
Abstract
Introduction
Reports vary on the impact of obesity on the incidence of lower extremity fractures after a fall. We hypothesized that obese adolescents (OA) presenting after a fall have a higher risk of any and severe lower extremity fractures compared to non-OAs.
Methods
A national database was queried for adolescents (12–17 years old) after a fall. Primary outcome included lower extremity fracture. Adolescents with a body mass index (BMI) ≥ 30 (OA) were compared to adolescents with a BMI < 30 (non-OA).
Results
From 20,264 falls, 2523 (12.5%) included OAs. Compared to non-OAs, the rate of any lower extremity fracture was higher for OAs (51.5% vs. 30.7%, p < 0.001). This remained true for lower extremity fractures at all locations (all p < 0.05). After adjusting for sex and age, associated risk for any lower extremity fracture (OR 2.41, CI 2.22–2.63, p < 0.001) and severe lower extremity fracture (OR 1.31, CI 1.15–1.49, p < 0.001) was higher for OAs. This remained true in subset analyses of ground level falls (GLF) and falls from height (FFH) (all p < 0.05).
Conclusions
Obesity significantly impacts adolescents’ risk of all types of lower extremity fractures after FFH or GLF. Hence, providers should have heightened awareness for possible lower extremity fractures in OAs.
Level of evidence
IV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the United States, childhood obesity is a growing epidemic with nearly 20% of children classified as obese based on body mass index (BMI) [1]. Furthermore, obese adolescents (OAs) have greater long-term risk of developing chronic diseases such as diabetes and cardiovascular disease, as well as increased risk of musculoskeletal injuries [2,3,4,5].
The impact of obesity on clinical outcomes and injury patterns in adult trauma patients has been well studied. Obesity has been linked with an increased risk of mortality, multisystem organ failure, acute renal failure, and increased intensive care unit (ICU) days following trauma [6,7,8,9]. While a linear association between higher BMI and increased risk of falling has been identified in adult patients, there are mixed reports about the impact of obesity on the incidence of extremity fractures [10]. There is even less known about adolescent trauma patients and obesity particularly after a fall.
While most ground level falls (GLFs) occur in the elderly [10, 11], adolescent patients can suffer injuries from GLFs or falls from height (FFH). In fact, previous studies have demonstrated that OAs, in comparison to non-obese adolescents (non-OAs), sustain more severe fractures, present with higher injury severity scores (ISS), and are at increased risk of death following all traumatic injuries in general [12,13,14,15,16]. Additionally, OAs have been demonstrated to have a significantly higher risk of lower extremity injuries than upper extremity injuries [17, 18]. However, there are no high-quality studies evaluating the risk of lower extremity fractures in OAs after a fall. Thus, we hypothesized that OAs presenting after a fall have a higher risk of any and severe lower extremity fractures compared to non-OAs. We also performed subset analyses for adolescents presenting after a GLF and FFH.
Methods
This study was deemed exempt, and a waiver of consent was granted for use of a de-identified national database. We utilized the Trauma Quality Improvement Program (TQIP) database, a quality improvement initiative incorporating data submitted by participating trauma centers across the United States [19]. The TQIP database was queried from 2017 to 2019 to identify adolescents (12–17-years-old) presenting after any fall (GLF or FFH). All trauma mechanisms in TQIP are defined by a corresponding event code (e-code). GLF was defined by any event code which indicated “Fall on same level” while FFH was defined by e-codes indicating “Fall from height.” We excluded all patients with missing data regarding height and weight. Two groups were compared: OAs with a BMI ≥ 30 kg/m2 and non-OAs with a BMI < 30 kg/m2. Patient demographic information was collected along with vitals on admission. Pre-hospital comorbidities included attention deficit/hyperactivity disorder (ADHD), diabetes mellitus, hypertension, smoking status, and substance abuse. The injury profile included ISS, fractures of the head, spine, ribs, upper extremity, pelvis, and lower extremity as well as solid organ injuries (i.e. kidney, liver, spleen).
The primary outcome was a lower extremity fracture. A severe fracture was defined by abbreviated injury scale (AIS) grade ≥ 3. Lower extremity fractures were further categorized based on location including fracture of the femur, knee, tibia, fibula, ankle, and foot. We performed subset analyses on patients presenting after a GLF and FFH. Other measured outcomes included the total hospital length of stay (LOS), ICU LOS, ventilator days, and mortality. Additionally, inpatient complications analyzed included deep vein thrombosis (DVT), unplanned intubation, acute kidney injury (AKI), and ventilator acquired pneumonia (VAP).
