
Abstract
Purpose
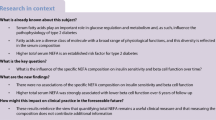
Type 2 diabetes mellitus (T2DM) is characterized by both impaired pancreatic β-cell function (BCF) and insulin resistance. In the etiology of T2DM, BCF basically determines whether a person with a certain degree of insulin resistance develops T2DM, as β-cells are able to compensatorily increase insulin secretion. The effects of dietary intake on BCF are largely unknown. Our study aim was to investigate whether dietary macronutrient intake predicts BCF.
Methods
Prospective data (median follow-up 7 years) of 303 individuals recruited from the CODAM study population (aged 40–70 years, 39% women) were analyzed. BCF was measured by C-peptide deconvolution and physiological modeling of data from a 5-point, 75-g, 2-h oral glucose tolerance test. Macronutrient intake was estimated by a 178-item Food Frequency Questionnaire.
Results
Associations adjusted for relevant covariates of baseline macronutrient intake with model-derived parameters describing BCF (glucose sensitivity, rate sensitivity or potentiation) or C-peptidogenic index were detected for trans fat [standardized regression coefficient (95%-CI) glucose sensitivity − 0.14 (− 0.26, − 0.01)] per g, cholesterol [potentiation 0.20 (0.02, 0.37)] per 100 mg, dietary fiber [glucose sensitivity 0.21 (0.08, 0.33)] per 10 g, MUFA glucose sensitivity 0.16 (0.02, 0.31) per 10 g, and polysaccharide [potentiation − 0.24 (− 0.43, − 0.05), C-peptidogenic index − 0.16 (− 0.29 − 0.03); odds ratio lowest versus highest tertile (95%-CI) rate sensitivity 1.51 (1.06, 2.15)) per 50 g.
Conclusions
In this population at high risk for developing T2DM, polysaccharide and trans fat intake were associated with worse BCF, whereas increased intake of MUFA, dietary cholesterol, and fiber were associated with better BCF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The number of people with type 2 diabetes mellitus (T2DM) is expected to rise from 366 million worldwide in 2011 to 552 million in 2030 [1]. This enormous rise in T2DM prevalence will most likely be accompanied by an increase in T2DM complications and associated diseases, including cardiovascular disease, neuropathy, nephropathy, and retinopathy, and reduced life expectancy [2,3,4]. Lifestyle modification, including eating healthier diets, has been suggested to reduce the risk of developing T2DM by 40–70% [5]. A reduced intake of total fat, saturated fat, trans fat, cholesterol, mono- and disaccharides, and an increased intake of fiber, MUFA and PUFA is recommended by several organizations, including the American Diabetes Association [6], Canadian Diabetes Association [7] and Diabetes and Nutrition Study Group of the European Association for the Study of Diabetes [8].
Results of a meta-analysis [9] of prospective cohort studies showed associations that are not in line with current dietary recommendations regarding total fat, saturated fat, MUFA, n-6 PUFA, total protein and vegetable protein. Furthermore, results were inconsistent for total carbohydrate (positive versus no association), trans fat (positive versus negative versus no association), n-3 PUFA (negative versus no association) and animal protein (positive versus no association) [9]. Moreover, evidence is inconsistent regarding the association of polysaccharide, mono- and disaccharide, and dietary fiber intake with T2DM (not evaluated in the meta-analysis) [10,11,12,13]. Although, observational studies are not an ideal approach to show causality, they can provide a good indication of the associations between dietary intake and T2DM.
These inconsistencies in results between studies may be caused by among others heterogeneity in study populations, study design, dietary assessment, and statistical analyses [14, 15]. Furthermore, T2DM represents the final stage of glucose metabolism impairmen. Besides as T2DM is a dichotomous outcome measure, it reduces the power of statistical analyses. Reduced β-cell function (BCF) can be considered as the critical determinant for the development of prediabetes and T2DM because β-cells can compensate for a decreased insulin sensitivity by upregulating insulin secretion and thereby prevent the development of T2DM. However, in the condition of reduced insulin sensitivity and decreased BCF, in which β-cells are not able to secrete sufficient insulin, hyperglycemia arises, which eventually results in prediabetes or T2DM [16, 17].
The use of BCF, as an outcome measure in epidemiological studies, has several methodological advantages. First of all, it provides physiological information on early abnormalities in glucose metabolism which eventually result in prediabetes and T2DM development. Furthermore, as BCF is a continuous measure, the issue of misclassifications of subjects with borderline blood glucose value is not relevant. Moreover, significant changes in BCF not resulting in the development of T2DM are taken into account, which is important as the impairment of BCF starts already in the normal glucose metabolism range [17]. The last two mentioned advantages increase the statistical power to detect associations [18].
So far, few studies evaluated the association between macronutrient intake and BCF in adults. These were cross-sectional studies [19,20,21,22,23] which focused on a limited selection of macronutrients, including total carbohydrate, total fat, saturated fat, MUFA, total PUFA, and dietary fiber, mainly in relation to early-phase insulin secretion (i.e. starting almost immediately after ingestion of a meal and inhibits glucose release by the liver). Based on the recommendations of diabetes organizations [6,7,8], we hypothesized an inverse association of saturated fat, trans fat, cholesterol, mono- and disaccharides intake with BCF, and a positive association of fiber, MUFA and PUFA intake with BCF. Therefore, the aim of this study was to investigate whether intake of dietary carbohydrate, fat and protein is prospectively associated with multiple components of BCF, e.g. early-phase insulin secretion, overall insulin secretion, β-cell glucose sensitivity, β-cell rate sensitivity, and β-cell potentiation factor, taking the degree of insulin sensitivity into account.
