
Abstract
Necrotizing enterocolitis (NEC) is one of the diseases in neonates, with a high morbidity and mortality rate, especially in preterm infants. This review aimed to briefly introduce the latest epidemiology, susceptibility factors, and clinical diagnosis and presentation of NEC. We also organized new prevention strategies by risk factors according to different pathogeneses and then discussed new treatment methods based on Bell's staging and complications, and the classification of mild to high severity based on clinical and imaging manifestations. Such a generalization will help clinicians and researchers to gain a deeper understanding of the disease and to conduct more targeted classification, grading prevention, and exploration. We focused on prevention and treatment of the early and suspected stages of NEC, including the discovery of novel biomarkers and drugs to control disease progression. At the same time, we discussed its clinical application, future development, and shortcomings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Necrotizing enterocolitis (NEC) is a devastating and destructive intestinal necrosis syndrome of the immature intestine in newborns, especially in preterm and low birth weight infants (LBWIs), with a prevalence of about 1‰ [1], up to 11% in very low birth weight infants (VLBWIs) of < 1500 g [2], and up to 22% in extremely low birth weight infants (ELBWIs) of < 1000 g [3]. A systematic review by Jones and Hall provided the most recent data on the epidemiology of NEC [4]: the total mortality rate of infants diagnosed with NEC is 23.5%, with the highest mortality rate of 50.9% for ELBWIs with NEC combined with surgery. Even if they survive, their prognosis is poor, with neurodevelopmental disorders (NDD) and intestinal failure (IF) being the most serious complications, occurring in 24.8% and 15.2% of all children with NEC, and in 59.3% and 35.3% of children with NEC requiring surgery, respectively.
Conventional understanding of NEC
The etiology of NEC has not been determined, however, prematurity is the main cause of the disease [5]. This is due to the fact that in preterm infants and in cases of intrauterine growth restriction, newborns have immature intestines with poor peristalsis, but high permeability and low secretion of gastric acid and digestive enzymes; thus, their viability is low [6, 7]. In addition, the intestinal mucosa is easily damaged and deteriorates under inflammatory conditions, leading to total necrosis and perforation, which in turn leads to systemic inflammation, causing complications, such as neurodevelopmental disorders and lung damage [8]. In addition, local ischemia and hypoxia and/or impaired microcirculation, disturbances in the intestinal flora, and formula feeding (NEC occurs mainly in preterm infants who have received enteral feeding) are also major pathogenic factors [6,7,8].
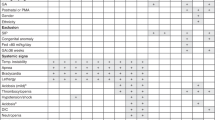
NEC can lead to intestinal inflammation and intestinal necrosis [9]. Currently, the confirmation of NEC diagnosis is complex and lacks clinical diagnostic indicators with good specificity and high sensitivity. A combination of the following clinical signs is generally required: sudden onset of feeding intolerance, abdominal distention, bloody stools, and signs of sepsis (i.e., changes in the heart rate, respiratory rate, temperature, and blood pressure) in preterm infants [10, 11]. Subsequently, the C-reactive protein (CRP) and procalcitonin (PCT) values in routine blood tests; acid replacement and coagulation in blood gas analysis and electrolytes; and blood, urine, fecal, and cerebrospinal fluid culture results in pathogenesis are taken into account. The current and commonly used clinical staging of NEC is the Bell scale, which integrates the clinical and radiological manifestations of the child and classifies NEC into stages I, II, and III according to severity [12]. In 1986, Kliegman and Walsh modified and refined the Bell scale and used it widely to grade the severity of the disease and to guide treatment [13].
In stage I (suspected stage), children exhibit mild intestinal symptoms, non-specific systemic symptoms, and radiographical changes. In stage II (confirmed stage), the child's systemic symptoms worsen, with obvious abdominal distension, abdominal pressure and abdominal wall edema, thrombocytopenia with metabolic acidosis, and typical pneumatosis of the intestinal wall on X-rays. The child is then treated with nasogastric decompression, intravenous fluids, and broad-spectrum antibiotics. In view of the medical treatment, Bell stages I and II are also collectively referred to as the "medical NEC" stage. In stage III (progressive stage), the child develops peritonitis and hypotension together with worsening of stage II symptoms, metabolic acidosis and shock in severe cases, pneumoperitoneum on imaging, multi-organ failure, and intestinal perforation in critically ill children [7]. For children with stage III NEC, it is clear that surgery is urgently needed [14], with 20–50% of these children undergoing surgery [15, 16]. A long length of the bowel is removed, which predisposes patients to short bowel syndrome (SBS). Children with SBS require long-term parenteral nutrition (PN) [14], increasing the risk of complications, including NDD, IF, abnormal development of intestinal structures, pulmonary sequelae, and cholestatic liver disease caused by an inflammatory cascade response [1, 17,18,19,20]. In addition, the surgery also increases NEC mortality from 3 to 30% [21].
Hot topics in NEC
Development of new scores
Bell staging is the first criteria for necrotizing enterocolitis, and is widely used in clinical practice, so this standard is mainly mentioned in this paper. Despite wide use of Bell staging to define NEC, there are several limitations as discussed below. Bell staging is not an explicit case definition, this can lead to over- or underestimation of NEC as was reported in a recent Swedish cohort study [22]. In addition, neither Bell staging nor modified Bell staging accounts for baseline risk, particularly gestational age, which is a major risk factor that influences the baseline risk of NEC. In recent years, newer scoring criteria or diagnostic definitions for NEC have made certain new progress [23].
Vermont Oxford Network (VON) definition
VON is a collaborative, currently including more than 1200 hospitals around the world that supports benchmarking of outcomes and quality improvement. The VON criteria define NEC as a diagnosis at surgery or on post-mortem examination or based on clinical and radiographic criteria (comprises features from Bell staging). Recent reports have noted a declining incidence of NEC in the United States, from 7.1% in 2005 to 5.2% in 2014, using this definition [24].
Centers for Disease Control and Prevention (CDC) definition
The CDC is a US Health Agency that performs infectious disease surveillance through the National Health Safety Network. The CDC surveillance definition for NEC is similar to the VON definition, with some modifications. Surgical NEC is defined as meeting one of the following findings: surgical evidence of extensive bowel necrosis (> 2 cm of bowel affected) or surgical evidence of pneumatosis intestinalis with or without intestinal perforation [23].
Gestational age-specific case definition of NEC (UK)
The UK Neonatal Collaborative NEC (UKNC-NEC) Study Group developed a point-based gestational age-specific case definition using a population-based cohort of infants [25]. The authors reported a lower error rate in classifying infants with NEC when compared to the VON definition.
Two out of 3 rule
The 2 out of 3 rule (2 of 3) is a scoring system, and the authors who proposed this rule have highlighted defining NEC subsets based on possible etiology or risk factors [26].
Stanford NEC score
This Stanford NEC score was developed using a six-center cohort of 520 infants with suspicion of NEC [27], which can be used to classify the severity of disease and also determine the risk of progression of disease.
International Neonatal Consortium (INC) NEC workgroup definition
A workgroup of stakeholders was assembled by the INC to guide the development of a new definition of NEC [28]. The report recommends infants with NEC that do not meet the criteria for “preterm NEC” should be classified as either “atypical NEC” or “term NEC” for reporting in clinical research.
Clinical scenarios
The traditional "Textbook" NEC is less common in clinical practice and more common in atypical manifestations, such as staccato NEC and pan-intestinal NEC [29]. In view of the heterogeneity of clinical presentation of patients with NEC, Hackam et al. have recently described five different types of presentation [30]. This classification based on clinical scenarios can help clinicians better understand the pathogenesis and determine the best treatment [31].
“Textbook”NEC
“Textbook” NEC refers to the presentation in which a premature infant who is predominantly formula-fed develops abdominal distention and bloody stools, and which is associated with the presence of a characteristic finding on abdominal plain films termed pneumatosis intestinalis, which refers to the presence of gas within the wall of the bowel, including the reversibility of the accompanying septic process and the presence of comorbidities.
Persistent NEC without free air
This presentation refers to the infant who develops NEC as above (presence of pneumatosis intestinalis) and fails to improve clinically but does not demonstrate obvious intestinal perforation. In the absence of clear improvement, exploratory laparotomy may reveal patchy necrosis and evidence of acute or indolent intestinal perforations.
Portal venous gas and abdominal tenderness
This presentation refers to the child with abdominal findings of air within the portal system, which generally suggests significant intestinal necrosis in the setting of abdominal tenderness.
Staccato NEC
This presentation refers to the child with NEC who is initially relatively stable yet rapidly develops deterioration characterized by overwhelming sepsis accompanied by clinical and radiographic evidence of NEC that evolves over hours.
NEC totalis
The child with NEC totalis exhibits extensive necrosis that involves nearly all the small and large intestines. While NEC totalis may be suspected on abdominal X-rays based upon the extent of pneumatosis intestinalis, the diagnosis of NEC totalis is often only made at laparotomy.
Given the complexity of NEC diagnosis and the limited availability of treatments, basic and clinical research on NEC has favored early prevention and treatment to control the disease at the "medical NEC" stage, avoiding surgery in the Bell III stage, which can cause irreversible suffering to the child. To date, the most accepted prevention and treatment measures are standardized feeding regimens, progressive feeding, breast milk, prophylactic antibiotics, and probiotics [6]. In addition, with the development of NEC diagnosis and treatment research, some new prevention and treatment strategies are gradually emerging in the field of preclinical and clinical research. Therefore, this review analyzes the prevention and treatment protocols based on risk factors and mild to high severity grading of NEC, with the aim of developing individualized prevention and treatment protocols for children with NEC with different pathogeneses, thereby improving the cure rate and reducing complications in children with NEC.
Prevention strategy of NEC
In recent years, researchers have explored new strategies to reduce the risk factors of NEC, and here, we classify them according to their predisposing factors and possible pathogenesis, and summarize the latest research results (Table 1).
Prevention of premature delivery and intestinal immaturity
Prevention of preterm birth and promotion of intestinal maturation in preterm infants can help prevent the development of NEC. One study found that prophylactic use of prenatal glucocorticoids reduced the morbidity and mortality of premature delivery-related neonatal disorders, including NEC [32]. A meta-analysis of 15 randomized controlled trials showed that prenatal application of glucocorticosteroids was effective in reducing the incidence of NEC [33]. In addition, a review of 30 randomized controlled trials (including 8158 infants) showed that prenatal application of corticosteroids reduced the morbidity and mortality of preterm birth and NEC in newborns without significant harm to the mother or the newborn [34]. Similarly, guiding the mother's diet and antibiotic use, and intervening in her microbiota and infections, might also influence the early gut flora colonization pattern of the infant and prevent NEC [17, 35]. Evidence-based medicine has shown that currently, the most practical approaches to prevent NEC include optimizing maternal health care, reducing obstetric complications in mothers, and decreasing their risk of preterm birth [36].
