
Abstract
Background
Smartphone apps are increasingly utilised by patients and physicians for medical purposes. Thus, numerous applications are provided on the App Store platforms.
Objectives
The aim of the study was to establish a novel, expanded approach of a semiautomated retrospective App Store analysis (SARASA) to identify and characterise health apps in the context of cardiac arrhythmias.
Materials and methods
An automated total read-out of the “Medical” category of Apple’s German App Store was performed in December 2022 by analysing the developer-provided descriptions and other metadata using a semiautomated multilevel approach. Search terms were defined, based on which the textual information of the total extraction results was automatically filtered.
Results
A total of 435 of 31,564 apps were identified in the context of cardiac arrhythmias. Of those, 81.4% were found to deal with education, decision support, or disease management, and 26.2% (additionally) provided the opportunity to derive information on heart rhythm. The apps were intended for healthcare professionals in 55.9%, students in 17.5%, and/or patients in 15.9%. In 31.5%, the target population was not specified in the description texts. In all, 108 apps (24.8%) provided a telemedicine treatment approach; 83.7% of the description texts did not reveal any information on medical product status; 8.3% of the apps indicated that they have and 8.0% that they do not have medical product status.
Conclusion
Through the supplemented SARASA method, health apps in the context of cardiac arrhythmias could be identified and assigned to the target categories. Clinicians and patients have a wide choice of apps, although the app description texts do not provide sufficient information about the intended use and quality.
Zusammenfassung
Hintergrund
Smartphone-Apps werden von Patient*innen und Ärzt*innen zunehmend für medizinische Zwecke genutzt. Zahlreiche Anwendungen sind in den App-Stores verfügbar.
Ziel der Arbeit
Ziel dieser Studie war es, über einen neuartigen und erweiterten Ansatz einer halbautomatischen retrospektiven App-Store-Analyse (SARASA) Gesundheits-Apps im Zusammenhang mit kardialen Arrhythmien zu identifizieren und zu charakterisieren.
Material und Methoden
Im Dezember 2022 wurde eine automatisierte Auslese der gesamten Kategorie „Medizin“ des deutschen Apple-App-Stores durchgeführt. Dafür wurden die von den Entwicklern stammenden Beschreibungstexte und andere Metadaten in einem halbautomatischen mehrstufigen Ansatz analysiert. Die textlichen Informationen aller Extraktionsergebnisse wurden anhand definierter Suchbegriffe automatisch gefiltert.
Ergebnisse
Unter 31.564 Apps wurden 435 mit einem Anwendungszweck im Kontext kardialer Arrhythmien gefunden. Von diesen dienten 81,4 % der Bildung, der Entscheidungshilfe oder dem Krankheitsmanagement und 26,2 % boten (zusätzlich) die Möglichkeit, Informationen über den Herzrhythmus abzuleiten. Die Anwendungen richteten sich in 55,9 % der Fälle an medizinisches Fachpersonal, in 17,5 % an Studierende und/oder in 15,9 % an Patient*innen. In 31,5 % der Beschreibungstexte war die Zielgruppe nicht angegeben. Insgesamt 108 Apps (24,8 %) enthielten einen telemedizinischen Behandlungsansatz. Während 83,7 % der Beschreibungstexte keinerlei Angaben zum Medizinproduktstatus enthielten, wurde in 8,3 % ein Medizinproduktstatus bejaht und in 8,0 % ein solcher verneint.
Schlussfolgerung
Durch die erweiterte SARASA-Methode konnten Apps im Kontext kardialer Arrhythmien identifiziert und charakterisiert werden. Heutzutage steht eine große Auswahl an Apps für Kliniker*innen und Patient*innen zur Verfügung. Leider liefern die Beschreibungstexte häufig keine ausreichenden Informationen über Verwendungszweck und Qualität.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction and background
Due to the technological advances of recent years and the extensive use of smartphones and smartwatches, efforts have grown to utilise apps for medical purposes [18]. Health apps are poised to take on significant importance as a vehicle for health guidance and remote data acquisition of digital biomarkers [7]. Thus, several manufacturers provide numerous applications with a health purpose on the App store platforms [1].
