
Abstract
Aims
As there is limited evidence regarding the prognostic impact of prior left ventricular ejection fraction (LVEF) in patients with heart failure with mildly reduced ejection fraction (HFmrEF), this study investigates the prognostic impact of longitudinal changes in LVEF in patients with HFmrEF.
Methods
Consecutive patients with HFmrEF (i.e. LVEF 41–49% with signs and/or symptoms of HF) were included retrospectively in a monocentric registry from 2016 to 2022. Based on prior LVEF, patients were categorized into three groups: stable LVEF, improved LVEF, and deteriorated LVEF. The primary endpoint was 30-months all-cause mortality (median follow-up). Secondary endpoints included in-hospital and 12-months all-cause mortality, as well as HF-related rehospitalization at 12 and 30 months. Kaplan–Meier and multivariable Cox proportional regression analyses were applied for statistics.
Results
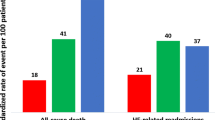
Six hundred eighty-nine patients with HFmrEF were included. Compared to their prior LVEF, 24%, 12%, and 64% had stable, improved, and deteriorated LVEF, respectively. None of the three LVEF groups was associated with all-cause mortality at 12 (p ≥ 0.583) and 30 months (31% vs. 37% vs. 34%; log rank p ≥ 0.376). In addition, similar rates of 12- (p ≥ 0.533) and 30-months HF-related rehospitalization (21% vs. 23% vs. 21%; log rank p ≥ 0.749) were observed. These findings were confirmed in multivariable regression analyses in the entire study cohort.
Conclusion
The transition from HFrEF and HFpEF towards HFmrEF is very common. However, prior LVEF was not associated with prognosis, likely due to the persistently high dynamic nature of LVEF in the follow-up period.
Graphical Abstract

Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Within the last decades, the prevalence of heart failure (HF) has steadily increased due to ongoing demographic changes related to an overall ageing population [1, 2]. Global estimates have shown that approximately 64 million people are affected by HF and data from the United States suggests that total health care expenditure for the management of HF could rise to 70 billion US-dollars by 2030 [3, 4]. Even though HF can be described through a variety of parameters, clinical signs, or symptomatology, it is most commonly classified by left ventricular ejection fraction (LVEF) [5, 6]. Until recently, patients were either divided into the category of HF with reduced (HFrEF) or preserved ejection fraction (HFpEF). However, within the past years, the European and American HF guidelines have introduced an additional category of HF with an LVEF of 41–49%, the so-called heart failure with mildly reduced ejection fraction (HFmrEF) [5, 6]. This category accounts for 16–24% of patients with HF [7, 8]. Furthermore, the category of HF with improved ejection fraction (HFimpEF) has been defined in a widely accepted position paper on the universal definition and classification of HF [9]. This classification aims to consider the potential prognostic implications of longitudinal changes of LVEF. According to this position paper, HFimpEF should be defined by a baseline LVEF ≤ 40% and a second measurement of LVEF > 40% with a ≥ 10% increase from baseline LVEF. Recent evidence from the ESC Heart Failure Long-Term Registry suggests that despite improvements in medical management, mortality of HF remains high with 1-year mortality rates of 8.8%, 7.8%, and 6.4% for HFrEF, HFmrEF, and HFpEF, respectively [7]. Within the same registry, Chioncel et al. were able to demonstrate a nearly linear increase in mortality and HF-related rehospitalization across every decile of reduced LVEF [7, 10]. However, since LVEF is a dynamic parameter, prognostic implications of LVEF changes over time must be considered to properly guide medical management of patients. As previous studies have demonstrated, improvement of LVEF in patients suffering from HFrEF is associated with favourable outcomes compared to patients with persistently reduced LVEF and maybe even those with stable HFpEF [11, 12]. Accordingly, deterioration of LVEF over time was observed to coincide with a worse prognosis [13,14,15]. Despite the importance of longitudinal changes in LVEF, there is limited evidence regarding the prognostic impact of prior LVEF in patients with HFmrEF. Since the category of HFmrEF was recently introduced, evidence guiding clinical decision-making for this cohort remains limited and the few guideline recommendations currently available are predominantly based on post hoc analyses of prior trials enrolling patients within the LVEF range of HFmrEF (e.g. CHARM-Preserved [16], TOPCAT [17], or PARAGON-HF [18]).
Therefore, the present study investigates the prognostic impact of prior LVEF in consecutive patients hospitalized with HFmrEF within a large-scaled retrospective registry-based analysis.
Methods
Study patients, design, and data collection
For the present study, all consecutive patients hospitalized with HFmrEF at one University Medical Centre were included from January 2016 to December 2022, as recently published [19]. Using the electronic hospital information system, all relevant clinical data related to the index event were documented, such as baseline characteristics; vital signs on admission; prior medical history; prior medical treatment; length of index hospital and intensive care unit (ICU) stay; laboratory values; data derived from all non-invasive or invasive cardiac diagnostics and device therapies, such as echocardiographic data, coronary angiography, and data being derived from prior or newly implanted cardiac devices. Every re-visit at the outpatient clinic or rehospitalizations related to HF or adverse cardiac events were documented until the end of the year 2022.
The present study is derived from the “Heart Failure With Mildly Reduced Ejection Fraction Registry” (HARMER), representing a retrospective single-centre registry including consecutive patients with HFmrEF hospitalized at the University Medical Centre Mannheim (UMM), Germany (clinicaltrials.gov identifier, NCT05603390). The registry was carried out according to the principles of the Declaration of Helsinki and was approved by the medical ethics committee II of the Medical Faculty Mannheim, University of Heidelberg, Germany (ethical approval code, 2022–818).
