL and through tunnel techniques [9]. However, patellar tunnels violate the bone structure, reducing the stability and resistance, leading to an increased risk of secondary fracture [10,11,12,13]. In recent times, to avoid tunnelling through the whole length of the patella and related complications, suture anchors techniques have been introduced [14,15,16,17]. There are still controversies concerning graft source, positioning, and fixation, and up to date, no consensus has been reached. Hence, the purpose of the present study was to carry out a systematic review of the literature to investigate and compare the role of isolated MPFL reconstruction via suture anchors versus tunnel techniques for recurrent patellofemoral instability.
Materials and methods
Search strategy
This systematic review of the literature was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) [18]. The following criteria were used to guide the literature search:
-
P (population): recurrent patellofemoral instability;
-
I (intervention): isolated MPFL reconstruction;
-
C (comparison): graft fixation techniques;
-
O (outcomes): clinical scores, clinical examination, complication.
Literature search
The literature search was performed by two independent reviewers (FM, JE). In September 2019, the main databases were accessed: PubMed, Medline, Embase, Scopus, and Google Scholar. For the database search, the following keywords and Boolean operators were used in combination: patellofemoral instability, medio-patellofemoral ligament, MPFL, graft, fixation, patellar, femoral, bone, tunnel, suture, anchors, Endobutton, dislocation, re-dislocation, failure, anterior knee pain, Kujala, Tegner, Lysholm, IKDC, range of motion, complications, apprehension test. The full text of the articles of interest was accessed. The bibliographies of the included articles were also screened. Disagreements between the authors were mutually debated and solved.
Eligibility criteria
All the clinical trials performing isolated MPFL reconstruction in patients with recurrent patellofemoral instability were included in the present study. Only articles describing the graft fixation technique were considered for inclusion. Only articles fixing the MPFL graft through suture anchors and/ or two-patellar tunnel techniques were included in the analyses. According to the author’s language capabilities, only articles in English, Spanish, Italian, German, French were considered for inclusion. According to the Oxford Centre of Evidenced-Based Medicine [19], articles level of evidence I–III were included in the present study. Articles reporting data from acute patellar dislocations were excluded. Articles reporting duration of the follow-up less than 12 months were excluded. Given the quickly evolution of indications and techniques, articles published before the year 2000 were excluded. Articles treating MPFL reconstruction during revision setting or during total knee arthroplasty were excluded. Case reports, expert opinions, editorials, biomechanics, cadaveric and animal studies were excluded. Only articles reporting quantitative Data under the outcomes of interest were included in the present study. Missing data under the outcomes of interest warranted the exclusion from the present study.
Outcomes of interest
Data extraction was performed by two independent reviewers (FM, JE). The following generalities were extracted: author and year, the number of procedures, mean age of the samples at time of surgery, mean follow-up duration, type of study, graft source, and bundle. The type of surgical techniques and fixations were screened and recorded for each study. Patient outcomes were analysed through the following scores: Kujala Anterior Knee Pain Scale [20], Lysholm Knee Scoring Scale [21], Tegner Activity Scale [22], International Knee Documentation Committee (IKDC) [23], Visual Analogic Scale (VAS), range of motion (ROM). The following complications were recorded: apprehension test, revision surgeries, further re-dislocations, and anterior knee pain. Furthermore, we collected data from other complications (arthrofibrosis, hemarthrosis, subluxation, reduced ROM, quadriceps atrophy, persistent sensation of instability, others).
Methodological quality assessment
The methodological quality assessment was performed through the PEDro score. This score was performed by two independent authors (FM, JE). The PEDro score has been validated in previous studies [24, 25]. This score evaluated the included studies under 11 dichotomous endpoints. The final value ranked 0–10. Values > 6 are considered satisfactory.
Statistical analysis
For the statistical analyses, we referred to SPSS software (Version 25, IBM SPSS Statistics). Continuous data were evaluated through the arithmetic mean, standard deviation, and range of intervals. Dichotomous data were evaluated through the odds ratio (OR) statistical method. The interval of confidence was set at 95%. The statistical significance was evaluated through the unpaired t test. Values of p > 0.05 were considered satisfactory.
