
Abstract
Aims
Coagulopathy and venous thromboembolism are common findings in coronavirus disease 2019 (COVID-19) and are associated with poor outcome. Timely initiation of anticoagulation after hospital admission was shown to be beneficial. In this study we aim to examine the association of pre-existing oral anticoagulation (OAC) with outcome among a cohort of SARS-CoV-2 infected patients.
Methods and results
We analysed the data from the large multi-national Lean European Open Survey on SARS-CoV-2 infected patients (LEOSS) from March to August 2020. Patients with SARS-CoV-2 infection were eligible for inclusion. We retrospectively analysed the association of pre-existing OAC with all-cause mortality. Secondary outcome measures included COVID-19-related mortality, recovery and composite endpoints combining death and/or thrombotic event and death and/or bleeding event. We restricted bleeding events to intracerebral bleeding in this analysis to ensure clinical relevance and to limit reporting errors. A total of 1 433 SARS-CoV-2 infected patients were analysed, while 334 patients (23.3%) had an existing premedication with OAC and 1 099 patients (79.7%) had no OAC. After risk adjustment for comorbidities, pre-existing OAC showed a protective influence on the endpoint death (OR 0.62, P = 0.013) as well as the secondary endpoints COVID-19-related death (OR 0.64, P = 0.023) and non-recovery (OR 0.66, P = 0.014). The combined endpoint death or thrombotic event tended to be less frequent in patients on OAC (OR 0.71, P = 0.056).
Conclusions
Pre-existing OAC is protective in COVID-19, irrespective of anticoagulation regime during hospital stay and independent of the stage and course of disease.
Graphic abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The novel coronavirus disease 2019 (COVID-19) is currently spreading rapidly, causing significant morbidity and mortality worldwide. An infection with the underlying severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) predominantly causes respiratory symptoms of varying degrees, ranging from mild dyspnoea to acute respiratory distress syndrome [1,2,3]. In addition, coagulopathy is a common and potentially outcome-limiting complication in SARS-CoV-2-infected patients, especially in severe cases [4, 5]. It has been argued that COVID-19 coagulopathy may differ from other causes of coagulopathy leading to venous thromboembolism (VTE), including important contribution of systemic inflammatory activation and endotheliitis, which may not be adequately targetable by conventional anticoagulation [6,7,8]. Consistent with that hypothesis, VTE has been observed in 30–60% of severe COVID-19 cases [9, 10], sometimes even despite therapeutic or prophylactic anticoagulation [10, 11]. Emerging evidence indicates that anticoagulation is nevertheless beneficial for patients with COVID-19, especially in severe cases [12,13,14]. The current consensus statements recommend a repeated risk assessment for VTE and bleeding, to enable timely diagnosis and adequate treatment of coagulation abnormalities in COVID-19 [15].
All these data and recommendations focus on anticoagulation during hospitalization; however, the association of pre-existing oral anticoagulation (OAC) with outcome parameters in COVID-19 is still unclear. Analysing relevant outcome parameters of patients pre-treated with OAC may provide essential information, because mainly older patients suffering from comorbidities such as chronic cardiovascular disease are at risk for fatal outcomes, a patient group also frequently pre-treated with OAC. Using the Lean European Open Survey on SARS-CoV-2 Infected Patients (LEOSS) registry [16], an extensive database on the clinical course of SARS-CoV-2 infected patients, we performed a retrospective risk-adjusted analysis to evaluate the association between pre-existing OAC and outcome in COVID-19.
Patients and methods
Study population
We here report data from the Lean European Open Survey on SARS-CoV-2 Infected Patients (LEOSS). LEOSS is a multi-centre, non-interventional registry study for the documentation of SARS-CoV-2 infected patients mandated by the Emerging Infections Task Force (EITaF) of the European Society for Clinical Microbiology and Infectious Diseases (ESCMID) and supported by the German Center for Infection Research (DZIF) and the German Infectious Disease Society (DGI).