Methods
Study population and design
The current study used prospective data from the Cohort on Diabetes and Atherosclerosis Maastricht (CODAM) study. The CODAM study population consists of participants at high risk for the development of T2DM. Inclusion criteria were: age 40–70 years and either a BMI ≥ 25 kg/m2, a family history for T2DM, a history of gestational diabetes, the use of antihypertensive medication, a postprandial blood glucose ≥ 6.0 mmol/L or glycosuria. The CODAM study has been previously described in detail [24]. Briefly, 574 individuals were extensively characterized at baseline [1999–2002] with regard to their lifestyle, and cardiovascular and metabolic profile during two visits to the University’s metabolic research unit. At the follow-up examination [2006–2009], with a median follow-up period of 7.0 years (IQR 6.9–7.1), the measurements were repeated in 491 individuals (overall attrition rate 14%). The CODAM study was approved by the Medical Ethics Committee of the Maastricht University Medical Center, and all subjects gave written informed consent. For the present analyses, exclusion criteria were no participation in follow-up measurements (n = 79), previously diagnosed diabetes (defined as self-reported diagnosis and/or use of glucose lowering medication) (n = 66), suffering from any type of cancer (n = 46), incomplete oral glucose tolerance test (OGTT) data (n = 45), unreliable FFQ data (defined as > 10% missing items in the FFQ) (n = 30) and implausible total energy intake (< 800 or > 4200 kcal/day for men and < 500 or > 3500 kcal/day for women) [25] (n = 5). This resulted in a final study population of 303 individuals.
OGTT-derived measurements
Participants underwent an OGTT at baseline and after 7 years of follow-up. After an overnight fast (> 12 h), venous blood samples were collected before, and 15, 30, 60, and 120 min after ingestion of a 75 g oral glucose load. Plasma for the assessment of insulin and C-peptide was collected in EDTA tubes on ice, separated after centrifugation (3000×g for 15 min at 4 °C), and stored at − 80 °C until the assays were performed. The time between collection and storage was < 2 h. Insulin and C-peptide were measured by use of a custom duplex array of MesoScale Discovery (MesoScale Discovery, Gaithersburg, MD, USA, http://www.mesoscale.com). In short, 96 well-plates, with capture antibodies against insulin and C-peptide patterned on distinct spots in the same well, were supplied by the manufacturer. Samples (10 µL/well), detection antibodies and read buffer for electrochemiluminescence were applied according to manufacturer’s instruction and plates were read using a SECTOR® 2400 Imager. Detection ranges of the assay were 35−25,000 pg/mL for insulin and 70−50,000 pg/mL for C-peptide. Interassay coefficients of variation for insulin and C-peptide were 9.7 and 7.9%, respectively. Insulin and C-peptide values were converted from pg/mL to pmol/L using a molar mass of 5808 g for insulin and 3010 g for C-peptide. Plasma for the assessment of glucose was collected in NaF/KOx tubes on ice. Glucose was measured by use of the hexokinase method (HK-G6PD method; ABX Diagnostics Glucose HK 125, Montpellier, France).
Glucose metabolism status was defined according to the WHO 2006 criteria [26]: normal glucose metabolism (NGM; fasting plasma glucose < 6.1 mmol/L and 2 h post plasma glucose < 7.8 mmol/L), prediabetes (fasting plasma glucose levels between 6.1 and 7.0 mmol/L and/or 2 h post glucose levels between 7.8 and 11.1 mmol/L) and T2DM (fasting plasma glucose ≥ 7.0 mmol/L and/or 2 h post glucose ≥ 11.1 mmol/L).
β-cell function
As BCF consists of multiple components, it cannot be described by a single measure. Therefore, we used three mathematical model-based parameters (β-cell glucose sensitivity, β-cell potentiation factor ratio and β-cell rate sensitivity) according to a previously described model [27], and two classic, relatively simple BCF-indices (C-peptidogenic index and the ratio of the C-peptide to glucose area under the curve). Only dynamic measures of BCF were included in the analyses, because these provide a more accurate reflection of BCF than basal measures. Furthermore, these dynamic measures reflect both basal and post-load insulin secretory responses [28, 29].
The first mathematical model parameter ‘β-cell glucose sensitivity’ is the slope of the glucose-insulin secretion dose–response function [27], and represents the dependence of insulin secretion on absolute glucose concentration at any time point during the OGTT. β-cell glucose sensitivity is a sensitive index to quantify β-cell dysfunction [17, 30, 31]. The dose–response relationship is modulated by β-cell potentiation, which accounts for higher insulin secretion during the descending phase of hyperglycaemia than during the ascending phase of an OGTT, for the same glucose concentration. The second parameter β-cell potentiation is set as a positive function of time and averages 1 during the OGTT. Therefore, it represents the relative potentiation of the insulin secretion response to glucose. The β-cell potentiation parameter used in the present analysis represents the ratio of the β-cell potentiation factor at the end of the 2-h OGTT relative to the β-cell potentiation factor at the start. The third parameter ‘β-cell rate sensitivity’ is a marker of early phase insulin release, and represents the dynamic dependence of insulin secretion on the rate of change in glucose concentration [27].
The simple BCF-indices C-peptidogenic index (ΔCP30/ΔG30) and the ratio of the C-peptide to glucose area under the curve (CPAUC/GAUC) were also calculated. The C-peptidogenic index (the equivalent of the insulinogenic index) reflects early phase insulin secretion and has good discriminatory ability to predict (pre)T2DM (ROC AUCs ≥ 78%) [32].
Dietary intake
Habitual dietary intake over the past 12 months was estimated by a semi-quantitative 178 food item food frequency questionnaire (FFQ) [33, 34]. Briefly, for each food item, frequency (ranging from ‘never or less than once a month’ to ‘every day’) and amount was noted by the participants in a closed answer format. Total energy and macronutrient intake were computed using the extended version of the Dutch food composition table (NEVO) of 2001 [35].
The food items in the FFQ were selected using the Dutch National Food Consumption Survey 1987–1988 dataset. Products that accounted for at least 90% of the population mean intake of macronutrients and food groups were selected [33]. According to the Dutch National Food Consumption Survey (1997–1998), the main product groups of macronutrient intake in the Dutch population were as follows: For protein intake, the main product groups were meat and poultry, followed by milk products. For saturated fatty acids, dairy (including milk products and cheese), followed by fats, oils, and savoury sauces, and for unsaturated fatty acids the product group fats, oil and savoury sauces, followed by nuts, seeds, and snacks, meat and poultry. For mono- and disaccharides the main sources were sugar, sweets, and sweet sauces, followed by milk products, sugar-sweetened beverages and fruit, and for polysaccharides, bread, followed by potatoes and cereal products.