Results
Search result
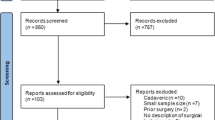
The literature search resulted in 1352 papers. Of them, 398 were rejected because of duplicated. The other 458 studies were excluded because of a poor level of evidence or not performing a clinical study. Further 450 papers were excluded: language incompatibility (51), treating acute dislocations (24), follow-up < 12 months (74); year of publication before 2000 (83), revision setting (31), missing data (77), uncertain results (3), lack of quantitative data under the outcomes of interest (107). Finally, 46 papers were included: 5 randomized clinical trials (RCT), 17 prospective (PCS) and 24 retrospectives (RCS) clinical trials. The literature search is shown in Fig. 1.

PRISMA flowchart of the literature search
Methodological quality assessment
The PEDro score evidenced some limitations of the present study. First, the lack of randomization and blinding methods among the studies. This will reduce noteworthy the quality of methodological assessment and improve the risk of selection bias. The point of strength was the adequate follow-up of the studies, and the acceptable analyses performed. Concluding, the overall PEDro score resulted in 7.1 points, attesting to the present study a good methodological quality assessment. The PEDro score assigned to each study is shown in Table 1.
Demographic data
Data from a total of 1712 patients were recorded. The mean follow-up was 40 ± 18 months. A total of 817 were included in the suture anchors fixation. The mean age of this cohort was 26 ± 3 years. In the double-tunnel technique, a total of 895 knees were analysed, with a mean age of 22 ± 7 years. No differences were found concerning the patient’s age (p = 0.08). Demographic data are shown in Table 1.
Clinical endpoints
No differences were found concerning the Kujala score (87.60 ± 5.2 versus 87.23 ± 6.4, p = 0.4), Lysholm score (89.17 ± 4.3 versus 91.51 ± 2.7, p = 0.1), Tegner score (5.92 ± 1.2 versus 5.15 ± 0.6, p = 0.1), IKDC (72.81 ± 1.6 versus 78.53 ± 5.2, p = 0.1), VAS (19.50 ± 2.0 versus 16.88 ± 2.7, p = 0.1), ROM (132.14 ± 8.8 versus 132.70 ± 10.9, p = 0.5). Noteworthy, analysing the subgroup “double bundle graft”, the only difference was the greater value of the Kujala score in favour of the suture anchors group (89.71 ± 3.5 versus 86.02 ± 6.6, p = 0.03). An overview of the clinical results is shown in Table 2.
Complication rate
The suture anchors fixation group detected reduced rate of post-operative apprehension test (OR: 0.5706; 95% CI: 0.3486–0.9338, p = 0.03), revision surgeries (OR: 0.4108; 95% CI: 0.1898–0.8890; p = 0.02) and anterior knee pain (OR: 0.0522; 95% CI: 0.0126–0.2162; p < 0.0001). Re-dislocations were in favour of the suture anchors cohort, but no statistical significance was detected (OR: 0.6086; 95% CI: 0.3215–1.1522; p = 0.1). Concerning other not classified complications, the doubled tunnel cohort reported a higher risk (OR: 0.1826; 95% CI: 0.1048–0.3180; p < 0.0001). Analysing the subgroup “double bundle graft”, the only differences were found regarding the re-dislocation risk, that were reduced in favour of the suture anchors group (OR: 0.2953; 95% CI: 0.0856–1.0186; p = 0.05). An overview of the complication rate is shown in Table 3.
Discussion
The main findings of this systematic review of the literature are that both the suture anchors and the bone-tunnels are a feasible solution for isolated MPFL reconstruction in patients with recurrent patellofemoral instability. MPFL reconstruction through suture anchors reported a statistically significant reduced rate of postoperative anterior knee pain, along with an overall reduced complication compared to the bone-tunnels technique. Moreover, the subgroup suture anchors via double-bundle graft detected a statistically significant reduction of the re-dislocations rate and a minimal improvement of the Kujala score compared to the double tunnel technique. No differences were found in terms of ROM and clinical scores.