A Mann–Whitney U test was used to compare continuous variables and chi-square to compare categorical variables. Categorical data was reported as percentages and continuous data was reported as medians with interquartile range or as means with standard deviation. A multivariable logistic regression model was then used for further analysis controlling for variables including age and sex. These variables were chosen based on author consensus as they are characteristics that can be identified in the pre-hospital setting and are associated with differences in bone mineral density, bone size and bone accrual as influenced by hormonal effects on bone metabolism [4] and thus may affect rates of lower extremity fractures. The adjusted risk for lower extremity fractures was reported with odds ratios (OR) and 95% confidence intervals (CI). All p-values were two-sided with a statistical significance level of < 0.05. All analyses were performed with IBM SPSS Statistics for Windows (Version 28, IBM Corp., Armonk, NY).
Results
Demographics of adolescent patients presenting following a fall
From 20,264 adolescent falls, 2,523 (12.5%) included OAs. The median BMI was 34 kg/m2 in the OA group versus 21 kg/m2 in the non-OA group (p < 0.001). On presentation, the OA group had higher rates of diabetes (1.4% vs. 0.5%, p < 0.001), hypertension (0.9% vs. 0.2%, p < 0.001), and mental/personality disorders (6.0% vs. 3.6%, p < 0.001). However, OAs had a lower incidence of severe trauma (ISS > 15) (4.9% vs. 6.8%, p < 0.001) (Table 1).
Types of injuries sustained as a result of a fall in non-OAs vs. OAs
OAs had a higher rate of lower extremity fractures (51.5% vs. 30.7%, p < 0.001) and severe lower extremity fractures (12.7% vs. 10.1%, p < 0.001) compared to non-OAs. This injury association remained true in all lower extremity fracture locations: femur (9.6% vs. 8.4%, p = 0.047), knee (1.0% vs. 0.5%, p = 0.002), tibia (31.3% vs. 18.4%, p < 0.001), fibula (16.1% vs. 9.2%, p < 0.001), ankle (9.0% vs. 2.8%, p < 0.001), and foot (2.6% vs. 1.8%, p = 0.01). In a subset analysis of GLFs, OAs continued to have a higher rate of lower extremity fractures (55.4% vs. 33.8%, p < 0.001) and severe lower extremity fractures (13.7% vs. 9.9%, p < 0.001) compared to non-OAs, with similarly increased rates at all lower extremity fracture locations: femur (12.1% vs. 8.9%, p < 0.001), knee (1.2% vs. 0.6%, p = 0.02), tibia (33.9% vs. 21.6%, p < 0.001), fibula (14.2% vs. 9.3%, p < 0.001), ankle (7.4% vs. 2.5%, p < 0.001), and foot (1.4% vs. 0.7%, p = 0.02). Furthermore, in a subset analysis of FFH, OAs had a higher rate of lower extremity fractures (46% vs. 26.4%, p < 0.001) and severe lower extremity fractures (13.2% vs. 8.6%, p < 0.001), with similarly increased rates at all lower extremity fracture locations: femur (7.6% vs. 6.3%, p = 0.18), knee (1.1% vs. 0.5%, p = 0.03), tibia (27.2% vs. 15%, p < 0.001), fibula (16.5% vs. 9%, p < 0.001), ankle (9.9% vs. 3.1%, p < 0.001), and foot (4.4% vs. 3.3%, p = 0.1) (Table 2). Compared to non-OAs, OAs suffered lower rates of solid organ injuries: spleen (1.0% vs. 2.8%, p < 0.001), lung (1.7% vs. 3.4%, p < 0.001), liver (0.8% vs. 1.3%, p = 0.02), and kidney (0.8% vs. 1.9%, p < 0.001) (Table 3).
Other measured outcomes of non-OAs vs. OAs following a fall
OAs had increased mean hospital LOS (3.19 days vs. 2.93 days, p < 0.001) and ICU LOS (4.10 days vs. 3.22 days, p = 0.03), as well a higher rate of VAP (0.1% vs. 0%, p = 0.02). The risk of all other measured in-hospital complications including mortality (p = 0.45) was similar between the two groups (Table 4).
Lower extremity fracture risk factors in adolescent patients
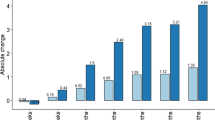
After adjusting for age and sex, OAs had an increased associated risk of any lower extremity fracture (OR 2.41, CI 2.22–2.63, p < 0.001) and severe lower extremity fracture (OR 1.31, CI 1.15–1.49, p < 0.001), compared to non-OAs. These findings remained true in subset analyses of GLFs and FFH: FFH lower extremity fracture (OR 2.39, CI 2.05–2.79, p < 0.001), FFH severe lower extremity fracture (OR 1.66, CI 1.32–2.09, p < 0.001), GLF lower extremity fracture (OR 2.44, CI 2.14–2.77, p < 0.001), GLF severe lower extremity fracture (OR 1.46, CI 1.21–1.76, p < 0.001) (Table 5).