Anthropometric and other measurements
Body height (cm) and weight (kg) were measured to the nearest 1 cm and 0.1 kg with the participants wearing light clothing and no shoes [24]. Waist circumference, blood pressure, the presence of a history of cardiovascular disease (CVD) and blood lipid profiles, including triglycerides, total cholesterol, HDL and LDL cholesterol, were determined as described previously [36, 37]. Smoking status (never, ex, or current smoker), presence of cancer and medication use were self-reported [38]. Finally, physical activity level (min/week × intensity) was measured by the validated Short Questionnaire to Assess Health-enhancing Physical Activity (SQUASH) [39].
Statistical analysis
All analyses were performed using the software package SPSS Statistics version 23.0 for Windows (SPSS, IBM Corp, Armonk, NY, USA).
Study population characteristics were described by medians (25th-75th percentiles) or number of participants per category (% of study population). β-cell potentiation factor and the C-peptidogenic index were log-transformed as these were not normally distributed.
Linear regression analyses were performed to assess associations between macronutrient intake at baseline and BCF at follow-up. Associations were presented as standardized betas (βs) per 100 mg, 1 g, 10 g or 50 g increment for macronutrient intake, depending on the amount of the specific macronutrient intake in the CODAM population. As the distribution of β-cell rate sensitivity could not be normalized by transformations, β-cell rate sensitivity was categorized into tertiles. Multinomial regression analyses were performed for β-cell rate sensitivity, with the highest tertile [i.e. participants with the best β-cell rate sensitivity) as the reference category, and presented as odds ratios (OR (95% CI)].
Macronutrients were energy-adjusted using the residual method of Willett et al. [40] and additionally adjusted for total energy intake. Furthermore, continuous BCF measures at follow-up were adjusted for BCF at baseline (derived from a 2 h, 4-points OGTT including 0, 30, 60, and 120 min), by including baseline BCF as covariate in the regression models. In addition, to assess BCF relative to the prevailing level of insulin resistance, the Matsuda index (10,000/√G0 × I0 × mean G × mean I) [41], was included as a covariate in the regression models.
Potential confounders were included as covariates in the regression models if the regression coefficient of at least one BCF-index changed by > 10%. Accordingly, model 1 was adjusted for insulin resistance, age, and sex. Model 2 was further adjusted for BMI, mean arterial blood pressure, anti-hypertensive medication, lipid-modifying medication, family history of T2DM, total energy intake, and intake of dietary fiber, polysaccharide (except for the regression analysis of total carbohydrate), and MUFA (except for the regression analysis of total fat). Based on our data, total physical activity, CVD, smoking status, and the intake of alcohol, saturated fat, trans fat, n-3 and n-6 PUFA, mono- and disaccharides, animal protein and vegetable protein had no confounding effects on the associations of macronutrient intake with BCF, and were, therefore, not included as confounders.
Results
Population characteristics
The demographics of the total CODAM population (n = 574) and of the individuals included in the analyses of the current study (n = 303) are shown in Table 1. The median age of the final study population was 58.8 years, and 61.7% were men. Altogether, almost 80% of the participants were overweight (56.8%) or obese (22.2%). NGM, prediabetes, and newly diagnosed T2DM were present in 65.3%, 26.1%, and 8.6% of the final study population, respectively. During the follow-up period, 53 NGM persons (26.8%) developed prediabetes and 15 NGM persons (7.6%) developed T2DM. Furthermore, 32 prediabetic persons (40.5%) developed T2DM.
Relative to the total study population, the analysis population included smaller proportions of individuals with obesity, prediabetes, T2DM, CVD, lipid-lowering and blood pressure lowering medication, and overall individuals who were more physically active and had a slightly better mean BCF (Table 1).
The consumption of carbohydrate, fat, protein, and alcohol, in the analysis population, was on average 44.8, 34.9, 15.6, and 4.7 En%, respectively. Macronutrient intake was essentially the same for the analysis population and the total study population (Table 2).
Associations between baseline macronutrient intake and BCF after 7 years of follow-up
Polysaccharide intake was associated with worse β-cell potentiation factor, C-peptidogenic index [βs − 0.24 (− 0.43, − 0.05) and − 0.16 (− 0.29,− 0.03), respectively, per 50 g in fully adjusted models] and with worse β-cell rate sensitivity [OR 1.51 (95% CI 1.06, 2.15) per 50 g for the first versus the third tertile (i.e. reference group which has the best β-cell rate sensitivity)]. Furthermore, polysaccharide intake was associated with worse β-cell glucose sensitivity and overall insulin secretion, but non-significantly. Mono- and disaccharide intake were associated with better β-cell rate sensitivity in model 1 only [OR 0.76 (95% CI 0.60, 0.96) per 50 g for the first versus the third tertile (i.e. reference group which has the best β-cell rate sensitivity)] (Tables 3, 4).
Regarding fats, trans fat intake was associated with worse β-cell glucose sensitivity [βs of − 0.12 (− 0.23, − 0.01) and − 0.14 (− 0.26, − 0.01) per gram in age- and sex-adjusted, and fully adjusted models, respectively]. Furthermore, saturated fat was associated with worse β-cell rate sensitivity revealed [OR 1.52 (1.08–2.12) per 10 g for the second tertile compared with the third tertile (reference group)]. Besides, n-3 PUFA was associated with better β-cell rate sensitivity [OR of 0.01 (0.00, 0.44) per gram for the second tertile compared with the third tertile (reference group) in the fully adjusted model], and MUFA intake was associated with better β-cell glucose sensitivity [β 0.16 (0.02, 0.31) per 10 g in the fully adjusted model]. Furthermore, dietary cholesterol was associated with better β-cell potentiation factor [β 0.20 (0.02, 0.37) per 100 mg in the fully adjusted model] (Table 3).
