
Abstract
Background
Heyde syndrome (HS) is known as the association of severe aortic stenosis (AS) and recurrent gastrointestinal bleeding (GIB) from angiodysplasia. Data on the prevalence of HS and results after TAVI remain scarce.
Methods
2548 consecutive patients who underwent TAVI for the treatment of AS from 2008 to 2017 were evaluated for a history of GIB and the presence of HS. The diagnosis of HS was defined as a clinical triad of severe AS, a history of recurrent GIB, and an endoscopic diagnosis of angiodysplasia. These patients (Heyde) were followed to investigate clinical outcomes, bleeding complications and the recurrence of GIB and were compared to patients with GIB unrelated to HS (Non-Heyde).
Results
A history of GIB prior to TAVI was detected in 190 patients (7.5%). Among them, 47 patients were diagnosed with HS (1.8%). Heyde patients required blood transfusions more frequently compared to Non-Heyde patients during index hospitalization (50.0% vs. 31.9%, p = 0.03). Recurrent GIB was detected in 39.8% of Heyde compared to 21.2% of Non-Heyde patients one year after TAVI (p = 0.03). In patients diagnosed with HS and recurrent GIB after TAVI, the rate of residual ≥ mild paravalvular leakage (PVL) was higher compared to those without recurrent bleeding (73.3% vs. 38.1%, p = 0.05).
Conclusion
A relevant number of patients undergoing TAVI were diagnosed with HS. Recurrent GIB was detected in a significant number of Heyde patients during follow-up. A possible association with residual PVL requires further investigation to improve treatment options and outcomes in patients with HS.
Graphic abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The association of aortic valve stenosis (AS) and gastrointestinal bleeding (GIB) from angiodysplasia is known as Heyde syndrome (HS) [1]. The prevalence of GIB related to HS has been described as 1 to 3 percent of patients with aortic stenosis [2,3,4,5].
The prevalence, pathogenesis and treatment options of HS remain controversial. The development of angiodysplasia has been associated with mucosal ischemia leading to vessel dilatation and formation of coral-formed vessels throughout the GI tract with highest prevalence in the right colon and cecum [6]. The pathogenesis of HS involves hemostaseologic alterations leading to an acquired von Willebrand syndrome (aVWS). High shear stress caused by severe aortic stenosis leads to a decreased content of the high-molecular-weight multimers (HMWM) and decreased collagen-binding activity of VWF [7,8,9]. The combination of both factors, vascular malformations, i.e. angiodysplasia, and hemostaseologic alterations due to AS, result in a higher bleeding risk in these patients [10].
Surgical or transcatheter implantation of an aortic valve prosthesis is commonly performed for the treatment of severe AS. A resolution of GIB from angiodysplasia in patients with HS by surgical aortic valve replacement (SAVR) in the majority of patients has been previously reported [11, 12]. Since transcatheter aortic valve implantation (TAVI) has become the preferred treatment in the majority of patients with severe AS, it remains to be determined whether TAVI would likewise resolve recurrent GIB in patients with HS. First reports suggested a resolution of bleeding but these assumptions were drawn from small analyses including only few Heyde patients or case reports and evidence overall remains scarce [3, 4, 8, 13,14,15,16].
Thus, we aimed to evaluate the prevalence of HS in a real-life cohort of patients undergoing TAVI, to identify variables associated with bleeding events in HS and to analyze the incidence of recurrent GIB during post-TAVI follow-up in these patients.
Methods
Study population
We conducted a retrospective single-center analysis of 2548 consecutive patients who underwent TAVI for the treatment of severe AS at a single academic heart center between 2008 and 2017. The diagnosis of severe AS was made according to the current ESC/EACTS guidelines for the treatment of valvular heart disease [17]. Among all patients treated with TAVI at our institution, those with a history of GIB were identified. A history of GIB was defined as an episode of GIB recorded in a patient’s chart, earlier diagnoses or endoscopy reports. The diagnosis of HS was based on the clinical triad of severe AS, a history of recurrent GIB, and an endoscopic (esophagogastroduodenoscopy or colonoscopy) diagnosis of angiodysplasia. GIB of unknown origin or related to other causes (e.g. malignant process, ulcer) was defined as bleeding unrelated to angiodysplasia. We collected baseline and follow-up data of both groups (a) Heyde patients (n = 47) and (b) those with GIB unrelated to angiodysplasia (Non-Heyde patients, n = 143).