Discussion
Adolescent obesity is a growing epidemic with a continued expected high occurrence of falls in this age group. While there is existing literature on the effects of obesity on risk of fracture in both adult and pediatric trauma patients, to our knowledge, this is the first study evaluating the effects of obesity on the risk of lower extremity fractures in adolescent fall patients. This national analysis demonstrated that despite having a lower rate of severe trauma, OAs presenting after a GLF or FFH had an increased associated risk of lower extremity fractures and severe lower extremity fractures, compared to non-OAs. Additionally, OAs had a lower rate of solid organ injuries after a fall suggesting that obesity may serve as a protective factor for these types of injuries.
Obesity significantly impacts the risk of lower extremity fractures in adolescents following all falls. McGregor et al. demonstrated that obese children are two times more likely to have low energy mechanisms of tibia fracture, such as from a GLF, compared to non-obese children [1]. Similarly, our study’s subgroup analysis found OAs have a twofold increased risk of lower extremity fracture for GLFs and FFH, implicating obesity as a potential risk factor for lower extremity fracture regardless of mechanism of fall. Furthermore, we found that the fracture risk is ubiquitous across the lower extremity, occurring at the femur, knee, tibia, fibula, ankle, or foot. This finding is consistent with previous literature analyzing all trauma mechanisms and demonstrating a stepwise increased risk of fractures in the foot, ankle, leg, and knee with increasing BMI most pronounced in children 6–11 years old [20]. This increased risk for OAs extends beyond lower extremity fractures to other extremity injuries such as sprains/strains and dislocations [20]. We did note that the most significant differences between OAs and non-OAs occurred below the knee with OAs having a significantly higher rate of fractures to the tibia, fibula, and ankle. Several potential mechanisms could explain this observation. Firstly, the increased weight borne by the lower extremities in OAs can lead to greater mechanical stresses, making the bones more susceptible to injury even from minor trauma. This is particularly relevant for weight-bearing bones like the tibia and fibula, which are situated below the knee. Secondly, OAs often have altered biomechanics due to their increased body mass, including changes in gait and balance. These changes can increase the risk of falls and subsequent fractures. In particular, falls that are “off-axis” or at an unusual angle may be more common in this population, leading to more injuries below the knee.
Increased risk of injury may be attributed to numerous biomechanical factors related to weight distribution and alignment in the lower extremity affecting balance and ultimately contributing to negative outcomes following a fall [21]. Obese patients demonstrate altered kinetic characteristics of locomotion that can lead to poor intrinsic coordination and falling in a suboptimal position [22,23,24]. Additionally, previous studies have demonstrated that OAs fall with greater force from equal heights when compared to non-OAs [12]. Weight is directly proportional to energy transfer and momentum accounting for increased severity and likelihood of fracture for all falls regardless of height in OAs [12, 25]. Ultimately obesity proves deleterious to the outcomes of adolescents as obesity is associated with a greater risk of all types of lower extremity fractures regardless of whether the fall was from ground level or FFH.
Metabolic differences in OAs may contribute to a higher risk of lower extremity fracture. Studies have shown obesity to have a negative effect on attaining peak bone mass in adolescents due to the alteration of bone metabolism during this period of rapid skeletal growth [26, 27]. Obesity has been demonstrated in animal and cellular models to promote low grade inflammation. Inflammation in turn contributes to rearrangement of bone microarchitecture through bone reabsorption by reduced osteoblast and enhanced osteoclast activity. This results in increased cortical porosity and decreased trabecular thickness potentially increasing the bone’s susceptibility to fracture [14, 28, 29]. The nonspecific effect of obesity on bone, therefore contributes to greater incidence of fracture in OAs at all lower extremity locations. Ultimately, mechanical disadvantages and compromised bone microarchitecture combined may contribute to increased lower extremity fracture risk of OAs during GLFs and FFH.
In our study, we observed a small but noteworthy difference in age between obese and non-obese adolescents. This raises interesting questions about the interplay between age and obesity during adolescence, a critical period of physical growth and development. One potential explanation for this difference could be related to the onset of puberty, which varies widely and can significantly affect growth patterns and body composition. It is also important to consider lifestyle factors that change as children age. Older adolescents might be more independent in their food choices and potentially more sedentary due to increased academic pressure and decreased physical education opportunities, which might contribute to weight gain.
