
Abstract
Objectives
A series of human field studies demonstrated that acute exposure to simulated nocturnal traffic noise is associated with cardiovascular complications and sleep disturbance, including endothelial dysfunction, increased blood pressure, and impaired sleep quality. A pooled analysis of these results remains to be established and is of tremendous interest to consolidate scientific knowledge.
Methods
We analyzed data from four randomized crossover studies (published between 2013 to 2021 and conducted at the University Medical Center Mainz, Germany). A total of 275 subjects (40.4% women, mean age 43.03 years) were each exposed to one control scenario (regular background noise) and at least to one traffic noise scenario (60 aircraft or train noise events) in their homes during nighttime. After each night, the subjects visited the study center for comprehensive cardiovascular function assessment, including the measurement of endothelial function and hemodynamic and biochemical parameters, as well as sleep-related variables.
Results
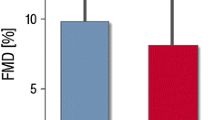
The pooled analysis revealed a significantly impaired endothelial function when comparing the two different noise sequences (0–60 vs. 60–0 simulated noise events, mean difference in flow-mediated dilation −2.00%, 95% CI −2.32; −1.68, p < 0.0001). In concordance, mean arterial pressure was significantly increased after traffic noise exposure (mean difference 2.50 mmHg, 95% CI 0.54; 4.45, p = 0.013). Self-reported sleep quality, the restfulness of sleep, and feeling in the morning were significantly impaired after traffic noise exposure (all p < 0.0001).
Discussion
Acute exposure to simulated nocturnal traffic noise is associated with endothelial dysfunction, increased mean arterial pressure, and sleep disturbance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Emerging evidence highlights the importance of environmental noise exposure as a substantial public health threat [6, 11]. In support of this, the European Environment Agency concludes that at least about 20% of the EU population in average, in many cities this percentage can reach up to 50% of the urban population, are exposed to long-term noise levels considered potentially harmful to health. Specifically, about 95 million people are exposed to harmful road traffic noise levels. Furthermore, it is estimated that at least 18 million people are highly annoyed and 5 million are highly sleep disturbed by long-term transportation noise in the EU, causing about 11,000 premature deaths and 40,000 new cases of ischemic heart disease per year [1].
During the last few years, strong evidence from epidemiological studies has emerged to demonstrate that traffic noise exposure is a risk factor for cardiovascular disease. For instance, in nationwide studies from Switzerland and Denmark, it was shown that transportation noise exposure is associated with all and cause-specific cardiovascular disease mortality [8, 13, 21] as well as significant cardiovascular outcomes including ischemic heart disease and its’ acute manifestations myocardial infarction, angina pectoris, as well as heart failure, atrial fibrillation, and stroke [18,19,20]. However, at the same time, it should be noted that evidence from human studies that provide a mechanistic basis for the adverse cardiovascular effects of noise is scarce and scientific knowledge is mainly derived from a series of human field studies [9, 14,15,16]. In this context, it is important to identify central pathomechanisms underlying the noise-disease-relationship to establish a central framework that displays how noise initiates and contributes to cardiovascular disease. This may help to intensify efforts to officially acknowledge noise not only as an additional noticed enhancer of cardiovascular disease, but as an established and manifest cardiovascular risk factor in a political and medical setting.
In our field studies, we consistently demonstrated that acute exposure to simulated nocturnal aircraft [14,15,16] or train noise [9] was associated with impaired endothelial function and decreased sleep quality. Less consistent or partly insignificant results were observed in the case of stress hormone release, blood pressure, and other hemodynamic and biochemical parameters. Significant heterogeneity in these studies concerning design and sample included the (a) source of noise—aircraft [14,15,16] or train noise [9], (b) subjects—younger healthy adults [9, 15] or older subjects with established cardiovascular disease or increased cardiovascular risk [14, 16], (c) number of subjects and sex ratio—N = 75 (61% women) [15], N = 60 (27% women) [14], N = 70 (50% women) [9], or N = 70 (20% women) [16], and (d) the number of noise events and corresponding mean sound pressure levels—30 (43 dB(A)) vs. 60 (46 dB(A)) aircraft noise events [15], 60 aircraft noise events (46 dB(A) [14], 30 (52 dB(A)) vs. 60 (54 dB(A)) train noise events [9], or 60 vs. 120 aircraft noise events (both with a mean value of around 45 dB(A)) [16].