Protein intake was not associated with any of the BCF parameters (Tables 3, 4).
Dietary fiber intake was associated with better β-cell glucose sensitivity [β 0.21 (0.08, 0.33) per 10 g in the fully adjusted model] (Table 3).
Discussion
This is the first study focusing on the prospective association of carbohydrate, fat and protein intake with multiple measures of BCF. Results revealed that trans fat and polysaccharide intake were associated with worse BCF, and MUFA, dietary cholesterol and fiber intake with better BCF.
In our study, statistically significant associations were found for polysaccharide intake with worse of β-cell rate sensitivity, β-cell potentiation factor, and C-peptidogenic index. No associations of mono- and disaccharides intake with BCF could be detected in the fully adjusted models. Our findings suggest that a higher intake of polysaccharides may result in reduced early-phase insulin release, and impaired potentiation of insulin secretion to glucose, which may explain the associations of polysaccharide intake with increased risk of T2DM observed in some [12, 42, 43], but not all [10, 44], prospective studies. It is conceivable that these findings are caused by the quality of dietary carbohydrates. According to the Dutch National Food Consumption Survey (1997–1998), the main sources of polysaccharides in the Dutch population were potatoes, bread, and cereals. Bread and cereals often consist of refined carbohydrates. These refined carbohydrates and potatoes might influence glucose homeostasis via their high glycemic load [43, 45, 46]. A high glycaemic load causes high peaks in blood glucose and insulin concentrations thereby increasing T2DM risk [47]. Regarding mono- and disaccharide intake, a prospective study revealed a positive association of fructose and glucose intake with T2DM risk and a negative association of sucrose intake with T2DM risk [10]. Whether these mono- and disaccharides subcategories also have opposite associations with BCF, which in turn might explain the null association of mono- and disaccharide intake with BCF in the current study, should be further explored.
Regarding dietary fat intake, an inverse association was observed for trans fat with β-cell glucose sensitivity. Furthermore, positive associations were observed for MUFA intake with β-cell glucose sensitivity, and for dietary cholesterol intake with β-cell potentiation factor. On top of that, n-3 PUFA was associated with a lower risk of moderate impairment of β-cell rate sensitivity, as represented by the second tertile of rate sensitivity.
In a meta-analysis, only one study showed an association between trans fat intake and increased T2DM risk [9], which may be explained by the inverse association between trans fat intake and β-cell glucose sensitivity, as observed in the present study. The mechanisms underlying the negative association between trans fat intake and β-cell glucose sensitivity observed in our study are unclear, but it is suggested that trans fat intake is positively associated with several proinflammatory markers, which in turn may cause β-cell damage [48]. Of note, over the last decades trans fat intake declined strongly [49], therefore, the relevance of this finding for today is uncertain.
The absence of an association between saturated fat intake and BCF found the current study is in line with previous studies focused on BCF [19, 21] and a meta-analysis focused on T2DM [9]. However, a prospective study showed an association of even-chain saturated fatty acids with increased T2DM risk and an association of odd-chain saturated fatty acids with decreased T2DM risk [50]. Whether these saturated fat subcategories have opposite associations with BCF, like with T2DM (55), should be further explored. Potentially involved mechanisms are inflammation, glucolipotoxicity, endoplasmic reticulum stress and oxidative stress [19, 48, 51].
The positive association of MUFA intake with β cell glucose sensitivity found in our study is in line with the positive association of MUFA intake with fasting insulin secretion observed in a previous cross-sectional study [22]. It has been hypothesized that MUFA intake preserves or even enhances β-cell proliferation and acts anti-apoptotic [51], thereby improving BCF. This contrasts with the null association observed between MUFA intake and T2DM in a meta-analysis [9].
Evidence of the associations of n-3 and n-6 PUFA intake with T2DM is conflicting [9, 52,53,54]. A positive association of n-3 PUFA with BCF was found in animal and in vitro studies [53, 55]. These studies suggest that n-3 PUFA decreases the circulating levels of inflammatory cytokines and endoplasmic reticulum stress, which in turn will result in lower levels of β-cell apoptosis [53, 55]. Two randomized controlled trials showed no association of n-3 PUFA with early-phase BCF [56, 57]. One randomized controlled trial showed an inverse association of n-6 PUFA with the early-phase BCF disposition index [56]. The inverse association found in that trial is in line with the inverse association found between n-6 PUFA intake and the β-cell potentiation factor disposition index in our study. This might implicate that n-6 PUFA intake is primarily associated with worse insulin sensitivity. However, more studies investigating the association of n-3 and n-6 with BCF are required.
Finally, literature demonstrated an association between dietary cholesterol intake and increased risk of T2DM [58, 59], which contrasts our finding that dietary cholesterol is associated with better β-cell potentiation factor. As there are no previous studies directed at dietary cholesterol and BCF, future studies are necessary to confirm our results.
Higher dietary fiber intake was associated with higher β-cell sensitivity to glucose. Evidence regarding the association between dietary fiber intake and BCF is inconsistent [19, 20, 23], and, so far only focused on early-phase insulin secretion. In line with our findings, one of these studies did not show an association between dietary fiber intake and early-phase insulin secretion [20]. Two other studies [19, 23] revealed a positive association of dietary fiber intake with early-phase insulin secretion, of which one in women only [19]. Such a protective effect of dietary fiber on BCF might be due to delayed glucose uptake from the intestine after dietary fiber intake, resulting in lower postprandial insulin and glucose peaks, and thereby decreased levels of glucotoxicity and a lower burden on β-cells [19, 48, 60]. Furthermore, it was suggested that the high satiating effect of dietary fiber decreases adiposity-associated inflammation, thereby preserving BCF [19, 48, 60]. Significant positive associations of dietary fiber with the other BCF indices might arise when differentiating dietary fiber subtypes, as cereal fibers have much stronger anti-diabetogenic effects than other types of fiber, such as fruit and vegetable fiber [61]. Therefore, future studies should evaluate the association between subcategories of dietary fiber intake and BCF.