Inclusion and exclusion criteria
All consecutive patients ≥ 18 years of age hospitalized with HFmrEF at one institution were included. Patients without echocardiographic assessment of LVEF prior to the index hospitalization were excluded. Furthermore, patients with a prior LVEF ≤ 40% but an LVEF improvement < 10% were excluded [9]. All included patients underwent at least one standardized transthoracic echocardiography at the cardiologic department at index hospitalization, where the diagnosis of HFmrEF was assessed. The diagnosis of HFmrEF was determined according to the “2021 European Society of Cardiology (ESC) Guidelines for the diagnosis and treatment of acute and chronic HF” [20]. Accordingly, all patients with an LVEF of 41–49% and symptoms and/or signs of HF were included. The presence of elevated amino-terminal prohormone of brain natriuretic peptide (NT-proBNP) levels and other evidence of structural heart disease were considered to make the diagnosis more likely but were not mandatory for the diagnosis of HFmrEF. Transthoracic echocardiography was exclusively performed by attending cardiologists or under their direct supervision in clinically stable patients and in accordance with current European guidelines [21] to ensure high standards of echocardiographic examination. The corresponding cardiologists were blinded to the final study analysis. LVEF was routinely measured by the established biplane method of disks summation (modified Simpson’s rule) recommended by the American Society of Echocardiography and the European Association of Cardiovascular Imaging [22]. All echocardiographic examinations and reports of the index admission were re-assessed post hoc by two independent cardiologists. In cases of ambiguous findings or documentation, echocardiographic source data was re-assessed based on the available Digital Imaging and Communications in Medicine (DICOM) files. Information on LVEF before the index admission was obtained through comprehensive investigation of all patient-related documents stored in the electronic hospital information system, including previous visits at our University Medical Centre Mannheim and available medical reports of other clinics or outpatient cardiology visits. In accordance with the index echocardiography, data on prior LVEF was only ascertained from documented transthoracic echocardiographic examinations measuring LVEF with the modified Simpson’s rule. To clarify, data on LVEF during the index admission was solely ascertained from inpatients, whereas data on prior LVEF was derived from patients in both the inpatient and outpatient settings.
Risk stratification
For the present study, risk stratification was performed according to longitudinal changes of LVEF, and patients were divided into the following three groups in line with the universal definition and classification of HF [9]: stable LVEF (i.e. prior LVEF of 41–49%), improved LVEF (i.e. prior LVEF ≤ 40% and an improvement ≥ 10% compared to the prior LVEF), and deteriorated LVEF (i.e. prior LVEF ≥ 50%). The value of prior LVEF used for the categorization of patients into the three groups (i.e. stable, improved, and deteriorated) was defined as the most recent available LVEF assessment preceding the index hospitalization. No maximum time interval between the index admission and the previous echocardiographic assessment of prior LVEF was applied for the main analyses. Subanalyses with a minimum time interval of 1 month and a maximum time interval of 12 as well as 24 months between the prior and index echocardiography were performed. Furthermore, prognosis of patients with stable, improved, and deteriorated LVEF was also investigated stratified by the etiology of heart failure (i.e. ischemic and non-ischemic cardiomyopathy). Ischemic cardiomyopathy (ICM) comprised patients with prior documented coronary artery disease (CAD) or newly diagnosed CAD assessed by coronary angiography at the index hospitalization sufficient to cause myocardial dysfunction. Identification of CAD (i.e. at least one relevant stenosis of one epicardial coronary artery of more than 50%) was based on the judgment of the investigating interventional cardiologist during routine care. All coronary angiograms and reports were re-assessed post hoc by two independent interventional cardiologists to determine whether the CAD is sufficient for causality of myocardial dysfunction [23]. The group of non-ischemic cardiomyopathy (NICM) comprised all patients with other etiologies of heart failure as listed in Table 2 (i.e. primary non-ischemic cardiomyopathy [23], hypertensive cardiomyopathy [24], congenital heart disease, valvular heart disease [25, 26], tachycardia-induced [27], and pacemaker-induced cardiomyopathy [28]) excluding patients with unknown etiology. The parameter of right ventricular dysfunction (RVD) used in multivariable analyses was defined as a tricuspid annular plane systolic excursion (TAPSE) of < 17 mm. In patients with a history of cardiac surgery, systolic velocity of the tricuspid annulus (S′) < 9.5 cm/s was additionally considered to confirm RVD.
Study endpoints
The primary endpoint was long-term all-cause mortality. Long-term was defined as the median time of clinical follow-up in months (i.e. 30 months). Secondary endpoints comprised in-hospital all-cause mortality, all-cause mortality at 12 months, rehospitalization for worsening HF at 12 and 30 months as well as cardiac rehospitalization, acute myocardial infarction (AMI), stroke, coronary revascularization, and major adverse cardiac and cerebrovascular events (MACCE) at long-term follow-up as well as changes in LVEF and NT-pro BNP levels during the follow-up period. All-cause mortality was documented using the electronic hospital information system and by directly contacting state resident registration offices (“bureau of mortality statistics”). HF-related hospitalization was defined as a rehospitalization due to worsening HF requiring intravenous diuretic therapy. HF-related rehospitalization comprised patients with hospitalization due to worsening HF as the primary cause or as a result of another cause but associated with worsening HF at the time of admission, or as a result of another cause but complicated by worsening HF during its cause. Cardiac rehospitalization was defined as rehospitalization due to a primary cardiac condition, including worsening HF, AMI, coronary revascularization, and symptomatic atrial or ventricular arrhythmias. MACCE was defined as the composite of all-cause mortality, coronary revascularization, non-fatal AMI, and non-fatal stroke. Time-trend subanalyses evaluated the course of LVEF and NT-proBNP serum levels at follow-up every 6 months in patients assigned to the stable, improved, and deteriorated LVEF groups. Here, all available echocardiographic examinations being investigated during routine care either within (re-)hospitalization or in the outpatient clinic at our institution were documented at the intervals of 0–6, 6–12, 12–18, 18–24, and 24–30 months. Assessments of dynamic transitions between LVEF-based HF categories were only presented for the 12 months following the index admission due to the limited number of consecutive echocardiographic LVEF assessments in patients during the follow-up period.