To provide overall and robust estimates acknowledging the heterogeneity between studies, we sought to determine the pooled acute effect of simulated nocturnal traffic noise exposure on cardiovascular and sleep-related outcomes based on the data from our human field studies.
Methods
Study design
The conception and the design of the included human field studies study have been described in detail previously [9, 14,15,16]. Briefly, all human field studies were set up as randomized, double-blinded, crossover studies conducted between 2011 and 2020 at the Department of Cardiology of the University Medical Center in Mainz, Germany. Potential participants were found through social media and the distribution of flyers and posters in Mainz, Germany. All participants underwent nights in which they were exposed to a control scenario and at least one noise scenario according to the study protocol. In the morning, after each study night, participants went to the study center for comprehensive and standardized examination follow-up. All participants were exposed to the different scenarios in the participants’ bedrooms in a randomized manner. Study visits were prescheduled with at least three non-study nights between two study nights and on the same weekday, if possible. In female participants, care was taken to synchronize hormonal status with study nights. The control scenario contained no “playback-generated” noise events, but the participants were exposed to normal background noise in their home environments. The noise scenarios consisted of playback of aircraft or train noise events with a varying number of events. The events comprised the noise of a starting or landing aircraft or passing trains. The noise scenarios started with playback of a 30 s lasting tone signaling the beginning of the study night and enabling checking of the equipment. This was followed by 45 min of silence to enable subjects to fall asleep, after which the first noise event was played. Noise events were recorded under controlled circumstances in the bedroom of a resident living near an airport or railway track in Germany. Noise patterns were played back as MP3 files via customary portable audio systems, which were positioned 1 m above the floor at the end of the bed. The sound pressure level (SPL) was continuously measured via class-2 sound level measuring station, which was placed near the head of the participant. Exclusion criteria consisted of the following: exposure to higher residential levels of nocturnal traffic noise as determined by noise maps (LAeq,22–6 h > 45 dB(A) road traffic, railway, or aircraft noise), being an anti-traffic noise activist, sleep disorder (indicated by a score > 10 on the Pittsburgh Sleep Quality Index (PSQI) [23] or psychiatric disorder assessed by the Mini-International Neuropsychiatric Interview (M.I.N.I.) [17], age-adjusted hearing loss of 30 dB(A) or more, obstructive sleep apnea in the screening test, current shift work and/or regular drug intake except oral contraceptives. Other hormonal therapies led to exclusion. Included participants were advised to refrain from intake of caffeine-containing beverages, alcohol, and supplemental vitamins the day before, during, and in the morning after each study night. Participants were financially compensated when completing the study protocol. All procedures conducted in the field studies were in accordance with the declaration of Helsinki and approved by the Statutory Physician Board of the State Rhineland-Palatinate ethics committee. Written informed consent was obtained before participation in the study. Table 1 gives an overview of the important characteristics of the included studies.