Patient follow-up
Baseline and follow-up variables were recorded from patients’ charts and entered into a dedicated database. Mean follow-up was 11.2 months. Clinical outcomes were evaluated with emphasis on bleeding complications and recurrence of GIB. Clinical endpoints and periprocedural complications were defined in accordance with the updated Valve Academic Research Consortium-2 (VARC-2) definitions [18]. Endpoint adjudication was performed independently from this study by a team of experienced cardiologists who were blinded to the study groups.
Statistical analyses
Continuous variables were shown as median (25th and 75th percentile) or as mean ± standard deviation. Binary variables or absolute and relative frequencies were shown as number (n) and percentage. Differences to total n were due to missing values, the calculation of proportions did not include missing values in the denominator. For two group comparison Mann–Whitney test was used for continuous variables, and χ2 test for binary ones. Survival curves for GIB after TAVI during 1-year follow-up were produced using the Kaplan–Meier method. Survival curve differences were tested using the log-rank test. For overall tests p < 0.05 was considered statistically significant. All statistical analyses were performed using R version 4.0.3 (R Foundation for Statistical Computing).
Results
Baseline characteristics
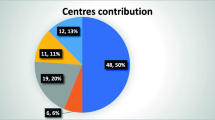
The median age of all patients undergoing TAVI (n = 2548) was 81.2 years (76.4, 85.0) and 49.3% were male. Among these patients, a total of 190 patients (7.5%) had a history of GIB. Overall 47 patients (1.8%) fulfilled the clinical characteristics for HS (history of recurrent GIB and an endoscopic diagnosis of angiodysplasia of the GI tract), while 143 patients (5.6%) had a history of GIB unrelated to angiodysplasia (Non-Heyde patients, see Fig. 1). Both groups were similar with regard to age, gender, comorbidities, and risk profiles (see Table 1). Antithrombotic regimens in Heyde vs. Non-Heyde patients did not differ significantly at baseline (single antiplatelet: 44.4% vs. 50.0%, p = 0.61; dual antiplatelet: 8.9% vs. 6.5%, p = 0.74; oral anticoagulation: 28.9% vs. 39.9%, p = 0.22). Hemoglobin levels were lower in patients with HS compared to those with GIB unrelated to angiodysplasia (all results as follows Heyde vs. Non-Heyde, Hb 10.0 (8.7,11.1) g/dl vs. 10.8 (9.4,12.2) g/dl; p = 0.02, see Table 1). The number of patients with hemoglobin concentrations < 8 g/dl was numerically higher in Heyde vs. Non-Heyde, albeit not statistically significant.

Distribution of patients with GIB among all patients with severe AS treated with TAVI
Periprocedural data
TAVI was performed with immediate technical success in all cases (n = 190), most frequently by endovascular access (68.1% vs. 76.2%, p = 0.34). Effective orifice areas (EOA) increased from 0.8 ± 0.2 cm2 to 2.1 ± 0.5 cm2 overall and similar in both groups. VARC-2 defined complications including major access site complications (12.8% vs. 9.1%, p = 0.57), any stroke or TIA (4.8% vs. 4.2%, p = 1.00) and permanent pacemaker implantations (16.7% vs. 20.3%, p = 0.66) were similar in both groups. We observed a trend to more acute renal failure (AKIN ≥ 2) in Heyde vs. Non-Heyde patients (9.5% vs. 2.5%, p = 0.08). Periprocedural major or life-threatening bleeding events were numerically higher in Heyde vs. Non-Heyde patients, albeit not statistically significant (21.3% vs. 13.4%, p = 0.24). Among these patients GIB occurred more often in patients with HS during 30-day follow-up (19.4 vs. 7.0%, p = 0.05, see Table 2). The incidence of GIB in the overall TAVI cohort was 1.5%. 50.0% of Heyde patients required transfusion of 2.3 \(\pm\) 4.6 packed red blood cells (PRBC) during the index hospitalization compared to 1.5 \(\pm\) 4.0 PRBC in 31.9% of patients with a history of GIB unrelated to angiodysplasia (Non-Heyde) (p = 0.03, see Table 2).