Statistical methods
Quantitative data is presented as mean ± standard error of mean (SEM) or median with IQR, depending on the distribution of the data. They were compared using Student’s t-test for normally distributed data or the Mann–Whitney U test for nonparametric data. Deviations from a Gaussian distribution were tested by the Kolmogorov–Smirnov test. Qualitative data is presented as absolute and relative frequencies and were compared using the chi-square test or Fisher’s exact test, as appropriate. Kaplan–Meier analyses were performed stratified by the three LVEF groups (i.e. stable, improved, and deteriorated). Univariable hazard ratios (HR) were given together with 95% confidence intervals (CI). The prognostic impact of stable, improved, and deteriorated LVEF was thereafter investigated within multivariable Cox regression models. Multivariable Cox regression analyses were performed within the entire study cohort, as well as in pre-specified subgroups stratified by ≥ 75 and < 75 years of age, sex, acute decompensated heart failure (ADHF) in the index admission, and HF etiology as well as medical therapy at discharge. Multivariable Cox regression analyses were visualized using forest plots. LVEF and NT-pro BNP levels were compared among patients stratified by stable, improved, and deteriorated LVEF within 6-months intervals following the index hospitalization using Student’s t-test or the Mann–Whitney U Test.
Results of all statistical tests were considered significant for p ≤ 0.05. SPSS (Version 28, IBM, Armonk, NY) was used for statistics.
Results
Study population
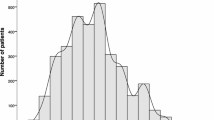
From 2016 to 2022, 2228 patients hospitalized with HFmrEF were included in the HARMER registry. Of those, 44 patients with no evidence on long-term follow-up (corresponding lost-to follow-up rate, 1.97%), 1395 with no evidence on prior LVEF, and 100 patients with prior LVEF ≤ 40% but an improvement < 10% were excluded. Therefore, the final study cohort comprised 689 patients with a median duration between prior and index echocardiography of 308 days with an interquartile range (IQR) of 105–764 days. Within the entire study cohort, 166 (24%), 83 (12%), and 440 (64%) were assigned to the stable, improved, and deteriorated LVEF groups, respectively (Fig. 1; flow chart). Accordingly, longitudinal LVEF changes were very common in the HFmrEF cohort, with only 24% of patients remaining in the LVEF range of HFmrEF over time.

Study flow chart
Table 1 displays baseline characteristics stratified by the three LVEF groups. Age and sex were equally distributed among the three groups (p ≥ 0.203 for all comparisons). Prior coronary artery disease (CAD) was most common among patients with stable LVEF (71.7%), but also highly prevalent in those with improved and deteriorated LVEF (66.3% and 57.5%, respectively). Accordingly, prevalence of prior myocardial infarction was significantly higher in the stable LVEF group when compared to the improved and deteriorated groups (48.2% and 34.9% vs. 33.4%; p ≤ 0.047 for both comparisons), which was reflected in the proportions of patients who had received percutaneous coronary intervention (PCI) in the past (57.2% and 45.8% vs. 43.0%). ADHF in the 12 months prior to the index admission was more common in the groups of stable and improved LVEF than in the group with deteriorated LVEF (30.7% and 39.8% vs. 18.0%; p ≤ 0.001 for both comparisons). Median LVEF determined prior to the index admission was 45%, 33%, and 60% in the groups with stable, improved, and deteriorated LVEF, respectively. In line with the guideline recommendations for the implantation of cardioverter defibrillators, the highest rates of implanted cardioverter defibrillators and cardiac resynchronization therapy with defibrillators were observed in patients with improved LVEF (i.e. prior LVEF ≤ 40% and an improvement ≥ 10% compared to the prior LVEF). There were no differences regarding prior comorbidities (i.e. chronic kidney disease or stroke) or most cardiovascular risk factors such as arterial hypertension, diabetes, or hyperlipidemia between all three groups (p ≥ 0.05 for all comparisons). Comorbidities during the index hospitalization were also equally distributed with only minor differences among the three LVEF groups. Data on medical therapies on admission is provided in the lower section of Table 1.
Additional HF-related and procedural data is outlined in Table 2. Considering HF etiologies, the proportion of ICM was higher in patients with stable LVEF compared to those with improved LVEF and deteriorated LVEF (74.7% and 62.7% vs. 62.7%; p ≤ 0.049 for both comparisons). Additionally, hypertensive cardiomyopathy was more prevalent in the deteriorated compared to the stable and improved LVEF groups (7.7% vs. 1.8% and 2.4%). Echocardiographically measured left ventricular end-diastolic diameter (LVEDD) was higher in patients with stable and improved compared to deteriorated LVEF (50 mm and 52 mm vs. 48 mm; p ≤ 0.05 for both comparisons). Furthermore, diastolic dysfunction was most common in the deteriorated LVEF group (75.5%) and significantly more common than in the improved LVEF group (65.1; p = 0.048). Parameters regarding coronary angiography and baseline laboratory values were equally distributed between the stable, improved, and deteriorated LVEF groups. There were many differences in the medication at discharge, especially between the improved and deteriorated groups. Discharge prescription of angiotensin-converting enzyme inhibitors (59.8% vs. 44.8%; p = 0.013), aldosterone antagonists (30.5% vs. 14.5; p = 0.001), loop diuretics (74.4% vs. 57.1%; p = 0.004), and amiodarone (8.5% vs. 3.3%; p = 0.031) was more common in the improved compared to the deteriorated LVEF group. However, discharge prescription of angiotensin receptor blockers was more common in the deteriorated group (29.8% vs. 17.1%; p = 0.019).
