
Summary
Incidence of life-threatening hypernatremia due to intoxication in adults is rare. Depending on the rate of its onset severe hypernatremia causes cellular dehydration resulting in extracellular fluid shift. CNS symptoms such as convulsions, lethargy and coma are most common. Typical complications are intracranial bleeding in the early course while cerebral edema can occur secondary to seizures or intracranial bleeding as well as a result of brisk lowering therapy of hypernatremia. To prevent those eventually life-limiting complications, intensivists should be familiar with the management of acute hypernatremia. We report on a case of fatal hypernatremia due to accidental ingestion of a sapidity agent.
Case Report
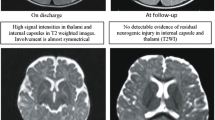
A 26-year old patient with mental retardation accidentally ingested about 875 ml of a flavor intensifier called “Maggi®” containing a total amount of 227.5 g sodium chloride and 2.62 g sodium glutamate, respectively. Serum-sodium peaked at 176 mmol/l, 4 hours after ingestion. Besides immediate diluting-therapy, infusion of glucose 5% as well as therapy with furosemide was started. Another 10 hours after ingestion, hypertensive crisis, generalized convulsions and respiratory depression occurred. Intubation and mechanical ventilation were started. At that time, CCT and CT angiography showed subarachnoidal bleeding, generalized cerebral edema with imminent cerebral herniation and lack of cerebral venous blood flow. Criteria of brain death were fulfilled and the patient succumbed 10 days after admission.
Conclusion
Threatening hypernatremia despite normal renal function is rare, but instantaneous management of this complication can become a vital aspect. Sodium restriction, administration of glucose 5% and diuretics are recommended as a first-line therapy. In case of renal dysfunction or life threatening hypernatremia, extracorporeal elimination procedures like hemodialysis or hemodiafiltration could possibly be necessary within the first 1–2 hours. In chronic cases of hypernatremia, when there was enough time to permit the production of “idiogenic osmoles”, more gradual correction of serum sodium is needed to limit rapid intracellular shifts of water and electrolytes. The ideal rate for serum sodium decrease is between 10–15 mmol per day. The role of sodium glutamate in the development of cerebral edema in our case remains unclear. Existing data in the literature suggests that glutamate could enhance the formation of cerebral edema. However, a total amount of 2.62 g glutamate does not seem enough to effectuate cerebral edema alone.
Zusammenfassung
Die Inzidenz vergiftungsbedingter, lebensbedrohlicher Hypernatriämien bei Erwachsenen ist gering. Abhängig von der Geschwindigkeit der Entwicklung kommt es zur zellulären Dehydrierung durch Flüssigkeitsverschiebungen nach extrazellulär. Neurologische Störungen wie cerebrale Krampfanfälle, Lethargie und komatöse Verlaufsformen gehören zu den häufigsten Symptomen. Typische Komplikationen sind intrakranielle Blutungen in der Frühphase während sich ein Hirnödem sekundär (Blutung, cerebrale Krampfanfälle) oder in Folge einer forcierten Senkung des Serum-Natrium entwickeln kann. Um diese möglicherweise lebensbedrohlichen Komplikationen zu vermeiden, sollten Intensivmediziner mit der Behandlung der akuten Hypernatriämie vertraut sein. Wir berichten über einen Patienten, der nach Konsum einer großen Menge eines Gewürzmittels an den Folgekomplikationen der Hypernatriämie verstarb.
Fallbericht
Ein 26-jähriger, autistischer, mental retardierter Patient hatte akzidentell 875 ml Maggi®-Gewürzmittel getrunken, das eine Gesamtmenge von 227,5 g Natriumchlorid und 2,62 g Natriumglutamat enthielt. 4 Stunden nach Aufnahme lag die Natriumkonzentration im Serum bei maximal 176 mmol/l. Neben einer sofort eingeleiteten Verdünnungstherapie wurde 5%ige Glucoselösung und Furosemid verabreicht. Etwa 10 Stunden nach Einnahme entwikkelte der Patient eine hypertensive Krise, cerebrale Krampfanfälle sowie eine respiratorische Insuffizienz, so dass mit einer Beatmungstherapie begonnen wurde. Zu dieser Zeit waren im CCT ein generalisiertes Hirnödem, eine SAB sowie ein fehlender venöser Blutfluss nachweisbar. Die Diagnose des Hirntodes wurde gestellt und der Patient verstarb 10 Tage nach Aufnahme.
Schlussfolgerung
Bedrohliche Hypernatriämie trotz intakter Nierenfunktion ist selten und bedarf einer umgehend einzuleitenden Therapie, um bleibende neurologische Schäden oder einen letalen Verlauf zu verhindern. Als Erstmaßnahme kommen neben der Natriumrestriktion die Zufuhr elektrolytfreier Glucoselösung sowie die Therapie mit einem Schleifendiuretikum in Frage. In Fällen einer Niereninsuffizienz oder einer lebensbedrohlichen Hypernatriämie können innerhalb der ersten 1–2 Stunden extrakorporale Eliminationsverfahren wie die Hämodialyse oder die Hämodiaperfusion zum Einsatz kommen, um das Absenken des Serum- Natrium gezielt steuern zu können. Die Rolle von Natriumglutamat in unserer Kasuistik bleibt unklar, wenngleich Literaturhinweise existieren, dass Natriumglutamat ein Effekt in der Ödemgenese des ZNS zugeschrieben wird. Die Menge von 2,62 g Natriumglutamat scheint als alleinige Ursache für die Entwicklung des Hirnödems allerdings nicht auszureichen.