Additional analyses were performed in which the disposition indices (DI), another commonly used method to take insulin resistance into account [62], were used as an outcome. The intake of fiber and MUFA were associated with a better DI β-cell glucose sensitivity βs of 0.23 (0.11, 0.34) and 0.25 (0.11, 0.38), respectively, per 10 g of fiber and MUFA intake. Furthermore, trans fat intake was associated with a worse DI β-cell glucose sensitivity (β − 0 .14 (− 0.25, − 0.03) per g). Finally, the intake of saturated fat was associated with worse DI β-cell glucose sensitivity and DI C-peptidogenic index per 10 g of intake (βs − 0.22 (− 0.38, − 0.07) and − 0.18 (− 0.38, − 0.01), respectively)(see Supplementary Tables 1 and 2). There are some methodological considerations using the disposition index. First of all, a hyperbolic function between BCF and insulin sensitivity has been suggested as a requirement to apply the disposition index. In our data, such a hyperbolic function was not present, which is in line with some other studies [63, 64]. In addition, artificial relations between indices of BCF and insulin sensitivity may arise when these indices are obtained from insulin and glucose concentrations during a single OGTT [31, 63].
Strengths and limitations
Strengths of this study are the prospective study design, and the inclusion of participants covering the total glucose metabolism spectrum from NGM to newly diagnosed T2DM, which improves external validity. Other strengths are the simultaneous use of multiple dynamic BCF-indices to assess different aspects of BCF, including both mathematical model parameters and simple BCF measures (66), and the extensive adjustment of our data analyses for potential confounders. However, a methodological consideration is that the CODAM study population is at relatively high risk of developing T2DM, which may reduce external validity. Furthermore, both the exposure and outcome measures were estimated by indirect methods. Even though the FFQ is prone to measurement error, FFQs are well suited to rank individuals according to their intake [65]. However, there may be selective misreporting of fat, sugar, and possibly alcohol, and energy adjustment cannot correct for such selective misreporting. In an attempt to minimize the risk of selective over- or underreporting of specific macronutrients, including sugar and fat, analyses were corrected for BMI; also, persons with previously diagnosed T2DM were excluded from analyses. The FFQ applied in the present study had a reasonable to good reproducibility (> 70%) and validity (60%) for macronutrient intake [34].
As there is no golden standard available to measure BCF, the OGTT was used in this study. Advantages of the OGTT are the relatively good reflection of the physiological insulin secretory response to a glucose load and the provision of a good compromise between accuracy and applicability in an epidemiological study [28, 66].
As BCF is one of the hallmarks of T2DM, the associations of macronutrient intake with multiple aspects of BCF can provide insights into the effects of macronutrients on early abnormalities in glucose metabolism that eventually result in prediabetes and T2DM. As this is the first prospective study evaluating the associations of macronutrient intakes with multiple BCF components, additional observational studies, followed by intervention studies are needed to verify the observed associations. In addition, as nutrients are not being consumed in isolation, an important next step will be to investigate the associations of specific food groups and dietary patterns with BCF.
Conclusion
In a population at high risk of developing T2DM, MUFA, dietary cholesterol, and dietary fiber intake were associated with a better BCF, whereas polysaccharide and trans fat intake were associated with a worse BCF. Our results support the recommendations of several diabetes organizations regarding MUFA, trans fat, and dietary fiber intake. As this is the first prospective study evaluating the associations of macronutrient intakes with multiple BCF components, additional studies are needed to verify the observed associations.
Abbreviations
- BCF:
-
β-cell function
- CODAM:
-
Cohort on Diabetes and Atherosclerosis Maastricht
- CP:
-
C-peptide
- CVD:
-
Cardiovascular disease
- DI:
-
Disposition Index
- G:
-
Glucose
- I:
-
Insulin
- NGM:
-
Normal glucose metabolism
- OGTT:
-
Oral glucose tolerance test
- T2DM:
-
Type 2 diabetes mellitus
References
Whiting DR, Guariguata L, Weil C, Shaw J (2011) IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract 94(3):311–321. https://doi.org/10.1016/j.diabres.2011.10.029
Prevention of Diabetes Mellitus (1994)
Harris MI, Klein R, Welborn TA, Knuiman MW (1992) Onset of NIDDM occurs at least 4–7 year before clinical diagnosis. Diabetes care 15(7):815–819
Tuomilehto J, Rastenyte D, Qiao Q, Jakovljevic D (1997) Epidemiology of macrovascular disease and hypertension in diabetes mellitus. In: Alberti KGMM, Zimmet P, De Fronzo RA (eds) International textbook of diabetes mellitus. Wiley, Hoboken. https://doi.org/10.1002/0470862092.d1002
Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M (2012) Prediabetes: a high-risk state for diabetes development.Lancet 379(9833):2279–2290
Evert AB, Boucher JL, Cypress M, Dunbar SA, Franz MJ, Mayer-Davis EJ, Neumiller JJ, Nwankwo R, Verdi CL, Urbanski P, Yancy WS, Jr (2014) Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 37 Suppl 1:120-143. https://doi.org/10.2337/dc14-S120