Prognostic impact of prior LVEF in patients with HFmrEF
The development of LVEF over time was not significantly associated with the primary endpoint. Therefore, compared to the previously documented LVEF, patients with stable (HR = 0.880; 95% CI 0.646–1.198; p = 0.416), improved (HR = 1.133; 95% CI 0.776–1.653; p = 0.518), and deteriorated (HR = 1.041; 95% CI 0.796–1.361; p = 0.770) LVEF had similar rates of long-term all-cause mortality (31.3% vs. 37.3% vs. 34.1%; log rank p ≥ 0.376 for all comparisons, respectively) (Fig. 2, left panel). Furthermore, development of LVEF had no significant impact on long-term HF-related rehospitalization (stable LVEF 21.1% vs. improved LVEF 24.1% vs. deteriorated LVEF 20.7%; log rank p ≥ 0.749 for all comparisons) (Fig. 2, right panel). Even at a shorter follow-up duration of 12 months, no significant differences between the stable, improved, and deteriorated LVEF groups were observed regarding all-cause mortality (21.1% vs. 24.1% vs. 23.0%) and HF-related rehospitalization (16.1% vs. 13.4% vs. 16.2%), respectively. Other secondary endpoints (e.g. in-hospital all-cause mortality, cardiac rehospitalization, MACCE at long-term follow-up) were also equally distributed among the three groups (Table 3). Even after excluding patients with a time interval of less than 1 month or more than 12 (Supplemental Fig. 1) or 24 months (Supplemental Fig. 2) between the prior and index LVEF assessment, similar rates of long-term all-cause mortality and long-term HF-related rehospitalization were observed in all three LVEF groups. The analysis of the prognostic endpoints of long-term all-cause mortality (log rank p ≥ 0.354 across groups) and HF-related rehospitalization (log rank p ≥ 0.374 across groups) in patients with stable, improved, and deteriorated LVEF stratified by the etiology of heart failure (i.e. ischemic and non-ischemic cardiomyopathy) also did not demonstrate significant differences between the three LVEF groups (Fig. 3).

Kaplan–Meier analyses comparing patients with stable, improved, and deteriorated LVEF regarding the primary endpoint of long-term all-cause mortality (left panel) and secondary endpoint of long-term heart failure–related rehospitalization (right panel) within the entire study cohort

Kaplan–Meier analyses comparing patients with stable, improved, and deteriorated LVEF regarding the primary endpoint of long-term all-cause mortality (left panels) and secondary endpoint of long-term heart failure–related rehospitalization (right panels) within subgroups of patients with ischemic (upper panels) or non-ischemic cardiomyopathy (lower panels)
Multivariate Cox regression analysis in the entire study cohort and within pre-specified subgroups
After multivariable adjustment, the development of LVEF was still not associated with the risks of all-cause mortality and HF-related rehospitalization at long-term follow-up. However, age (HR = 1.021; 95% CI 1.006–1.037; p = 0.005), chronic kidney disease (CKD; HR = 1.654; 95% CI 1.190–2.298; p = 0.003), RVD (HR = 1.488; 95% CI 1.083–2.044; p = 0.014), ADHF during the index admission (HR = 1.542; 95% CI 1.055–2.255; p = 0.025), and NYHA functional class (HR = 1.228; 95% CI 1.028–1.467; p = 0.023) were identified as predictors of higher mortality, whereas increasing body mass index (BMI) was associated with a lower risk of mortality (HR = 0.967; 95% CI 0.937–0.999; p = 0.044) within the study cohort (Fig. 4, upper panel). Furthermore, CKD (HR = 1.671; 95% CI 1.113–2.509; p = 0.013), atrial fibrillation (HR = 1.655; 95% CI 1.114–2.460; p = 0.013), and NYHA functional class (HR = 1.461; 95% CI 1.182–1.806; p = 0.001) were associated with a higher risk for long-term HF-related rehospitalization in patients with HFmrEF (Fig. 4, lower panel). Using improved LVEF as the reference group, multivariable analyses in pre-specified subgroups defined by age, sex, ADHF, HF etiology, and medical therapy at discharge demonstrated significant differences in the prognostic impact of stable, improved, and deteriorated LVEF. Deteriorated LVEF was associated with significantly lower risk of mortality in females (HR = 0.522; 95% CI 0.279–0.975; p = 0.041) and in those not receiving combined angiotensin-converting enzyme inhibitor (ACEi)/angiotensin receptor blocker (ARB)/angiotensin receptor neprilysin inhibitor (ARNI) + β-blocker therapy (HR = 0.438; 95% CI 0.229–0.840; p = 0.013). In the subgroup of patients suffering from ADHF during the index admission, both stable (HR = 0.468; 95% CI 0.240–0.912; p = 0.026) and deteriorated LVEF (HR = 0.535; 95% CI 0.311–0.920; p = 0.024) were associated with lower long-term all-cause mortality compared to the improved LVEF group (Fig. 5, upper panel). However, the groups of stable, improved, and deteriorated LVEF were not associated with HF-related rehospitalization at long-term follow-up, even in the pre-determined subgroups (p ≥ 0.232 for all comparisons) (Fig. 5, lower panel).

Forest plots demonstrating multivariable Cox regression analyses within the entire study cohort regarding the risk of all-cause mortality (upper panel) and heart failure–related rehospitalization (lower panel) at 30 months

Forest plots demonstrating multivariable Cox regression analyses in pre-determined subgroups regarding the risk of long-term all-cause mortality (upper panel) and heart failure–related rehospitalization (lower panel). The multivariable Cox regression model was adjusted for age, sex, ICM, diabetes, and chronic kidney disease
Distribution of LVEF-based HF categories and dynamic changes of LVEF in the follow-up period
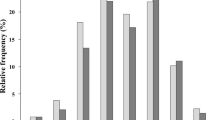
LVEF remained a dynamic parameter in the follow-up period. Recurrent changes in the distribution of LVEF-based HF categories across 24 months of follow-up were observed. At any given time point during follow-up, 20–24%, 32–44%, and 34–45% of patients were categorized as HFrEF, HFmrEF, or HFpEF/normal LVEF without HF (Fig. 6, upper panel). In addition, transitions between HF categories observed in echocardiographic LVEF assessments in the 12 months following the index admission are displayed in the lower panel of Fig. 6. At last, available data on median LVEF and NT-proBNP levels obtained in clinical routine follow-up are displayed in Supplemental Fig. 3. Notably, a recurrent deterioration of LVEF at 24 and 30 months of follow-up was observed in patients initially assigned to the improved LVEF group. The difference in median LVEF reached statistical significance when comparing the improved with the deteriorated (p ≤ 0.047 for the comparison at 24 and 30 months), but not the stable LVEF group (p ≥ 0.080 for the comparison at 24 and 30 months) (Supplemental Fig. 3, left panel). No statistically significant differences regarding NT-proBNP levels (corrected for estimated glomerular filtration rate) during the follow-up period were observed between the groups of stable, improved, and deteriorated LVEF (p ≥ 0.103 for all comparisons) (Supplemental Fig. 3, right panel).