Prevention of abnormal colonization of intestinal bacteria and the microbiota
Early microbial ecological dysbiosis is associated with the occurrence of NEC, and therefore, research on NEC prevention has focused on the use of probiotics in past decades. Several meta-analyses reviewed clinical trials involving more than 10,000 infants and came to the overall conclusion that probiotics can prevent NEC [37]. Breast milk contains a large amount of probiotics; however, the amount of breast milk from mothers of preterm infants is clinically low, making the administration of probiotics a reasonable measure to prevent NEC. In addition, bifidobacteria and lactobacilli are equally effective in the prevention of NEC in children, although a mixture of bifidobacteria and streptococci is more effective; however, there is a lack of clinically accurate comparative data [38], and both the inclusion criteria and strain doses are major barriers to forming evidence-based conclusions [39]. Currently, the systematic use of probiotics for NEC prevention is controversial because of the complexity of the strains and the lack of valid evidence for their clinical use, in addition to a series of published cases showing that probiotics use can lead to adverse outcomes such as sepsis [40].
Prevention of risks associated with formula feeding and enteral nutrition
Breast milk is rich in several bioactive factors that improve the gastrointestinal defenses of infants. Several clinical trials have shown that breastfeeding can standardize feeding regimens, prevent postnatal growth restriction, and reduce the incidence of NEC [41]. Two randomized trials have also demonstrated that breastfeeding reduces the incidence of NEC in preterm infants compared with formula feeding [42, 43]. A study involving 207 infants also found a significantly lower incidence of NEC in infants who were exclusively breastfed compared with those fed with breast milk fortified products [44].
Donor breast milk is also a good option when the mother is unable to provide breast milk. A systematic review and meta-analysis of 11 randomized or quasi-randomized trials, involving 1809 preterm or low birth weight (LBW) infants, found that donor breast milk was effective in preventing NEC [45], with a 64% reduction in the risk of NEC compared with breast milk fortification [46]. However, ethically, preterm infants should only receive pasteurized donor breast milk if they do not have their own mother's breast milk [47]. Notably, slow feeding patterns have been proposed; however, the available experimental data demonstrate that slow advancement of enteral nutrition might have little or no effect on the risk of NEC and mortality in preterm or VLBW infants, and might even slightly increase the risk of feeding intolerance and invasive infections [48].
Indeed, in a compelling article, “Can We Cut the Incidence of Necrotizing Enterocolitis in Half-Today?” [49], Dr Robert Christensen argued that adopting two practices: near-exclusive breast milk feeding and the use of standardized feeding protocols (SFPs), could do just that [50]. SFPs address a consistent approach to the: (a) preferred feeding substance; (b) advancement and fortification of feeding; (c) criteria to stop and specifying how to re-start feedings once held; (d) identification and handling of feeding intolerance; and (e) initiation and duration of trophic feeding. SFPs are simple, inexpensive, effective, and transmissible methods for prevention of NEC [41].
Prevention of infection and inflammation
Prevention of infection and control of inflammation are equally crucial in the prevention and treatment of NEC. It was reported that interleukin 10 (IL-10) prevents disease progression in NEC mice by regulating intestinal inflammation [51]. Toll-like receptor 4 (TLR4) signaling plays a key role in mediating intestinal inflammatory imbalance, and intra-intestinal strategies targeting TLR4 in preterm infants might represent a new approach to NEC prevention [52]. Fetal intestinal lumen immersion in amniotic fluid has been documented to prevent TLR4 activation and thus NEC [53]. Breast milk is rich in the nitric oxide precursor, sodium nitrate [54], and oligosaccharide, both of which are absorbed in circulation and promote nitric oxide release [55]. This counteracts the effects of TLR4 signaling on the mesenteric endothelium, reducing intestinal inflammation, and thus decreasing the incidence of NEC. Recent studies have shown that chondroitin sulfate (CS) attenuates inflammation, prevents intestinal ecological dysregulation, and reduces the severity and mortality of NEC [56].
Prevention of local ischemia-hypoxia reperfusion injury of the intestine
Studies have demonstrated the presence of microcirculatory injury in the intestine of children with NEC [57, 58], and this injury can be improved by direct peritoneal resuscitation [59, 60]. It was found that prostaglandin E2 (PGE2) and its receptor, prostaglandin E receptor 4 (PTGER4, also known as EP4) improved intestinal blood flow and provided intestinal protection against NEC in neonatal rats [61]. Similarly, 1.5% glucose solution delivered by intraperitoneal infusion enhanced ileal blood flow and prevented NEC in neonatal rats [62]. Several other clinical studies have shown that measures, such as reducing feeding during transfusion [63], screening children for congenital heart disease [64], and supplementation with arginine (arginine and/or citrulline, amino acids that play an important role in nitric oxide production and the regulation of intestinal blood flow, showing a reduced level in NEC) [65], can prevent NEC [66]. A recent study of intestinal tissue from children with NEC showed that the levels of hypoxia markers hypoxia-inducible factor 1 (HIF-1) and glucose transporter 1 (GLUT1) were elevated in NEC, suggesting their potential role in the prevention of reperfusion injury in NEC [67].
Remote ischemic conditioning (RIC) is a new approach to prevent and treat NEC. Preclinical studies have led to the discovery of remote ischemic conditioning (RIC) as a promising non-invasive intervention in protecting the intestine against ischemia-induced damage during early-stage NEC. RIC involves the administration of brief reversible cycles of ischemia and reperfusion in a limb (similar to taking standard blood pressure measurement) which activate endogenous protective signaling pathways that are conveyed to distant organs such as the intestine. RIC targets the intestinal microcirculation and by improving blood flow to the intestine, reduces the intestinal damage of experimental NEC and prolongs survival [68]. A phase II feasibility randomized controlled trial involving 12 centers in 6 countries is currently underway, to investigate the feasibility of RIC as a treatment for early-stage NEC in preterm neonates [69].
Treatment of NEC
The early clinical manifestations of NEC are not specific, and the lack of specific biological markers often makes it difficult to diagnose. The most widely used is the Bell score, which integrates the clinical and imaging manifestations of the child. We will summarize the current treatments for NEC in a step-by-step manner based on the clinical manifestations and imaging examinations of the child in Bell's staging, and organize them according to disease severity (Fig. 1, Table 2).

Summarized treatments for NEC according to disease severity
Treatment of mild or suspected NEC
Suspension of enteral feeding strategy (Non-per os, NPO status)
Clinically, NPO significantly improves the early suspected symptoms of NEC; however, clinicians often hesitate about when to start refeeding after NPO because of the lack of an optimal time point for refeeding [70]. Similarly, a meta-analysis showed no significant difference in outcomes for children who resumed feeding early (within 5 days of NEC diagnosis) and late (> 5 days after NEC diagnosis) [71]. However, ultrasound was used to compare children who were fed without portal gas for 3 consecutive days with children who were fed without portal gas for 10 consecutive days, and it was found that early resumption of feeding had a lower complication rate, a shorter course of antibiotics, faster feeding progress, and a shorter hospital stay [72]. Therefore, the duration of NPO should be minimized clinically and the child should start to feed immediately after stabilization of vital signs, resolution of thrombocytopenia, and clinical improvement, as determined by abdominal radiography or ultrasonography.
Biomarker screening for the early identification of NEC
Unlike the sudden appearance of overt clinical signs in mid- to late-stage disease, the onset of NEC is often subtle and insidious; therefore, many researchers have attempted to identify new biomarkers from serum, stool, and urine samples to help confirm or rule out NEC [19]. Urine of children with NEC had significantly higher levels of intestinal fatty acid binding protein (I-FABP), and I-FABP levels in the intestines of children with severe NEC are significantly higher than those of infants who do not need surgery, suggesting that I-FABP levels might indicate the severity of the disease. The levels of an intestinal tight junction protein, claudin-3, are also elevated in children with NEC, implying a loss of intestinal wall integrity [73]. Plasma levels of the inter-α-inhibitor protein (which helps to regulate systemic inflammation) are significantly lower in children with NEC [74]. Calprotectin levels are significantly higher in the stools of children with NEC [73, 75] and correlate with disease severity [76]. Ultrasound [77] and near-infrared spectroscopy (NIRS) [78] mainly detect changes in blood flow and oxygenation, which are helpful in the early prediction of NEC. The intestinal microbiota related to the occurrence and development of NEC has also been profoundly investigated [79]. These emerging prediction methods for early diagnosis of NEC mentioned above have been systematically reviewed recently [80].
Mining potential biomarkers and integrating multi-signal scoring systems are also hot research topics. The Apolipoprotein-Serum Amyloid A (ApoSAA) scoring system, which integrates apolipoprotein-CII and a des-arginine variant of serum amyloid A, scores higher in children with NEC, and can be used to identify which children that can be taken off antibiotics[81]. Another study integrated fecal calprotectin and urinary I-FABP-binding protein to confirm the diagnosis of preterm infants with clinically suspected NEC [82]. There are also many candidate biomarkers that can be integrated and used to differentiate NEC from other benign neonatal intestinal disorders and to assess disease prognosis. In a prospective observational cohort study, determination of local intestinal oxygen saturation (rintSO2) in the urine of 27 preterm infants with the aid of NIRS, and intestinal I-FABP levels, predicted intestinal strictures after the onset of NEC, but not the rate of NEC recurrence [83]. A recent study of infants at a corrected age of 24–40 weeks [84] demonstrated higher intestinal alkaline phosphatase (IAP) and lower IAP enzyme activity in the stool of children with NEC. IAP is also a useful biomarker that responds to disease severity and could be used to improve clinical NPO duration [84].
The above are the most promising traditional biological markers available. However, an ideal biomarker would be non-invasive, specific for intestinal inflammation, and have the ability to differentiate NEC from other non-NEC diseases. It is difficult to find a single biomarker or a group of biomarkers that meet all of these criteria. Using omics technologies is possible to quantify a very large number of small molecules simultaneously with a very small number of specimens. Thus, metabolomics and proteomics have been used to explore NEC biomarkers over the last 10 years or so, and these studies have been systematically reviewed [85]. Among them, four studies dealt with metabolomics [86,87,88,89], six with proteomics [90,91,92,93,94,95], and four studies integrated metabolomics with either proteomics (one study) [96] or metagenomics (three studies) [87, 97, 98]. These published clinical studies on metabolomics and proteomics have potential to discover NEC biomarkers.
Nutritional support strategies
Delaying the start of enteral feeding was previously thought to reduce the incidence of NEC; however, recent studies have shown that early initiation of enteral nutrition does not increase the incidence of NEC [99, 100].
Breast milk is the only factor that has consistently been shown to improve NEC [101, 102]. The incidence of NEC in formula-only fed infants is 6–10 times higher than that in exclusively breastfed infants [103]. Recognized nutrients aside, some non-nutrient components of breast milk contribute to gastrointestinal immune function and mucosal integrity [104], including IgA, growth hormones (epidermal growth factor, insulin, and insulin-like growth factor), polyunsaturated fatty acids, and oligosaccharides. It was found that IgA in the first month of life was mainly derived from breast milk, while children with NEC at the same age had more IgA-unconjugated bacteria. Animal studies have also shown that mouse pups fed by IgA-deficient mothers are more susceptible to NEC [105]. Oligosaccharides in breast milk are known to stimulate beneficial bacteria and downregulate bacteria-associated inflammatory signaling in mouse models [106]. Breast milk-derived exosomes significantly reduced the incidence and severity of NEC in experimental animals [107] and reduced inflammation in intestinal-like organs [108]. Moreover, exosomes of colostrum origin are more protective [109], and breast milk exosomes from mothers of preterm infants enhance the proliferation and migration of IECs compared with those of full-term infants [110]. Mechanistically, breast milk-derived exosomes attenuate intestinal epithelial cell death [111] and protect intestinal stem cells from oxidative stress damage through the Wnt/β-catenin signaling pathway [112].