Concerning the clinical scores, only the subgroup suture anchors fixation through double-bundle MPFL graft evidenced a significantly greater value of the Kujala score over the bone tunnel techniques. Contextualizing, these data found no clinical relevance, since the small difference of 3.69%. All the other scores of interest detected similarity among the two techniques. Concerning complications, the suture anchors fixation group detected an overall reduction of the complications. The outcomes apprehension test and revision surgeries detected a significant halved risk in the suture anchors group respect to the bone tunnel cohort. Noteworthy, the risk of developing anterior knee pain was strongly reduced in the suture anchors group. The re-dislocation rate of the suture anchors versus bone tunnel fixation was similar. Interestingly, the analysis of the subgroup anchor fixation via double-bundle showed a significantly reduced re-dislocations risk of about one-third compared to the bone tunnel techniques.
In the literature, there is a lack of clinical studies comparing directly suture anchors fixations and bone tunnel techniques. Kang et al. [69] performed a systematic review of the literature including 21 studies, consisting of 691 patients undergoing 36-month follow-up. They found no differences among the two techniques concerning Kujala, apprehension test, dislocations, and complications. Several studies analysed the biomechanics of the various patellar insertion techniques. From a biomechanical point of view, the suture anchors evidenced lower stiffness than the tunnel techniques (21 N/mm versus 28 N/mm), while no differences were found in the ultimate load (299 N versus 304 N, respectively) [70]. The biomechanical study of Lenschow et al. [71] evaluated the maximum load to failure and elongation. The suture anchors showed a higher maximum load to failure than the bone tunnel techniques (401 Nm versus 354 Nm), better elongation after 1000 cycles (3.7 mm versus 1.9 mm) [71]. He et al. [72] compared the native MPFL reconstruction versus double and single bundle. They found similarity between single bundle and native MPFL in terms of tensile strength (146 N versus 159 N) and elongation (8.39 mm versus 7.64 mm) [72]. In their study, they found a considerably higher tensile strength and elongation in double-bundle suture anchors group (314 N and 12 N, respectively) [72]. In the cadaveric study of Mountney et al. [9], the load to failure was tested of the native MPFL versus several different MPFL repair and reconstruction in ten knees. They found that suture anchors showed lower failure strength than the native MPFL [9].
The higher complexity of this topic, along with the controversial and reduced knowledge concerning the patellofemoral disorders considerably pose important limitation to draw solid conclusions. Even if the overall methodological assessment via the PEDro score resulted acceptably, an important limitation of the present study was the overall low quality of the included studies. Only one-tenth of the studies provided a randomization allocation, no one took advantage of a blinding method. This increases considerably the risk of selection bias, therefore, data from this study must interpret with caution. The following study analysed outcomes and complications with regard to the patellar fixation exclusively. Type of graft, femoral insertion and tensioning were not considered. This represents another important limitation of the present work. The good baseline comparability and the comprehensive nature of the literature search, along with the strict eligibility criteria represented the most important point of strength of this study.
Conclusion
Both the suture anchors and the bone-tunnels are a feasible solution for isolated MPFL reconstruction in patients with recurrent patellofemoral instability. MPFL reconstruction through suture anchors reported a statistically significant reduced rate of postoperative anterior knee pain, apprehension test and revisions, along an overall reduced complication compared to the bone-tunnels technique. Moreover, the subgroup suture anchors via double-bundle graft detected a statistically significant reduction of the re-dislocations rate and a minimal improvement of the Kujala score compared to the double tunnel technique. No differences were found in terms of ROM and clinical scores.
