
Abstract
Background
Patients with cardiogenic shock or cardiac arrest undergoing venoarterial extracorporeal membrane oxygenation (V-A ECMO) frequently present with blood glucose levels out of normal range. The clinical relevance of such findings in the context of V-A ECMO is unknown. We therefore investigated the prognostic relevance of blood glucose at time of cannulation for V-A ECMO.
Methods
We conducted a single-center retrospective registry study. All patients receiving V-A ECMO from October 2010 to January 2020 were included if blood glucose level at time of cannulation were documented. Patients were divided in five groups according to the initial blood glucose level ranging from hypoglycemic (< 80 mg/dl), normoglycemic (80–140 mg/dl), to mild (141-240 mg/dl), moderate (241–400 mg/dl), and severe (> 400 mg/dl) hyperglycemia, respectively. Clinical presentation, arterial blood gas analysis, and survival were compared between the groups.
Results
392 patients met inclusion criteria. Median age was 62 years (51.5–70.0), SAPS II at admission was 54 (43.5–63.0), and 108/392 (27.6%) were female. 131/392 were discharged alive (hospital survival 33.4%). At time of cannulation, survivors had higher pH, hemoglobin, calcium, bicarbonate but lower potassium and lactate levels compared to non-survivors (all p < 0.01). Outcome of patients diagnosed with particularly high (> 400 mg/dl) and low (< 80 mg/dl) blood glucose at time of V-A ECMO cannulation, respectively, was worse compared to patients with normoglycemic, mildly or moderately elevated values (p = 0.02). Glucose was independently associated with poor outcome after adjustment for other predictors of survival and persisted in all investigated subgroups.
Conclusion
Arterial blood glucose at time of V-A ECMO cannulation predicts in-hospital survival of patients with cardiac shock or after ECPR. Whether dysglycemia represents a potential therapeutic target requires further evaluation in prospective studies.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Venoarterial extracorporeal membrane oxygenation therapy (V-A ECMO) is increasingly used for treatment of severe cardiogenic shock or for extracorporeal cardiopulmonary resuscitation (ECPR). Despite great efforts, mortality rate in patients undergoing V-A ECMO is still about 70% [1, 2], which means a great medical need for improvement.
Previously, admission blood glucose level was identified as a potential prognostic factor in patients with cardiogenic shock. Severe hypo- or hyperglycemia, respectively, was associated with increased in-hospital mortality [3]. Likewise, recent findings suggest that initial blood glucose level below 150 mg/dl is associated with adverse neurological outcome after cardiac arrest [4]. For non-diabetic patients after intra-hospital cardiac arrest (IHCA), extreme blood glucose levels during the first 24 h, hyper- and hypoglycemic, were associated with poor survival [5]. Interestingly, in a large retrospective analysis for patients after out-of-hospital cardiac arrest (OHCA), neurological outcome did not differ between treated and untreated intra-arrest hypoglycemia [6].
Several studies investigated the prognostic value of blood markers including pH, lactate, or standard bicarbonate concentration (SBC) in V-A ECMO [7, 8]. However, the impact of blood glucose has not been investigated yet. Limited data on extreme blood glucose levels only exist for pediatric patients on V-A ECMO therapy [9]. Thus, the aim of the present study was to evaluate the association between blood glucose level at time of cannulation for V-A ECMO and hospital survival.
Methods
Study setting
We conducted a single-center retrospective registry study. Data derive from a registry of all patients on V-A ECMO treated at a medical intensive-care unit (ICU) located at a tertiary university hospital. All patients receiving V-A ECMO from October, 2010 to January, 2020 were included in the analysis. Exclusion criteria were cannulation in the operation theatre, treatment at a different intensive-care unit and missing values for glucose level at the start of the V-A ECMO therapy. In the case of extracorporeal cardiopulmonary resuscitation (ECPR), patients after intra- as well as out-of-hospital cardiac arrest (IHCA and OHCA, respectively) were included.