While some applications address healthcare professionals and serve as educational or disease-management tools, others are intended for patients [1]. Targeting patients, the opportunity to remotely derive information on the patient’s heart rhythm, which enables the embedment into telemedicine treatment approaches, raised interest in the utilisation of health apps in the field of cardiac arrhythmias [9]. However, concerns about quality and safety exist and comprise loss of data privacy, poor data management, misdiagnosis by unvalidated sensors, and lack of evidence for improving medical endpoints [6]. Beyond this, due to the considerable increase in available applications in recent years, it remains difficult to find applications that meet one’s needs and fulfill quality claims [2].
Thus, methods are required to identify commercially available health apps and obtain information on purpose, target group, costs, certification as a medical product, and other quality distinctions [2]. Recently, we developed and published a semiautomated retrospective App Store analysis (SARASA) to identify and characterise health apps available on Apple’s (Cupertino, CA, USA) App Store and applied it to data from the German storefront [2, 3]. However, there have been some changes to the extent of the apps listed on the App Store’s overview pages since the inception of the methodology, necessitating an expanded approach of SARASA for obtaining a more comprehensive list of apps than would have been possible with our initial read-out methodology. Here, we present the first application of this novel approach for identifying health apps in the context of cardiac arrhythmias from Apple’s German App Store and their assignment to predefined categories.
Study design and investigation methods
App store read-out.
The initial description of SARASA has been published previously [2, 3] but was expanded for this work using a novel approach to improve the hit rate. In summary, the algorithm analyses the developer-provided descriptions and other metadata in the German App Store using a semiautomated multilevel approach [2, 3]. The first step is an automated total read-out of the “Medical” App Store category. For this analysis, the read-out was performed between November 30th and December 3rd, 2022. The search was limited to apps assigned to the “Medical” category (primary or secondary category).
The read-out was conducted by accessing the alphabetical listings of the applications provided by Apple on the country-specific websites of the App Store by using a script-based approach via the “iTunes Search APIs” [21]. Surprisingly, some known apps were not included in the initial read-out. Thus, we modified our method to obtain a more comprehensive dataset by separately parsing the alphabetical pages for apps starting with lower case letters and special characters, followed by an additional evaluation of the manufacturer’s store pages (stratified by device categories such as iPad or iPhone) of those manufacturers with at least one listed app in the initial read-out. For the results obtained from the manufacturers’ pages, we also had to filter out non-health apps, as these pages also listed entries for other store categories. Using the language detector of the cld2-bibliography [13], we excluded apps that did not have German or English as the main language in their description texts.
Identification of apps in the context of cardiac arrhythmias.
To identify only those apps related to cardiac arrhythmias, we subsequently defined search terms based on which the textual information of the total extraction results was automatically filtered by SARASA. We used Perl notations based on the regular expressions as used in “R” for the description of the search terms to allow for capture of different combinations of words [22]. The filtering process was conducted by an automated analysis considering the developer-provided descriptions as well as other metadata of the applications (information on the manufacturer, description texts, costs, requirements for the operating systems, evaluations by users, and the date of publication or actualisations). The used search terms are summarised in Table 1. Initially, the terms “(?<!(om|im|ro|l ))puls(?!(e of smart|ed|at|tar|ier|e practice|nitz|e studio|e.com))”, “heart[ ]*beat”, “herzschlag”, “herz[ -]*frequ”, “heart[ -]*rate” were included but then waived due to a high number of mismatches. Additionally, terms related to veterinary medicine were defined as exclusion criteria (Table 1). The resulting applications, including their metadata, were available for further investigation and categorisation.
Manual categorisation.