Since LEOSS was initiated in March 2020, more than 120 sites predominantly located in Germany, but also in Austria, Belgium, Bosnia, Canada, Ireland, Italy, Latvia, Spain, Switzerland, Turkey, United Kingdom and the USA have retrospectively reported data on hospitalized and outpatient SARS-CoV-2 infected patients at all different stages of disease severity (from asymptomatic to life threatening). LEOSS is registered at the German Clinical Trials Register (DRSK, S00021145) and was approved by the applicable local ethics committees of all participating centers.
The primary outcome was all-cause mortality. Secondary outcome measures were COVID-19-related mortality, recovery (defined as significant improvement of clinical status as defined in the design of the LEOSS registry, Fig. 1) and the composite endpoints death and/or thrombotic event and death and/or bleeding event. Bleeding event was characterized as intracerebral bleeding in this analysis. We restricted bleeding events to intracerebral bleeding in this analysis to ensure clinical relevance and to limit reporting errors. Other bleeding events were not systematically recorded in the LEOSS registry. The composite endpoints were chosen to inform about clinically relevant events and to account for expected low numbers of thrombotic or bleeding events in the examined cohorts. OAC was defined as premedication with any Vitamin-K antagonist or Non-Vitamin-K antagonist (rivaroxaban, apixaban, edoxaban, dabigatran etexilate). Indication for OAC premedication was not assessed systematically, but atrial fibrillation with increased risk for systemic embolization was likely a main reason for patients to take OAC.

Definition of the different phases (uncomplicated, complicated and critical) of COVID-19 disease used for this analysis
Data collection
The data were recorded at each site in an electronic case report form (eCRF) operated using the cohort platform ClinicalSurveys.net and software developed by Questback (Oslo, Norway). The data entry was conducted in an anonymized manner. Moreover, the LEOSS study team performed further data anonymization and categorization of data to prevent the possibility to draw conclusions to a single hospital.
Data analysis
Difference between categorical and continuous variables were analysed using Fisher's exact test and Students’ t tests, respectively. Since our analysis was solely retrospective and patients were not randomized to the two treatment options (anticoagulation vs. no anticoagulation), multivariable logistic regression analyses were applied to verify the impact of anticoagulation. As potential confounders, a total of 10 baseline patient characteristics (all covariates listed in Table 1) were used. In detail, we considered age, gender, BMI and smoking status as well as the phase of disease at diagnosis and a number of pre-existing cardiovascular diseases, e.g. atrial fibrillation or coronary artery disease. Missing values for age (n = 6) were imputed using median imputation (median age = 70 years). For BMI and smoking status, missing values were more frequent and used as separate variables. For other pre-existing diseases, there were no codes to indicate that data were missing; thus if the patient’s electronic health record did not include information on a clinical characteristic, it was assumed that that characteristic was not present. No adjustment for multiple testing was carried out. Thus, p values may not be interpreted as confirmatory but are descriptive in nature and inferences drawn from the 95% confidence intervals may not be reproducible. All analyses were carried out using Stata 16.1 (StataCorp, College Station, TX, USA).
Results
Patients
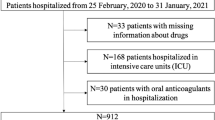
The final anonymized dataset included 3 165 patients infected with SARS-CoV-2 at different phases of disease (uncomplicated, complicated, critical, recovery; Fig. 1). We had to exclude 1 643 patients because of missing information about pre-existing oral anticoagulation or atrial fibrillation or because of retrospective COVID-19 diagnosis post mortem. We included 1 433 patients in our analysis (Fig. 2). A total of 334 patients (23.3%) had an existing premedication with OAC, 1 099 patients (79.7%) had no OAC. Patients with pre-existing OAC were significantly older (77.0 years vs. 69.6 years, P < 0.001), tended to be more likely female (56.3% male with OAC vs. 61.4% male without OAC, P = 0.097) and had more comorbidities. They suffered significantly more frequently from solid tumours (17.1% vs. 12.5%, P = 0.036), coronary artery disease (36.8% vs. 20.0%, P < 0.001), prior myocardial infarction (16.8% vs. 8.6%, P < 0.001), atrial fibrillation (66.5% vs. 12.9%, P < 0.001), peripheral vascular disease (14.1% vs. 6.1%, P < 0.001) and cerebrovascular disease (21.6% vs. 12.5%, P < 0.001). Arterial hypertension was significantly more frequent in patients without OAC (87.6% vs. 82.9%, P = 0.035). The severity of disease at diagnosis was comparable in both groups, indicating similar grades of illness (complicated phase 34.1% in patients with OAC vs. 32.9% in patients without OAC, P = 0.691; critical phase 7.2% in patients with OAC vs. 8.8% in patients without OAC, P = 0.371; Table 1).