Local V-A ECMO setting
The center provides a 24/7 service for referral of patients as well as for in-house patients after and during cardiopulmonary resuscitation or in severe cardiogenic shock for V-A ECMO support. As for local policy, decision to cannulate for V-A ECMO is made after multidisciplinary discussion at the bedside. ECPR was defined as V-A ECMO cannulation during continuous cardiopulmonary resuscitation without return of spontaneous circulation (ROSC); or as V-A ECMO cannulation within the first 20 min after ROSC in case of persistent hemodynamic instability as previously suggested [10]. V-A ECMO cannulation and maintenance were done according to regularly revised standard operating procedures as described earlier [11, 12]. In brief, cannulation was performed in Seldinger’s technique by two experienced intensivists and supported by a perfusionist and additional ICU staff. ECMO systems used were SCPC (Sorin Centrifugal Pump Console, LivaNova, London, United Kingdom), Cardiohelp (Maquet Getinge Group, Rastatt, Germany), or CARL controller (Resuscitec GmbH, Freiburg, Germany). Standard venous draining cannulas were 21–23 Fr. / 55 cm and arterial return cannulas 15–17 Fr. / 23 cm (HLS cannula, Maquet Getinge Group, Rastatt, Germany). For patients without life-threatening bleeding, anticoagulation was provided by intravenous administration of unfractionated heparin aiming at a partial thromboplastin time of 50–60 s. The management of vasopressors and fluid therapy was driven by clinical judgement of the ECMO-experienced intensivist as reported earlier [13, 14].
Blood gas analysis
Blood gas analysis was routinely made by point of care testing (POCT) and results were automatically transferred to the electronic patient files. Frequency of POCT was influenced by clinical judgement of the ICU staff, hemodynamic stability, and dynamics of the different parameters. During the first 24 h after cannulation, blood gas analyses were acquired before and after cannulation and approximately every 1–2 h afterwards. Missing values could occur because of out-of-hospital cannulation, errors during the transfer to the hospital information system, POCT machine not connected to the network or because of inaccurately entered information. A minimum of 18 different values were routinely measured with each blood gas analysis, including partial pressure of carbon dioxide (pCO2) and oxygen (pO2), hemoglobin, lactate, sodium, potassium, calcium, chloride, and base excess.
Data acquisition and statistical analysis
Present data derived from a single-center retrospective registry analysis. Parameters at certain times during and after V-A ECMO implantation were automatically sorted and extracted from the data with a search range of ± 1 h. If no glucose value was detected at implantation, a manual search was performed. For blood gas analysis, only arterial samples were used. Patients were grouped according to their initial glucose value (< 80 mg/dl, 81–140 mg/dl, 141–240 mg/dl, 241–400 mg/dl, > 400 mg/dl), which were altered from [3]. Additionally, a second analysis was conducted separating extreme values from moderate measurements. One group consisted of extreme glucose values below 80 mg/dl and above 400 mg/dl, respectively. These patients were compared to all remaining patients with normal, mildly, or moderately elevate blood glucose (81–400 mg/dl). Apart from glucose and other laboratory parameters, we recorded patient demographics and medical history, occurrence of different events (e.g., decannulation, death, discharge from ICU) and different severity of disease scores. For data analysis, SPSS (version 23, IBM Statistics), Python programming language (version 3.8.3, Python Software Foundation), and Prism (version 8, GraphPad) were used. For statistical analysis, unpaired t test, Fisher’s exact/Chi-square test, and Log-rank/Gehan–Breslow test were used as applicable. Multivariate logistic regression analysis was performed for known predictors of survival in patients with V-A ECMO (ECPR, age, lactate, pH, glucose, female gender, and diabetes mellitus). For Cox regression analysis, independent predictors of hospital survival detected in the multivariate logistic regression analysis were included in the model. A p value of < 0.05 was considered statistically significant. All categorical variables were presented in absolute number (percent of all patients) or were presented as median with inter-quartile range for continuous variables if not stated otherwise.