Subsequently, we manually reviewed the generated results to determine whether they really met the criteria for inclusion. Apps that were not found to fulfill the requirements for inclusion were removed. The remaining apps were categorised regarding purpose (“education/decision support/disease management” and/or “derivation of electrocardiogram [ECG]/photoplethysmography [PPG]/other information on the heart rhythm”), target group (“healthcare professionals” and/or “students” and/or “patients” or “target population not specified”), telemedicine approach (“yes” or “no”) and information on medical product status disclosed in the description text (“app is a medical product which is indicated by the description text” or “app is NOT a medical product which is indicated by the description text” or “medical product status not indicated by the description text”). These categories, including detailed definitions, are summarised in Table 2.
Analysis.
The apps related to cardiac arrhythmias were assessed with respect to purpose, target group, telemedicine approach, and information on medical product status. Furthermore, we investigated information on costs, length of the description texts, counts of user ratings, and average user ratings. By analysing the average user ratings, we identified the top-rated health apps in the specific category. Therefore, those apps having at least one evaluation were firstly assorted to the absolute rating counts and only the apps of the upper quartile or upper median (latter in case of < 10 apps related to the upper quartile) considered for ranking.
Results
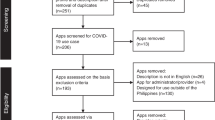
The initial read-out of the category “Medical”, obtained between November 30th (10:21:25 p.m.) and December 3rd 2022 (9:00:08 p.m.), found 28,970 apps. By parsing the manufacturer pages, we identified another 2594 apps which resulted in overall 31,564 applications in the “Medical” category at that time. Of those, for 22,713 apps (72.0%), the primary category was “Medical”, while for 8849 apps (28.0%), “Medical” was only assigned as a secondary category. By considering only those apps with German or English description texts, 22,674 apps remained for further analysis. After applying the German and English language search terms, exclusion of duplicates, as well as utilisation of the above-mentioned exclusion terms, 479 apps (2.1%) remained with a supposed context in cardiac arrhythmias. The number of hits per search term is shown in Table 1. After the manual review process, a further 44 apps were excluded since they were mismatches and unrelated to cardiac arrhythmias.
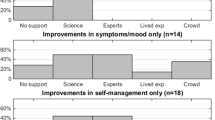
The remaining 435 apps were manually categorised according to the above-described scheme (Table 2). In all, 354 apps (81.4%) were found to deal with education, decision support, or disease management, and 114 apps (26.2%) (additionally) provided the opportunity to derive information on the heart rhythm (Fig. 1). Most of the apps were identified to be intended for healthcare professionals (243 apps; 55.9%; Fig. 1). Students and patients were addressed in 76 (17.5%) and 69 (15.9%) apps, as indicated by the description texts, respectively. In 137 apps (31.5%), the target population was not specified in the description texts. We found 108 apps (24.8%) providing a telemedicine treatment approach. Most of the description texts did not reveal any information on medical product status (364 apps; 83.7%). Based on the information provided in the description texts, we found 36 apps (8.3%), that stated to have medical device status, and 35 apps (8.0%) explicitly denying this status (Fig. 2). The median length of the description texts was 1410 characters, including spaces and characters related to formatting (min.: 65; max.: 4021). Of the 435 apps related to cardiac arrhythmias, 311 (71.5%) were free of charge. The median cost for the other apps was 5.99 € (Min.: 1.19; Max.: 1199.99).

Purpose and target group of the 435 health apps in the context of cardiac arrhythmias. ECG electrocardiogram, PPG photoplethysmography

Medical product status based on the information disclosed in the description texts
A total of 143 apps (32.9%) had customer ratings. These had a median count of five ratings (Min.: 1 rating; Max.: 89,069 ratings). The median rating score of apps with at least one rating was 4.43 (out of 5 achievable). The top-rated health apps for the specific categories are shown in Table 3. Of note, those apps having at least one evaluation were firstly sorted to the absolute rating counts, and only the apps of the upper quartile or upper median (latter in case of < 10 apps related to the upper quartile) were considered for the ranking. Our methods and findings are summarised in a graphical illustration in Fig. 3.