Schematic representation of the allocation to the cohort with or without pre-existing oral anticoagulation. Of the 3165 patients initially included in this analysis, we had to exclude 1643 patients due to missing information on oral anticoagulation or atrial fibrillation as a relevant comorbidity. Furthermore, all patients with retrospective COVID-19 diagnosis post mortem were excluded. Finally, 334 patients with pre-existing OAC and 1099 patients without pre-existing oral anticoagulation were included in the analysis. The flow diagram is based on the STROBE criteria for reporting of observational studies [38, 39]
There were relatively large frequencies of unknown data on BMI (35.3% in the group with OAC and 36.7% in the group without OAC) and smoking status (53.6% in the group with OAC and 49.2% in the group without OAC).
Unadjusted outcomes
Unadjusted outcomes did not differ significantly between patients with or without OAC. The rate of all-cause death and COVID-19 related death was slightly higher in patients with OAC without statistical significance (any death: 26.1% vs. 23.7%, P = 0.382; COVID-19 related death: 22.8% vs. 20.7%, P = 0.444). A similar proportion of patients recovered from COVID-19 in both groups (67.1% with OAC vs. 68.9% without OAC, P = 0.545). Thrombotic events occurred only in a few cases in both groups, with 4.2% in patients with OAC and 3.7% in patients without OAC, respectively (P = 0.745). Intracerebral bleedings occurred in 1.2% of patient without OAC and in 0.9% of patients with OAC in similar proportions (P = 1.0). Death or thrombotic event as combined endpoint occurred numerically slightly more often without statistical significance in the group with OAC (28.7% vs. 26.2%, P = 0.360) as well as the combined endpoint death or intracerebral bleeding (26.1% vs. 24.4%, P = 0.563; Table 2).
Risk adjusted outcomes
After risk adjustment for comorbidities, a pre-existing OAC was associated with a significant better outcome regarding the endpoint all-cause death (OR 0.62, P = 0.013) as well on the secondary endpoint COVID-19 related death (OR 0.64, P = 0.023), non-recovery (OR 0.66, P = 0.014) and the combined endpoint death or intracerebral bleeding (OR 0.62, P = 0.01). Patients with pre-existing OAC tended to have a better outcome at the combined endpoint death or thrombotic event (OR 0.71, P = 0.056; Table 3, Fig. 3).

Risk-adjusted outcomes in patients pre-treated with oral anticoagulation and in a cohort without oral anticoagulation pre-treatment. The results of multivariate logistic regression analyses with 23 predefined baseline patient characteristics included as potential confounders (all covariates listed in Table 3)
Analysing the different comorbidities and its risk-adjusted influences on the different endpoints, the complicated or critical stage of disease had a significant influence on all endpoints for a worse outcome. Patients with atrial fibrillation had a significant higher risk for mortality (OR 1.54, P = 0.015), whereas patients with coronary artery disease (OR 1.16, P = 0.394) or prior myocardial infarction did not (OR 1.03, P = 0.9). Also patients with peripheral vascular disease (OR 0.77, P = 0.301), cerebrovascular disease (OR 0.99, P = 0.941) or hypertension (OR 0.87, P = 0.513) did not have an increased risk of mortality. If patients had diabetes mellitus with organ damage, risk for mortality was significantly increased (OR 1.98, P < 0.001), whereas patients with diabetes mellitus without organ damage did not (OR 1.24, P = 0.231). Age and sex (being male has a higher mortality, OR 1.8, P < 0.001; Table 3) had a significant worsening influence on all endpoints. In our analyses we did not see a significant influence of the smoking status or the BMI of the patients on all endpoints. For further information on the influence of the different covariates see Table 3.