Dworatzek PD, Arcudi K, Gougeon R, Husein N, Sievenpiper JL, Williams SL (2013) Nutrition therapy. Can J Diabetes 37(Suppl 1):S45-55. https://doi.org/10.1016/j.jcjd.2013.01.019
Mann J, De Leeuw I, Hermansen K, Karamanos B, Karlström B, Katsilambros N, Riccardi G, Rivellese A, Rizkalla S, Slama G (2004) Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr Metab Cardiovasc Dis 14(6):373–394
Alhazmi A, Stojanovski E, McEvoy M, Garg ML (2012) Macronutrient intakes and development of type 2 diabetes: a systematic review and meta-analysis of cohort studies. J Am Coll Nutr 31(4):243–258
Meyer KA, Kushi LH, Jacobs DR Jr, Slavin J, Sellers TA, Folsom AR (2000) Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am J Clin Nutr 71(4):921–930
Schulze MB, Schulz M, Heidemann C, Schienkiewitz A, Hoffmann K, Boeing H (2008) Carbohydrate intake and incidence of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Br J Nutr 99(5):1107–1116. https://doi.org/10.1017/s0007114507853360
Hodge AM, English DR, O’Dea K, Giles GG (2004) Glycemic index and dietary fiber and the risk of type 2 diabetes. Diabetes Care 27(11):2701–2706
Salmeron J, Ascherio A, Rimm EB, Colditz GA, Spiegelman D, Jenkins DJ, Stampfer MJ, Wing AL, Willett WC (1997) Dietary fiber, glycemic load, and risk of NIDDM in men. Diabetes Care 20(4):545–550
Deeks JJ, Altman DG, Bradburn MJ Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey-Smith G, Altman D (eds) Systematic reviews in health care: meta-analysis in context, 2nd edn. Wiley, Hoboken, pp 285–312. http://download.xuebalib.com/xuebalib.com.2787.pdf
Dennis LK, Snetselaar LG, Smith BJ, Stewart RE, Robbins ME (2004) Problems with the assessment of dietary fat in prostate cancer studies. Am J Epidemiol 160(5):436–444
Nolan CJ, Damm P, Prentki M (2011) Type 2 diabetes across generations: from pathophysiology to prevention and management. Lancet 378(9786):169–181. https://doi.org/10.1016/s0140-6736(11)60614-4
Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA (2005) beta-Cell function in subjects spanning the range from normal glucose tolerance to overt diabetes: a new analysis. J Clin Endocrinol Metab 90(1):493–500. https://doi.org/10.1210/jc.2004-1133
Altman DG, Royston P (2006) The cost of dichotomising continuous variables. BMJ 332(7549):1080. https://doi.org/10.1136/bmj.332.7549.1080
Heikkila HM, Krachler B, Rauramaa R, Schwab US (2014) Diet, insulin secretion and insulin sensitivity–the dose-responses to exercise training (DR’s EXTRA) Study (ISRCTN45977199). Br J Nutr 112(9):1530–1541. https://doi.org/10.1017/s0007114514002426
Ylonen K, Saloranta C, Kronberg-Kippila C, Groop L, Aro A, Virtanen SM (2003) Associations of dietary fiber with glucose metabolism in nondiabetic relatives of subjects with type 2 diabetes: the Botnia Dietary Study. Diabetes Care 26(7):1979–1985
Mayer-Davis EJ, Levin S, Bergman RN, D’Agostino RB Jr, Karter AJ, Saad MF (2001) Insulin secretion, obesity, and potential behavioral influences: results from the Insulin Resistance Atherosclerosis Study (IRAS). Diabetes Metab Res Rev 17(2):137–145
Rojo-Martinez G, Esteva I, Ruiz de Adana MS, Garcia-Almeida JM, Tinahones F, Cardona F, Morcillo S, Garcia-Escobar E, Garcia-Fuentes E, Soriguer F (2006) Dietary fatty acids and insulin secretion: a population-based study. Eur J Clin Nutr 60(10):1195–1200. https://doi.org/10.1038/sj.ejcn.1602437
Liese AD, Schulz M, Fang F, Wolever TM, D’Agostino RB Jr, Sparks KC, Mayer-Davis EJ (2005) Dietary glycemic index and glycemic load, carbohydrate and fiber intake, and measures of insulin sensitivity, secretion, and adiposity in the Insulin Resistance Atherosclerosis Study. Diabetes Care 28(12):2832–2838
Kruijshoop M, Feskens EJ, Blaak EE, de Bruin TW (2004) Validation of capillary glucose measurements to detect glucose intolerance or type 2 diabetes mellitus in the general population. Clin Chim Acta 341(1–2):33–40. https://doi.org/10.1016/j.cccn.2003.10.033
Willett WC (1998) Issues in analysis and presentation of dietary data. In: willett W (ed) Nutritional Epidemiology, 2nd edn. Oxford University Press, New York
Organization WH (2006) Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia: report of a WH
Mari A, Schmitz O, Gastaldelli A, Oestergaard T, Nyholm B, Ferrannini E (2002) Meal and oral glucose tests for assessment of beta -cell function: modeling analysis in normal subjects. Am J Physiol Endocrinol Metab 283(6):1159–1166. https://doi.org/10.1152/ajpendo.00093.2002
Cersosimo E, Solis-Herrera C, Trautmann ME, Malloy J, Triplitt CL (2014) Assessment of pancreatic beta-cell function: review of methods and clinical applications. Curr Diabetes Rev 10(1):2–42
Cobelli C, Toffolo GM, Dalla Man C, Campioni M, Denti P, Caumo A, Butler P, Rizza R (2007) Assessment of β-cell function in humans, simultaneously with insulin sensitivity and hepatic extraction, from intravenous and oral glucose tests. A J Physiol Endocrinol Metab 293(1):E1–E15
Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Pettiti M, Natali A, Mari A, DeFronzo RA (2003) Predominant role of reduced beta-cell sensitivity to glucose over insulin resistance in impaired glucose tolerance. Diabetologia 46(9):1211–1219. https://doi.org/10.1007/s00125-003-1169-6
Ferrannini E, Mari A (2014) beta-Cell function in type 2 diabetes. Metabolism 63(10):1217–1227. https://doi.org/10.1016/j.metabol.2014.05.012