Recurrence of GI-bleeding during follow-up
Freedom from GIB after TAVI during 1-year follow-up was significantly lower in Heyde patients (60.2%) compared to patients with GIB unrelated to angiodysplasia (Non-Heyde, 78.8%; p = 0.03, see Fig. 2). During the follow-up period 15 (44%) patients with Heyde syndrome compared to 26 (26%) of Non-Heyde patients had recurrent GIB (p = 0.02, see table S1, Supplementary Material). A total of 9 (60%) Heyde patients had a diagnosis of upper or lower GIB, 6 of whom had an endoscopic diagnosis of angiodysplasia. In the remaining 9 Heyde patients there was either no evidence of angiodysplasia or endoscopy was not completed. In Non-Heyde patients 11 (42%) had a diagnosis of upper of lower GIB during follow-up and 15 (58%) had GIB of unknown origin. The source of bleeding was multifactorial (e.g. ulcers, gastritis) but angiodysplasia was found in two cases, one of whom had moderate PVL at the time of endoscopy.

Freedom from GIB in patients with Heyde syndrome compared to those with GIB unrelated to angiodysplasia (Non-Heyde) during 1 year of follow-up (post TAVI). Significantly higher GI-bleeding complications in patients with Heyde syndrome during 1 year of follow-up were revealed (p = 0.03)
Antithrombotic and anticoagulation regimens after TAVI were similar among Heyde vs. Non-Heyde patients (see Table 2). The duration of intensified antithrombotic therapy (i.e. combination of (oral) anticoagulation (OAC) and single or dual antiplatelet therapy (SAPT/DAPT)) did not differ between both groups. Antithrombotic strategies did not differ in HS patients with and without recurrent bleeding during follow-up. A trend towards higher rates of intensified antithrombotic therapy (OAC + SAPT or DAPT) was observed in Non-Heyde patients with recurrent GIB (see figure S2, Supplementary Material).
In patients diagnosed with HS and recurrent GIB after TAVI the rate of residual mild or moderate paravalvular regurgitation was higher compared to those with an unremarkable course while statistically this difference reached borderline significance (73.3% vs. 38.1%, p = 0.05, see Fig. 3).

Distribution of paravalvular leakage (PVL) in patients with and without Heyde syndrome with regard to recurrence of gastrointestinal bleeding during follow-up
Discussion
In the present study we assessed the prevalence of HS in a real-life cohort of patients with severe AS undergoing TAVI and evaluated bleeding complications and GIB during follow-up.
Three key findings can be drawn from this retrospective single-center analysis: First, HS was prevalent in a relevant number of TAVI patients (1.8%) which was in line with previously published data from smaller observational analyses [2,3,4,5]. To date, the present study is the largest cohort of TAVI patients evaluating the prevalence of HS. Second, during a follow-up period of 12 months after TAVI the recurrence of GIB in Heyde patients was significant (39.8%) and higher compared to patients with GIB unrelated to angiodysplasia. Third, patients with HS and recurrent GIB during follow-up had more residual paravalvular regurgitation compared to Heyde patients with an unremarkable course.
Previous studies reported a resolution of GIB from angiodysplasia after SAVR in the majority of Heyde patients, although systematic evidence was lacking [11, 12, 19,20,21,22]. Hemostaseologic findings with a correction of the HMWM content after SAVR suggested a “surgical cure” of HS [9, 23]. Within the past decade, TAVI has become the preferred treatment option for AS in most patients [24, 25]. A normalization of hemostasis parameters including vWF was reported after TAVI, especially in those with pre-existing aVWS [4, 8]. Few small studies and case series reported no recurrence of GIB in patients with HS after TAVI, albeit limited due to short-term follow-up and small patient numbers [3, 4, 8, 13,14,15]. In contrast to these earlier publications, we observed that a substantial number of Heyde patients suffered from recurrent GIB after TAVI already during 1-year follow-up despite adequate treatment of AS.