Discussion
In this retrospective analysis of the LEOSS registry, an anonymized multi-center registry for the documentation of SARS-CoV-2 infected patients, we studied outcome with regard of pre-existing oral anticoagulation (OAC) irrespective of anticoagulation during hospital stay. In this real-world cohort, pre-existing OAC was associated with less mortality and increased recovery rate.
The hypothesis that pre-existing OAC might have an effect on the outcome of COVID-19 was based on the recent findings on thrombotic events and anticoagulation during SARS-CoV-2 infection [17,18,19]. Thromboembolic complications have emerged as a common and often limiting complication in COVID-19. Since first case series from Wuhan reported an association between pulmonary embolism and COVID-19 [20], various studies described that patients suffering from COVID-19 present a high rate of venous and arterial thromboembolic events, partly even despite anticoagulation at prophylactic or therapeutic doses [10, 21, 22]. It has been suggested that hyperinflammation and hypoxemia lead to endothelial dysfunction and endotheliitis and as a consequence to enhanced risk for thrombus formation [23,24,25,26,27]. The increased incidence of VTEs in patients with COVID-19 despite anticoagulation and the occurrence of major bleeding in up to 5.6% of severe cases has stimulated a debate about the ideal anticoagulation scheme [28]. Furthermore, a recent trial showed an increase in oral anticoagulant plasma levels in patients with SARS-CoV-2 infection treated with antiviral agents [29]. However, recent studies indicated that the benefits of anticoagulation during hospital-stay outweighed the risk of bleeding: Tang et al. reported that patients with severe COVID-19 receiving anticoagulation with unfractionated or (in most cases) low-molecular weight heparin appeared to have a lower mortality than patients without heparin therapy [13]. Nadkarni et al. described that anticoagulation during hospital stay was associated with lower mortality and intubation in COVID-19 and therapeutic anticoagulation tended to be more efficient than prophylactic doses [14]. Yet, most available data on the effects of anticoagulation in COVID-19 are based on the anticoagulation during hospital stay.
Few recent studies showed inconclusive and oppositional results of mortality in patients with SARS-CoV-2 infection on pre-existing oral anticoagulation. One study from Spain showed worse outcome in patients on oral anticoagulation with a surprisingly high mortality rate of 68.2% in this cohort[30]. In contrast two studies from Italy showed improved outcomes of patients on pre-existing oral anticoagulation [17, 31]. Other studies from Italy and Sweden did not show any protective or worsening effect of oral anticoagulation treatment [32, 33].
Our colleagues could show elevated markers of thrombo-inflammatory activation in patients with cardiovascular diseases and their prediction for a worse outcome in the population of the LEOSS registry [34], reinforcing the benefit of early or even pre-existing anticoagulation in these patients in line with our findings in the same population.
We aimed to evaluate the effects of pre-existing OAC on prognosis and outcome of COVID-19 of all stages of disease irrespective of anticoagulation regime during inpatient treatment and irrespective of the stage and course of SARS-CoV-2 infection. Patients pre-treated with OAC are more likely to suffer from cardiovascular comorbidities that make them susceptible for a more severe course of COVID-19 [35]. The findings of our analysis are in line with this hypothesis, showing that patients with OAC were older and had higher rates of atrial fibrillation and other cardiovascular comorbidities. Despite this, mortality rates did not differ between both cohorts in the unadjusted outcome analysis. After risk adjustment, a protective effect of a pre-existing OAC became evident: pre-existing OAC was associated with significantly reduced all-cause and COVID-19-related mortality and improved the recovery rate. Atrial fibrillation itself shows in our covariate adjustment a negative influence on all outcomes. As shown in Table 1, a substantial part of the patients hospitalized with OAC was not diagnosed with atrial fibrillation. At the same time, a substantial part of the patients that was diagnosed with atrial fibrillation was not treated with OAC at hospital admission. In a real-world cohort like ours, this seems realistic as patients with atrial fibrillation might have discontinued medication and patients undergoing OAC treatment might have had other underlying diseases than atrial fibrillation (e.g. thrombosis, mechanical heart valves). As a result, we believe it is of special interest to identify the independent contribution of each predictor: “What is the impact of OAC treatment independent of the patients sex, age, atrial fibrillation and stage of disease?” and “What is the impact of atrial fibrillation independent of OAC treatment, sex, age and stage of disease?”. To answer both questions in one regression model, we believe our methodology is most appropriate compared to other statistical methods [36]. Notably our results were independent of in-hospital anticoagulation regime and irrespective of the clinical stage and course of COVID-19 disease. Taken together, we show with the data from a large multi-national cohort study that a pre-existing oral anticoagulation has a protective effect on the outcome of COVID-19.