Change history
22 June 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00402-021-03987-w
References
Migliorini F, Rath B, Tingart M, Meisen N, Eschweiler J (2019) Surgical management for recurrent patellar dislocations in skeletally immature patients. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-019-02483-7
Li L, Wang H, He Y, Si Y, Zhou H, Wang X (2018) Treatment of recurrent patellar dislocation via knee arthroscopy combined with C-arm fluoroscopy and reconstruction of the medial patellofemoral ligament. Exp Ther Med 15(6):5051–5057. https://doi.org/10.3892/etm.2018.6055
Petri M, Ettinger M, Stuebig T, Brand S, Krettek C, Jagodzinski M, Omar M (2015) Current concepts for patellar dislocation. Arch Trauma Res 4(3):e29301. https://doi.org/10.5812/atr.29301
Bartsch A, Lubberts B, Mumme M, Egloff C, Pagenstert G (2018) Does patella alta lead to worse clinical outcome in patients who undergo isolated medial patellofemoral ligament reconstruction? A systematic review. Arch Orthop Trauma Surg 138(11):1563–1573. https://doi.org/10.1007/s00402-018-2971-4
Ren B, Zhang X, Zhang L, Zhang M, Liu Y, Tian B, Zhang B, Zheng J (2019) Isolated trochleoplasty for recurrent patellar dislocation has lower outcome and higher residual instability compared with combined MPFL and trochleoplasty: a systematic review. Arch Orthop Trauma Surg 139(11):1617–1624. https://doi.org/10.1007/s00402-019-03244-1
Steensen RN, Bentley JC, Trinh TQ, Backes JR, Wiltfong RE (2015) The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: a magnetic resonance imaging study. Am J Sports Med 43(4):921–927. https://doi.org/10.1177/0363546514563904
Migliorini F, Rath B, Tingart M, Niewiera M, Eschweiler J (2019) Distal alignment procedures for patellofemoral instability: comprehensive review of the literature. Eur J Orthop Surg Traumatol 29(7):1579–1588. https://doi.org/10.1007/s00590-019-02451-1
Buckens CF, Saris DB (2010) Reconstruction of the medial patellofemoral ligament for treatment of patellofemoral instability: a systematic review. Am J Sports Med 38(1):181–188. https://doi.org/10.1177/0363546509353132
Mountney J, Senavongse W, Amis AA, Thomas NP (2005) Tensile strength of the medial patellofemoral ligament before and after repair or reconstruction. J Bone Jt Surg Br 87(1):36–40
Christiansen SE, Jacobsen BW, Lund B, Lind M (2008) Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes. Arthroscopy 24(1):82–87. https://doi.org/10.1016/j.arthro.2007.08.005
Smith TO, Walker J, Russell N (2007) Outcomes of medial patellofemoral ligament reconstruction for patellar instability: a systematic review. Knee Surg Sports Traumatol Arthrosc 15(11):1301–1314. https://doi.org/10.1007/s00167-007-0390-0
Thaunat M, Erasmus PJ (2008) Recurrent patellar dislocation after medial patellofemoral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 16(1):40–43. https://doi.org/10.1007/s00167-007-0418-5
Schuttler KF, Hoeger A, Heyse TJ, Figiel J, Timmesfeld N, Stein T, Ziring E, Efe T (2018) Femoral tunnel widening is associated with tunnel malposition but not with clinical failure after medial patellofemoral ligament reconstruction with a free gracilis tendon graft. Arch Orthop Trauma Surg 138(7):979–984. https://doi.org/10.1007/s00402-018-2923-z
Ahmad CS, Brown GD, Shubin Stein BE (2009) The docking technique for medial patellofemoral ligament reconstruction: surgical technique and clinical outcome. Am J Sports Med 37(10):2021–2027. https://doi.org/10.1177/0363546509336261