Bar charts displaying the distribution of LVEF-based HF categories (i.e. HFpEF/normal LVEF without HF, HFmrEF, and HFrEF) (upper panel) and a flow diagram demonstrating dynamic changes between HF categories during follow-up (lower panel)
Discussion
The present study investigates the prognostic impact of longitudinal changes of LVEF in a large retrospective cohort of patients hospitalized with HFmrEF. Through the comparison of prior LVEF and index LVEF, patients were stratified into three groups termed stable (i.e. prior LVEF of 41–49%), improved (i.e. prior LVEF ≤ 40% and an improvement ≥ 10% compared to the prior LVEF), and deteriorated LVEF (i.e. prior LVEF ≥ 50%). Longitudinal changes of LVEF were very common with only 24% of patients remaining in the category of HFmrEF at a median duration of 308 days between the prior and index echocardiography. However, prior LVEF was not associated with the primary endpoint of long-term all-cause mortality or with secondary endpoints including in-hospital or 12-month all-cause mortality as well as HF-related rehospitalization at 12 and 30 months. Analyses of LVEF assessments in the follow-up period demonstrated a persistently high dynamic of LVEF.
Since the new category of HF (i.e. HFmrEF) has been established in 2016, efforts have grown to characterize this cohort. Observational studies suggest that the median age and the proportion of women is higher in HFmrEF compared to HFrEF, but lower than in HFpEF [7, 29, 30]. In addition, prevalence of ischemic etiology seems to be similarly prevalent in HFrEF and HFmrEF and therefore more prevalent than in HFpEF [7, 30, 31]. Therefore, it has often been argued that HFmrEF could represent a transitional state between HFrEF and HFpEF, which are both characterized by more distinct pathophysiological properties [32, 33]. Accordingly, a large proportion of patients with HFmrEF transition to either HFrEF or HFpEF and vice versa, which was further confirmed by the main findings of the present study [15, 29, 34]. As displayed in Fig. 6, LVEF was also a highly dynamic parameter within our study cohort, with frequent transitions between LVEF-based HF categories observed in the time following the index admission. Even though LVEF is an established prognostic metric in HF, there is limited data on how prior LVEF impacts the prognosis of patients with HFmrEF. In a study by Savarese et al. [15] investigating the prognostic impact of longitudinal changes of LVEF across the spectrum of HF categories, 21% and 16% of patients previously classified as having HFpEF or HFrEF transitioned to HFmrEF, respectively [15]. In contrast, in the present study, 12% of patients with a prior LVEF ≤ 40% as well as an improvement of LVEF ≥ 10% and 64% with a prior LVEF ≥ 50% transitioned to HFmrEF. Especially the higher proportion of transitions from preserved LVEF could be explained by the fact that this group not only included patients with prior HFpEF but also patients with no established HF diagnosis before the index admission, whereas the study by Savarese et al. only included patients with established HF. This finding could suggest that, beyond patients transitioning from HFpEF to HFmrEF, there might be a large proportion of patients with incident HFmrEF. In general, Savarese et al. observed that an improvement in LVEF was associated with a more favourable prognosis, while deterioration of LVEF predicted adverse outcomes. However, this effect was more pronounced when comparing more extensive transitions between HFrEF and HFpEF rather than transitions to and from HFmrEF and — depending on the used comparator — changes to and from HFmrEF were not significantly associated with outcomes [15]. An association between transitions from HFpEF or HFrEF to HFmrEF and patient outcomes was not observed in the present study. A possible explanation for the absence of adverse prognosis in the deteriorated LVEF group of the present study could be explained by a significantly higher rate of hypertensive cardiomyopathy observed in this group, since previous research has indicated that hypertensive cardiomyopathy tends to have a more favourable prognosis compared to other HF etiologies [35,36,37]. In addition, improved LVEF was not associated with favourable outcomes. This finding was likely connected to the recurrent deterioration of LVEF observed in some patients of this cohort during the follow-up period (Supplementary Fig. 3, left panel). In general, the missing prognostic impact of the assigned LVEF groups might be explained by the dynamic nature of LVEF during the follow-up period. This dynamic could be particularly noteworthy in the cohort of HFmrEF due to its narrow EF interval (41–49%) and the presence of interrater variability in the assessment of LVEF. Considering the findings of previous studies investigating longitudinal changes of LVEF over time and our observations demonstrated in Fig. 6, it seems likely that a relevant proportion of patients will experience recurrent transitions between HF categories in the time following the index admission [29, 38]. As these changes could impact patients’ prognosis, prospective studies with pre-determined time intervals for LVEF assessment performed repeatedly by the same operators are required to further investigate the prognostic impact of longitudinal changes of LVEF, especially in patients with HFmrEF. At last, the equal proportion of patients experiencing ADHF in the index admission across all three LVEF groups should be considered as a noteworthy finding of the present study. Despite the distinct trajectories of LVEF development in the three groups, the event of ADHF occurred — at least in part — irrespective of longitudinal changes of LVEF. As ADHF itself is a prognostic marker in the disease course of HF, the similar rates of ADHF during the index admission and HF-related rehospitalization during the follow-up period could further explain the absence of prognostic differences between patients with stable, improved, and deteriorated LVEF.