Limitations
Apart from the limitations commonly associated with retrospective studies, the LEOSS registry has some specific limitations. Despite its multinational approach, most patients were documented in Germany and a generalization of our results could be biased. Furthermore, the data on the extent of underlying comorbidities or regarding substance, dose or duration of treatment with OAC were not incorporated in the LEOSS database, as both, comorbidities and medication intake, were collected as binary categories. Numerous patients had to be excluded due to missing data on anticoagulation.
Furthermore the anticoagulation regime during hospitalization was not recorded systemically. The lack of knowledge how and if patients were anticoagulated during the hospital stay significantly limits the interpretation of the data, e.g. whether anticoagulation was reduced in prior anticoagulated patients or whether previously non-anticoagulated patients received "full" anticoagulation as a prevention measure. Anonymization and categorization of data made it impossible to consider parameters such as length of hospital stay or length of mechanical ventilation as outcome parameters. Furthermore, major bleeding events such as gastrointestinal bleedings have not been recorded systematically in the LEOSS registry, only intracerebral bleedings were considered systematically in the database. Furthermore the chosen endpoint "intracranial bleeding" occurred only 3 times the anticoagulated group, a number way too small to draw valuable conclusions.
Conclusion
In this observational study evaluating real-world data on the pre-existing OAC on outcome in COVID-19, we investigated mortality, recovery, thrombotic events and intracerebral bleeding using data from the Lean European Open Survey on SARS-CoV-2 Infected Patients (LEOSS). After risk adjustment, a substantial decrease in all-cause and COVID-19-related mortality and an increased recovery rate in patients with pre-existing OAC compared to patients without pre-existing OAC was observed. The combined outcome measure “thrombotic event and/or death” indicated beneficial effects of pre-existing OAC. We did not evaluate anticoagulation regimes during potential hospital stays. While there may be patients benefitting from full-dose anticoagulation, in general prophylactic or moderate dose might be sufficient. Current studies are ongoing [37].
Our results were independent of the clinical stage and course of COVID-19. Our findings need validation in other COVID-19 cohorts or larger registries that can confirm this hypothesis and should not inform directly on the management of patients with COVID-19. However, they support the observations made by many groups that anticoagulation may be beneficial for most patients with COVID-19.
Availability of data and material
Data is available from the authors or the LEOSS study group.
Code availability
Not applicable.