Graphical illustration of the methods and results. ECG electrocardiogram, PPG photoplethysmography. a Multiple counting allowed
Discussion
The technical advances of the past decade led to tremendous growth in the mobile applications market. In the past, there were efforts to gather the full extent of apps provided for the common mobile platforms and develop tools for further characterisation concerning particular features [2, 4, 11, 19]. However, those efforts were often limited to incomplete read-outs and imprecise classifications [2, 4, 11, 19]. Via the novel, expanded approach for our semiautomated method SARASA, we were able to identify overall 31,564 apps in the “Medical” category in Apple’s German App Store. We established an automated identification of apps related to cardiac arrhythmias based on search terms and found 479 apps. Of those, only 9.2% were found not to fit the purpose, necessitating manual exclusion. This indicated a good accuracy of the search algorithm and a proper selection of the search terms. As a result, a surprisingly high number of 435 apps remained in the specific context of cardiac arrhythmias.
Whether healthcare professionals or patients, users commonly rely on the information from the description texts when choosing a suitable app. However, we found that 31.5% of the description texts did not even specify the target population. This may result in misuse of these applications on the one hand or in users refraining from downloading an app on the other hand.
Besides, many of the applications identified aimed to be instantly integrated into patient care processes, thus meeting the definition of a medical product. For the European Union, such applications have to provide evidence that the requirements of the Regulation (EU) 2017/745 of the European Parliament have been fulfilled [14]. After completing the conformity assessment, the manufacturers can attach the CE certificate to their applications [14]. In the United States, applications are approved as medical products by the U. S. Food and Drug Administration (FDA) [8]. The designation, whether a health app has been approved as a medical product or not, is highly relevant for the users and should be disclosed on the download platforms. However, according to other publications, the proportion of apps providing information on the medical product status in the description text was negligible [3]. In our analysis, only in 16.3% of the description texts did the manufacturers provide information about whether the app had medical product status (or not).
Albeit some may consider the CE certificate and FDA-clearance as quality features for medical products, these labels are rather indicators of compliance with conformity requirements that allow for market participation of medical products. They are not to be seen as quality assessments [3]. There have been some efforts to further evaluate health apps regarding quality issues. Previously, we and others worked out quality criteria for software in the context of health apps [1, 5, 15, 16]. Nevertheless, the manufacturers of medical apps are still not asked to follow a standardised quality assessment. In our opinion, an EU-wide standard is required to allow for objective and reliable quality evaluation of medical apps [1]. Due to the lack of such evaluations, users often rely on the average customer ratings to choose an application that fits their purposes. This must be seen in a critical light, but ratings are one of the few information points that can be used in coming to a decision. To provide some clinical implications, we identified the top-rated apps for the most common purposes in the context of cardiac arrhythmias (Table 3).
Nowadays, the technical advances in the field of ECG and PPG allow for remote monitoring of a patient’s heart rhythm by using smartphones or smartwatches alone or in combination with coupled sensors [9, 17]. Such applications may be helpful in diagnosing rhythm disorders in symptomatic subjects, for screening, or to follow-up patients after receiving antiarrhythmic therapy [10, 17]. Health apps for diagnosing cardiac arrhythmias are increasingly accepted [12]. In a recently conducted survey, physicians predominantly saw the advantages of using wearable rhythm devices in daily practice [12]. Although the cardiological societies have published clinical advisories for health apps in the context of cardiac arrhythmias, they avoid explicitly recommending certain manufacturers and products [10, 17]. Due to the high number of 114 apps identified in our analysis to (additionally) provide the opportunity to derive information on the heart rhythm, it is challenging for physicians to maintain an overview over which applications are approved as medical products and fulfill the required quality criteria for the particular purpose.