When maternal the breast milk supply is inadequate, infants often require supplemental donor breast milk or formula. Donor breast milk reduces the risk of NEC by 79% compared with cow's milk and other formulas [44, 113, 114]. A review of 12 clinical trials found that children fed using formula milk exhibited a higher risk of NEC [115]. The incidence of NEC was also higher when cow's milk was used [44, 116]. This is due to the protective factors contained in donor breast milk. Of course, the high reactivity of the intestine to milk proteins also contributes to the development of NEC. Studies have found that cytokines (interferon-gamma, IL-4, and IL-5) are more sensitive to milk proteins (lactoglobulin and casein) and are more prone to inflammation [117]. However, purification of milk to obtain exosomes improves NEC by stimulating cupped cells to attenuate mucin 2 (MUC2) and glucose-regulated protein 94 (GRP94) levels, which benefits children at high risk of NEC who do not have access to donor breast milk [118].
In addition, PN is commonly used in children undergoing NPO after the diagnosis of NEC. Intravenous nutrients (carbohydrates, amino acids, lipids, electrolytes, minerals and vitamins) are administered to maintain nutrition while resting the intestine. PN starts with adequate protein (3.5–4 g/kg/day) to maintain a positive nitrogen balance, improve body weight, and repair damaged tissues [10, 119,120,121]. However, some studies have shown that PN did not significantly improve the prognosis of NEC, nor did it reduce the proportion of children undergoing surgery or hospital mortality [122]; thus, the role of PN needs to be further confirmed.
New drug development
Novel biological agents might play a role in the treatment of NEC. Heparin-conjugated epidermal growth factor (EGF)-like growth factor reversed NEC in multiple animal models by promoting mucosal healing [123], restoring intestinal stem cell function [124], and improving microcirculation [57, 125]. A readily absorbed, nontoxic oligosaccharide, C34, is a 2-acetamidopyranoside (MW 389) with the formula C17H27NO9, which attenuated intestinal inflammation by inhibiting TLR4 signaling, ameliorated NEC lesions in mice and piglets, and reduced inflammation in human intestinal organoids obtained during NEC treatment [126]. Breast milk oligosaccharides have also been shown to have an important role in NEC treatment [127, 128]. Amniotic fluid is rich in growth factors to protect the mucosa and inhibits TLR4 signaling to reduce inflammation; thus, the use of simulated amniotic fluid is beneficial in the treatment of NEC [53, 129, 130]. Oral lactoferrin (with or without prebiotics) has been shown to be effective in blocking the development of NEC [131]. These therapies still need to be refined in clinical trials before they can be widely used in the clinical setting. The current hot topic is the treatment of NEC with various stem cells (bone marrow mesenchymal stem cells, amniotic fluid stem cells, and umbilical cord blood stem cells) and their exosomes, in addition to the treatment of NEC using breast milk exosomes mentioned above [132]. Recent studies have also identified some new therapeutic pathways and targets. Silencing angiopoietin-2 to block the Notch signaling pathway reduces lipopolysaccharide-induced inflammation, barrier dysfunction, and endoplasmic reticulum stress in intestinal epithelial cells [133]. The regulatory role of IL1-β on intestinal epithelial cell tight junctions and potential targeted therapies has also been studied [134]. The low-dose cyclooxygenase 2 (COX-2) inhibitor, celecoxib, improved the histopathological profile of the ileum of NEC rats, attenuated oxidative stress and inflammation, and reduced epithelial cell apoptosis, making it a potential therapeutic approach for NEC [135]. Sodium butyrate alleviated intestinal inflammation in mice with necrotizing small intestinal colitis [136]. Intestinal supplementation with dihydroxyacetone (DHA) might reduce the incidence of NEC in preterm infants by modulating the production of regulatory cytokines through its immunomodulatory effects [137]. Fecal filtrate transplantation (FFT) is effective in preventing NEC with no significant side effects [138] and amniotic fluid stem cell injection therapy prevented epithelial cell damage in necrotizing small bowel colitis [139]. Finally, tocilizumab inhibition of IL-6 may be a potential option for the treatment of NEC [140].
Treatment of moderate NEC
Intravenous fluids, respiratory support, and condition monitoring
Supportive infusions include standard metabolic and hydride resuscitation (electrolyte and glucose added solutions) [141] to avoid water overload or excessive positive balance. A meta-analysis found that fluid restriction significantly reduced the incidence of NEC [142]. Preterm infants can develop NEC 48 h after receiving a transfusion [143, 144]; therefore, for children at risk for NEC, the potential risk of fluid overload should be considered [145]. Neurological, cardiac, hepatic, renal, and pulmonary organ function need to be evaluated regularly as NEC progresses [145]. Blood gas and the metabolic/electrolyte balance are checked regularly, different levels of respiratory support (from oxygen delivery to mechanical assistance) are provided [146, 147], and children with progressive disease need to be treated in intensive care and monitored for indications for surgery [145].
Antibiotic therapy
Standardized antibiotic therapy for NEC aims to provide a broad-spectrum combination of antibiotics targeting gram-negative, gram-positive, and anaerobic bacteria [141]. The collection of various body fluid samples (blood, oral swabs, stool, urine, ascites, or cerebrospinal fluid) for bacteriological culture is initiated at the Bell I stage. The most common bacteria in confirmed cases of NEC include Escherichia coli, Enterobacter, Klebsiella, and Coagulase-negative Staphylococci [146]. The classical antibiotic regimen combines gentamicin and ampicillin, in combination with metronidazole (Europe) or clindamycin (USA) for 10–14 days of treatment [128]. However, there are no prospective or randomized studies of the safety or efficacy of the latter two antibiotics, and there has been only one case report of intestinal stricture that occurred in a child following their use [148]. Other antibiotic regimens may be used to target specific bacteria or resistance, for example, vancomycin is used to treat increasingly common Coagulase-negative Staphylococci infections; third-generation cephalosporins may be added in the treatment of children with renal failure and severe NEC. The most recent recommendations from the Infectious Diseases Society of America (IDSA) and the Surgical Infection Society include one of the following regimens: ampicillin, gentamicin, and metronidazole; or ampicillin, cefotaxime, and metronidazole or meropenem. It is also recommended that 7–10 days of treatment after etiological control is achieved is sufficient [149, 150]. Considering the scope of the disease and the potential need for surgical intervention, neonatologists, infectious disease specialists, surgeons, and pharmacists should collaborate to develop antibiotic regimens for NEC. Antifungal and viral therapy for children with NEC should be individually designed [151].
Treatment of severe NEC
Controversies in the surgical treatment of severe NEC
For children with mild symptoms, conservative treatment can be used to alleviate the symptoms, while surgical management may be necessary for children with severe symptoms. Pneumoperitoneum and clinical deterioration remain the most common indications for operative treatment [152]. However, the criteria for determining surgical indications have not been fully unified, and different doctors may have different judgment results. In addition, there are certain controversies in terms of surgical timing, surgical methods, and postoperative care.
Surgery timing: The time to perform a surgical intervention in necrotizing enterocolitis remains a challenge for the pediatric surgeon. There is the article reporting that by comprehensively analyzing the risk factors of conservative treatment and surgical treatment through imaging findings to predict the timing of surgery, the results show that when ultrasound examination reveals thickening of the intestinal wall and poor peristalsis, early surgery is recommended [153]. There is the study applied multivariate logistic regression modeling to identify factors that could provide accurate risk of surgical NEC. Children requiring surgical treatment have presented an antecedent of respiratory distress (worsening of the ventilatory requirements) in the perinatal period, they present higher values of glycemia at diagnosis of the illness, debut with coagulopathy and have in laboratory findings marked neutrophilia [154]. The choice of surgical timing needs to be weighed and judged according to the specific situation of the child.
Surgical methods: Current surgical strategies for necrotizing enterocolitis (NEC) include primary drainage, resection with enterostomies, and primary anastomosis. The research shows, the postoperative outcomes in newborns undergoing laparotomy were associated with the surgical type, which was determined by disease location in the bowel [155]. There are also different practices in how to avoid damage to the intestinal wall and how to deal with residuals in the intestinal cavity during surgery. Necrotizing enterocolitis (NEC) often is associated with extensive bowel necrosis. These cases may require extensive enterectomy and the formation of high or multiple stomas, and frequently are complicated by short bowel syndrome, excessive fluid losses, fistulas, stenosis, and skin breakdown. A report describes a “clip and drop-back” technique, followed by delayed anastomosis performed 48–72 h later. The technique is a useful addition to the pediatric surgeon’s operative armamentarium in selective cases [156]. Some doctors advocate enteroplasty, and late abdominal resurgery was performed after necrotizing enterocolitis and spontaneous bowel perforation. Late abdominal reoperations occurred in 15% of patients with NEC with nil mortality [157].
Postoperative care: As for the specific measures of postoperative care, some doctors advocate giving patients antibiotics, nutritional support and other treatments. But unlike most surgical diseases, clear guidelines for the type and duration of peri-operative antibiotic therapy have not been established. There is a high degree of variability in the antibiotic regimen for the treatment of NEC, even within a single NICU, with no regimen appearing superior over another. This research highlights the need for guidelines in the antibiotic treatment of NEC and suggests that an abbreviated course of post-operative antibiotics may be safe [158]. Meanwhile, both physiological and psychological responses need to be understood in light of family centered care [159].
Nutritional management of short bowel syndrome (parenteral and enteral nutrition)
Short bowel syndrome (SBS) is the most serious complication in children with NEC. Prolonged ischemic necrosis of the intestine requires excessive resection to remove the necrotic tissue, leading to functional failure along with ultra-short length of the residual intestine and structural abnormalities [160]. Neonates who develop SBS require long-term PN support and are prone to nutritional deficiencies, leading to poor growth and development [17], and are at risk of developing neurodevelopmental disorders. Individualized treatment plans and surgical treatment with limited bowel resection are the basis for avoiding the eventual development of severe NEC into SBS [14]. The basic principle of providing optimal nutritional support for children is to stimulate the residual intestine as much as possible, while ensuring the energy needed for growth and maintaining the normal growth and function of the residual intestine. This requires a combination of PN and EN and the treatment plan needs to be frequently evaluated and revised to adapt to the growth and intestinal needs of the child, developing "intestinal rehabilitation" and rejecting intestinal transplantation [160].