den Biggelaar LJ, Sep SJ, Eussen SJ, Mari A, Ferrannini E, van Greevenbroek MM, van der Kallen CJ, Schalkwijk CG, Stehouwer CD, Dagnelie PC (2016) Discriminatory ability of simple OGTT-based beta cell function indices for prediction of prediabetes and type 2 diabetes: the CODAM study. Diabetologia. https://doi.org/10.1007/s00125-016-4165-3
OCKÉ MC, BUENO-DE-MESQUITA HB, GODDIJN HE, JANSEN A, POLS MA, VAN STAVEREN WA KROMHOUTD (1997) The Dutch EPIC Food Frequency Questionnaire. I. Description of the Questionnaire, and Relative Validity and Reproducibility for Food Groups
Ocké MC, Bueno-de-Mesquita HB, Pols MA, Smit HA, van Staveren WA, Kromhou TD (1997) The Dutch EPIC Food Frequency Questionnaire. II. Relative Validity and Reproducibility for Nutrients. Int J Epidemiol 26(1):S49–S58
Stichting N (2001) NEVO tabel, Nederlands Voedingsstoffenbestand 2001. Voedingscentrum, Den Haag
Brouwers MC, Cantor RM, Kono N, Yoon JL, van der Kallen CJ, Bilderbeek-Beckers MA, van Greevenbroek MM, Lusis AJ, de Bruin TW (2006) Heritability and genetic loci of fatty liver in familial combined hyperlipidemia. J Lipid Res 47(12):2799–2807. https://doi.org/10.1194/jlr.M600312-JLR200
Jacobs M, van Greevenbroek MM, van der Kallen CJ, Ferreira I, Blaak EE, Feskens EJ, Jansen EH, Schalkwijk CG, Stehouwer CD (2009) Low-grade inflammation can partly explain the association between the metabolic syndrome and either coronary artery disease or severity of peripheral arterial disease: the CODAM study. Eur J Clin Invest 39(6):437–444. https://doi.org/10.1111/j.1365-2362.2009.02129.x
van Greevenbroek MM, Jacobs M, van der Kallen CJ, Vermeulen VM, Jansen EH, Schalkwijk CG, Ferreira I, Feskens EJ, Stehouwer CD (2011) The cross-sectional association between insulin resistance and circulating complement C3 is partly explained by plasma alanine aminotransferase, independent of central obesity and general inflammation (the CODAM study). Eur J Clin Invest 41(4):372–379. https://doi.org/10.1111/j.1365-2362.2010.02418.x
Wendel-Vos GW, Schuit AJ, Saris WH, Kromhout D (2003) Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol 56(12):1163–1169
Willett WC, Howe GR, Kushi LH (1997) Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr 65 (4 Suppl):1220–1228. discussion 1229S–1231S
Matsuda M, DeFronzo RA (1999) Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22(9):1462–1470
Sluijs I, van der Schouw YT, van der AD, Spijkerman, Hu AM, Grobbee FB, Beulens DE JW (2010) Carbohydrate quantity and quality and risk of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition-Netherlands (EPIC-NL) study. Am J Clin Nutr 92(4):905–911. https://doi.org/10.3945/ajcn.2010.29620
AlEssa HB, Bhupathiraju SN, Malik VS, Wedick NM, Campos H, Rosner B, Willett WC, Hu FB (2015) Carbohydrate quality and quantity and risk of type 2 diabetes in US women. Am J Clin Nutr 102(6):1543–1553. https://doi.org/10.3945/ajcn.115.116558
Barclay AW, Flood VM, Rochtchina E, Mitchell P, Brand-Miller JC (2007) Glycemic index, dietary fiber, and risk of type 2 diabetes in a cohort of older Australians. Diabetes Care 30(11):2811–2813. https://doi.org/10.2337/dc07-0784
Liu S, Manson JE, Stampfer MJ, Hu FB, Giovannucci E, Colditz GA, Hennekens CH, Willett WC (2000) A prospective study of whole-grain intake and risk of type 2 diabetes mellitus in US women. Am J Pub Health 90(9):1409
Atkinson FS, Foster-Powell K, Brand-Miller JC (2008) International tables of glycemic index and glycemic load values: 2008. Diabetes care 31(12):2281–2283
Bhupathiraju SN, Tobias DK, Malik VS, Pan A, Hruby A, Manson JE, Willett WC, Hu FB (2014) Glycemic index, glycemic load, and risk of type 2 diabetes: results from 3 large US cohorts and an updated meta-analysis. Am J Clin Nutr 100(1):218–232. https://doi.org/10.3945/ajcn.113.079533
Thomas T, Pfeiffer AF (2012) Foods for the prevention of diabetes: how do they work? Diabetes Metab Res Rev 28(1):25–49. https://doi.org/10.1002/dmrr.1229
Van Rossum C, Fransen H, Verkaik-Kloosterman J, Buurma-Rethans E, Ocké M (2011) Dutch National Food Consumption Survey 2007–2010: Diet of children and adults aged 7 to 69 years. RIVM rapport 350050006
Forouhi NG, Koulman A, Sharp SJ, Imamura F, Kroger J, Schulze MB, Crowe FL, Huerta JM, Guevara M, Beulens JW, van Woudenbergh GJ, Wang L, Summerhill K, Griffin JL, Feskens EJ, Amiano P, Boeing H, Clavel-Chapelon F, Dartois L, Fagherazzi G, Franks PW, Gonzalez C, Jakobsen MU, Kaaks R, Key TJ, Khaw KT, Kuhn T, Mattiello A, Nilsson PM, Overvad K, Pala V, Palli D, Quiros JR, Rolandsson O, Roswall N, Sacerdote C, Sanchez MJ, Slimani N, Spijkerman AM, Tjonneland A, Tormo MJ, Tumino R, van der AD, van der Schouw, Langenberg YT, Riboli C, Wareham E NJ (2014) Differences in the prospective association between individual plasma phospholipid saturated fatty acids and incident type 2 diabetes: the EPIC-InterAct case-cohort study. Lancet Diabetes Endocrinol 2(10):810–818. https://doi.org/10.1016/s2213-8587(14)70146-9
Morgan NG, Dhayal S, Diakogiannaki E, Welters HJ (2008) The cytoprotective actions of long-chain mono-unsaturated fatty acids in pancreatic beta-cells. Biochem Soc Trans 36(Pt 5):905–908. https://doi.org/10.1042/bst0360905
Dixon G, Nolan J, McClenaghan NH, Flatt PR, Newsholme P (2004) Arachidonic acid, palmitic acid and glucose are important for the modulation of clonal pancreatic beta-cell insulin secretion, growth and functional integrity. Clin Sci (London: 1979) 106(2):191–199. https://doi.org/10.1042/cs20030261
Wang J, Song MY, Bae UJ, Lim JM, Kwon KS, Park BH (2015) n-3 Polyunsaturated fatty acids protect against pancreatic beta-cell damage due to ER stress and prevent diabetes development. Mol Nutr Food Res 59(9):1791–1802. https://doi.org/10.1002/mnfr.201500299