Results
Patient cohort: A total of 467 V-A ECMO patients were screened and 392 met the inclusion criteria (Fig. 1). Median age was 62 years (51.5–70.0 years) at time of V-A ECMO implantation and the group consisted of 284 men and 108 women (27.6%) (Table 1). At time of initiation for V-A ECMO, 173/392 (44%) were in cardiogenic shock and 219/392 (56%) had a cardiac arrest. There was no difference in the rate of comorbidities, age, sex, and BMI between the five groups. Both dysglycemic groups (< 80 mg/dl and > 400 mg/dl) had a trend towards higher SAPS II scores at admission and lower overall duration of ICU stay and V-A ECMO duration compared to the other groups. Survival was higher in the cardiogenic shock group, and age, sex, body measurements, and severity of illness were similar between survivors and non-survivors (suppl. Table 1, online supplement). When comparing blood gas analyses for the different groups, patients with blood glucose levels < 80 mg/dl or > 400 mg/dl had a trend towards lower pH, hemoglobin, bicarbonate but higher lactate levels compared to the other groups (Table 2). At time of cannulation, survivors had higher pH, hemoglobin, calcium, bicarbonate but lower potassium and lactate levels compared to non-survivors (all p < 0.01, suppl. Table 2, online supplement).

Patient selection
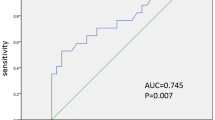
Arterial glucose and outcome: 56/392 (14.3%) patients showed extreme arterial blood glucose levels either above 400 mg/dl or below 80 mg/dl at time of cannulation for V-A ECMO. We observed a significant association of hospital survival with glucose levels determined at start of V-A ECMO. Survival in patients with extreme glucose levels above 400 mg/dl or below 80 mg/dl was 16.1% compared to 36.3% in patients with arterial glucose of 80–400 mg/dl (p = 0.020, Fig. 2). Lower survival occurred in both groups, patients with blood glucose levels < 80 mg/dl and > 400 mg/dl (p < 0.001, Fig. 3). A subgroup analysis of patients with cardiogenic shock patients or ECPR revealed lower survival in patients with extreme glucose levels in both indications (p = 0.005 for ECPR and p = 0.008 for cardiogenic shock, Fig. 3). Additional subgroup analyses including sex, age, elevated HbA1c over 6.5%, and high lactate values over 4 mmol/l consistently revealed a trend towards reduced survival in the extreme glucose group in all subgroups except for HbA1c over 6.5% (Fig. 4).

Survival in relation to different plasma glucose levels. The red stars represent the survival rate of each group, and the blue bars the number of patients per group

Kaplan–Meier survival curves. Glucose unit in mg/dl. a and b all patients with different grouping, c only ECPR patients, and d only patients with cardiogenic shock. V-A ECMO venoarterial extracorporeal membrane oxygenation therapy, ECPR extracorporeal cardiopulmonary resuscitation, CS cardiogenic shock

Forrest plot of different subgroups. OR Odds ratio, CI confidence interval, ECPR extracorporeal cardiopulmonary resuscitation, CS cardiogenic shock
Adjustment of confounders: In a multivariate logistic regression analysis, arterial glucose at V-A ECMO cannulation was an independent predictor of in-hospital mortality (p = 0.019, Table 3). Adjusting for significant predictors of hospital mortality detected in the multivariate logistic regression analysis in a Cox regression model confirmed that glucose is associated with poor outcome (p = 0.032, Table 4).
Discussion
We found a strong, inverse U-shaped association of arterial blood glucose at time of V-A ECMO cannulation and in-hospital survival. This correlation persisted in all investigated models and after adjustment for confounders.