Intervention studies for neurodevelopmental disorders
NEC is not only an intestinal disorder [161, 162], but also its broader sequelae include systemic inflammation, hypoxia, ischemia and, in severe cases, triggered multisystem organ dysfunction, particularly affecting brain and lung function [163]. NEC has been reviewed as an independent risk factor for neurodevelopmental delays and poor neurocognition in preterm infants [164,165,166]. Children exhibit neurological and motor dysplasia around 2 years of age, and cognitive deficits can persist into school age [164, 167, 168]. The pathogenesis might be related to the NEC-associated microbiome alterations to neurotransmitter levels in the brain development of affected children [169]. Murine models have demonstrated an irreversible increase in blood–brain barrier (BBB) permeability and barrier dysfunction caused by altered bacterial composition affecting tight junction proteins, resulting in reduced expression of short-chain fatty acids (SCFAs) in the brain [164]. Immune cells, such as microglia and astrocytes, maintain normal brain function; participate in synaptic pruning, formation and transmission; and regulate neurogenesis, neuronal migration, and synaptic plasticity [170]. As the severity of NEC disease increases, protective factors are exposed to an inflammatory environment and the disease progresses into surgical NEC [171]. Increased levels of pro-inflammatory factors [161] lead to poorer neurodevelopmental outcomes in affected children.
The TLR4 signaling pathway is now known to be involved in NEC-related encephalopathy [172]. In mouse models of NEC, TLR4 activation activates its endogenous ligand, high mobility base box 1 (HMGB1), and is released from the intestine, activating TLR4 on microglia, leading to reactive oxygen species (ROS) accumulation in the brain, oligodendrocyte progenitor cells (OPCs) loss, myelin disorders, and cognitive impairment. Anti-inflammatory and antioxidant treatments targeting microglia alleviate neurological dysfunction and thus represent new therapeutic targets for NEC-related brain injury. Recent studies have found that CD4+ T cells in the intestine of patients with NEC and NEC mice can infiltrate into the brain and secrete IFN-γ, which induces microglia activation and myelin loss, leading to brain injury, suggesting that early management of intestinal inflammation in children with NEC can improve the neurological prognosis of NEC [173].
Remission of pulmonary complications
Pulmonary injury, characterized by neutrophil infiltration and upregulation of inflammatory factors, occurs in approximately 15% of children with NEC. Recent studies on NEC-induced lung injury have revealed a TLR4-mediated pathogenesis similar to that of NEC-associated brain injury [174, 175]. TLR4 is highly expressed in the lung epithelium of NEC mice and can be activated by HMGB1 from the intestinal epithelium to upregulate C–X–C motif chemokine ligand 5 (CXCL5) recruitment of neutrophils. A novel TLR4 small molecule inhibitor, C34, reverses this inflammatory cascade and prevents NEC from triggering lung injury [174]. Th17 in NEC can drive cytokine upregulation and immune cell infiltration leading to inflammation and lung injury [176, 177]. Upregulation of the chemokine C–C motif chemokine ligand 25 (CCL25) mediates the development of inflammation, and TLR4 in the lung activates downstream CCL25 upregulation, causing protective T cell (regulatory T cells (Tregs)) depletion in the lung epithelium [175]. A recent study has shown that a "PDF system" (pre-digested fat system), in which a nutritional formula rich in pre-digested glycerol (without lipase action) was given in a mouse model. The PDF system, which affects lung maturation and reduces intrapulmonary ROS, protects against NEC-induced lung injury, and increases lung maturation in non-NEC mice, can significantly reduce the severity of NEC [178].
Conclusions
In this review, we have systematically described the possible pathogenesis of NEC in terms of epidemiology, risk factors, pathophysiology, clinical diagnosis, and manifestations. Intervention strategies to arrest the development of NEC have been slow to be perfected because of the complexity of its etiology and pathogenesis, and the diversity of its clinical manifestations. Therefore, we categorized and summarized the disease with respect to its multifaceted pathogenesis and clinical manifestations, with preventive tools including maternal health care to avoiding preterm birth, probiotic and breastfeeding for preterm infants (including donor breast milk) to avoid formula feeding, and targeting IL-10 and TLR4 and chondroitin sulfate to avoid infection and inflammation. We also have discussed new approaches to improve ischemia and reperfusion like RIC, and therapeutic measures for suspected NEC, such as NPO, early identification biomarkers, nutritional support, and exploration of new drug therapies. For moderate to severe NEC, not only the controversies in the surgical management have been discussed, but also new targets for treating complications have been identified after symptomatic and surgical treatment. We have talked about hot topics in NEC, such as the development of new scores and clinical scenarios. We also have described current interventions and management approaches, provided a more comprehensive review of current approaches for NEC prevention and treatment, thus deepening our understanding of intervention mechanisms. Considering the irreversible suffering caused by severe NEC in children and the poor long-term prognosis caused by surgical treatment, we should focus on providing guidance for better diagnosis and prevention of the disease before the onset and at the suspected stage of NEC. The current study offers the possibility of developing more adapted individualized prevention and treatment strategies in future.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author Yunyun Xu (Email: xyy0208@suda.edu.cn) upon reasonable request.
Abbreviations
- Apo-SAA:
-
Apolipoprotein-Serum Amyloid A
- BBB:
-
Blood–Brain Barrier
- CCL25:
-
C–C Motif Chemokine Ligand 25
- CDC:
-
Centers for Disease Control and Prevention
- COX-2:
-
Cyclooxygenase 2
- CRP:
-
C-Reactive Protein
- CS:
-
Chondroitin Sulfate
- CXCL5:
-
C–X–C Motif Chemokine Ligand 5
- DHA:
-
Dihydroxyacetone
- EGF:
-
Epidermal Growth Factor
- ELBWIs:
-
Extremely Low Birth Weight Infants
- FFT:
-
Fecal Filtrate Transplantation
- GLUT1:
-
Glucose Transporter 1
- GRP94:
-
Glucose-Regulated Protein 94
- HIF-1:
-
Hypoxia-Inducible Factor 1
- HMGB1:
-
High Mobility Base Box 1
- IAP:
-
Intestinal Alkaline Phosphatase
- IDSA:
-
Infectious Diseases Society of America
- IF:
-
Intestinal Failure
- I-FABP:
-
Intestinal Fatty Acid Binding Protein
- IL-10:
-
Interleukin 10
- INC:
-
International Neonatal Consortium
- LBW:
-
Low Birth Weight
- LBWIs:
-
Low Birth Weight Infants
- MUC2:
-
Mucin 2
- NDD:
-
Neurodevelopmental Disorders
- NEC:
-
Necrotizing Enterocolitis
- NIRS:
-
Near-Infrared Spectroscopy
- OPCs:
-
Oligodendrocyte Progenitor Cells
- PCT :
-
Procalcitonin
- PDF system:
-
Pre-Digested Fat System
- PGE2:
-
Prostaglandin E2
- PN:
-
Parenteral Nutrition
- PTGER4/EP4:
-
Prostaglandin E Receptor 4
- rintSO2:
-
Regional Intestinal Oxygen Saturation
- RIC :
-
Remote ischemic conditioning
- ROS:
-
Reactive Oxygen Species
- SBS:
-
Short Bowel Syndrome
- SCFAs:
-
Short-Chain Fatty Acids
- SFPs:
-
Standardized Feeding Protocols
- TLR4:
-
Toll-Like Receptor 4
- Tregs:
-
Regulatory T Cells
- UKNC-NEC:
-
UK Neonatal Collaborative NEC
- VLBWIs:
-
Very Low Birth Weight Infants
- VON:
-
Vermont Oxford Network
References
Holman RC, Stoll BJ, Curns AT, Yorita KL, Steiner CA, Schonberger LB (2006) Necrotising enterocolitis hospitalisations among neonates in the United States. Paediatr Perinat Epidemiol 20:498–506. https://doi.org/10.1111/j.1365-3016.2006.00756.x
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC et al (2010) Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 126:443–456. https://doi.org/10.1542/peds.2009-2959
Battersby C, Santhalingam T, Costeloe K, Modi N (2018) Incidence of neonatal necrotising enterocolitis in high-income countries: a systematic review. Arch Dis Child Fetal Neonatal Ed 103:F182–F189. https://doi.org/10.1136/archdischild-2017-313880
Jones IH, Hall NJ (2020) Contemporary outcomes for infants with necrotizing enterocolitis—a systematic review. J Pediatr 220:86-92.e3. https://doi.org/10.1016/j.jpeds.2019.11.011
Samuels N, van de Graaf RA, de Jonge RCJ, Reiss IKM, Vermeulen MJ (2017) Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr 17:105. https://doi.org/10.1186/s12887-017-0847-3
Filip R (2021) An update on the role of extracellular vesicles in the pathogenesis of necrotizing enterocolitis and inflammatory bowel diseases. Cells. https://doi.org/10.3390/cells10113202
Nino DF, Sodhi CP, Hackam DJ (2016) Necrotizing enterocolitis: new insights into pathogenesis and mechanisms. Nat Rev Gastroenterol Hepatol 13:590–600. https://doi.org/10.1038/nrgastro.2016.119
Eaton S, Rees CM, Hall NJ (2017) Current research on the epidemiology, pathogenesis, and management of necrotizing enterocolitis. Neonatology 111:423–430. https://doi.org/10.1159/000458462
Flahive C, Schlegel A, Mezoff EA (2020) Necrotizing enterocolitis: updates on morbidity and mortality outcomes. J Pediatr 220:7–9. https://doi.org/10.1016/j.jpeds.2019.12.035
Neu J, Walker WA (2011) Necrotizing enterocolitis. N Engl J Med 364:255–264. https://doi.org/10.1056/NEJMra1005408
Sharma R, Hudak ML (2013) A clinical perspective of necrotizing enterocolitis: past, present, and future. Clin Perinatol 40:27–51. https://doi.org/10.1016/j.clp.2012.12.012