Limitations
Our study has some imitations. Firstly, the read-out was limited to Apple’s App Store, and thus, applications only offered on other platforms are missing. Secondly, even with our expanded read-out methodology, some apps were known to be available in the store but were still missing in our acquired dataset (e.g., Fibricheck, Qompium Inc. Hasselt, Belgium). This may be due to several factors. On the one hand, Apple seems to include only apps conforming to specific (unknown) criteria on the store overview pages, probably related to an app’s performance on the store. Similarly, even via the manufacturers’ store pages (stratified by device category), there may be apps for the “Medical” category that we were unable to find. These manufacturer pages only list up to 100 apps per device category, even for manufacturers with considerably more apps in the initial read-out. Besides, there may be some manufacturers with no apps at all in the initial read-out, and we may thus have missed apps for those manufacturers as well. The high market dynamics and the associated fluctuation of apps on offer during the read-out process may also be aggravating factors. Due to the long duration for the complete read-out (aside from network speeds, also attributable to limitations in the number of requests allowed per minute by Apple’s servers), there were a few apps specified in the original lists (obtained from the overview pages), but that were missing for the metadata read-out later on. For our read-out, this was true for two apps. Thirdly, some health apps in the context of cardiac arrhythmias may have been missed due to not matching any of the keywords chosen to identify eligible apps.
Practical conclusion
-
Utilising the supplemented SARASA method, health apps in the context of cardiac arrhythmias could be identified and assigned to the target categories.
-
Clinicians and patients have a wide choice of apps, although the app description texts do not provide sufficient information about the intended use and quality.
References
Albrecht U‑V, Aumann I, Breil B, Amelung V (2016) Chancen und Risiken von Gesundheits-Apps (CHARISMHA) https://doi.org/10.24355/dbbs.084-201210110913-53
Albrecht U‑V, Hasenfuß G, von Jan U (2018) Description of cardiological Apps from the German app store: semiautomated retrospective app store analysis. JMIR Mhealth Uhealth 6:e11753. https://doi.org/10.2196/11753
Albrecht U‑V, Hillebrand U, von Jan U (2018) Relevance of trust marks and CE labels in German-language store descriptions of health Apps: analysis. JMIR Mhealth Uhealth 6:e10394. https://doi.org/10.2196/10394
Berardi G, Esuli A, Fagni T, Sebastiani F (2015) Multi-store metadata-based supervised mobile app classification. In: Proceedings of the 30th Annual ACM Symposium on Applied Computing. Association for Computing Machinery, New York, pp 585–588
Bertelsmannstiftung G (2019) AppQ – Gütekriterien-Kernset für mehr Qualitätstransparenz bei digitalen Gesundheitsanwendungen
Grundy QH, Wang Z, Bero LA (2016) Challenges in assessing mobile health app quality: a systematic review of prevalent and innovative methods. Am J Prev Med 51:1051–1059. https://doi.org/10.1016/j.amepre.2016.07.009
Hasenfuß G, Vogelmeier CF (2019) Digitale Medizin. Internist 60:317–318. https://doi.org/10.1007/s00108-019-0594-7
Health C for D and R (2021) Products and medical procedures. In: FDA. https://www.fda.gov/medical-devices/products-and-medical-procedures. Accessed 27 Feb 2023
Hermans ANL, Gawalko M, Dohmen L, van der Velden RMJ, Betz K, Duncker D, Verhaert DVM, Heidbuchel H, Svennberg E, Neubeck L, Eckstein J, Lane DA, Lip GYH, Crijns HJGM, Sanders P, Hendriks JM, Pluymaekers NAHA, Linz D (2021) Mobile health solutions for atrial fibrillation detection and management: a systematic review. Clin Res Cardiol. https://doi.org/10.1007/s00392-021-01941-9