Our findings add on previous studies reporting an association of dysglycemia with mortality. Indeed, in numerous reports from critically ill patient cohorts, hyperglycemia correlated with prognosis. Hyperglycemia is associated with adverse outcomes in critically ill patients with cardiac shock not treated with V-A ECMO [3], after myocardial infarction [15], pneumonia [16], or in mixed collectives of ICU patients [17]. This observation, however, is not new [18]. It has been known for over a century that patients with hemorrhagic shock can develop a hyperglycemia in response to tissue ischemia [19]. A similar correlation between hypoglycemia and poor outcome has been reported [20, 21]. This results in a U-shaped correlation with poor prognosis in dysglycemic patients after myocardial infarction [22]. While some studies suggest that after adjustment for blood lactate, stress hyperglycemia is not associated with outcome [23], other studies suggest hyperglycemia to be an independent predictor of unfavorable outcome [3].
In our study, we found a trend towards higher mortality for dysglycemic patients in all investigated subgroups, except for the diabetic subgroup. The latter is in line with previous studies, suggesting that the association of hyperglycemia with poor outcome is much weaker in diabetic patients [24] and supports the notion that acute rather than chronic hyperglycemia is associated with adverse outcomes [25]. The important question remains, however, in what way dysglycemia causes an increase in all-cause mortality. It has been suggested that hyperglycemia was proportional to the extent of injury [26] and might be a marker for endogenous stress.
There is an ongoing debate whether hypo- and hyperglycemia are only markers of disease severity or causally related to increased mortality and a potential therapeutic target [18]. While preventing hypoglycemia clearly improves outcome, a tight glucose control did not improve outcome in various randomized-controlled trials [27,28,29]. It has even been suggested that stress hyperglycemia is an essential survival response [30], a hypothesis that matches our data since best survival was detected in the patient group with moderately elevated blood glucose levels (140–240 mg/dl) at cannulation.
Extreme glucose levels have been associated with an increased risk for detrimental arrhythmia [31,32,33], cardiogenic shock [34], and cardiovascular death [33]. Importantly, we only investigated patients under V-A ECMO therapy, which should be the best possible therapy to compensate for arrhythmia or impaired tissue perfusion. The fact that the association between outcome and dysglycemia persists under V-A ECMO therapy therefore argues against a causal relationship. However, this should be evaluated in a prospective study. Our results nevertheless encourage incorporating arterial blood glucose in prognostication of patients after cannulation for V-A ECMO.
Conclusion
Arterial blood glucose at time of V-A ECMO cannulation predicts in-hospital survival of patients with cardiac shock or after ECPR. Whether dysglycemia represents a potential therapeutic target requires further evaluation in prospective studies.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BE:
-
Base excess
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- CO:
-
Carbon monoxide
- CS:
-
Cardiogenic shock
- ECPR:
-
Extracorporeal cardiopulmonary resuscitation
- Hb:
-
Hemoglobin
- HbA1c:
-
Glycated hemoglobin
- HCO3 :
-
Bicarbonate
- HCT:
-
Hematocrit
- ICU:
-
Intensive-care unit
- IHCA:
-
In hospital cardiac arrest
- OHCA:
-
Out of hospital cardiac arrest
- PAD:
-
Peripheral artery disease
- pCO2 :
-
Partial pressure of carbon dioxide
- pO2 :
-
Partial pressure of oxygen
- POCT:
-
Point of care testing
- ROSC:
-
Return of spontaneous circulation
- SAPS2:
-
Simplified Acute Physiology Score 2
- SBC:
-
Standard bicarbonate concentration
- SpO2 :
-
Peripheral oxygen saturation
- V-A ECMO:
-
Venoarterial extracorporeal membrane oxygenation therapy
References
Duerschmied D, Zotzmann V, Rieder M, Bemtgen X, Biever PM, Kaier K et al (2020) Myocardial infarction type 1 is frequent in refractory out-of-hospital cardiac arrest (OHCA) treated with extracorporeal cardiopulmonary resuscitation (ECPR). Sci Rep 10:8423
Zavalichi MA, Nistor I, Nedelcu A-E, Zavalichi SD, Georgescu CMA, Stătescu C et al (2020) Extracorporeal membrane oxygenation in cardiogenic shock due to acute myocardial infarction: a systematic review. Biomed Res Int 2020:6126534
Kataja A, Tarvasmäki T, Lassus J, Cardoso J, Mebazaa A, Køber L et al (2017) The association of admission blood glucose level with the clinical picture and prognosis in cardiogenic shock—results from the CardShock Study. Int J Cardiol 226:48–52
Wang C-H, Chang W-T, Huang C-H, Tsai M-S, Chou E, Yu P-H et al (2020) Associations between intra-arrest blood glucose level and outcomes of adult in-hospital cardiac arrest: a 10-year retrospective cohort study. Resuscitation 146:103–110
Beiser DG, Carr GE, Edelson DP, Peberdy MA, Hoek TLV (2009) Derangements in blood glucose following initial resuscitation from in-hospital cardiac arrest: a report from the national registry of cardiopulmonary resuscitation. Resuscitation 80:624–630
Abramson TM, Bosson N, Loza-Gomez A, Eckstein M, Gausche-Hill M. Utility of glucose testing and treatment of hypoglycemia in patients with out-of-hospital cardiac arrest. Prehospital Emerg Care 2021:1–9.