Schottle PB, Fucentese SF, Romero J (2005) Clinical and radiological outcome of medial patellofemoral ligament reconstruction with a semitendinosus autograft for patella instability. Knee Surg Sports Traumatol Arthrosc 13(7):516–521. https://doi.org/10.1007/s00167-005-0659-0
Schottle PB, Hensler D, Imhoff AB (2010) Anatomical double-bundle MPFL reconstruction with an aperture fixation. Knee Surg Sports Traumatol Arthrosc 18(2):147–151. https://doi.org/10.1007/s00167-009-0868-z
Schottle PB, Romero J, Schmeling A, Weiler A (2008) Technical note: anatomical reconstruction of the medial patellofemoral ligament using a free gracilis autograft. Arch Orthop Trauma Surg 128(5):479–484. https://doi.org/10.1007/s00402-007-0300-4
Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen JP, Mulrow C, Catala-Lopez F, Gotzsche PC, Dickersin K, Boutron I, Altman DG, Moher D (2015) The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 162(11):777–784. https://doi.org/10.7326/M14-2385
Howick J CI, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford levels of evidence. Oxford centre for evidence-based medicine. https://www.cebm.net/indexaspx?o=5653. Accessed Sept 2019
Dammerer D, Liebensteiner MC, Kujala UM, Emmanuel K, Kopf S, Dirisamer F, Giesinger JM (2018) Validation of the German version of the Kujala score in patients with patellofemoral instability: a prospective multi-centre study. Arch Orthop Trauma Surg 138(4):527–535. https://doi.org/10.1007/s00402-018-2881-5
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10(3):150–154. https://doi.org/10.1177/036354658201000306
Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR (2009) The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med 37(5):890–897. https://doi.org/10.1177/0363546508330143
Higgins LD, Taylor MK, Park D, Ghodadra N, Marchant M, Pietrobon R, Cook C, International Knee Documentation C (2007) Reliability and validity of the International Knee Documentation Committee (IKDC) subjective knee form. Jt Bone Spine 74(6):594–599. https://doi.org/10.1016/j.jbspin.2007.01
de Morton NA (2009) The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother 55(2):129–133
Migliorini F, Biagini M, Rath B, Meisen N, Tingart M, Eschweiler J (2018) Total hip arthroplasty: minimally invasive surgery or not? Meta-analysis of clinical trials. Int Orthop. https://doi.org/10.1007/s00264-018-4124-3
Amin NH, Lynch TS, Patel RM, Patel N, Saluan P (2015) Medial patellofemoral ligament reconstruction. JBJS Rev. https://doi.org/10.2106/JBJS.RVW.N.00089
Astur DC, Gouveia GB, Borges JH, Astur N, Arliani GG, Kaleka CC, Cohen M (2015) Medial patellofemoral ligament reconstruction: a longitudinal study comparison of 2 techniques with 2 and 5-years follow-up. Open Orthop J 9:198–203. https://doi.org/10.2174/1874325001509010198
Ballal M, VasinathBasha PN (2018) Functional outcome of medial patellofemoral ligament injury (MPFL) reconstruction in recurrent patellar dislocation. Int J Orthop Sci 4(4):204–207. https://doi.org/10.22271/ortho.2018.v4.i4d.38
Berruto M, Ferrua P, Uboldi F, Usellini E, Gala L, Tassi A, Marelli B (2014) Medial patellofemoral ligament reconstruction with bioactive synthetic ligament is an option. A 3-year follow-up study. Knee Surg Sports Traumatol Arthrosc 22(10):2419–2425. https://doi.org/10.1007/s00167-014-2970-0
Carnesecchi O, Neri T, Di Iorio A, Farizon F, Philippot R (2015) Results of anatomic gracilis MPFL reconstruction with precise tensioning. Knee 22(6):580–584. https://doi.org/10.1016/j.knee.2015.01.006
Csintalan RP, Latt LD, Fornalski S, Raiszadeh K, Inacio MC, Fithian DC (2014) Medial patellofemoral ligament (MPFL) reconstruction for the treatment of patellofemoral instability. J Knee Surg 27(2):139–146. https://doi.org/10.1055/s-0033-1360652