Few studies [39, 40] have investigated the prognostic impact of transitions from reduced or preserved LVEF to the specific subgroup of HFmrEF and should therefore be acknowledged and discussed to provide a comprehensive overview of the current evidence. In a retrospective cohort study by Brann et al. [39] including 448 patients with HFmrEF, the deterioration of previous LVEF ≥ 50% compared to the improvement of previous LVEF ≤ 40% was associated with a significantly higher rate of both investigated composite endpoints (all-cause mortality or hospitalization and cardiovascular mortality or HF-related hospitalization) at a median follow-up of 2.24 years. However, analyses of the individual components of these composite endpoints did not demonstrate statistically significant differences (p ≥ 0.06 for all comparisons). Furthermore, the threshold for statistical significance was only met for all-cause mortality (p = 0.05) and all-cause hospitalization (p = 0.04) after multivariable adjustment, which could suggest an influence of other confounding factors. In contrast to our study, the deteriorated group was characterized by a significantly larger proportion of patients with malignancy (20%) compared to the improved (11%) and stable groups (5%) which showed significant impact on patient prognosis in univariate analysis. To address this, a separate analysis excluding patients with a history of malignancy and treatment with chemotherapy was performed, demonstrating that the composite endpoint of all-cause mortality and hospitalization no longer reached statistical significance. Additionally, the median time between the prior and index transthoracic echocardiography was around 1300 days and therefore significantly longer than in the present study (308 days), adding another level of diversity when comparing results [39]. Furthermore, Zhang et al. [40] investigated the prognostic impact of prior LVEF in a total of 1168 patients with HFmrEF hospitalized for ADHF at one institution. Higher risk for the composite of all-cause mortality and all-cause hospitalization was demonstrated when comparing the groups with improved and deteriorated LVEF, which was mainly driven by higher mortality. Besides other differences in baseline characteristics, significantly higher prevalence of malignancy was — once again — found in the deteriorated LVEF group. In contrast to our findings, there were higher rates of CAD within the deteriorated group, which could have impacted patients’ prognosis depending on the extent of previous therapeutic interventions. Unfortunately, no data regarding parameters such as prior PCI were provided to assess the impact of this difference [40]. Prescription of medical therapies (i.e. ACEi/ARB/ARNI, β-blockers, mineralocorticoid receptor antagonists (MRA), and statins) were relatively similar across all three groups when comparing data of the present study with data provided by Brann et al. and Zhang et al., except for generally higher prescription rates of MRA in the study by Zhang et al. However, discrepancies regarding higher prescription rates of ACEi/ARB/ARNI, β-blockers, and MRA in the improved compared to the stable and deteriorated LVEF groups were more pronounced in their cohorts. In general, contemporary studies investigating the prognostic impact of prior LVEF in HFmrEF are characterized by varying study settings, heterogeneous cohort characteristics and differences in the definitions of endpoints. Therefore, the observed prognostic differences may be attributed to the presence or absence of confounding factors associated with LVEF that influence prognosis in patients with HFmrEF, regardless of the development of LVEF.
LVEF has been identified as a prognostic marker in previous studies and has been the cornerstone of defining inclusion criteria in many clinical trials [5,6,7, 10]. However, the classification of HF based predominantly on this parameter has been criticized for its inherent limitations [41, 42]. Firstly, measurement of LVEF through echocardiography is dependent on patients’ current condition (i.e. heart rate, bundle branch blocks, or pre- and afterload) and associated with high interobserver and intraobserver variability which can result in the misclassification of patients, especially considering the narrow LVEF range of HFmrEF [43,44,45]. This can be detrimental for patients because guideline recommendations for initiating cardioprotective pharmacotherapies and device therapies in HF are based on established LVEF thresholds [5, 6]. Secondly, it is debatable how accurately LVEF represents actual myocardial (dys)function, as normal values only indicate an appropriate ratio between stroke volume and left ventricular end-diastolic volume [46]. For example, studies have demonstrated that global longitudinal strain could be a stronger predictor of adverse clinical outcomes than LVEF, especially in cohorts with an LVEF > 35% [47]. Therefore, we believe the consideration of additional measures of myocardial form and function beside LVEF is necessary to provide more comprehensive medical management and improve the assessment of patients’ prognosis [48].
Study limitations
Despite the efforts of statistical adjustment, the study results may be influenced by measured and unmeasured confounding due to the retrospective study design. Furthermore, only patients at our University Medical Centre were included in this study which limits generalizability to other patient cohorts. Specific causes of death beyond those occurring within the index hospitalization were not available for the present study since state resident registration offices are not allowed to disclose any personal information beyond the date of death due to German law. In addition, the use of medical therapies was not standardized, which could have impacted prognosis. Notably, echocardiographic assessments of prior LVEF were not obtained at pre-specified time intervals but were simply included based on availability. To obtain such a large patient cohort, echocardiographic data on prior LVEF was not only ascertained from our institution, but also from records of other hospitals or ambulatory cardiology visits stored in our electronic hospital information system. It is important to acknowledge that this approach might have introduced more heterogeneity and interobserver variability to the data and could have affected the precision of LVEF measurements.
Conclusion
The present study supports the high frequency of transitions between HF categories (i.e. HFrEF, HFmrEF, and HFpEF) observed in previous observational studies. Transitions from prior LVEF values below or above the 41–49% threshold into the HFmrEF category were not associated with adverse outcomes in the follow-up period. These findings might be attributable to the dynamic nature of LVEF and the recurrent deterioration of LVEF in the improved group during the time of follow-up as well as the absence of additional prognostically negative factors in the deteriorated group, which often contributed to worse outcomes in prior studies.