Slottosch I, Liakopoulos O, Kuhn E, Scherner M, Deppe A-C, Sabashnikov A et al (2017) Lactate and lactate clearance as valuable tool to evaluate ECMO therapy in cardiogenic shock. J Crit Care 42:35–41
Wengenmayer T, Duerschmied D, Graf E, Chiabudini M, Benk C, Mühlschlegel S et al (2019) Development and validation of a prognostic model for survival in patients treated with venoarterial extracorporeal membrane oxygenation: the PREDICT VA-ECMO score. Eur Heart J Acute Cardiovasc Care 8:350–359
Lou S, MacLaren G, Paul E, Best D, Delzoppo C, Butt W (2015) Prevalence of dysglycemia and association with outcomes in pediatric extracorporeal membrane oxygenation. Pediatr Crit Care Med 16:270–275
Jacobs I, Nadkarni V, Bahr J, Berg RA et al (2004) cardiac arrest and cardiopulmonary resuscitation outcome reports. Circulation 110:3385–3397
Supady A, Wengenmayer T, Bode C, Staudacher DL (2016) Extrakorporale CPR (eCPR). Notfall Rettungsmed 19:574–581
Wengenmayer T, Rombach S, Ramshorn F, Biever P, Bode C, Duerschmied D et al (2017) Influence of low-flow time on survival after extracorporeal cardiopulmonary resuscitation (eCPR). Crit Care 21:157
Staudacher DL, Gold W, Biever PM, Bode C, Wengenmayer T (2017) Early fluid resuscitation and volume therapy in venoarterial extracorporeal membrane oxygenation. J Crit Care 37:130–135
Wengenmayer T, Schroth F, Biever PM, Duerschmied D, Benk C, Trummer G et al (2018) Albumin fluid resuscitation in patients on venoarterial extracorporeal membrane oxygenation (VA-ECMO) therapy is associated with improved survival. Intensive Care Med 44:2312–2314
Deckers JW, van Domburg RT, Akkerhuis M, Nauta ST (2013) Relation of admission glucose levels, short- and long-term (20-year) mortality after acute myocardial infarction. Am J Cardiol 112:1306–1310
Lepper PM, Ott S, Nüesch E, von Eynatten M, Schumann C, Pletz MW et al (2012) Serum glucose levels for predicting death in patients admitted to hospital for community acquired pneumonia: prospective cohort study. BMJ 344:e3397
Siegelaar SE, Hermanides J, Oudemans-van Straaten HM, van der Voort PH, Bosman RJ, Zandstra DF et al (2010) Mean glucose during ICU admission is related to mortality by a U-shaped curve in surgical and medical patients: a retrospective cohort study. Crit Care 14:R224
Mesotten D, Preiser J-C, Kosiborod M (2015) Glucose management in critically ill adults and children. Lancet Diabetes Endocrinol 3:723–733
Bernard C (1877) Leçons sur le diabète et la glycogenèse animale. Librairie J.-B. Baillière, Paris
Vriesendorp TM, van Santen S, DeVries JH, de Jonge E, Rosendaal FR, Schultz MJ et al (2006) Predisposing factors for hypoglycemia in the intensive care unit. Crit Care Med 34:96–101
NICE-SUGAR Study Investigators, Finfer S, Liu B, Chittock DR, Norton R, Myburgh JA, et al (2012) Hypoglycemia and risk of death in critically ill patients. N Engl J Med 367:1108–18.