Feller JA, Richmond AK, Wasiak J (2014) Medial patellofemoral ligament reconstruction as an isolated or combined procedure for recurrent patellar instability. Knee Surg Sports Traumatol Arthrosc 22(10):2470–2476. https://doi.org/10.1007/s00167-014-3132-0
Fernandez E, Sala D, Castejon M (2005) Reconstruction of the medial patellofemoral ligament for patellar instability using a semitendinosus autograft. Acta Orthop Belg 71(3):303–308
Ellera Gomes JL (1992) Medial patellofemoral ligament reconstruction for recurrent dislocation of the patella: a preliminary report. Arthroscopy 8(3):335–340
Gonçaives MBJ, Júnior LHdC, Soares LFM, Gonçaives TJ, dos Santos RL, Pereira ML (2011) Medial patellofemoral ligament reconstruction to treat recurrent patellar dislocation. Rev Bras Ortop 46(2):160–164. https://doi.org/10.1016/s2255-4971(15)30233-0
Han H, Xia Y, Yun X, Wu M (2011) Anatomical transverse patella double tunnel reconstruction of medial patellofemoral ligament with a hamstring tendon autograft for recurrent patellar dislocation. Arch Orthop Trauma Surg 131(3):343–351. https://doi.org/10.1007/s00402-010-1173-5
Hiemstra LA, Kerslake S, Lafave M (2017) Medial patellofemoral ligament reconstruction femoral tunnel accuracy: relationship to disease-specific quality of life. Orthop J Sports Med 5(2):2325967116687749. https://doi.org/10.1177/2325967116687749
Howells NR, Barnett AJ, Ahearn N, Ansari A, Eldridge JD (2012) Medial patellofemoral ligament reconstruction: a prospective outcome assessment of a large single centre series. J Bone Jt Surg Br 94(9):1202–1208. https://doi.org/10.1302/0301-620X.94B9.28738
Kang H, Cao J, Yu D, Zheng Z, Wang F (2013) Comparison of 2 different techniques for anatomic reconstruction of the medial patellofemoral ligament: a prospective randomized study. Am J Sports Med 41(5):1013–1021. https://doi.org/10.1177/0363546513480468
Kang CH, Kim HK, Shiraj S, Anton C, Kim DH, Horn PS (2016) Patellofemoral instability in children: T2 relaxation times of the patellar cartilage in patients with and without patellofemoral instability and correlation with morphological grading of cartilage damage. Pediatr Radiol 46(8):1134–1141. https://doi.org/10.1007/s00247-016-3574-2
Kim TS, Kim HJ, Ra IH, Kyung HS (2015) Medial patellofemoral ligament reconstruction for recurrent patellar instability using a gracilis autograft without bone tunnel. Clin Orthop Surg 7(4):457–464. https://doi.org/10.4055/cios.2015.7.4.457
Kita K, Tanaka Y, Toritsuka Y, Amano H, Uchida R, Takao R, Horibe S (2015) Factors affecting the outcomes of double-bundle medial patellofemoral ligament reconstruction for recurrent patellar dislocations evaluated by multivariate analysis. Am J Sports Med 43(12):2988–2996. https://doi.org/10.1177/0363546515606102
Krishna Kumar M, Renganathan S, Joseph CJ, Easwar T, Rajan DV (2014) Medial patellofemoral ligament reconstruction in patellar instability. Indian J Orthop 48(5):501–505. https://doi.org/10.4103/0019-5413.139864
Lind M, Enderlein D, Nielsen T, Christiansen SE, Fauno P (2016) Clinical outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent patella instability. Knee Surg Sports Traumatol Arthrosc 24(3):666–671. https://doi.org/10.1007/s00167-014-3439-x
Lin KY, Lu YC, Renn JH (2015) The double-pulley technique for anatomical double-bundled medial patellofemoral ligament reconstruction. Injury 46(8):1619–1624. https://doi.org/10.1016/j.injury.2015.04.017