References
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for disease control and prevention. JAMA 323:1239–1242
Wang D, Hu B, Hu C et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323:1061–1069
Guan W, Ni Z, Hu Y et al (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382:1708–1720
Pavoni V, Gianesello L, Pazzi M, Stera C, Meconi T, Frigieri FC (2020) Evaluation of coagulation function by rotation thromboelastometry in critically ill patients with severe COVID-19 pneumonia. J Thromb Thrombolysis. https://doi.org/10.1007/s11239-020-02130-7
Tang N, Li D, Wang X, Sun Z (2020) Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost 18:844–847
Engelmann B, Massberg S (2013) Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol 13:34–45
Delabranche X, Helms J, Meziani F (2017) Immunohaemostasis: a new view on haemostasis during sepsis. Ann Intensive Care 7:117
Jackson SP, Darbousset R, Schoenwaelder SM (2019) Thromboinflammation: challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 133:906–918
Wichmann D, Sperhake J-P, Lütgehetmann M et al (2020) Autopsy findings and venous thromboembolism in patients with COVID-19: a prospective cohort study. Ann Intern Med. https://doi.org/10.7326/M20-2003
Llitjos J, Leclerc M, Chochois C, Monsallier J, Ramakers M, Auvray M, Merouani K (2020) High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J Thromb Haemost 18(7):1743–1746
Maatman TK, Jalali F, Feizpour C et al (2020) Routine venous thromboembolism prophylaxis may be inadequate in the hypercoagulable state of severe coronavirus disease 2019. Crit Care Med. https://doi.org/10.1097/CCM.0000000000004466
Paranjpe I, Fuster V, Lala A et al (2020) Association of treatment dose anticoagulation with in-hospital survival among hospitalized patients with COVID-19. J Am Coll Cardiol 76:122–124
Tang N, Bai H, Chen X, Gong J, Li D, Sun Z (2020) Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost 18:1094–1099
Nadkarni GN, Lala A, Bagiella E et al (2020) Anticoagulation, mortality, bleeding and pathology among patients hospitalized with COVID-19: a single health system study. J Am Coll Cardiol. https://doi.org/10.1016/j.jacc.2020.08.041
Zhai Z, Li C, Chen Y, Gerotziafas G, Zhang Z, Wan J, Liu P, Elalamy I, Wang C, Prevention Treatment of VTE Associated with COVID-19 Infection Consensus Statement Group (2020) Prevention and treatment of venous thromboembolism associated with coronavirus disease 2019 infection: a consensus statement before guidelines. Thromb Haemost 120:937–948
Jakob C, Borgmann S, Duygun F et al (2020) First results of the Lean European Open Survey on SARS-CoV-2 infected patients (LEOSS). Infection. https://doi.org/10.1007/s15010-020-01499-0
Rossi R, Coppi F, Talarico M, Boriani G (2020) Protective role of chronic treatment with direct oral anticoagulants in elderly patients affected by interstitial pneumonia in COVID-19 era. Eur J Intern Med 77:158–160
Harenberg J, Bauersachs R, Ageno W (2020) Does chronic treatment with oral anticoagulants ameliorate the clinical course of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in coronavirus disease 2019 (COVID-19)? Semin Thromb Hemost 47(04):338–340
Inama G, Dodi C, Provini M, Bossoni E, Inama L, Balzarini L, Mancini C, Ramponi S, Marvisi M (2020) Coronavirus disease 2019 infection in patients with recent cardiac surgery: does chronic anticoagulant therapy have a protective effect? J Cardiovasc Med (Hagerstown) 21:765–771
Ullah W, Saeed R, Sarwar U, Patel R, Fischman DL (2020) COVID-19 complicated by acute pulmonary embolism and right-sided heart failure. JACC Case Rep 2:1379–1382
Chi G, Lee JJ, Jamil A, Gunnam V, Najafi H, Memar Montazerin S, Shojaei F, Marszalek J (2020) Venous thromboembolism among hospitalized patients with COVID-19 undergoing thromboprophylaxis: a systematic review and meta-analysis. J Clin Med. https://doi.org/10.3390/jcm9082489
Lodigiani C, Iapichino G, Carenzo L et al (2020) Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 191:9–14