While obesity may be deleterious, there have been multiple studies that suggest obesity as providing an armor or shielding effect from injury [25, 30,31,32]. Obesity has been shown to decrease peak force of impact and increase tissue energy absorption due to increased soft tissue thickness [30]. As such, this study found that in contrast to extremity injuries, OAs had a lower rate of solid organ injuries after a fall, compared to non-OAs. With adipose tissue often localized to the abdomen in OAs, the cushion effect may not prove helpful in providing protection against extremity fractures.
As a national retrospective database study, there are inherent limitations including reporting bias, coding errors, and missing data. In addition, causation cannot be established. Also, information regarding adolescents’ level of physical activity, nutritional status, and bone density are not available in TQIP. There also exist limitations inherent to BMI as a tool for determining obesity status as BMI only takes into account weight and height, barring distinction between body fat and muscle content. Likewise, information regarding the body composition of adolescents is lacking as BMI does not provide any relevant indication of an individual’s fat distribution which may have effects on forces generated during a fall. Additionally, the circumstances preceding and ultimately causing the fall remain unknown precluding analysis of the increased risk of weight based victimization that OAs face and its effects on fracture risk [33]. Finally, TQIP is confined to index hospitalization data, thus we cannot make any statements regarding the long term outcomes of fractures in OAs.
Conclusion
In conclusion, the influence of obesity on fracture patterns is important to understand given the increasing prevalence of obesity in adolescents. Furthermore, obese adolescents had an increased risk of all types of lower extremity fractures after both ground level falls and falls from height compared to non-obese adolescents. On the other hand, obese adolescents had a lower rate of solid organ injuries after a fall. Based on these findings, trauma providers should have increased vigilance in evaluating for lower extremity fractures in obese adolescents.
References
McGregor PC, Lyons MM, Wozniak A et al (2022) The effect of obesity on pediatric tibia fractures. Iowa Orthop J 42:41–46
Donati F, Costici PF, De Salvatore S et al (2020) A perspective on management of limb fractures in obese children: is it time for dedicated guidelines? Front Pediatr 8:207. https://doi.org/10.3389/fped.2020.00207
Li NY, Kalagara S, Hersey A et al (2019) Impact of obesity on operative treatment and inpatient outcomes of paediatric limb fractures. Bone Joint J 101:491–496. https://doi.org/10.1302/0301-620X.101B4.BJJ-2018-0740.R2
Goulding A (2007) Risk factors for fractures in normally active children and adolescents. Med Sport Sci 51:102–120. https://doi.org/10.1159/000103007
Patil MS, Baseer H (2017) Obesity and fracture healing. Al Ameen J Med Sci 10:107–111
Brahmbhatt TS, Hernon M, Siegert CJ et al (2017) Trauma and BMI mortality. Curr Obes Rep 6:211–216. https://doi.org/10.1007/s13679-017-0264-9
Tay-Lasso E, Grigorian A, Lekawa M et al (2022) Obesity does not increase risk for mortality in severe sepsis trauma patients. Am Surg. https://doi.org/10.1177/00031348221078986. (Published online ahead of print)
Covarrubias J, Grigorian A, Schubl S et al (2021) Obesity associated with increased postoperative pulmonary complications and mortality after trauma laparotomy. Eur J Trauma Emerg Surg 47:1561–1568. https://doi.org/10.1007/s00068-020-01329-w
Farhat A, Grigorian A, Nguyen NT et al (2020) Obese trauma patients have increased need for dialysis. Eur J Trauma Emerg Surg 46:1327–1334. https://doi.org/10.1007/s00068-019-01147-9
Himes CL, Reynolds SL (2012) Effect of obesity on falls, injury, and disability. J Am Geriatr Soc 60:124–129. https://doi.org/10.1111/j.1532-5415.2011.03767.x
Chang MC (2016) National Trauma Databank 2016 Annual Report. Committee on Trauma, American College of Surgeons, Chicago
Nhan DT, Leet AI, Lee RJ (2021) Associations of childhood overweight and obesity with upper-extremity fracture characteristics. Med Baltimore 100:18. https://doi.org/10.1097/MD.0000000000025302
Ashley P, Gilbert SR (2018) Obesity in pediatric trauma. Orthop Clin North Am 49:335–343. https://doi.org/10.1016/j.ocl.2018.02.007