Lippacher S, Dreyhaupt J, Williams SR, Reichel H, Nelitz M (2014) Reconstruction of the medial patellofemoral ligament: clinical outcomes and return to sports. Am J Sports Med 42(7):1661–1668. https://doi.org/10.1177/0363546514529640
Ma LF, Wang F, Chen BC, Wang CH, Zhou JW, Wang HY (2013) Medial retinaculum plasty versus medial patellofemoral ligament reconstruction for recurrent patellar instability in adults: a randomized controlled trial. Arthroscopy 29(5):891–897. https://doi.org/10.1016/j.arthro.2013.01.030
Matsushita T, Kuroda R, Oka S, Matsumoto T, Takayama K, Kurosaka M (2014) Clinical outcomes of medial patellofemoral ligament reconstruction in patients with an increased tibial tuberosity-trochlear groove distance. Knee Surg Sports Traumatol Arthrosc 22(10):2438–2444. https://doi.org/10.1007/s00167-014-2919-3
Mikashima Y, Kimura M, Kobayashi Y, Miyawaki M, Tomatsu T (2006) Clinical results of isolated reconstruction of the medial patellofemoral ligament for recurrent dislocation and subluxation of the patella. Acta Orthop Belg 72(1):65–71
Monllau JC, Masferrer-Pino A, Ginovart G, Perez-Prieto D, Gelber PE, Sanchis-Alfonso V (2017) Clinical and radiological outcomes after a quasi-anatomical reconstruction of medial patellofemoral ligament with gracilis tendon autograft. Knee Surg Sports Traumatol Arthrosc 25(8):2453–2459. https://doi.org/10.1007/s00167-015-3934-8
Neri T, Philippot R, Carnesecchi O, Boyer B, Farizon F (2015) Medial patellofemoral ligament reconstruction: clinical and radiographic results in a series of 90 cases. Orthop Traumatol Surg Res 101(1):65–69. https://doi.org/10.1016/j.otsr.2014.09.023
Niu J, Qi Q, Fu K, Duan G, Liu C, Wang F (2017) Medial patellofemoral ligament reconstruction with semi-patellar tunnel fixation: surgical technique and mid-term follow-up. Med Sci Monit 23:5870–5875. https://doi.org/10.12659/msm.905583
Nomura E, Horiuchi Y, Kihara M (2000) A mid-term follow-up of medial patellofemoral ligament reconstruction using an artificial ligament for recurrent patellar dislocation. Knee 7(4):211–215
Nomura E, Inoue M (2006) Hybrid medial patellofemoral ligament reconstruction using the semitendinous tendon for recurrent patellar dislocation: minimum 3 years’ follow-up. Arthroscopy 22(7):787–793. https://doi.org/10.1016/j.arthro.2006.04.078
Nomura E, Inoue M, Kobayashi S (2007) Long-term follow-up and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 35(11):1851–1858. https://doi.org/10.1177/0363546507306161
Panni AS, Alam M, Cerciello S, Vasso M, Maffulli N (2011) Medial patellofemoral ligament reconstruction with a divergent patellar transverse 2-tunnel technique. Am J Sports Med 39(12):2647–2655. https://doi.org/10.1177/0363546511420079
Pinheiro Junior LFB, Cenni MHF, Nicolai OP, Gomes LPH, Leal RS, Coelho DGP (2018) Outcomes of medial patellofemoral ligament reconstruction in patients with patella alta. Rev Bras Ortop 53(5):570–574. https://doi.org/10.1016/j.rboe.2017.06.014
Raghuveer RK, Mishra CB (2012) Reconstruction of medial patellofemoral ligament for chronic patellar instability. Indian J Orthop 46(4):447–454. https://doi.org/10.4103/0019-5413.97259
Ronga M, Oliva F, Longo UG, Testa V, Capasso G, Maffulli N (2009) Isolated medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 37(9):1735–1742. https://doi.org/10.1177/0363546509333482
Sadigursky D, de Melo Laranjeira MS, Nunes M, Caneiro RJ, Colavolpe PO (2016) Reconstruction of the medial patellofemoral ligament by means of the anatomical double-bundle technique using metal anchors. Rev Bras Ortop 51(3):290–297. https://doi.org/10.1016/j.rboe.2015.07.011