Examinations
After each study night, participants were invited to the study center in a fasted state, with all measurements conducted and samples collected before 10 a.m. During the study nights, a range of hemodynamic parameters, including heart rate, blood pressure, and pulse transit time, was continuously measured by wearing portable polygraphic screening. The participants put on devices immediately before starting the study night after being carefully advised and trained at the study center. The primary outcome of all studies was endothelial function measured by flow-mediated dilatation (FMD) of the brachial artery using high‐resolution ultrasound based on standardized methods as described [10, 12]. Briefly, the brachial artery diameter was measured before and after an increase in shear stress that is induced by reactive hyperemia. Therefore, the sphygmomanometer cuff was placed proximal to the brachial artery and was then inflated up to 200 mmHg for a period of 5 min. After cuff release, the reactive, flow‐dependent dilation of the brachial artery was recorded. This amount of dilation largely reflects endothelial function. Imaging was performed in a dark, quiet room at a temperature of 21–23 °C. Patients rested in the supine position for at least 10 min before the first scan and remained supine until the final recording was acquired. Image acquisition and analysis were performed under blinded conditions. Measurement of FMD was performed in all studies by a high trained technician with at least 12 months of experience in measuring FMD before getting involved in the endothelial function studies. Afterwards, our in-house clinical chemistry laboratory drew and immediately analyzed blood samples. The sleep quality was evaluated by a visual analog scale (VAS) with the following question: “Overall, how well did you sleep last night?” (VAS ranging from 0 cm meaning very good sleep quality to 10 cm meaning very bad sleep quality). The restfulness of sleep was evaluated with the question: “How restful was your sleep?” (answer format ranging from 0 very good to 5 very bad). Feeling in the morning after the study nights were assessed with the question: “How do you feel now?” (answer format ranging from 0 very good to 15 very bad). Standard laboratory methods were used to determine stress hormone levels and biochemical parameters.
Statistical analysis
In order to test for a noise exposure effect, within-subject difference in outcome between the two study periods (nights) was calculated and compared between the two different noise sequences (0–60 vs. 60–0 simulated noise events) with an independent samples test. In case of a normal distributed outcome variable, a two-sample t-test otherwise a Wilcoxon rank sum test was used. Data were presented as mean/median differences and 95% confidence intervals (CI). To check for potential carry-over effects, the sum of the values measured in the two periods is calculated for each subject and compared across the two sequence groups by means of another test for independent samples. Effect modification by sex and age was analyzed via linear regression with delta as the dependent variable. Moreover, we performed sensitivity analysis by excluding the train noise study [9], as this was the only study that examined train instead of aircraft noise. All tests were two-sided, and p values < 0.05 were considered significant. The statistical data analyses were performed using the software R Version 4.2.3 (http://www.r-project.org/).
Results
Pooled analysis of the primary outcome—FMD
In total, 275 subjects (111 women, 40.4%) were enrolled with a mean age of 43 ± 20 years.
The pooled analysis of the primary outcome, FMD (Table 2 and Fig. 1A), revealed a significant mean difference between the control scenario and noise scenario with 60 events, indicating worsened endothelial function upon noise exposure. Results remained stable after excluding the train noise study [9]. There was no evidence for a carry-over effect. Effect modification analysis indicated no effect of sex and age on the mean difference in FMD (Supplemental Table S1).

Forest plots of the results presented in the Tables 2, 3, 4, 5 displaying mean or median differences comparing the two different noise sequences (0–60 vs. 60–0 simulated noise events) (x-axis) for A flow-mediated dilation (FMD %), B mean arterial pressure (MAP mmHg), C feeling in the morning after study night (answer format ranging from 0 very good to 15 very bad), D restfulness (answer format ranging from 0 very good to 5 very bad), and E sleep quality (VAS ranging from 0 cm meaning very good sleep quality to 10 cm meaning very bad sleep quality) in our human field studies and pooled results (y-axis)
Pooled analysis of the secondary outcomes
The pooled analysis of secondary outcomes, including mean arterial pressure, feeling in the morning after study night, restfulness, and sleep quality (Tables 3, 4, 5, 6 and Fig. 1B–E) indicated significant mean/median differences, compatible with a higher mean arterial pressure as well as disturbed feeling in the morning, sleep quality, and restfulness due to noise exposure. All estimates remained stable when excluding the train noise study [9]. There was evidence for a carry-over effect in the pooled analysis for restfulness and sleep quality. Significant effect modification by age was revealed in the case of mean differences in the feeling in the morning after study night and sleep quality, indicating a positive association between higher age and an increased disturbed feeling in the morning and sleep quality (Supplemental Tables S2 to S5). No significant mean/median differences were observed in the case of heart rate, the laboratory results regarding adrenaline, cortisol, C-reactive protein, interleukin 6, and neutrophils, as well as pulse transit time (Supplemental Tables S6 to S19).