Henry BM, Vikse J, Benoit S, Favaloro EJ, Lippi G (2020) Hyperinflammation and derangement of renin-angiotensin-aldosterone system in COVID-19: a novel hypothesis for clinically suspected hypercoagulopathy and microvascular immunothrombosis. Clin Chim Acta 507:167–173
Panigada M, Bottino N, Tagliabue P, Grasselli G, Novembrino C, Chantarangkul V, Pesenti A, Peyvandi F, Tripodi A (2020) Hypercoagulability of COVID-19 patients in Intensive Care Unit. A report of thromboelastography findings and other parameters of hemostasis. J Thromb Haemost. https://doi.org/10.1111/jth.14850
Poor HD, Ventetuolo CE, Tolbert T, Chun G, Serrao G, Zeidman A, Dangayach NS, Olin J, Kohli-Seth R, Powell CA (2020) COVID-19 critical illness pathophysiology driven by diffuse pulmonary thrombi and pulmonary endothelial dysfunction responsive to thrombolysis. Clin Transl Med 10:e44
Wichmann D, Sperhake J-P, Lütgehetmann M et al (2020) Autopsy findings and venous thromboembolism in patients with COVID-19: a prospective cohort study. Ann Intern Med 173:268–277
Ackermann M, Verleden SE, Kuehnel M et al (2020) Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med 383:120–128
Al-Samkari H, Karp Leaf RS, Dzik WH et al (2020) COVID-19 and coagulation: bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 136:489–500
Testa S, Prandoni P, Paoletti O et al (2020) Direct oral anticoagulant plasma levels’ striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral agents: the Cremona experience. J Thromb Haemost 18:1320–1323
Rivera-Caravaca JM, Núñez-Gil IJ, Vivas D et al (2020) Clinical profile and prognosis in patients on oral anticoagulation before admission for COVID-19. Eur J Clin Investig 51:e13436
Denas G, Gennaro N, Ferroni E, Fedeli U, Lorenzoni G, Gregori D, Iliceto S, Pengo V (2020) Reduction in all-cause mortality in COVID-19 patients on chronic oral anticoagulation: a population-based propensity score matched study. Int J Cardiol. https://doi.org/10.1016/j.ijcard.2020.12.024
Flam B, Wintzell V, Ludvigsson JF, Mårtensson J, Pasternak B (2020) Direct oral anticoagulant use and risk of severe COVID-19. J Intern Med. https://doi.org/10.1111/joim.13205
Schiavone M, Gasperetti A, Mancone M et al (2021) Oral anticoagulation and clinical outcomes in COVID-19: an Italian multicenter experience. Int J Cardiol 323:276–280
Cremer S, Jakob C, Berkowitsch A et al (2020) Elevated markers of thrombo-inflammatory activation predict outcome in patients with cardiovascular comorbidities and COVID-19 disease: insights from the LEOSS registry. Clin Res Cardiol. https://doi.org/10.1007/s00392-020-01769-9
Lu Q-B, Jiang W-L, Zhang X et al (2020) Comorbidities for fatal outcome among the COVID-19 patients: a hospital-based case–control study. J Infect 82(1):159–198
Elze MC, Gregson J, Baber U, Williamson E, Sartori S, Mehran R, Nichols M, Stone GW, Pocock SJ (2017) Comparison of propensity score methods and covariate adjustment: evaluation in 4 cardiovascular studies. J Am Coll Cardiol 69:345–357
Talasaz AH, Sadeghipour P, Kakavand H et al (2021) Recent randomized trials of antithrombotic therapy for patients with COVID-19. J Am Coll Cardiol 77:1903–1921
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2014) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg 12:1495–1499
Cuschieri S (2019) The STROBE guidelines. Saudi J Anaesth 13:S31–S34
Acknowledgements
We express our deep gratitude to all study teams supporting the LEOSS study. The LEOSS study groups that contributed at least 5 per mille to the analyses of this study: Hospital Ingolstadt PD Dr. Dr. Stefan Borgmann; Technical University of Munich PD Dr. Christoph Spinner; University Hospital Freiburg Prof. Siegbert Rieg; Hospital Leverkusen Dr. Lukas Eberwein; University Hospital Jena Dr. Maria Madeleine Rüthrich; Hospital Ernst von Bergmann Lukas Tometten; University Hospital Essen Dr. Sebastian Dolff; Johannes Wesling Hospital Minden Dr. Kai Wille; Hospital Passau Dr. Julia Lanznaster; Klinikum Dortmund Martin Hower; University Hospital Frankfurt Prof. Dr. Maria Vehreschild; University Hospital Regensburg Dr. Frank Hanses; University Hospital Würzburg Dr. Nora Isberner; University