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L et al (1978) Neonatal necrotizing enterocolitis. therapeutic decisions based upon clinical staging. Ann Surg 187:1–7. https://doi.org/10.1097/00000658-197801000-00001
Walsh MC, Kliegman RM (1986) Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am 33:179–201. https://doi.org/10.1016/s0031-3955(16)34975-6
Moschino L, Duci M, Fascetti Leon F, Bonadies L, Priante E, Baraldi E et al (2021) Optimizing nutritional strategies to prevent necrotizing enterocolitis and growth failure after bowel resection. Nutrients. https://doi.org/10.3390/nu13020340
Papillon S, Castle SL, Gayer CP, Ford HR (2013) Necrotizing enterocolitis: contemporary management and outcomes. Adv Pediatr 60:263–279. https://doi.org/10.1016/j.yapd.2013.04.011
Henry MC, Moss RL (2009) Necrotizing enterocolitis. Annu Rev Med 60:111–124. https://doi.org/10.1146/annurev.med.60.050207.092824
Sampah MES, Hackam DJ (2021) Prenatal immunity and influences on necrotizing enterocolitis and associated neonatal disorders. Front Immunol 12:650709. https://doi.org/10.3389/fimmu.2021.650709
Guthrie SO, Gordon PV, Thomas V, Thorp JA, Peabody J, Clark RH (2003) Necrotizing enterocolitis among neonates in the United States. J Perinatol 23:278–285. https://doi.org/10.1038/sj.jp.7210892
Frost BL, Modi BP, Jaksic T, Caplan MS (2017) New medical and surgical insights into neonatal necrotizing enterocolitis: a review. JAMA Pediatr 171:83–88. https://doi.org/10.1001/jamapediatrics.2016.2708
Guillet R, Stoll BJ, Cotten CM, Gantz M, McDonald S, Poole WK et al (2006) Association of H2-blocker therapy and higher incidence of necrotizing enterocolitis in very low birth weight infants. Pediatrics 117:e137–e142. https://doi.org/10.1542/peds.2005-1543
Schnabl KL, Van Aerde JE, Thomson AB, Clandinin MT (2008) Necrotizing enterocolitis: a multifactorial disease with no cure. World J Gastroenterol 14:2142–2161. https://doi.org/10.3748/wjg.14.2142
Challis P, Larsson L, Stoltz Sjostrom E, Serenius F, Domellof M, Elfvin A (2019) Validation of the diagnosis of necrotising enterocolitis in a Swedish population-based observational study. Acta Paediatr 108:835–841. https://doi.org/10.1111/apa.14585
Patel RM, Ferguson J, McElroy SJ, Khashu M, Caplan MS (2020) Defining necrotizing enterocolitis: current difficulties and future opportunities. Pediatr Res 88:10–15. https://doi.org/10.1038/s41390-020-1074-4
Horbar JD, Edwards EM, Greenberg LT, Morrow KA, Soll RF, Buus-Frank ME et al (2017) Variation in performance of neonatal intensive care units in the United States. JAMA Pediatr 171:e164396. https://doi.org/10.1001/jamapediatrics.2016.4396
Battersby C, Longford N, Costeloe K, Modi N, Group UKNCNES (2017) Development of a gestational age-specific case definition for neonatal necrotizing enterocolitis. JAMA Pediatr 171:256–263. https://doi.org/10.1001/jamapediatrics.2016.3633
Gordon PV, Swanson JR, MacQueen BC, Christensen RD (2017) A critical question for NEC researchers: can we create a consensus definition of NEC that facilitates research progress? Semin Perinatol 41:7–14. https://doi.org/10.1053/j.semperi.2016.09.013
Ji J, Ling XB, Zhao Y, Hu Z, Zheng X, Xu Z et al (2014) A data-driven algorithm integrating clinical and laboratory features for the diagnosis and prognosis of necrotizing enterocolitis. PLoS ONE 9:e89860. https://doi.org/10.1371/journal.pone.0089860
Caplan MS, Underwood MA, Modi N, Patel R, Gordon PV, Sylvester KG et al (2019) Necrotizing enterocolitis: using regulatory science and drug development to improve outcomes. J Pediatr 212(208–215):e1. https://doi.org/10.1016/j.jpeds.2019.05.032
Sabbatini S, Ganji N, Chusilp S, Balsamo F, Li B, Pierro A (2022) Intestinal atresia and necrotizing enterocolitis: embryology and anatomy. Semin Pediatr Surg 31:151234. https://doi.org/10.1016/j.sempedsurg.2022.151234
Scheese DJ, Sodhi CP, Hackam DJ (2023) New insights into the pathogenesis of necrotizing enterocolitis and the dawn of potential therapeutics. Semin Pediatr Surg 32:151309. https://doi.org/10.1016/j.sempedsurg.2023.151309
Lopez CM, Sampah MES, Duess JW, Ishiyama A, Ahmad R, Sodhi CP et al (2023) Models of necrotizing enterocolitis. Semin Perinatol 47:151695. https://doi.org/10.1016/j.semperi.2022.151695
Battarbee AN (2020) Use of antenatal corticosteroids in preterm prelabor rupture of membranes. Obstet Gynecol Clin North Am 47:587–594. https://doi.org/10.1016/j.ogc.2020.08.004
Crowley PA (1995) Antenatal corticosteroid therapy: a meta-analysis of the randomized trials, 1972 to 1994. Am J Obstet Gynecol 173:322–335. https://doi.org/10.1016/0002-9378(95)90222-8
Roberts D, Brown J, Medley N, Dalziel SR (2017) Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 3:CD004454. https://doi.org/10.1002/14651858.CD004454.pub3
Lundgren SN, Madan JC, Emond JA, Morrison HG, Christensen BC, Karagas MR et al (2018) Maternal diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner. Microbiome 6:109. https://doi.org/10.1186/s40168-018-0490-8
Watson SN, McElroy SJ (2021) Potential prenatal origins of necrotizing enterocolitis. Gastroenterol Clin N Am 50:431–444. https://doi.org/10.1016/j.gtc.2021.02.006
Seghesio E, De Geyter C, Vandenplas Y (2021) Probiotics in the prevention and treatment of necrotizing enterocolitis. Pediatr Gastroenterol Hepatol Nutr 24:245–255. https://doi.org/10.5223/pghn.2021.24.3.245
Sharif S, Meader N, Oddie SJ, Rojas-Reyes MX, McGuire W (2020) Probiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants. Cochrane Database Syst Rev 10:CD005496. https://doi.org/10.1002/14651858.CD005496.pub5
Adams M, Bassler D, Darlow BA, Lui K, Reichman B, Hakansson S et al (2019) Preventive strategies and factors associated with surgically treated necrotising enterocolitis in extremely preterm infants: an international unit survey linked with retrospective cohort data analysis. BMJ Open 9:e031086. https://doi.org/10.1136/bmjopen-2019-031086
Fleming P, Wilks M, Eaton S, Panton N, Hutchinson R, Akyempon A et al (2021) Bifidobacterium breve BBG-001 and intestinal barrier function in preterm babies: exploratory studies from the PiPS trial. Pediatr Res 89:1818–1824. https://doi.org/10.1038/s41390-020-01135-5
Jin YT, Duan Y, Deng XK, Lin J (2019) Prevention of necrotizing enterocolitis in premature infants - an updated review. World J Clin Pediatr 8:23–32. https://doi.org/10.5409/wjcp.v8.i2.23
Cristofalo EA, Schanler RJ, Blanco CL, Sullivan S, Trawoeger R, Kiechl-Kohlendorfer U et al (2013) Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J Pediatr 163(1592–1595):e1. https://doi.org/10.1016/j.jpeds.2013.07.011
Schanler RJ, Shulman RJ, Lau C (1999) Feeding strategies for premature infants: beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics 103:1150–1157. https://doi.org/10.1542/peds.103.6.1150
Sullivan S, Schanler RJ, Kim JH, Patel AL, Trawoger R, Kiechl-Kohlendorfer U et al (2010) An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products. J Pediatr 156:562–7.e1. https://doi.org/10.1016/j.jpeds.2009.10.040
Quigley M, Embleton ND, McGuire W (2018) Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev 6:CD002971. https://doi.org/10.1002/14651858.CD002971.pub4
Gephart SM, Hanson C, Wetzel CM, Fleiner M, Umberger E, Martin L et al (2017) NEC-zero recommendations from scoping review of evidence to prevent and foster timely recognition of necrotizing enterocolitis. Matern Health Neonatol Perinatol 3:23. https://doi.org/10.1186/s40748-017-0062-0
Section on B (2012) Breastfeeding and the use of human milk. Pediatrics 129:e827–41. https://doi.org/10.1542/peds.2011-3552
Oddie SJ, Young L, McGuire W (2021) Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst Rev 8:CD001241. https://doi.org/10.1002/14651858.CD001241.pub8
Christensen RD, Gordon PV, Besner GE (2010) Can we cut the incidence of necrotizing enterocolitis in half–today? Fetal Pediatr Pathol 29:185–198. https://doi.org/10.3109/15513815.2010.483874
Gephart SM, Hanson CK (2013) Preventing necrotizing enterocolitis with standardized feeding protocols: not only possible, but imperative. Adv Neonatal Care 13:48–54. https://doi.org/10.1097/ANC.0b013e31827ece0a
Emami CN, Chokshi N, Wang J, Hunter C, Guner Y, Goth K et al (2012) Role of interleukin-10 in the pathogenesis of necrotizing enterocolitis. Am J Surg 203:428–435. https://doi.org/10.1016/j.amjsurg.2011.08.016
Hackam DJ, Sodhi CP (2018) Toll-like receptor-mediated intestinal inflammatory imbalance in the pathogenesis of necrotizing enterocolitis. Cell Mol Gastroenterol Hepatol 6:229-238.e1. https://doi.org/10.1016/j.jcmgh.2018.04.001
Good M, Siggers RH, Sodhi CP, Afrazi A, Alkhudari F, Egan CE et al (2012) Amniotic fluid inhibits Toll-like receptor 4 signaling in the fetal and neonatal intestinal epithelium. Proc Natl Acad Sci USA 109:11330–11335. https://doi.org/10.1073/pnas.1200856109
Yazji I, Sodhi CP, Lee EK, Good M, Egan CE, Afrazi A et al (2013) Endothelial TLR4 activation impairs intestinal microcirculatory perfusion in necrotizing enterocolitis via eNOS-NO-nitrite signaling. Proc Natl Acad Sci USA 110:9451–9456. https://doi.org/10.1073/pnas.1219997110
Good M, Sodhi CP, Yamaguchi Y, Jia H, Lu P, Fulton WB et al (2016) The human milk oligosaccharide 2’-fucosyllactose attenuates the severity of experimental necrotising enterocolitis by enhancing mesenteric perfusion in the neonatal intestine. Br J Nutr 116:1175–1187. https://doi.org/10.1017/S0007114516002944
Knowles TA, Hosfield BD, Pecoraro AR, Li H, Shelley WC, Markel TA (2021) It’s all in the milk: chondroitin sulfate as potential preventative therapy for necrotizing enterocolitis. Pediatr Res 89:1373–1379. https://doi.org/10.1038/s41390-020-01125-7
Watkins DJ, Besner GE (2013) The role of the intestinal microcirculation in necrotizing enterocolitis. Semin Pediatr Surg 22:83–87. https://doi.org/10.1053/j.sempedsurg.2013.01.004