An association of paravalvular leakage (PVL), late bleeding complications and impaired survival was demonstrated before. An analysis from the PARTNER (Placement of Aortic Transcatheter Trial) trial found late bleeding events, mainly GIB, in a relevant number of patients (5.9%) after TAVI, which were associated with a fourfold increase in late mortality (26). Interestingly, PVL was the strongest predictor of these bleeding events between 30 days and 1 year after TAVI [26]. Moreover, mild to moderate PVL was discovered in patients without recovery of abnormal multimer levels, emphasizing the effect of persistent shear stress as cause of HMWM deficiency [8] Consistent with these findings, we discovered a significantly higher rate of ≥ mild PVL in Heyde patients with recurrent GIB after TAVI compared to those with an unremarkable course. As angiodysplasias persist after replacement of the aortic valve [2] this suggests that the association between PVL and recurrent GIB is caused by hemostaseologic rather than vascular alterations associated by PVL. Future studies should evaluate if individualized antithrombotic strategies, e.g. guided by post-TAVI HMWM levels or vWF activity can prevent GIB events in patients with HS (with PVL) after TAVI.
Furthermore, we found more periprocedural transfusion of packed red blood cells in Heyde patients, possibly related to lower baseline hemoglobin values and numerically higher rates of bleeding complications. The adverse impact of red blood cell transfusion after TAVI was previously described [27,28,29], emphasizing the need for close monitoring of this vulnerable patient cohort.
Individualized antithrombotic treatment will be essential to minimize bleeding risk in these patients at risk. Recent evidence demonstrated superiority for restrictive antithrombotic strategies after TAVI [30, 31]. Additional analyses suggested that patients after TAVI may have hemostatic disorders apart from aVWS that may cause bleeding complications [32]. Whether bleeding complications can be reduced with tailored antithrombotic strategies in these vulnerable HS patients, needs further investigation.
Limitations of the current study relate to the retrospective single-center study design. Since TAVI patients from 2008 to 2017 were included, early data include the learning curve, high rates of non-transfemoral access, paravalvular regurgitation and notable rates of short- and mid-term mortality compared to current practice. Despite careful evaluation of clinical documentation and discharge letters, incomplete detection of bleeding episodes cannot entirely be ruled out. Our focus was on the evaluation of clinical bleeding events rather than hemostaseologic parameters. Hence, levels of vWF were not be included in this analysis. Additional prospective studies with larger patient samples may address these shortcomings in the future.
Conclusion
In this large cohort, we demonstrated that Heyde syndrome was prevalent in a relevant number of patients presenting for the treatment of AS. In contrast to earlier publications, a substantial number of recurrent GIB events was observed despite correction of AS by TAVI. Patients with residual paravalvular regurgitation after TAVI may be at higher risk of GIB and should be monitored more closely for bleeding events. In the meantime, optimal hemodynamic results and individualized antithrombotic strategies should be targeted to minimize bleeding risk and improve outcomes in these vulnerable patients with Heyde syndrome.
Abbreviations
- AS:
-
Aortic stenosis
- GI:
-
Gastrointestinal
- GIB:
-
Gastrointestinal bleeding
- HS:
-
Heyde syndrome
- PVL:
-
Paravalvular leak
- SAVR:
-
Surgical aortic valve replacement
- STS PROM:
-
Society for Thoracic Surgeons—predicted risk of mortality
- TAVI:
-
Transcatheter aortic valve implantation
- VWF:
-
Von Willebrand factor
- aVWS:
-
Acquired von Willebrand syndrome
References
HEYDE., C. E. Gastrointestinal bleeding in aortic stenosis (letter). N Engl J Med 1958;259(4):196.