Hospital Ulm PD Dr. Beate Grüner; Hospital Bremen-Mitte Dr. Christiane Piepel; Tropical Clinic Paul-Lechler Hospital Tübingen Dr. Claudia Raichle; Hospital Maria Hilf GmbH Moenchengladbach Prof. Dr. Juergen vom Dahl; University Hospital Schleswig-Holstein-Kiel Dr. Anette Friedrichs; Municipal Hospital Karlsruhe Dr. Christian Degenhardt; University Hospital Heidelberg Prof. Dr. Uta Merle; University Hospital Cologne Prof. Dr. Norma Jung; Kreuznacher Diakonia Dr. med. Wolfgang Rimili; University Hospital Erlangen Dr. Richard Strauß; St. Josef Hospital Bochum Prof. Dr. Kerstin Hellwig; Protestant City Hospital Saarbrücken Dr. Mark Neufang; Petrus Hospital Wuppertal Dr. med Sven Stieglitz; University Hospital Duesseldorf Dr. Björn Jensen; University Hospital Dresden Dr. Dr. Katja de With; Bundeswehr Central Hospital Dr. Dominic Rauschning; Marien Hospital Herne Dr. Timm Westhoff; Robert-Bosch-Krankenhaus Dr. Katja Rothfuss; Malteser Krankenhaus St. Franziskus-Hospital Dr. Milena Milovanovic; München Klinik Dr. Wolfgang Guggemos; Sophien- und Hufeland Klinikum Weimar Dr. Jessica Rüddel; Oberlausitz-Kliniken Dr. Maximilian Worm; University Hospital Saarland Prof. Dr. Dr. Robert Bals; University Hospital Hamburg-Eppendorf Dr. Sabine Jordan; Hospital of the Augustinian Cologne Dr. Stefani Röseler, Nephrologisches Zentrum Villingen-Schwenningen Prof. Dr. Bernd Hohenstein; Justus-Liebig-University Giessen Dr. med. Janina Trauth; University Hospital Bonn Prof. Dr. Jacob Nattermann; University Hospital Tübingen Prof. Siri Göpel; Agaplesion Diaconia Hospial Rotenburg PD Dr. David Heigener; German Heart Center Munich Markus Freißmuth; Hospital Osbrück Dr. Annika Ritter; Charité Berlin Dr. Martina Bertolo; Thorax-Hospital Heidelberg Univ. -Prof. Dr. med. Felix Herth. The LEOSS study infrastructure group: Jörg Janne Vehreschild (Goethe University Frankfurt), Lisa Pilgram (Goethe University Frankfurt), Melanie Stecher (University Hospital of Cologne), Maximilian Schons (University Hospital of Cologne), Carolin E. M. Jakob (University Hospital of Cologne), Susana Nunes de Miranda (University Hospital of Cologne), Annika Claßen (University Hospital of Cologne), Sandra Fuhrmann (University Hospital of Cologne), Bernd Franke (University Hospital of Cologne), Nick Schulze (University Hospital of Cologne), Fabian Praßer (Charité, Universitätsmedizin Berlin) und Martin Lablans (University Medical Center Mannheim).
Funding
Open Access funding enabled and organized by Projekt DEAL. LEOSS is funded by the German Center for Infection Research (DZIF) and the Willy Robert Pitzer Foundation. M Rieder is funded by the IMM-PACT-Programme for Clinician Scientists, Department of Medicine II, Medical Center-University of Freiburg and Faculty of Medicine, University of Freiburg, funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—413517907. Nadine Gauchel and Daniel Duershcmied are members of SFB1425, funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—Project #422681845.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The Authors declare that there is no conflict of interest. All authors agreed to publish this manuscript.
Ethics approval
LEOSS is registered at the German Clinical Trials Register (DRSK, S00021145) and was approved by the applicable local ethics committees of all participating centres.
Consent to participate
Informed consent was waived in accordance with the ethical committees due to retrospective and anonymous data collection of standard of care treatment.
Consent for publication
Informed consent was waived in accordance with the ethical committees due to retrospective and anonymous data collection of standard of care treatment.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rieder, M., Gauchel, N., Kaier, K. et al. Pre-medication with oral anticoagulants is associated with better outcomes in a large multinational COVID-19 cohort with cardiovascular comorbidities. Clin Res Cardiol 111, 322–332 (2022). https://doi.org/10.1007/s00392-021-01939-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-021-01939-3