Ye C, Zhang Y, Ding X, Guo C (2021) High-mobility group box-1 is critical in the pathogenesis of mouse experimental necrotizing enterocolitis. J Interferon Cytokine Res 41:319–328. https://doi.org/10.1089/jir.2021.0056
Downard CD, Matheson PJ, Shepherd JA, Maki AC, Garrison RN (2012) Direct peritoneal resuscitation augments ileal blood flow in necrotizing enterocolitis via a novel mechanism. J Pediatr Surg 47:1128–1134. https://doi.org/10.1016/j.jpedsurg.2012.03.017
Maki AC, Matheson PJ, Shepherd JA, Garrison RN, Downard CD (2012) Intestinal microcirculatory flow alterations in necrotizing enterocolitis are improved by direct peritoneal resuscitation. Am Surg 78:803–807
Matheson PJ, Galganski LA, Garrison RN, Downard CD (2014) Application of prostaglandin E2 improves ileal blood flow in NEC. J Pediatr Surg 49:945–949. https://doi.org/10.1016/j.jpedsurg.2014.01.029. (discussion 949)
Walker SK, Matheson PJ, Schreiner MT, Smith JW, Garrison RN, Downard CD (2013) Intraperitoneal 1.5% Delflex improves intestinal blood flow in necrotizing enterocolitis. J Surg Res 184:358–364. https://doi.org/10.1016/j.jss.2013.04.007
Marin T, Josephson CD, Kosmetatos N, Higgins M, Moore JE (2014) Feeding preterm infants during red blood cell transfusion is associated with a decline in postprandial mesenteric oxygenation. J Pediatr 165(464–71):e1. https://doi.org/10.1016/j.jpeds.2014.05.009
Motta C, Scott W, Mahony L, Koch J, Wyckoff M, Reisch J et al (2015) The association of congenital heart disease with necrotizing enterocolitis in preterm infants: a birth cohort study. J Perinatol 35:949–953. https://doi.org/10.1038/jp.2015.96
Polycarpou E, Zachaki S, Tsolia M, Papaevangelou V, Polycarpou N, Briana DD et al (2013) Enteral L-arginine supplementation for prevention of necrotizing enterocolitis in very low birth weight neonates: a double-blind randomized pilot study of efficacy and safety. JPEN J Parenter Enteral Nutr 37:617–622. https://doi.org/10.1177/0148607112471561
Celik IH, Demirel G, Canpolat FE, Dilmen U (2013) Reduced plasma citrulline levels in low birth weight infants with necrotizing enterocolitis. J Clin Lab Anal 27:328–332. https://doi.org/10.1002/jcla.21607
Chen Y, Chang KT, Lian DW, Lu H, Roy S, Laksmi NK et al (2016) The role of ischemia in necrotizing enterocolitis. J Pediatr Surg 51:1255–1261. https://doi.org/10.1016/j.jpedsurg.2015.12.015
Ganji N, Biouss G, Sabbatini S, Li B, Lee C, Pierro A (2023) Remote ischemic conditioning in necrotizing enterocolitis. Semin Pediatr Surg 32:151312. https://doi.org/10.1016/j.sempedsurg.2023.151312
Ganji N, Li B, Ahmad I, Daneman A, Deshpande P, Dhar V et al (2022) Remote ischemic conditioning in necrotizing enterocolitis: study protocol of a multi-center phase II feasibility randomized controlled trial. Pediatr Surg Int 38:679–694. https://doi.org/10.1007/s00383-022-05095-1
Ou J, Courtney CM, Steinberger AE, Tecos ME, Warner BW (2020) Nutrition in necrotizing enterocolitis and following intestinal resection. Nutrients. https://doi.org/10.3390/nu12020520
Hock AM, Chen Y, Miyake H, Koike Y, Seo S, Pierro A (2018) Initiation of enteral feeding after necrotizing enterocolitis. Eur J Pediatr Surg 28:44–50. https://doi.org/10.1055/s-0037-1604436
Bohnhorst B, Muller S, Dordelmann M, Peter CS, Petersen C, Poets CF (2003) Early feeding after necrotizing enterocolitis in preterm infants. J Pediatr 143:484–487. https://doi.org/10.1067/S0022-3476(03)00443-8
Thuijls G, Derikx JP, van Wijck K, Zimmermann LJ, Degraeuwe PL, Mulder TL et al (2010) Non-invasive markers for early diagnosis and determination of the severity of necrotizing enterocolitis. Ann Surg 251:1174–1180. https://doi.org/10.1097/SLA.0b013e3181d778c4
Chaaban H, Shin M, Sirya E, Lim YP, Caplan M, Padbury JF (2010) Inter-alpha inhibitor protein level in neonates predicts necrotizing enterocolitis. J Pediatr 157:757–761. https://doi.org/10.1016/j.jpeds.2010.04.075
Aydemir O, Aydemir C, Sarikabadayi YU, Emre Canpolat F, Erdeve O, Biyikli Z et al (2012) Fecal calprotectin levels are increased in infants with necrotizing enterocolitis. J Matern Fetal Neonatal Med 25:2237–2241. https://doi.org/10.3109/14767058.2012.684172
Bin-Nun A, Booms C, Sabag N, Mevorach R, Algur N, Hammerman C (2015) Rapid fecal calprotectin (FC) analysis: point of care testing for diagnosing early necrotizing enterocolitis. Am J Perinatol 32:337–342. https://doi.org/10.1055/s-0034-1384640
Ahle M, Ringertz HG, Rubesova E (2018) The role of imaging in the management of necrotising enterocolitis: a multispecialist survey and a review of the literature. Eur Radiol 28:3621–3631. https://doi.org/10.1007/s00330-018-5362-x
Cortez J, Gupta M, Amaram A, Pizzino J, Sawhney M, Sood BG (2011) Noninvasive evaluation of splanchnic tissue oxygenation using near-infrared spectroscopy in preterm neonates. J Matern Fetal Neonatal Med 24:574–582. https://doi.org/10.3109/14767058.2010.511335
Tarracchini C, Milani C, Longhi G, Fontana F, Mancabelli L, Pintus R et al (2021) Unraveling the microbiome of necrotizing enterocolitis: insights in novel microbial and metabolomic biomarkers. Microbiol Spectr 9:e0117621. https://doi.org/10.1128/Spectrum.01176-21
Wu S, Di S, Liu T, Shi Y (2022) Emerging prediction methods for early diagnosis of necrotizing enterocolitis. Front Med 9:985219. https://doi.org/10.3389/fmed.2022.985219
Ng PC, Ma TP, Lam HS (2015) The use of laboratory biomarkers for surveillance, diagnosis and prediction of clinical outcomes in neonatal sepsis and necrotising enterocolitis. Arch Dis Child Fetal Neonatal Ed 100:F448–F452. https://doi.org/10.1136/archdischild-2014-307656
Reisinger KW, Van der Zee DC, Brouwers HA, Kramer BW, van Heurn LW, Buurman WA et al (2012) Noninvasive measurement of fecal calprotectin and serum amyloid A combined with intestinal fatty acid-binding protein in necrotizing enterocolitis. J Pediatr Surg 47:1640–1645. https://doi.org/10.1016/j.jpedsurg.2012.02.027
Kuik SJ, Kalteren WS, Mebius MJ, Bos AF, Hulscher JBF, Kooi EMW (2020) Predicting intestinal recovery after necrotizing enterocolitis in preterm infants. Pediatr Res 87:903–909. https://doi.org/10.1038/s41390-019-0634-y
Heath M, Buckley R, Gerber Z, Davis P, Linneman L, Gong Q et al (2019) Association of intestinal alkaline phosphatase with necrotizing enterocolitis among premature infants. JAMA Netw Open 2:e1914996. https://doi.org/10.1001/jamanetworkopen.2019.14996
Agakidou E, Agakidis C, Gika H, Sarafidis K (2020) Emerging biomarkers for prediction and early diagnosis of necrotizing enterocolitis in the era of metabolomics and proteomics. Front Pediatr 8:602255. https://doi.org/10.3389/fped.2020.602255
Wilcock A, Begley P, Stevens A, Whatmore A, Victor S (2016) The metabolomics of necrotising enterocolitis in preterm babies: an exploratory study. J Matern Fetal Neonatal Med 29:758–762. https://doi.org/10.3109/14767058.2015.1017462
Wandro S, Osborne S, Enriquez C, Bixby C, Arrieta A, Whiteson K (2018) The microbiome and metabolome of preterm infant stool are personalized and not driven by health outcomes, including necrotizing enterocolitis and late-onset sepsis. Sphere. https://doi.org/10.1128/mSphere.00104-18
Thomaidou A, Chatziioannou AC, Deda O, Benaki D, Gika H, Mikros E et al (2019) A pilot case-control study of urine metabolomics in preterm neonates with necrotizing enterocolitis. J Chromatogr B Analyt Technol Biomed Life Sci 1117:10–21. https://doi.org/10.1016/j.jchromb.2019.04.019
Sinclair TJ, Ye C, Chen Y, Zhang D, Li T, Ling XB et al (2020) Progressive metabolic dysfunction and nutritional variability precedes necrotizing enterocolitis. Nutrients. https://doi.org/10.3390/nu12051275
Sylvester KG, Ling XB, Liu GY, Kastenberg ZJ, Ji J, Hu Z et al (2014) Urine protein biomarkers for the diagnosis and prognosis of necrotizing enterocolitis in infants. J Pediatr 164(607–12):e1-7. https://doi.org/10.1016/j.jpeds.2013.10.091
Murgas Torrazza R, Li N, Young C, Kobeissy F, Chow M, Chen S et al (2013) Pilot study using proteomics to identify predictive biomarkers of necrotizing enterocolitis from buccal swabs in very low birth weight infants. Neonatology 104:234–242. https://doi.org/10.1159/000353721
Ng PC, Ang IL, Chiu RW, Li K, Lam HS, Wong RP et al (2010) Host-response biomarkers for diagnosis of late-onset septicemia and necrotizing enterocolitis in preterm infants. J Clin Invest 120:2989–3000. https://doi.org/10.1172/JCI40196
Jiang P, Smith B, Qvist N, Nielsen C, Wan JM, Sit WH et al (2013) Intestinal proteome changes during infant necrotizing enterocolitis. Pediatr Res 73:268–276. https://doi.org/10.1038/pr.2012.182
Sylvester KG, Ling XB, Liu GY, Kastenberg ZJ, Ji J, Hu Z et al (2014) A novel urine peptide biomarker-based algorithm for the prognosis of necrotising enterocolitis in human infants. Gut 63:1284–1292. https://doi.org/10.1136/gutjnl-2013-305130
Chatziioannou AC, Wolters JC, Sarafidis K, Thomaidou A, Agakidis C, Govorukhina N et al (2018) Targeted LC-MS/MS for the evaluation of proteomics biomarkers in the blood of neonates with necrotizing enterocolitis and late-onset sepsis. Anal Bioanal Chem 410:7163–7175. https://doi.org/10.1007/s00216-018-1320-3
Stewart CJ, Nelson A, Treumann A, Skeath T, Cummings SP, Embleton ND et al (2016) Metabolomic and proteomic analysis of serum from preterm infants with necrotising entercolitis and late-onset sepsis. Pediatr Res 79:425–431. https://doi.org/10.1038/pr.2015.235
Morrow AL, Lagomarcino AJ, Schibler KR, Taft DH, Yu Z, Wang B et al (2013) Early microbial and metabolomic signatures predict later onset of necrotizing enterocolitis in preterm infants. Microbiome 1:13. https://doi.org/10.1186/2049-2618-1-13
Stewart CJ, Embleton ND, Marrs EC, Smith DP, Nelson A, Abdulkadir B et al (2016) Temporal bacterial and metabolic development of the preterm gut reveals specific signatures in health and disease. Microbiome 4:67. https://doi.org/10.1186/s40168-016-0216-8