Smith TO, Mann CJ, Donell ST (2014) Does knee joint proprioception alter following medial patellofemoral ligament reconstruction? Knee 21(1):21–27. https://doi.org/10.1016/j.knee.2012.09.013
Song SY, Kim IS, Chang HG, Shin JH, Kim HJ, Seo YJ (2014) Anatomic medial patellofemoral ligament reconstruction using patellar suture anchor fixation for recurrent patellar instability. Knee Surg Sports Traumatol Arthrosc 22(10):2431–2437. https://doi.org/10.1007/s00167-013-2730-6
Thaunat M, Erasmus PJ (2007) The favourable anisometry: an original concept for medial patellofemoral ligament reconstruction. Knee 14(6):424–428. https://doi.org/10.1016/j.knee.2007.08.008
Toritsuka Y, Amano H, Mae T, Uchida R, Hamada M, Ohzono K, Shino K (2011) Dual tunnel medial patellofemoral ligament reconstruction for patients with patellar dislocation using a semitendinosus tendon autograft. Knee 18(4):214–219. https://doi.org/10.1016/j.knee.2010.05.007
Wang F, Kang HJ, Chen BC, Chen W, Su YL, Zhang YZ (2010) Combination of medial patellofemoral ligament reconstruction with vastus medialis advancement for chronic patellar dislocation. Chin Med J 123(21):3024–3029
Wang CH, Ma LF, Zhou JW, Ji G, Wang HY, Wang F, Wang J (2013) Double-bundle anatomical versus single-bundle isometric medial patellofemoral ligament reconstruction for patellar dislocation. Int Orthop 37(4):617–624. https://doi.org/10.1007/s00264-013-1788-6
Wang HD, Dong JT, Gao SJ (2016) Medial patellofemoral ligament reconstruction using a bone groove and a suture anchor at patellar: a safe and firm fixation technique and 3-year follow-up study. J Orthop Surg Res 11(1):138. https://doi.org/10.1186/s13018-016-0473-z
Zhang L, Li Z (2019) Long-term clinical results of double bundle reconstruction of the medial patellofemoral ligament for patellar instability. J Knee Surg 32(2):153–159. https://doi.org/10.1055/s-0038-1636913
Kang H, Zheng R, Dong C, Fu K, Wang F (2019) No influence of patellar fixation technique on clinical outcomes of double-bundle medial patellofemoral ligament reconstruction: a systematic review. Arch Orthop Trauma Surg 139(1):79–90. https://doi.org/10.1007/s00402-018-3008-8
Hapa O, Aksahin E, Ozden R, Pepe M, Yanat AN, Dogramaci Y, Bozdag E, Sunbuloglu E (2012) Aperture fixation instead of transverse tunnels at the patella for medial patellofemoral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 20(2):322–326. https://doi.org/10.1007/s00167-011-1582-1
Lenschow S, Schliemann B, Gestring J, Herbort M, Schulze M, Kosters C (2013) Medial patellofemoral ligament reconstruction: fixation strength of 5 different techniques for graft fixation at the patella. Arthroscopy 29(4):766–773. https://doi.org/10.1016/j.arthro.2012.12.004
He W, Yang YM, Liu M, Wang AY, Liu YJ (2013) Reconstruction of the medial patellofemoral ligament using hamstring tendon graft with different methods: a biomechanical study. Chin Med Sci J 28(4):201–205
Funding
Open Access funding enabled and organized by Projekt DEAL. No external source of funding was used.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Research involving human participants and/or animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised due to a retrospective Open Access order.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Driessen, A., Quack, V. et al. Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: a systematic review of the literature . Arch Orthop Trauma Surg 140, 1201–1210 (2020). https://doi.org/10.1007/s00402-020-03420-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-020-03420-8