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan G‑A, Dilaveris PE, Fauchier L, Filippatos G, Kalman JM, La Meir M, Lane DA, Lebeau J‑P, Lettino M, Lip GYH, Pinto FJ, Thomas GN, Valgimigli M, Van Gelder IC, Van Putte BP, Watkins CL, ESC Scientific Document Group (2021) 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation. Eur Heart J 42:373–498. https://doi.org/10.1093/eurheartj/ehaa612
Johann T, Stanik C, Alizadeh BAM, Maalej W (2017) SAFE: a simple approach for feature extraction from app descriptions and app reviews. In: 2017 IEEE 25th International Requirements Engineering Conference (RE), pp 21–30
Manninger M, Kosiuk J, Zweiker D, Njeim M, Antolic B, Kircanski B, Larsen JM, Svennberg E, Vanduynhoven P, Duncker D (2020) Role of wearable rhythm recordings in clinical decision making—The wEHRAbles project. Clin Cardiol 43:1032–1039. https://doi.org/10.1002/clc.23404
Ooms DS (2022) cld2: Google’s compact language detector 2
Participation E Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017on medical devices, amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and repealing Council Directives 90/385/EEC and 93/42/EEC. In: https://webarchive.nationalarchives.gov.uk/eu-exit/https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:02017R0745-20200424. Accessed 4 Mar 2023
Scherer J, Youssef Y, Dittrich F, Albrecht U‑V, Tsitsilonis S, Jung J, Pförringer D, Landgraeber S, Beck S, Back DA (2022) Proposal of a new rating concept for digital health applications in orthopedics and traumatology. Int J Environ Res Public Health 19:14952. https://doi.org/10.3390/ijerph192214952
Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M (2015) Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 3:e27. https://doi.org/10.2196/mhealth.3422
Svennberg E, Tjong F, Goette A, Akoum N, Di Biaise L, Bordachar P, Boriani G, Burri H, Conte G, Deharo J‑C, Deneke T, Drossart I, Duncker D, Han JK, Heidbuchel H, Jais P, de Oliviera Figueiredo MJ, Linz D, Lip GYH, Malaczynska-Rajpold K, Márquez M, Ploem C, Soejima K, Stiles MK, Wierda E, Vernooy K, Leclercq C, Meyer C, Pisani C, Pak H‑N, Gupta D, Pürerfellner H, Crijns HJGM, Chavez EA, Willems S, Waldmann V, Dekker L, Wan E, Kavoor P, Turagam MK, Sinner M (2022) How to use digital devices to detect and manage arrhythmias: an EHRA practical guide. Europace. https://doi.org/10.1093/europace/euac038
Walsworth DT (2012) Medical Apps: making your mobile device a medical device. Fam Pract Manag 19:10–13
Zhu H, Chen E, Xiong H, Cao H, Tian J (2014) Mobile app classification with enriched contextual information. IEEE Trans Mob Comput 13:1550–1563. https://doi.org/10.1109/TMC.2013.113
Cambridge English dictionary: meanings & definitions. https://dictionary.cambridge.org/dictionary/english/. Accessed 6 Feb 2023
iTunes search API: overview. https://developer.apple.com/library/archive/documentation/AudioVideo/Conceptual/iTuneSearchAPI/index.html#//apple_ref/doc/uid/TP40017632-CH3-SW1. Accessed 21 June 2022
R: regular expressions as used in R. https://stat.ethz.ch/R-manual/R-devel/library/base/html/regex.html. Accessed 21 June 2022
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
D. Lawin received research funding from Qompium Inc., Hasselt, Belgium, for another study unrelated to this manuscript. U. von Jan, E. Pustozerov, T. Lawrenz, C. Stellbrink and U.-V. Albrecht declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lawin, D., von Jan, U., Pustozerov, E. et al. Evaluation of a semiautomated App Store analysis for the identification of health apps for cardiac arrhythmias. Herzschr Elektrophys 34, 218–225 (2023). https://doi.org/10.1007/s00399-023-00947-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00399-023-00947-2