Morgan J, Bombell S, McGuire W (2013) Early trophic feeding versus enteral fasting for very preterm or very low birth weight infants. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD000504.pub4
Alshaikh B, Dharel D, Yusuf K, Singhal N (2021) Early total enteral feeding in stable preterm infants: a systematic review and meta-analysis. J Matern Fetal Neonatal Med 34:1479–1486. https://doi.org/10.1080/14767058.2019.1637848
Meinzen-Derr J, Poindexter B, Wrage L, Morrow AL, Stoll B, Donovan EF (2009) Role of human milk in extremely low birth weight infants’ risk of necrotizing enterocolitis or death. J Perinatol 29:57–62. https://doi.org/10.1038/jp.2008.117
Sisk PM, Lovelady CA, Dillard RG, Gruber KJ, O’Shea TM (2007) Early human milk feeding is associated with a lower risk of necrotizing enterocolitis in very low birth weight infants. J Perinatol 27:428–433. https://doi.org/10.1038/sj.jp.7211758
Lucas A, Cole TJ (1990) Breast milk and neonatal necrotising enterocolitis. Lancet 336:1519–1523. https://doi.org/10.1016/0140-6736(90)93304-8
Walsh V, McGuire W (2019) Immunonutrition for preterm infants. Neonatology 115:398–405. https://doi.org/10.1159/000497332
Gopalakrishna KP, Macadangdang BR, Rogers MB, Tometich JT, Firek BA, Baker R et al (2019) Maternal IgA protects against the development of necrotizing enterocolitis in preterm infants. Nat Med 25:1110–1115. https://doi.org/10.1038/s41591-019-0480-9
Good M, Sodhi CP, Egan CE, Afrazi A, Jia H, Yamaguchi Y et al (2015) Breast milk protects against the development of necrotizing enterocolitis through inhibition of Toll-like receptor 4 in the intestinal epithelium via activation of the epidermal growth factor receptor. Mucosal Immunol 8:1166–1179. https://doi.org/10.1038/mi.2015.30
Pisano C, Galley J, Elbahrawy M, Wang Y, Farrell A, Brigstock D et al (2020) Human breast milk-derived extracellular vesicles in the protection against experimental necrotizing enterocolitis. J Pediatr Surg 55:54–58. https://doi.org/10.1016/j.jpedsurg.2019.09.052
Miyake H, Lee C, Chusilp S, Bhalla M, Li B, Pitino M et al (2020) Human breast milk exosomes attenuate intestinal damage. Pediatr Surg Int 36:155–163. https://doi.org/10.1007/s00383-019-04599-7
Gao R, Zhang R, Qian T, Peng X, He W, Zheng S et al (2019) A comparison of exosomes derived from different periods breast milk on protecting against intestinal organoid injury. Pediatr Surg Int 35:1363–1368. https://doi.org/10.1007/s00383-019-04562-6
Wang X, Yan X, Zhang L, Cai J, Zhou Y, Liu H et al (2019) Identification and peptidomic profiling of exosomes in preterm human milk: insights into necrotizing enterocolitis prevention. Mol Nutr Food Res. https://doi.org/10.1002/mnfr.201801247
Martin C, Patel M, Williams S, Arora H, Brawner K, Sims B (2018) Human breast milk-derived exosomes attenuate cell death in intestinal epithelial cells. Innate Immun 24:278–284. https://doi.org/10.1177/1753425918785715
Dong P, Zhang Y, Yan DY, Wang Y, Xu X, Zhao YC et al (2020) Protective effects of human milk-derived exosomes on intestinal stem cells damaged by oxidative stress. Cell Transpl 29:963689720912690. https://doi.org/10.1177/0963689720912690
Schanler RJ, Lau C, Hurst NM, Smith EO (2005) Randomized trial of donor human milk versus preterm formula as substitutes for mothers’ own milk in the feeding of extremely premature infants. Pediatrics 116:400–406. https://doi.org/10.1542/peds.2004-1974
Boyd CA, Quigley MA, Brocklehurst P (2007) Donor breast milk versus infant formula for preterm infants: systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 92:F169–F175. https://doi.org/10.1136/adc.2005.089490
Quigley M, Embleton ND, McGuire W (2019) Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev 7:CD002971. https://doi.org/10.1002/14651858.CD002971.pub5
Chowning R, Radmacher P, Lewis S, Serke L, Pettit N, Adamkin DH (2016) A retrospective analysis of the effect of human milk on prevention of necrotizing enterocolitis and postnatal growth. J Perinatol 36:221–224. https://doi.org/10.1038/jp.2015.179
Chuang SL, Hayes PJ, Ogundipe E, Haddad M, MacDonald TT, Fell JM (2009) Cow’s milk protein-specific T-helper type I/II cytokine responses in infants with necrotizing enterocolitis. Pediatr Allergy Immunol 20:45–52. https://doi.org/10.1111/j.1399-3038.2008.00729.x
Li B, Hock A, Wu RY, Minich A, Botts SR, Lee C et al (2019) Bovine milk-derived exosomes enhance goblet cell activity and prevent the development of experimental necrotizing enterocolitis. PLoS ONE 14:e0211431. https://doi.org/10.1371/journal.pone.0211431
Neu J (2005) Neonatal necrotizing enterocolitis: an update. Acta Paediatr Suppl 94:100–105. https://doi.org/10.1111/j.1651-2227.2005.tb02163.x
Ibrahim HM, Jeroudi MA, Baier RJ, Dhanireddy R, Krouskop RW (2004) Aggressive early total parental nutrition in low-birth-weight infants. J Perinatol 24:482–486. https://doi.org/10.1038/sj.jp.7211114
Can E, Bulbul A, Uslu S, Comert S, Bolat F, Nuhoglu A (2012) Effects of aggressive parenteral nutrition on growth and clinical outcome in preterm infants. Pediatr Int 54:869–874. https://doi.org/10.1111/j.1442-200X.2012.03713.x
Akinkuotu AC, Nuthakki S, Sheikh F, Cruz SM, Welty SE, Olutoye OO (2015) The effect of supplemental parenteral nutrition on outcomes of necrotizing enterocolitis in premature, low birth weight neonates. Am J Surg 210:1045–1049. https://doi.org/10.1016/j.amjsurg.2015.08.004. (discussion 1049–1450)
Su Y, Yang J, Besner GE (2013) HB-EGF promotes intestinal restitution by affecting integrin-extracellular matrix interactions and intercellular adhesions. Growth Factors 31:39–55. https://doi.org/10.3109/08977194.2012.755966
Chen CL, Yu X, James IO, Zhang HY, Yang J, Radulescu A et al (2012) Heparin-binding EGF-like growth factor protects intestinal stem cells from injury in a rat model of necrotizing enterocolitis. Lab Invest 92:331–344. https://doi.org/10.1038/labinvest.2011.167
Yang J, Su Y, Zhou Y, Besner GE (2014) Heparin-binding EGF-like growth factor (HB-EGF) therapy for intestinal injury: Application and future prospects. Pathophysiology 21:95–104. https://doi.org/10.1016/j.pathophys.2013.11.008
Neal MD, Jia H, Eyer B, Good M, Guerriero CJ, Sodhi CP et al (2013) Discovery and validation of a new class of small molecule Toll-like receptor 4 (TLR4) inhibitors. PLoS ONE 8:e65779. https://doi.org/10.1371/journal.pone.0065779
Newburg DS (2009) Neonatal protection by an innate immune system of human milk consisting of oligosaccharides and glycans. J Anim Sci 87:26–34. https://doi.org/10.2527/jas.2008-1347
Jantscher-Krenn E, Zherebtsov M, Nissan C, Goth K, Guner YS, Naidu N et al (2012) The human milk oligosaccharide disialyllacto-N-tetraose prevents necrotising enterocolitis in neonatal rats. Gut 61:1417–1425. https://doi.org/10.1136/gutjnl-2011-301404
Jain SK, Baggerman EW, Mohankumar K, Namachivayam K, Jagadeeswaran R, Reyes VE et al (2014) Amniotic fluid-borne hepatocyte growth factor protects rat pups against experimental necrotizing enterocolitis. Am J Physiol Gastrointest Liver Physiol 306:G361–G369. https://doi.org/10.1152/ajpgi.00272.2013
Ostergaard MV, Bering SB, Jensen ML, Thymann T, Purup S, Diness M et al (2014) Modulation of intestinal inflammation by minimal enteral nutrition with amniotic fluid in preterm pigs. JPEN J Parenter Enteral Nutr 38:576–586. https://doi.org/10.1177/0148607113489313
Lu P, Sodhi CP, Jia H, Shaffiey S, Good M, Branca MF et al (2014) Animal models of gastrointestinal and liver diseases. Animal models of necrotizing enterocolitis: pathophysiology, translational relevance, and challenges. Am J Physiol Gastrointest Liver Physiol 306:G917–G928. https://doi.org/10.1152/ajpgi.00422.2013
Zeng R, Wang J, Zhuo Z, Luo Y, Sha W, Chen H (2021) Stem cells and exosomes: promising candidates for necrotizing enterocolitis therapy. Stem Cell Res Ther 12:323. https://doi.org/10.1186/s13287-021-02389-4
Dai L, Jie S, Bi S, Qing Q, Chen J, Le W (2021) Angiopoietin-2 silence alleviates lipopolysaccharide-induced inflammation, barrier dysfunction and endoplasmic reticulum stress of intestinal epithelial cells by blocking Notch signaling pathway. Bioengineered 12:8116–8124. https://doi.org/10.1080/21655979.2021.1985341
Kaminsky LW, Al-Sadi R, Ma TY (2021) IL-1beta and the intestinal epithelial tight junction barrier. Front Immunol 12:767456. https://doi.org/10.3389/fimmu.2021.767456
Sun L (2021) Low-dose cyclooxygenase-2 (COX-2) inhibitor celecoxib plays a protective role in the rat model of neonatal necrotizing enterocolitis. Bioengineered 12:7234–7245. https://doi.org/10.1080/21655979.2021.1980646
Sun Q, Ji YC, Wang ZL, She X, He Y, Ai Q et al (2021) Sodium butyrate alleviates intestinal inflammation in mice with necrotizing enterocolitis. Mediators Inflamm 2021:6259381. https://doi.org/10.1155/2021/6259381
Abou El Fadl DK, Ahmed MA, Aly YA, Darweesh EAG, Sabri NA (2021) Impact of Docosahexaenoic acid supplementation on proinflammatory cytokines release and the development of Necrotizing enterocolitis in preterm Neonates: a randomized controlled study. Saudi Pharm J 29:1314–1322. https://doi.org/10.1016/j.jsps.2021.09.012
Brunse A, Deng L, Pan X, Hui Y, Castro-Mejia JL, Kot W et al (2022) Fecal filtrate transplantation protects against necrotizing enterocolitis. ISME J 16:686–694. https://doi.org/10.1038/s41396-021-01107-5
Li B, Lee C, Cadete M, O’Connell JS, Alganabi M, Lee D et al (2022) Amniotic fluid stem cell administration can prevent epithelial injury from necrotizing enterocolitis. Pediatr Res 91:101–106. https://doi.org/10.1038/s41390-021-01657-6