Undas A, Natorska J (2015) Bleeding in patients with severe aortic stenosis in the era of transcatheter aortic valve replacement. JACC Cardiovasc Interv 8(5):701–703. https://doi.org/10.1016/J.JCIN.2015.03.001
Godino C, Lauretta L, Pavon AG et al (2013) Heyde’s syndrome incidence and outcome in patients undergoing transcatheter aortic valve implantation. J Am Coll Cardiol 61(6):687–689. https://doi.org/10.1016/j.jacc.2012.10.041
Caspar T, Jesel L, Desprez D et al (2015) Effects of transcutaneous aortic valve implantation on aortic valve disease-related hemostatic disorders involving von Willebrand factor. Can J Cardiol 31(6):738–743. https://doi.org/10.1016/j.cjca.2015.01.012
Desai R, Parekh T, Singh S et al (2019) Alarming increasing trends in hospitalizations and mortality with heyde’s syndrome: a nationwide inpatient perspective (2007 to 2014). Am J Cardiol 123(7):1149–1155. https://doi.org/10.1016/J.AMJCARD.2018.12.043
Sharma R, Gorbien MJ (1995) Angiodysplasia and lower gastrointestinal tract bleeding in elderly patients. Arch Intern Med 155(8):807. https://doi.org/10.1001/archinte.1995.00430080037005
Le TT, Susen S, Caron C et al (2008) Functional impairment of Von Willebrand factor in hypertrophic cardiomyopathy relation to rest and exercise obstruction. Circulation 18:1550–1557. https://doi.org/10.1161/CIRCULATIONAHA.108.786681
Spangenberg T, Budde U, Schewel D et al (2015) Treatment of acquired von willebrand syndrome in aortic stenosis with transcatheter aortic valve replacement. JACC Cardiovasc Interv 8(5):692–700. https://doi.org/10.1016/j.jcin.2015.02.008
Vincentelli A, Susen S, Le Tourneau T et al (2003) Acquired von Willebrand syndrome in aortic stenosis. N Engl J Med 349(4):343–349. https://doi.org/10.1056/NEJMoa022831
Warkentin TE, Moore JC, Anand SS, Lonn EM, Morgan DG (2003) Gastrointestinal bleeding, angiodysplasia, cardiovascular disease, and acquired von Willebrand syndrome. Transfus Med Rev 17(4):272–286
Thompson JL, Schaff HV, Dearani JA et al (2012) Risk of recurrent gastrointestinal bleeding after aortic valve replacement in patients with Heyde syndrome. J Thorac Cardiovasc Surg 144(1):112–116. https://doi.org/10.1016/j.jtcvs.2011.05.034
Abi-Akar R, El-Rassi I, Karam N, Jassar Y, Slim R, Jebara V (2011) Treatment of heyde’s syndrome by aortic valve replacement. Curr Cardiol Rev 7(1):47–49. https://doi.org/10.2174/157340311795677699
Ramachandran R, Uqdah H, Jani N (2018) A case of recurrent obscure gastrointestinal bleeding: Heyde’s syndrome - case report and review. J Community Hosp Intern Med Perspect 8(3):127–129. https://doi.org/10.1080/20009666.2018.1470441
Pozzi M, Hanss M, Petrosyan A et al (2014) Resolution of acquired von Willebrand syndrome after transcatheter aortic valve implantation through a left transcarotid approach. Int J Cardiol 176(3):1350–1351. https://doi.org/10.1016/j.ijcard.2014.07.267
Balbo CP, Seabra LP, Galoro VG et al (2016) Heyde’s syndrome and transcatheter aortic valve implantation. Arq Bras Cardiol 108(4):378–380. https://doi.org/10.5935/abc.20160193
Sedaghat A, Kulka H, Sinning J-M et al (2017) Transcatheter aortic valve implantation leads to a restoration of von Willebrand factor (VWF) abnormalities in patients with severe aortic stenosis – Incidence and relevance of clinical and subclinical VWF dysfunction in patients undergoing transfemoral TAVI. Thromb Res 151:23–28. https://doi.org/10.1016/J.THROMRES.2016.12.027
Baumgartner H, Falk V, Bax JJ et al (2018) 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev Esp Cardiol (Engl Ed) 71(2):110. https://doi.org/10.1016/j.rec.2017.12.013
Kappetein AP, Head SJ, Généreux P et al (2012) Updated standardized endpoint definitions for transcatheter aortic valve implantation. J Am Coll Cardiol 60(15):1438–1454. https://doi.org/10.1016/j.jacc.2012.09.001
Love JW (1982) The syndrome of calcific aortic stenosis and gastrointestinal bleeding: resolution following aortic valve replacement. J Thorac Cardiovasc Surg 83(5):779–783
Boyle JM, Rowen HE, Saito H, Vicic WJ, Ankeney JL (1981) Severe aortic stenosis in a patient with recurrent gastrointestinal bleeding: replacement of the aortic valve with a porcine xenograft. Am J Gastroenterol 75(2):135–139
King RM, Pluth JR, Giuliani ER (1987) The association of unexplained gastrointestinal bleeding with calcific aortic stenosis. Ann Thorac Surg 44(5):514–516. https://doi.org/10.1016/S0003-4975(10)62112-1
Anderson RP, McGrath K, Street A (1996) Reversal of aortic stenosis, bleeding gastrointestinal angiodysplasia, and von Willebrand syndrome by aortic valve replacement. Lancet (London, England) 347(9002):689–690
Warkentin TE, Moore JC, Morgan DG (2002) Gastrointestinal angiodysplasia and aortic stenosis. N Engl J Med 347(11):858–859. https://doi.org/10.1056/NEJM200209123471122
Mack MJ, Leon MB, Thourani VH et al (2019) Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med 380(18):1695–1705. https://doi.org/10.1056/nejmoa1814052
FDA expands indication for several transcatheter heart valves to patients at low risk for death or major complications associated with open-heart surgery | FDA. Available at: https://www.fda.gov/news-events/press-announcements/fda-expands-indication-several-transcatheter-heart-valves-patients-low-risk-death-or-major. Accessed January 10, 2021.