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
References
Roger VL (2021) Epidemiology of heart failure: a contemporary perspective. Circ Res 128(10):1421–1434. https://doi.org/10.1161/circresaha.121.318172
Bragazzi NL, Zhong W, Shu J, Abu Much A, Lotan D, Grupper A et al (2021) Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol 28(15):1682–1690. https://doi.org/10.1093/eurjpc/zwaa147
Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC et al (2013) Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail 6(3):606–619. https://doi.org/10.1161/HHF.0b013e318291329a
James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N et al (2018) Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159):1789–858. https://doi.org/10.1016/s0140-6736(18)32279-7
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M et al (2021) 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 42(36):3599–3726. https://doi.org/10.1093/eurheartj/ehab368
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM et al (2022) 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145(18):e895–e1032. https://doi.org/10.1161/CIR.0000000000001063
Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo-Leiro MG, Harjola VP et al (2017) Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail 19(12):1574–1585. https://doi.org/10.1002/ejhf.813
Koh AS, Tay WT, Teng THK, Vedin O, Benson L, Dahlstrom U et al (2017) A comprehensive population-based characterization of heart failure with mid-range ejection fraction. Eur J Heart Fail 19(12):1624–1634. https://doi.org/10.1002/ejhf.945
Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N et al (2021) Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail 23(3):352–380. https://doi.org/10.1002/ejhf.2115
Angaran P, Dorian P, Ha ACT, Thavendiranathan P, Tsang W, Leong-Poi H et al (2020) Association of left ventricular ejection fraction with mortality and hospitalizations. J Am Soc Echocardiogr 33(7):802–11.e6. https://doi.org/10.1016/j.echo.2019.12.016
Lupón J, Díez-López C, de Antonio M, Domingo M, Zamora E, Moliner P et al (2017) Recovered heart failure with reduced ejection fraction and outcomes: a prospective study. Eur J Heart Fail 19(12):1615–1623. https://doi.org/10.1002/ejhf.824
He Y, Ling Y, Guo W, Li Q, Yu S, Huang H et al (2021) Prevalence and prognosis of HFimpEF developed from patients with heart failure with reduced ejection fraction: systematic review and meta-analysis. Front Cardiovasc Med 8:757596. https://doi.org/10.3389/fcvm.2021.757596
Kalogeropoulos AP, Kim S, Rawal S, Jadonath A, Tangutoori R, Georgiopoulou V (2019) Serial changes in left ventricular ejection fraction and outcomes in outpatients with heart failure and preserved ejection fraction. Am J Cardiol 124(5):729–735. https://doi.org/10.1016/j.amjcard.2019.05.052
Okuhara Y, Asakura M, Orihara Y, Morisawa D, Matsumoto Y, Naito Y et al (2019) Reduction in left ventricular ejection fraction is associated with subsequent cardiac events in outpatients with chronic heart failure. Sci Rep 9(1):17271. https://doi.org/10.1038/s41598-019-53697-y
Savarese G, Vedin O, D’Amario D, Uijl A, Dahlström U, Rosano G et al (2019) Prevalence and prognostic implications of longitudinal ejection fraction change in heart failure. JACC Heart Fail 7(4):306–317. https://doi.org/10.1016/j.jchf.2018.11.019
Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ et al (2003) Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet 362(9386):777–781. https://doi.org/10.1016/s0140-6736(03)14285-7
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B et al (2014) Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 370(15):1383–1392. https://doi.org/10.1056/NEJMoa1313731
Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP et al (2019) Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med 381(17):1609–1620. https://doi.org/10.1056/NEJMoa1908655
Schmitt A, Schupp T, Reinhardt M, Abel N, Lau F, Forner J et al (2023) Prognostic impact of acute decompensated heart failure in patients with heart failure with mildly reduced ejection fraction. Eur Heart J Acute Cardiovasc Care 13(2):225–241. https://doi.org/10.1093/ehjacc/zuad139
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M et al (2021) 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599–3726. https://doi.org/10.1093/eurheartj/ehab368
Popescu BA, Andrade MJ, Badano LP, Fox KF, Flachskampf FA, Lancellotti P et al (2009) European Association of Echocardiography recommendations for training, competence, and quality improvement in echocardiography. Eur J Echocardiogr 10(8):893–905. https://doi.org/10.1093/ejechocard/jep151
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 16(3):233–270. https://doi.org/10.1093/ehjci/jev014
Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P et al (2008) Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 29(2):270–276. https://doi.org/10.1093/eurheartj/ehm342
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M et al (2018) 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J 39(33):3021–3104. https://doi.org/10.1093/eurheartj/ehy339
Lancellotti P, Tribouilloy C, Hagendorff A, Popescu BA, Edvardsen T, Pierard LA et al (2013) Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 14(7):611–644. https://doi.org/10.1093/ehjci/jet105
Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J et al (2021) 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 43(7):561–632. https://doi.org/10.1093/eurheartj/ehab395
Gopinathannair R, Etheridge SP, Marchlinski FE, Spinale FG, Lakkireddy D, Olshansky B (2015) Arrhythmia-induced cardiomyopathies: mechanisms, recognition, and management. J Am Coll Cardiol 66(15):1714–1728
Kaye G, Ng JY, Ahmed S, Valencia D, Harrop D, Ng ACT (2019) The prevalence of pacing-induced cardiomyopathy (PICM) in patients with long term right ventricular pacing - is it a matter of definition? Heart Lung Circ 28(7):1027–1033. https://doi.org/10.1016/j.hlc.2018.05.196
Tsuji K, Sakata Y, Nochioka K, Miura M, Yamauchi T, Onose T et al (2017) Characterization of heart failure patients with mid-range left ventricular ejection fraction—a report from the CHART-2 Study. Eur J Heart Fail 19(10):1258–1269. https://doi.org/10.1002/ejhf.807
Rickenbacher P, Kaufmann BA, Maeder MT, Bernheim A, Goetschalckx K, Pfister O et al (2017) Heart failure with mid-range ejection fraction: a distinct clinical entity? Insights from the Trial of Intensified versus standard Medical therapy in Elderly patients with Congestive Heart Failure (TIME-CHF). Eur J Heart Fail 19(12):1586–1596. https://doi.org/10.1002/ejhf.798
Farmakis D, Simitsis P, Bistola V, Triposkiadis F, Ikonomidis I, Katsanos S et al (2017) Acute heart failure with mid-range left ventricular ejection fraction: clinical profile, in-hospital management, and short-term outcome. Clin Res Cardiol 106(5):359–368. https://doi.org/10.1007/s00392-016-1063-0