Fintini D, Cianfarani S, Cofini M et al (2020) The bones of children with obesity. Front Endocrinol (Lausanne) 11:200. https://doi.org/10.3389/fendo.2020.00200
Fornari ED, Suszter M, Roocroft J et al (2013) Childhood obesity as a risk factor for lateral condyle fractures over supracondylar humerus fractures. Clin Orthop Relat Res 471:1193–1198. https://doi.org/10.1007/s11999-012-2566-2
Kim SJ, Ahn J, Kim HK et al (2016) Obese children experience more extremity fractures than nonobese children and are significantly more likely to die from traumatic injuries. Acta Paediatr 105:1152–1157. https://doi.org/10.1111/apa.13343
Pomerantz WJ, Timm NL, Gittelman MA (2010) Injury patterns in obese versus nonobese children presenting to a pediatric emergency department. Pediatrics 125:681–685. https://doi.org/10.1542/peds.2009-2367
Kessler J, Koebnick C, Smitt N et al (2013) Childhood obesity is associated with increased risk of most lower extremity fractures. Clin Orthop Relat Res 471:1199–1207. https://doi.org/10.1007/s11999-012-2621-z
Shafi S, Nathens AB, Cryer GH et al (2009) The trauma quality improvement program of the american college of surgeons committee on trauma. J Am Coll Surg 209:521–530. https://doi.org/10.1016/j.jamcollsurg.2009.07.001
Adams AL, Kessler JI, Deramerian K et al (2013) Associations between childhood obesity and upper and lower extremity injuries. Inj Prev 19:191–197. https://doi.org/10.1136/injuryprev-2012-040341
Shultz SP, Anner J, Hills AP (2009) Paediatric obesity, physical activity and the musculoskeletal system. Obes Rev 10:576–582. https://doi.org/10.1111/j.1467-789X.2009.00587.x
Valerio G, Gallè F, Mancusi C et al (2012) Prevalence of overweight in children with bone fractures: a case control study. BMC Pediatr 12:166. https://doi.org/10.1186/1471-2431-12-166
Nantel J, Brochu M, Prince F (2006) Locomotor strategies in obese and non-obese children. Obesity 14:1789–1794. https://doi.org/10.1038/oby.2006.206
Goulding A, Jones IE, Taylor RW et al (2003) Dynamic and static tests of balance and postural sway in boys: effects of previous wrist bone fractures and high adiposity. Gait Posture 17:136–141. https://doi.org/10.1016/s0966-6362(02)00161-3
Arbabi S, Wahl WL, Hemmila MR et al (2003) The cushion effect. J Trauma 54:1090–1093. https://doi.org/10.1097/01.TA.0000064449.11809.48
Tisano B, Anigian K, Kantorek N et al (2022) The insidious effects of childhood obesity on orthopedic injuries and deformities. Orthop Clin North Am 53:461–472. https://doi.org/10.1016/j.ocl.2022.06.008
Dimitri P, Bishop N, Walsh et al (2012) Obesity is a risk factor for fracture in children but is protective against fracture in adults: a paradox. Bone 50:457–466. https://doi.org/10.1016/j.bone.2011.05.011
Cao JJ (2011) Effects of obesity on bone metabolism. J Orthop Surg Res 6:30. https://doi.org/10.1186/1749-799X-6-30
Roy B, Curtis ME, Fears LS et al (2016) Molecular mechanisms of obesity-induced osteoporosis and muscle atrophy. Front Physiol 7:439. https://doi.org/10.3389/fphys.2016.00439
Liu Q, Wu M, Orgill DP et al (2022) Effect of obesity on inpatient outcomes in lower extremity trauma: a systematic review and meta-analysis. J Trauma Acute Care Surg 92:464–470. https://doi.org/10.1097/TA.0000000000003328
Modig K, Erdefelt A, Mellner C et al (2019) Obesity paradox” holds true for patients with hip fracture: a registry-based cohort study. J Bone Joint Surg Am 101:888–895. https://doi.org/10.2106/JBJS.18.01249
Dvorak JE, Lester EL, Maluso PJ et al (2020) The obesity paradox in the trauma patient: normal may not be better. World J Surg 44:1817–1823. https://doi.org/10.1007/s00268-020-05398-1
Bacchini D, Licenziati MR, Garrasi A et al (2015) Bullying and victimization in overweight and obese outpatient children and adolescents: an italian multicentric study. PLoS One 10(11):e0142715. https://doi.org/10.1371/journal.pone.0142715
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by NG and AG. The first draft of the manuscript was written by NG and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Informed consent
A waiver of consent was granted for use of a de-identified national database.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gonzalez, N., Nahmias, J., Schubl, S. et al. Obese adolescents have higher risk for severe lower extremity fractures after falling. Pediatr Surg Int 39, 235 (2023). https://doi.org/10.1007/s00383-023-05524-9
Accepted:
Published:
DOI: https://doi.org/10.1007/s00383-023-05524-9