Discussion
The results of our present pooled analysis demonstrate that acute exposure to simulated nocturnal traffic noise is associated with impaired endothelial function, higher mean arterial pressure, and disturbed sleep quality. We further outlined that feeling in the morning and restfulness of sleep were significantly disturbed after noise exposure during night. These results remained stable when excluding the only study in which train instead of aircraft noise was present. While mostly no effect modification by age and sex was observed in primary and secondary outcome variables, differences in sleep quality and feeling in the morning after study night appeared to be modified by age. We found also evidence for a carry-over effect in the pooled analysis for restfulness and sleep quality by applying appropriate statistical methods as recommended for crossover designs in clinical trials [22].
Babisch has proposed a noise reaction model in which the so-called “indirect pathway” is the crucial route by which noise exposure adversely affects the cardiovascular system [2]. Herein, annoyance and interference with daily routines and, importantly, sleep by chronic low-level noise exposure lead to higher psycho-physiological arousal associated with increased stress hormone levels, blood pressure, and heart rate. This, in turn, generates the development and acceleration of cardiovascular risk factors such as arterial hypertension, arrhythmia, dyslipidemia, increased blood viscosity and blood glucose, and activation of blood clotting factors, finally leading to manifest cardiovascular disease over time. In line, we have recently shown that noise annoyance due to different sources is associated with a higher risk of prevalent and incident atrial fibrillation in the Gutenberg Health Study (GHS), including 15,010 participants [3,4,5]. A further study based on data from the GHS also revealed that noise annoyance due to different sources was associated with increased midregional pro-atrial natriuretic peptide levels, a marker that is associated with endothelial function, which in turn was predictive of incident atrial fibrillation and cardiovascular disease as well as all-cause mortality [7].
Our results are in line with recently published epidemiological studies investigating the relationship between long-term exposure to traffic noise and cardiovascular events, as well as mechanistic animal studies (for review, see [11]). For instance, a nationwide study from Denmark demonstrated that road traffic noise at the most exposed façade was associated with a higher risk of incident ischemic heart disease, myocardial infarction, angina pectoris, and heart failure with hazard ratios (HRs) of 1.052 (95% CI 1.044–1.059), 1.041 (95% CI 1.032–1.051), 1.095 (95% CI 1.071–1.119), and 1.039 (95% CI 1.033–1.045), respectively. Likewise, Vienneau et al. revealed, based on a nationwide cohort from Switzerland, HRs of 1.029 (95% CI 1.024–1.034) and 1.013 (95% CI 1.010–1.017) for the association between road traffic and railway noise and cardiovascular disease mortality, respectively, whereas this association was weaker for aircraft noise (HR 1.003, 95% CI 0.996–1.010) [21]. It is important to note that although these risks increase seem small, the public health impacts are devastating as large parts of the population are routinely exposed to traffic noise and other noise sources [1]. Our results and epidemiological study results suggest that acute reactions in response to traffic noise, such as endothelial dysfunction, increased arterial pressure, and disturbed sleep, will accumulate over time to increase the risk of manifest cardiovascular disease and mortality.