Yarci E, Tayman C, Ozturk Yarci D, Cakir U, Gonel A, Taskin Turkmenoglu T (2021) Inhibition of Interleukin-6 signaling: a novel therapeutic approach to necrotizing enterocolitis. Int Immunopharmacol 101:108358. https://doi.org/10.1016/j.intimp.2021.108358
Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR et al (2007) Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol 196(147):e1-8. https://doi.org/10.1016/j.ajog.2006.09.014
Bell EF, Acarregui MJ (2001) Restricted versus liberal water intake for preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD000503
Stritzke AI, Smyth J, Synnes A, Lee SK, Shah PS (2013) Transfusion-associated necrotising enterocolitis in neonates. Arch Dis Child Fetal Neonatal Ed 98:F10–F14. https://doi.org/10.1136/fetalneonatal-2011-301282
Anand RJ, Leaphart CL, Mollen KP, Hackam DJ (2007) The role of the intestinal barrier in the pathogenesis of necrotizing enterocolitis. Shock 27:124–133. https://doi.org/10.1097/01.shk.0000239774.02904.65
Stoll BJ (1994) Epidemiology of necrotizing enterocolitis. Clin Perinatol 21:205–218
Lee JS, Polin RA (2003) Treatment and prevention of necrotizing enterocolitis. Semin Neonatol 8:449–459. https://doi.org/10.1016/S1084-2756(03)00123-4
Carter BM (2007) Treatment outcomes of necrotizing enterocolitis for preterm infants. J Obstet Gynecol Neonatal Nurs 36:377–384. https://doi.org/10.1111/j.1552-6909.2007.00157.x. (quiz 385)
Faix RG, Polley TZ, Grasela TH (1988) A randomized, controlled trial of parenteral clindamycin in neonatal necrotizing enterocolitis. J Pediatr 112:271–277. https://doi.org/10.1016/s0022-3476(88)80069-6
Mazuski JE, Tessier JM, May AK, Sawyer RG, Nadler EP, Rosengart MR et al (2017) The surgical infection society revised guidelines on the management of intra-abdominal infection. Surg Infect (Larchmt) 18:1–76. https://doi.org/10.1089/sur.2016.261
Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, Baron EJ et al (2010) Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis 50:133–164. https://doi.org/10.1086/649554
Katz S, Banerjee R, Schwenk H (2021) Antibiotic stewardship for the neonatologist and perinatologist. Clin Perinatol 48:379–391. https://doi.org/10.1016/j.clp.2021.03.009
Robinson JR, Rellinger EJ, Hatch LD, Weitkamp JH, Speck KE, Danko M et al (2017) Surgical necrotizing enterocolitis. Semin Perinatol 41:70–79. https://doi.org/10.1053/j.semperi.2016.09.020
Yu L, Liu C, Cui Y, Xue L, Ma L (2022) Imaging manifestations of neonatal necrotizing enterocolitis to predict timing of surgery. Turk J Pediatr 64:632–639. https://doi.org/10.24953/turkjped.2021.5048
Garcia Gonzalez M, Pertega S, Gonzalez C, Casal I (2023) Surgical treatment for necrotizing enterocolitis: a new score to extreme surveillance. Minerva Pediatr (Torino) 75:210–216. https://doi.org/10.23736/S2724-5276.19.05465-3
Geng Q, Wang Y, Li L, Guo C (2018) Early postoperative outcomes of surgery for intestinal perforation in NEC based on intestinal location of disease. Medicine (Baltimore) 97:e12234. https://doi.org/10.1097/MD.0000000000012234
Vaughan WG, Grosfeld JL, West K, Scherer LR, Villamizar E, Rescorla FJ (1996) Avoidance of stomas and delayed anastomosis for bowel necrosis: the “clip and drop-back” technique. J Pediatr Surg 31:542–545. https://doi.org/10.1016/s0022-3468(96)90492-3
Koivusalo A, Karila K, Pakarinen M (2021) Late abdominal reoperations after surgery for necrotizing enterocolitis and spontaneous intestinal perforation. Eur J Pediatr Surg 31:535–540. https://doi.org/10.1055/s-0040-1722616
Blackwood BP, Hunter CJ, Grabowski J (2017) Variability in antibiotic regimens for surgical necrotizing enterocolitis highlights the need for new guidelines. Surg Infect (Larchmt) 18:215–220. https://doi.org/10.1089/sur.2016.163
Hancock J (2000) Nursing the preterm surgical neonate. J Child Health Care 4:12–18. https://doi.org/10.1177/136749350000400102
Teresa C, Antonella D, de Ville GJ (2019) New nutritional and therapeutical strategies of NEC. Curr Pediatr Rev 15:92–105. https://doi.org/10.2174/1573396315666190313164753
Lodha A, Asztalos E, Moore AM (2010) Cytokine levels in neonatal necrotizing enterocolitis and long-term growth and neurodevelopment. Acta Paediatr 99:338–343. https://doi.org/10.1111/j.1651-2227.2009.01600.x
Wang FS, Yu ML, Li WZ, Hong K, Xu CB, Wang GH (2020) Intestinal tract and parenteral multi-organ sequential pathological injury caused by necrotizing enterocolitis. BMC Pediatr 20:418. https://doi.org/10.1186/s12887-020-02304-5
Cassir N, Simeoni U, La Scola B (2016) Gut microbiota and the pathogenesis of necrotizing enterocolitis in preterm neonates. Future Microbiol 11:273–292. https://doi.org/10.2217/fmb.15.136
Braniste V, Al-Asmakh M, Kowal C, Anuar F, Abbaspour A, Toth M et al (2014) The gut microbiota influences blood-brain barrier permeability in mice. Sci Transl Med 6:263ra158. https://doi.org/10.1126/scitranslmed.3009759
Schulzke SM, Deshpande GC, Patole SK (2007) Neurodevelopmental outcomes of very low-birth-weight infants with necrotizing enterocolitis: a systematic review of observational studies. Arch Pediatr Adolesc Med 161:583–590. https://doi.org/10.1001/archpedi.161.6.583
Rees CM, Pierro A, Eaton S (2007) Neurodevelopmental outcomes of neonates with medically and surgically treated necrotizing enterocolitis. Arch Dis Child Fetal Neonatal Ed 92:F193–F198. https://doi.org/10.1136/adc.2006.099929
Roze E, Ta BD, van der Ree MH, Tanis JC, van Braeckel KN, Hulscher JB et al (2011) Functional impairments at school age of children with necrotizing enterocolitis or spontaneous intestinal perforation. Pediatr Res 70:619–625. https://doi.org/10.1203/PDR.0b013e31823279b1
Humberg A, Spiegler J, Fortmann MI, Zemlin M, Marissen J, Swoboda I et al (2020) Surgical necrotizing enterocolitis but not spontaneous intestinal perforation is associated with adverse neurological outcome at school age. Sci Rep 10:2373. https://doi.org/10.1038/s41598-020-58761-6
Wikoff WR, Anfora AT, Liu J, Schultz PG, Lesley SA, Peters EC et al (2009) Metabolomics analysis reveals large effects of gut microflora on mammalian blood metabolites. Proc Natl Acad Sci USA 106:3698–3703. https://doi.org/10.1073/pnas.0812874106
Benarroch EE (2013) Microglia: multiple roles in surveillance, circuit shaping, and response to injury. Neurology 81:1079–1088. https://doi.org/10.1212/WNL.0b013e3182a4a577
Wadhawan R, Oh W, Hintz SR, Blakely ML, Das A, Bell EF et al (2014) Neurodevelopmental outcomes of extremely low birth weight infants with spontaneous intestinal perforation or surgical necrotizing enterocolitis. J Perinatol 34:64–70. https://doi.org/10.1038/jp.2013.128
Nino DF, Zhou Q, Yamaguchi Y, Martin LY, Wang S, Fulton WB et al (2018) Cognitive impairments induced by necrotizing enterocolitis can be prevented by inhibiting microglial activation in mouse brain. Sci Transl Med. https://doi.org/10.1126/scitranslmed.aan0237
Zhou Q, Nino DF, Yamaguchi Y, Wang S, Fulton WB, Jia H et al (2021) Necrotizing enterocolitis induces T lymphocyte-mediated injury in the developing mammalian brain. Sci Transl Med. https://doi.org/10.1126/scitranslmed.aay6621
Jia H, Sodhi CP, Yamaguchi Y, Lu P, Martin LY, Good M et al (2016) Pulmonary epithelial TLR4 activation leads to lung injury in neonatal necrotizing enterocolitis. J Immunol 197:859–871. https://doi.org/10.4049/jimmunol.1600618
Jia H, Sodhi CP, Yamaguchi Y, Lu P, Ladd MR, Werts A et al (2019) Toll like receptor 4 mediated lymphocyte imbalance induces Nec-induced lung injury. Shock 52:215–223. https://doi.org/10.1097/SHK.0000000000001255
Cho SX, Rudloff I, Lao JC, Pang MA, Goldberg R, Bui CB et al (2020) Characterization of the pathoimmunology of necrotizing enterocolitis reveals novel therapeutic opportunities. Nat Commun 11:5794. https://doi.org/10.1038/s41467-020-19400-w
Murdock BJ, Huffnagle GB, Olszewski MA, Osterholzer JJ (2014) Interleukin-17A enhances host defense against cryptococcal lung infection through effects mediated by leukocyte recruitment, activation, and gamma interferon production. Infect Immun 82:937–948. https://doi.org/10.1128/IAI.01477-13
Sodhi CP, Gonzalez Salazar AJ, Kovler ML, Fulton WB, Yamaguchi Y, Ishiyama A et al (2021) The administration of a pre-digested fat-enriched formula prevents necrotising enterocolitis-induced lung injury in mice. Br J Nutr. https://doi.org/10.1017/S0007114521004104
Funding
This work was supported by Suzhou Science and Technology Development Plan (SKY2022182, SKY2021051, SYS2020109), Boxi Culture Project of First Affiliated Hospital of Soochow University (BXQN202120). National Natural Science Foundation of China (Nos. 81701596, 81971423), Jiangsu Provincial Social Development Key General Project (BE2020658), Jiangsu Provincial Health and Family Planning Commission medical Research project (M2022102, ZD2021013), Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD), Suzhou Health Talent Training Project (GSWS2020048), Suzhou Health Young Backbone Talent "National Mentoring System" Training Program (Qngg2022013), Project of State Key Laboratory of Radiation Medicine and Protection, Soochow University (GZK1202107, GZK12023036).
Author information
Authors and Affiliations
Contributions
YYX and XPZ conceptualized the manuscript content. XHH and HSL performed the literature review, drafted the manuscript, and reviewed the final version. FL helped with manuscript writing. RZ and YBZ contributed to language editing or proofreading. XHH, HSL, FL, RZ, YBZ, XPZ, and YYX reviewed and edited the manuscript and approved the final product. All authors approved the final submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hu, X., Liang, H., Li, F. et al. Necrotizing enterocolitis: current understanding of the prevention and management. Pediatr Surg Int 40, 32 (2024). https://doi.org/10.1007/s00383-023-05619-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s00383-023-05619-3