Similar content being viewed by others


References
Barer J, Hill LL, Hill RM (1973) Fatal poisoning from salt used as an emetic. Am J Dis Child 125:889–890
Conley SB (1990) Hypernatremia. Pediatr Clin North Am 37:365–372
Roscelli JD, Clifton EY, Southgate WM (1994) Management of salt poisoning in an extremely low birth weight infant. Pediatr Neprol 8:172–174
Adrogué HJ, Madias N (2000) Hypernatremia. NEJM 20:1493–1499
Finberg L, Kiley J, Luttrell CN (1963) Mass accidental salt poisoning in infancy. A study of a hospital disaster. JAMA 184:121–124
Feldman K, Robertson WO (1979) Salt poisoning: presenting symptom of child abuse. Vet Hum Toxicol 21:341–343
Plum J, Grabensee B (1994) Störungen des Natrium- und Wasserhaushaltes beim kritisch Kranken. Intensivmed 31:254–263
Weiner M, Epstein FH (1970) Signs and symptoms of electrolyte disorders. Yale J Biol Med 43(2):76–109
Asahara H, Maruyama S, Motomura S, Tamura K, Miyoshi T (1998) A case of severe hypernatremia complicated with rhabdomyolysis. Rinsho Shinkeigaku 38(4):301–304
Konno S, Nakagawa T, Yoshida T, Hayashibe Y, Maemura T, Goto K, Kamaki M (1993) A case report of central pontine myelinolysis associated with serum hyperosmolality after open heart surgery. Kyobu Geka 46:150–154
Fleck S, Schumacher M, Smolle KH, Kaufmann P, Lueger A (1996) Rhabdomyolyse und zentrale Myelinolyse als Folge einer schweren Hypernatriämie mit Hyperosmolalität. Intensivmed 33:52–56
Ichai C, Fenouil E, Grimaud D (1994) Osmolality and brain. Ann Fr Anesth Reanim 13(1):68–79
Brass EP, Thompson WL (1982) Drug-induced electrolyte abnormalities. Drugs 24:207–228
Alpern RJ, Saxton CR, Seldin DW (1990) Clinical interpretation of laboratory values. In: Tannen R, Kokko JP (eds) Fluid and electrolytes. WB Saunders, Philadelphia, pp 3–58
Moder KG, Hurley DL (1990) Fatal hypernatremia from exogenous salt intake: report of a case and review of the literature. Mayo Clin Proc 65:1587–1594
Paut O, André N, Fabre P, Sobraqus P, Drouet G, Arditti J, Camboulives J (1999) The management of extreme hypernatriaemia secondary to salt poisoning in an infant. Paediatric Anaesthesia 9:171–174
Sanchez Martos I, Ros Perez P, Otheo de Tejada E, Vazquez Martinez JL, Perez-Caballero C, Fernandez Pineda L (2000) Fatal hypernatremia due to accidental administration of table salt. An Esp Pediatr 53(4):495–498
Arieff AI (1984) Central nervous system manifestations of disordered sodium metabolism. Clin Endocrinol Metab 13:269–294
Snyder NA, Feigal DW, Arieff AI (1987) Hypernatremia in elderly patients: a heterogeneous, morbid, and iatrogenic entity. Ann Intern Med 107:309–319
Palevsky PM, Bhagrath R, Greenberg A (1996) Hypernatremia in hospitalized patients. Ann Intern Med 124:197–203
Meadow R (1993) Non-accidental salt poisoning. Arch Dis Child 68:448–452
Ramadas DJ, Moyes CD (1994) Hypernatraemia still seen as a problem in paediatric practice. NZ Med J 107:311–313
Adrogué HJ, Wesson DE (1994) Hyponatremia and hypernatremia. In: Salt & water. Blackwell Scientific, Boston 205–284
Palevsky PM (1998) Hypernatremia. In: Greenberg A (ed) Primer on kidney diseases. 2nd. Academic Press, San Diego, Calif 64–71
Lien YH, Shapiro JI, Chan L (1990) Effects of hypernatremia on organic brain osmoles. J Clin Invest 85:1427–1435
Adrogué HJ, Madias NE (1997) Aiding fluid prescription for dysnatremias. Intensive Care Med 23:309–316
Kempski O, von Andrian U, Schurer L, Baethmann A (1990) Intravenous glutamate enhances edema formation after freezing lesion. Adv Neurol 52:219–223
Stover JF, Kempski OS (1999) Glutamate-containing parenteral nutrition doubles plasma glutamate: a risk factor in neurosurgical patients with blood-brain barrier damage? Crit Care Med 27(10):2252–2260
Butterworth RF (2002) Glutamate transporters in hyperammonemia. Neurochemistry International 41:81–85
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Eyer, F., Felgenhauer, N., Pfab, R. et al. Verlauf und Therapie einer akzidentellen Maggi®-Vergiftung mit tödlichem Ausgang. Intensivmed 41, 598–603 (2004). https://doi.org/10.1007/s00390-004-0471-y
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00390-004-0471-y