The results of our pooled analysis largely support the noise reaction model, showing important key mechanisms of disease initiation, such as noise-induced endothelial dysfunction, increased arterial pressure, and disturbed sleep. Nevertheless, we did not find evidence of noise-induced changes in heart rate, stress hormones, inflammation, and pulse transit time. Strengths of the present study include the novelty of conducting a pooled analysis of human field studies in the context of acute, controlled exposure to simulated traffic noise, which has several advantages compared to epidemiological designs, where exposure misclassification is more likely and might attenuate/influence or even bias the impact and effect strength of noise on health. A further novel finding includes the positive pooled association between acute nocturnal traffic noise exposure and mean arterial pressure. However, it should be noted that the corresponding confidence intervals are quite wide and that the study from Herzog et al. [9] displays a negative effect estimate, although not significant. Interestingly, this is also the only study in which evidence of a carry-over effect was noticed, which may have interfered with the results. We applied appropriate statistical methods as recommended for crossover designs in clinical trials [22], a substantial advantage compared to the primary studies included in the pooled analysis. Lastly, testing effect modification by sex and age was not done before in this setting. However, the present study also has some limitations that merit consideration. There was evidence for a carry-over effect in the pooled analysis for the secondary outcomes restfulness and sleep quality, which may have interfered with the results. However, care was taken to minimize carry-over effects using counterbalancing (participants were randomly given one of six different sequences of noise and control nights according to the randomization plan) and washout periods (at least three non-study nights between two study nights) where applicable. As stress hormone levels are known to show significant variations over the day, the measurement of associated biomarkers via blood samples hours after awakening may not have been optimal and may explain why stress hormones were not affected by noise in the present analysis. Samples should be collected immediately after awakening by e.g., collecting morning saliva, in future studies. The approach of collecting blood samples directly after awakening may also increase the accuracy of the measurement of other outcomes of interest such as inflammatory markers, that were found not to be affected by noise exposure in the present analysis. However, it may be also the case that an acute scenario of noise exposure is not sufficient to induce a measurable inflammatory response. Measurement of heart rate via standard wearable devices may not be accurate and sensitive enough to detect noise-induced heart rate variations, as it heavily relies on averaging over time periods, as well as it may be susceptible to various disruptive factors during the study night. In addition, measurement of endothelial function in different vascular beds (micro- and macrovascular) would allow a more complete picture of noise-induced vascular damage. Sleep-related variables does not meet the gold standard as it was measured via VAS rather than polysomnography or a wearable device, which could have delivered more objective data on sleep quality. Furthermore, overall sample size is still relatively small, and we cannot rule out the healthy volunteer bias due to the recruitment method. Also, our results only suggest acute noise exposure and not chronic, long-term noise exposure, wherein mechanisms such as adaptation and habituation may come into play. As the present analysis analyzed two distinct samples—young, healthy individuals and older adults with pre-existing cardiovascular conditions, generalizability of the findings to general population is limited, although we did not detect substantial effect modification by age.
In conclusion, our results demonstrate that acute nocturnal traffic noise exposure leads to endothelial dysfunction, higher mean arterial pressure, and disturbed sleep. Our results further highlight key mechanisms regarding the noise-disease-relationship centered on vascular endothelial dysfunction, increased arterial pressure, and impaired sleep quality. Noise is ubiquitous and a major public health challenge, that can only be addressed by appropriate system-level measures.
Data availability
The dataset analyzed for the current study is available from the corresponding author on reasonable request. Applicants will be required to obtain all necessary permissions relevant to data protection regulations before access to data is granted.