Généreux P, Cohen DJ, Mack M et al (2014) Incidence, predictors, and prognostic impact of late bleeding complications after transcatheter aortic valve replacement. J Am Coll Cardiol 64(24):2605–2615. https://doi.org/10.1016/j.jacc.2014.08.052
Généreux P, Cohen DJ, Williams MR et al (2014) Bleeding complications after surgical aortic valve replacement compared with transcatheter aortic valve replacement: Insights from the PARTNER i trial (Placement of Aortic Transcatheter Valve). J Am Coll Cardiol 63(11):1100–1109. https://doi.org/10.1016/j.jacc.2013.10.058
Pilgrim T, Stortecky S, Luterbacher F, Windecker S, Wenaweser P (2013) Transcatheter aortic valve implantation and bleeding: Incidence, predictors and prognosis. J Thromb Thrombolysis 35(4):456–462. https://doi.org/10.1007/s11239-012-0842-3
Seiffert M, Conradi L, Terstesse AC et al (2015) Blood transfusion is associated with impaired outcome after transcatheter aortic valve implantation. Catheter Cardiovasc Interv 85(3):460–467. https://doi.org/10.1002/ccd.25691
Brouwer J, Nijenhuis VJ, Delewi R et al (2020) Aspirin with or without clopidogrel after transcatheter aortic-valve implantation. N Engl J Med 383(15):1447–1457. https://doi.org/10.1056/nejmoa2017815
Nijenhuis VJ, Brouwer J, Delewi R et al (2020) Anticoagulation with or without clopidogrel after transcatheter aortic-valve implantation. N Engl J Med 382(18):1696–1707. https://doi.org/10.1056/NEJMoa1915152
Dauerman HL, DeStephan CM, Sommer HT et al (2019) Prolonged clotting time among patients undergoing transcatheter aortic valve replacement. J Am Coll Cardiol. https://doi.org/10.1016/j.jacc.2019.06.022
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Seiffert received travel support from Abbott Vascular, Biotronik, and Edwards Lifesciences, speaker honoraria from Abiomed, Amgen, AstraZeneca, Bayer Healthcare, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, Philips, Medtronic, and Shockwave Medical, and consulting honoraria from Boston Scientific and Shockwave Medical. Dr. Conradi is a proctor for and received speaker honoraria as well as travel compensation from JenaValve, Edwards Lifesciences and Boston Scientific, and received speaker honoraria and travel compensation from Medtronic and is a consultant for Edwards Lifesciences. Dr. Westermann received speaker honoraria from Abiomed, AstraZeneca, Bayer and Novartis. Dr. Schofer received travel compensation from Edwards Lifesciences and St. Jude Medical, as well as speaker honoraria and travel compensation from Boston Scientific. Dr. Ludwig received travel compensation from Edwards Lifesciences. All reported honoraria and travel compensation are outside the submitted work. All other authors report no conflict of interest.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
Cite this article
Waldschmidt, L., Drolz, A., Heimburg, P. et al. Heyde syndrome: prevalence and outcomes in patients undergoing transcatheter aortic valve implantation. Clin Res Cardiol 110, 1939–1946 (2021). https://doi.org/10.1007/s00392-021-01905-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-021-01905-z