Zhou Q, Li P, Zhao H, Xu X, Li S, Zhao J et al (2021) Heart failure with mid-range ejection fraction: a distinctive subtype or a transitional stage? Front Cardiovasc Med 8:678121. https://doi.org/10.3389/fcvm.2021.678121
Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ et al (2009) Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute. Circulation 119(24):3070–3077. https://doi.org/10.1161/circulationaha.108.815944
Tsukamoto K, Suzuki A, Shiga T, Arai K, Hagiwara N (2021) Changes in the left ventricular ejection fraction and outcomes in hospitalized heart failure patients with mid-range ejection fraction: a prospective observational study. Intern Med 60(10):1509–1518. https://doi.org/10.2169/internalmedicine.6388-20
Pecini R, Møller DV, Torp-Pedersen C, Hassager C, Køber L (2011) Heart failure etiology impacts survival of patients with heart failure. Int J Cardiol 149(2):211–215. https://doi.org/10.1016/j.ijcard.2010.01.011
Shore S, Grau-Sepulveda MV, Bhatt DL, Heidenreich PA, Eapen ZJ, Hernandez AF et al (2015) Characteristics, treatments, and outcomes of hospitalized heart failure patients stratified by etiologies of cardiomyopathy. JACC Heart Fail 3(11):906–916. https://doi.org/10.1016/j.jchf.2015.06.012
Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG et al (2017) Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail 19(10):1242–1254. https://doi.org/10.1002/ejhf.890
Yamamoto M, Seo Y, Ishizu T, Nishi I, Hamada-Harimura Y, Machino-Ohtsuka T et al (2019) Different impact of changes in left ventricular ejection fraction between heart failure classifications in patients with acute decompensated heart failure. Circ J 83(3):584–594. https://doi.org/10.1253/circj.CJ-18-0881
Brann A, Janvanishstaporn S, Greenberg B (2020) Association of prior left ventricular ejection fraction with clinical outcomes in patients with heart failure with midrange ejection fraction. JAMA Cardiol 5(9):1027–1035. https://doi.org/10.1001/jamacardio.2020.2081
Zhang X, Sun Y, Zhang Y, Chen F, Zhang S, He H et al (2021) Heart failure with midrange ejection fraction: prior left ventricular ejection fraction and prognosis. Front Cardiovasc Med 8:697221. https://doi.org/10.3389/fcvm.2021.697221
Marwick TH (2018) Ejection fraction pros and cons: JACC state-of-the-art review. J Am Coll Cardiol 72(19):2360–2379. https://doi.org/10.1016/j.jacc.2018.08.2162
Mann DL (2016) Is it time for a new taxonomy for heart failure? J Card Fail 22(9):710–712. https://doi.org/10.1016/j.cardfail.2016.07.432
Lupón J, Bayés-Genís A (2018) Left ventricular ejection fraction in heart failure: a clinician’s perspective about a dynamic and imperfect parameter, though still convenient and a cornerstone for patient classification and management. Eur J Heart Fail 20(3):433–435. https://doi.org/10.1002/ejhf.1116
Wood PW, Choy JB, Nanda NC, Becher H (2014) Left ventricular ejection fraction and volumes: it depends on the imaging method. Echocardiography 31(1):87–100. https://doi.org/10.1111/echo.12331
Barbier P, Mirea O, Cefalù C, Maltagliati A, Savioli G, Guglielmo M (2015) Reliability and feasibility of longitudinal AFI global and segmental strain compared with 2D left ventricular volumes and ejection fraction: intra- and inter-operator, test-retest, and inter-cycle reproducibility. Eur Heart J Cardiovasc Imaging 16(6):642–652. https://doi.org/10.1093/ehjci/jeu274
Kosaraju A, Goyal A, Grigorova Y, Makaryus AN (2022) Left ventricular ejection fraction. StatPearls. StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC, Treasure Island (FL)
Stanton T, Leano R, Marwick TH (2009) Prediction of all-cause mortality from global longitudinal speckle strain: comparison with ejection fraction and wall motion scoring. Circ Cardiovasc Imaging 2(5):356–364. https://doi.org/10.1161/circimaging.109.862334
Triposkiadis F, Butler J, Abboud FM, Armstrong PW, Adamopoulos S, Atherton JJ et al (2019) The continuous heart failure spectrum: moving beyond an ejection fraction classification. Eur Heart J 40(26):2155–2163. https://doi.org/10.1093/eurheartj/ehz158
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: AS, MB, KW, KM, MAb, MAy, IA, TS.
Methodology: AS, MB, KM, MR, NA, FL, MAb, MAy, IA, TS.
Software: MB, JF, TS.
Validation: AS, MB, KW, KM, MAb, MAy, IA, TS.
Formal analysis: AS, MB, KW, TS.
Investigation: AS, MR, NA, FL.
Resources: MB, IA, TS.
Data curation: AS, MR, NA, FL, JF.
Writing — original draft: AS, MB, TS.
Writing — review and editing: AS, MB, IA, TS.
Visualization: AS, MR, NA, FL, JF.
Supervision: MB, IA, TS.
Project administration: MB, IA, TS.
Funding acquisition: No funding was received.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study protocol was reviewed and approved by the medical ethics committee II of the Medical Faculty Mannheim, University of Heidelberg, Germany; ethical approval code, 2022–818. Written informed consent from patients was not required for this study because no additional data were achieved and solely data assembled in the daily clinical routine were used.
Conflict of interest
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
392_2024_2443_MOESM1_ESM.pptx
Supplementary file1 Supplemental figure 1: Kaplan-Meier analyses comparing patients with stable, improved, and deteriorated LVEF regarding long-term all-cause mortality (left panel) and heart failure-related rehospitalization (right panel) within a select study cohort excluding patients with a minimum time interval of less than 1 month or more than 12 months between the prior and index LVEF assessment. (PPTX 92 KB)
392_2024_2443_MOESM2_ESM.pptx
Supplementary file2 Supplemental figure 2: Kaplan-Meier analyses comparing patients with stable, improved, and deteriorated LVEF regarding long-term all-cause mortality (left panel) and heart failure-related rehospitalization (right panel) within a select study cohort excluding patients with a minimum time interval of less than 1 month or more than 24 months between the prior and index LVEF assessment. (PPTX 94 KB)
392_2024_2443_MOESM3_ESM.pptx
Supplementary file3 Supplemental figure 3: Line graphs demonstrating changes of LVEF (left panel) and NT-proBNP levels (right panel) during the follow-up period among patients stratified by prior LVEF as stable, improved, or deteriorated LVEF. The data is presented as the median with the corresponding 25% and 75% percentiles. (PPTX 129 KB)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schmitt, A., Behnes, M., Weidner, K. et al. Prognostic impact of prior LVEF in patients with heart failure with mildly reduced ejection fraction. Clin Res Cardiol (2024). https://doi.org/10.1007/s00392-024-02443-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00392-024-02443-0