Change history
26 September 2023
A Correction to this paper has been published: https://doi.org/10.1007/s00392-023-02309-x
References
European Environment Agency (2023) Noise. https://www.eea.europa.eu/en/topics/in-depth/noise. Accessed 8 May 2023
Babisch W (2002) The noise/stress concept, risk assessment and research needs. Noise Health 4:1–11
Hahad O, Beutel M, Gori T et al (2018) Annoyance to different noise sources is associated with atrial fibrillation in the Gutenberg Health Study. Int J Cardiol 264:79–84
Hahad O, Beutel M, Michal M et al (2022) Noise annoyance in the German general population: prevalence and determinants in the Gutenberg Health Study. Herz 47:265–279
Hahad O, Beutel ME, Gilan DA et al (2022) Noise annoyance and risk of prevalent and incident atrial fibrillation—a sex-specific analysis. Front Public Health 10:1061328
Hahad O, Kroller-Schon S, Daiber A et al (2019) The cardiovascular effects of noise. Dtsch Arztebl Int 116:245–250
Hahad O, Wild PS, Prochaska JH et al (2021) Midregional pro atrial natriuretic peptide: a novel important biomarker for noise annoyance-induced cardiovascular morbidity and mortality? Clin Res Cardiol 110:29–39
Heritier H, Vienneau D, Foraster M et al (2019) A systematic analysis of mutual effects of transportation noise and air pollution exposure on myocardial infarction mortality: a nationwide cohort study in Switzerland. Eur Heart J 40:598–603
Herzog J, Schmidt FP, Hahad O et al (2019) Acute exposure to nocturnal train noise induces endothelial dysfunction and pro-thromboinflammatory changes of the plasma proteome in healthy subjects. Basic Res Cardiol 114:46
Munzel T, Sinning C, Post F et al (2008) Pathophysiology, diagnosis and prognostic implications of endothelial dysfunction. Ann Med 40:180–196
Munzel T, Sorensen M, Daiber A (2021) Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol 18:619–636
Ostad MA, Eggeling S, Tschentscher P et al (2009) Flow-mediated dilation in patients with coronary artery disease is enhanced by high dose atorvastatin compared to combined low dose atorvastatin and ezetimibe: results of the CEZAR study. Atherosclerosis 205:227–232
Saucy A, Schaffer B, Tangermann L et al (2021) Does night-time aircraft noise trigger mortality? A case-crossover study on 24 886 cardiovascular deaths. Eur Heart J 42:835–843
Schmidt F, Kolle K, Kreuder K et al (2015) Nighttime aircraft noise impairs endothelial function and increases blood pressure in patients with or at high risk for coronary artery disease. Clin Res Cardiol 104:23–30
Schmidt FP, Basner M, Kroger G et al (2013) Effect of nighttime aircraft noise exposure on endothelial function and stress hormone release in healthy adults. Eur Heart J 34:3508–3514a
Schmidt FP, Herzog J, Schnorbus B et al (2021) The impact of aircraft noise on vascular and cardiac function in relation to noise event number: a randomized trial. Cardiovasc Res 117:1382–1390
Sheehan DV, Lecrubier Y, Sheehan KH et al (1998) The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 59(Suppl 20):22–33 (quiz 34-57)
Sorensen M, Poulsen AH, Hvidtfeldt UA et al (2021) Transportation noise and risk of stroke: a nationwide prospective cohort study covering Denmark. Int J Epidemiol 50:1147–1156
Thacher JD, Poulsen AH, Hvidtfeldt UA et al (2022) Long-term exposure to transportation noise and risk for atrial fibrillation: a Danish nationwide cohort study. Environ Res 207:112167
Thacher JD, Poulsen AH, Raaschou-Nielsen O et al (2022) Exposure to transportation noise and risk for cardiovascular disease in a nationwide cohort study from Denmark. Environ Res 211:113106
Vienneau D, Saucy A, Schaffer B et al (2022) Transportation noise exposure and cardiovascular mortality: 15-years of follow-up in a nationwide prospective cohort in Switzerland. Environ Int 158:106974
Wellek S, Blettner M (2012) On the proper use of the crossover design in clinical trials: part 18 of a series on evaluation of scientific publications. Dtsch Arztebl Int 109:276–281
Zisberg A, Gur-Yaish N, Shochat T (2010) Contribution of routine to sleep quality in community elderly. Sleep 33:509–514
Funding
Open Access funding enabled and organized by Projekt DEAL. The present work was supported by a vascular biology research grant from the Foundation Heart of Mainz and by the German Heart Foundation/ German Heart Research Foundation. Philipp S. Wild and Thomas Münzel are PI’s of the DZHK (German Center for Cardiovascular Research), Partner Site Rhine-Main, Mainz, Germany.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests in connection with this manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hahad, O., Schmidt, F.P., Hübner, J. et al. Acute exposure to simulated nocturnal traffic noise and cardiovascular complications and sleep disturbance—results from a pooled analysis of human field studies. Clin Res Cardiol 112, 1690–1698 (2023). https://doi.org/10.1007/s00392-023-02297-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-023-02297-y