Ukena C, Dobre D, Mahfoud F, Kindermann I, Lamiral Z, Tala S et al (2012) Hypo- and hyperglycemia predict outcome in patients with left ventricular dysfunction after acute myocardial infarction: data from EPHESUS. J Card Fail 18:439–445
Kaukonen K-M, Bailey M, Egi M, Orford N, Glassford NJ, Marik PE et al (2014) Stress hyperlactatemia modifies the relationship between stress hyperglycemia and outcome: a retrospective observational study*. Crit Care Med 42:1379–1385
Falciglia M, Freyberg RW, Almenoff PL, D’Alessio DA, Render ML (2009) Hyperglycemia-related mortality in critically Ill patients varies with admission diagnosis. Crit Care Med 37:3001–3009
Liao W-I, Wang J-C, Lin C-S, Yang C-J, Hsu C-C, Chu S-J et al (2019) Elevated glycemic gap predicts acute respiratory failure and in-hospital mortality in acute heart failure patients with diabetes. Sci Rep 9:6279
Ware J, Ljungqvist O, Norberg KA, Efendic S, Nylander G (1982) Glucose, insulin and osmolality changes in rats sustaining different hemorrhage volumes. Acta Physiol Scand 116:31–36
Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N et al (2008) Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 358:125–139
NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY-S, Blair D, Foster D, et al (2009) Intensive versus conventional glucose control in critically ill patients. N Engl J Med 360:1283–97.
Kalfon P, Giraudeau B, Ichai C, Guerrini A, Brechot N, Cinotti R et al (2014) Tight computerized versus conventional glucose control in the ICU: a randomized controlled trial. Intensive Care Med 40:171–181
Marik PE, Bellomo R (2013) Stress hyperglycemia: an essential survival response! Crit Care 17:305
Chow E, Bernjak A, Williams S, Fawdry RA, Hibbert S, Freeman J et al (2014) Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk. Diabetes 63:1738–1747
Grisanti LA (2018) Diabetes and arrhythmias: pathophysiology, mechanisms and therapeutic outcomes. Front Physiol 9:1669
Ponikowski P, Jankowska EA (2013) Hypoglycaemia in diabetic patients: highly undesirable by cardiologists. Eur Heart J 34:3102–3105
Zeller M, Cottin Y, Brindisi M-C, Dentan G, Laurent Y, Janin-Manificat L et al (2004) Impaired fasting glucose and cardiogenic shock in patients with acute myocardial infarction. Eur Heart J 25:308–312
Funding
Open Access funding enabled and organized by Projekt DEAL. None.
Author information
Authors and Affiliations
Contributions
XB, JR, and DS carried out the data collection, design, and planning of this study. XB and DS performed the statistical analysis and drafted the manuscript. AL and AS made substantial contributions to the intellectual content of this paper. All authors participated in the critical discussion of the study and interpretation of data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interests
AS reports research grants and lecture fees from CytoSorbents and lecture fees from Abiomed, both outside the submitted work. The other authors declare that they have no competing interests.
Ethics approval and consent to participate
This retrospective study was approved by the ethics committee of the Albert Ludwigs University of Freiburg, file number 151/14. Patient consent to participate was not needed.
Consent for publication
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bemtgen, X., Rilinger, J., Jäckel, M. et al. Admission blood glucose level and outcome in patients requiring venoarterial extracorporeal membrane oxygenation. Clin Res Cardiol 110, 1484–1492 (2021). https://doi.org/10.1007/s00392-021-01862-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-021-01862-7