Wu JHY, Marklund M, Imamura F, Tintle N, Ardisson Korat AV, de Goede J, Zhou X, Yang WS, de Oliveira Otto MC, Kroger J, Qureshi W, Virtanen JK, Bassett JK, Frazier-Wood AC, Lankinen M, Murphy RA, Rajaobelina K, Del Gobbo LC, Forouhi NG, Luben R, Khaw KT, Wareham N, Kalsbeek A, Veenstra J, Luo J, Hu FB, Lin HJ, Siscovick DS, Boeing H, Chen TA, Steffen B, Steffen LM, Hodge A, Eriksdottir G, Smith AV, Gudnason V, Harris TB, Brouwer IA, Berr C, Helmer C, Samieri C, Laakso M, Tsai MY, Giles GG, Nurmi T, Wagenknecht L, Schulze MB, Lemaitre RN, Chien KL, Soedamah-Muthu SS, Geleijnse JM, Sun Q, Harris WS, Lind L, Arnlov J, Riserus U, Micha R, Mozaffarian D (2017) Omega-6 fatty acid biomarkers and incident type 2 diabetes: pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies. Lancet Diabetes Endocrinol 5(12):965–974. https://doi.org/10.1016/s2213-8587(17)30307-8
Bhaswant M, Poudyal H, Brown L (2015) Mechanisms of enhanced insulin secretion and sensitivity with n-3 unsaturated fatty acids. J Nutr Biochem 26(6):571–584. https://doi.org/10.1016/j.jnutbio.2015.02.001
Giacco R, Cuomo V, Vessby B, Uusitupa M, Hermansen K, Meyer BJ, Riccardi G, Rivellese AA (2007) Fish oil, insulin sensitivity, insulin secretion and glucose tolerance in healthy people: is there any effect of fish oil supplementation in relation to the type of background diet and habitual dietary intake of n-6 and n-3 fatty acids? Nutr Metab Cardiovasc Dis 17(8):572–580. https://doi.org/10.1016/j.numecd.2006.06.006
Vessby B, Uusitupa M, Hermansen K, Riccardi G, Rivellese AA, Tapsell LC, Nälsén C, Berglund L, Louheranta A, Rasmussen B (2001) Substituting dietary saturated for monounsaturated fat impairs insulin sensitivity in healthy men and women: The KANWU Study. Diabetologia 44(3):312–319
Meyer KA, Kushi LH, Jacobs DR Jr, Folsom AR (2001) Dietary fat and incidence of type 2 diabetes in older Iowa women. Diabetes Care 24(9):1528–1535
Salmeron J, Hu FB, Manson JE, Stampfer MJ, Colditz GA, Rimm EB, Willett WC (2001) Dietary fat intake and risk of type 2 diabetes in women. Am J Clin Nutr 73(6):1019–1026
Juntunen KS, Laaksonen DE, Poutanen KS, Niskanen LK, Mykkanen HM (2003) High-fiber rye bread and insulin secretion and sensitivity in healthy postmenopausal women. Am J Clin Nutr 77(2):385–391
Schulze MB, Schulz M, Heidemann C, Schienkiewitz A, Hoffmann K, Boeing H (2007) Fiber and magnesium intake and incidence of type 2 diabetes: a prospective study and meta-analysis. Arch Intern Med 167(9):956–965. https://doi.org/10.1001/archinte.167.9.956
Bergman RN, Ader M, Huecking K, Van Citters G (2002) Accurate assessment of β-cell function the hyperbolic correction. Diabetes 51(suppl 1):S212–S220
Retnakaran R, Shen S, Hanley AJ, Vuksan V, Hamilton JK, Zinman B (2008) Hyperbolic relationship between insulin secretion and sensitivity on oral glucose tolerance test. Obesity (Silver Spring) 16(8):1901–1907. https://doi.org/10.1038/oby.2008.307
Solomon TP, Malin SK, Karstoft K, Knudsen SH, Haus JM, Laye MJ, Pedersen M, Pedersen BK, Kirwan JP (2014) Determining pancreatic β-cell compensation for changing insulin sensitivity using an oral glucose tolerance test. Am J Physiol Endocrinol Metab 307(9):E822–E829
Thompson FE, Subar AF (2008) Dietary assessment methodology. Nut Prevent Treat Dis 2:3–39
Ferrannini E, Mari A (2004) Beta cell function and its relation to insulin action in humans: a critical appraisal. Diabetologia 47(5):943–956
Acknowledgements
Part of this work was supported by Grants of the Netherlands Organization for Scientific Research (940-35-034) and the Dutch Diabetes Research Foundation (98.901). The Netherlands Organization for Scientific Research and the Dutch Diabetes Research Foundation had no role in the design, analysis or writing of this article.
Author information
Authors and Affiliations
Contributions
LdB and SS performed mathematical model analyses, statistical analyses, interpreted the data and wrote the manuscript; SS performed mathematical model analyses, contributed to the conception and interpretation of the data, to data analyses, and participated in drafting the article, and revising it critically for important intellectual content; SE and PD contributed to the conception and interpretation of the data, to data analyses, and participated in drafting the article, and revising it critically for important intellectual content; AM and EF designed the mathematical model, provided support in performing mathematical analyses, contributed to data quality of the mathematical analyses and made important contributions to the interpretation of the BCF data; MvG, CvdK contributed to data acquisition and study coordination; CS provided advice and contributed to the conception of the data, to data acquisition and to study coordination; All authors contributed to and/or provided critical comments and suggestions to the manuscript, and all authors reviewed the final draft of the manuscript and gave final approval of the version to be published. PD is the guarantor of this work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
den Biggelaar, L.J.C.J., Eussen, S.J.P.M., Sep, S.J.S. et al. Prospective associations of dietary carbohydrate, fat, and protein intake with β-cell function in the CODAM study. Eur J Nutr 58, 597–608 (2019). https://doi.org/10.1007/s00394-018-1644-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-018-1644-y