
Abstract
Background and aim
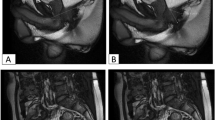
Paediatric rectal prolapse (RP) is rarely a diagnostic problem and resolves often spontaneously. We studied whether the assessment of recurrent RP (RP), postoperative relapsed RP (RRP) or anorectal discomfort without RP (ARD) benefits from dynamic defecography (DD) and describe DD findings in relation with outcome.
Patients and methods
Fifteen patients (7 males), median age of 10 (range 3.7–15) years, underwent 19 DD with a synchronic small bowel contrast study. Indications for DD were RP (n = 11), RD (n = 3) and RRP (n = 1). Three patients had solitary rectal ulcer and one juvenile rectal polyps (n = 1). Three patients underwent a total of four postoperative DD because of suspected relapse.
Results
In 11 patients with a clinically diagnosed prolapse DD displayed a simple prolapse (n = 3), prolapse with enterocele (n = 1), prolapse with small bowel interposition (n = 1), rectal intussusception with anterior rectocele (n = 1) and rectal intussusception (n = 1) and no pathology (n = 4) (37 %). In four patients with ARD DD displayed rectal prolapse originating from sigmoid intussusception (n = 1), enterocele (n = 1) and anterior rectocele (n = 1) and no pathology in one. Median follow-up was 8.1(range 3.0–44) months. Ten patients underwent surgery. Three patients with RP underwent simple laparoscopic rectopexy, five with RP or RD with enterocele or anterior rectocele had rectopexy with anterior peritoneoplasty and two (RP n = 1, RRP n = 1) with sigmoid intussusception had sigmoid resection with rectopexy. Two symptomatic patients (RP, negative DD) are scheduled for rectopexy. Three patients PPRP (n = 2) RD (n = 1) had spontaneous cure. Postoperative DD confirmed relapsed RP in one patient.
Conclusion
In patients, RP and associated disorders’ DD can disclose significant pathology (enterocele, rectocele or sigmoid intussusception) and thereby guide surgical treatment, and should be included in the pre-treatment assessment.



Similar content being viewed by others


References
Rintala RJ, Pakarinen MP (2012) Other disorders of the anus and the rectum, anorectal function, chapter 104. In: Coran AG, Adzick NS, Krummel T, Laberge J-M, Shamberger RC, Caldamone AA (eds) Pediatric surgery, vol 2, 7th edn. Elsevier Saunders, Philadelphia, pp 1316–1318
Mellgren A, Bremmer S, Johansson C, Dolk A, Udén R, Ahlbäck SO, Holmström B (1994) Defecography. Results of investigations in 2,816 patients. Dis Colon Rectum 37:1133–1141
Suzuki H, Amano S, Matsumoto K, Tsukamoto Y (1989) Anorectal motility in children with complete rectal prolapse. Prog Pediatr Surg 24:105–114
Hussain SZ, Dunn GD, Brown MF, Osman M (2010) Rectocele in children: a case report. J Pediatr Surg 45:e35–e38
Lesher AP, Hill JG, Schabel SI, Morgan KA, Hebra A (2010) An unusual pediatric case of chronic constipation and rectosigmoid prolapse diagnosed by video defecography. J Pediatr Surg 45:1050–1052
Ismail M, Gabr K, Shalaby R (2010) Laparoscopic management of persistent complete rectal prolapse in children. J Pediatr Surg 45:533–539
Laituri CA, Garey CL, Fraser JD, Aguayo P, Ostlie DJ, St Peter SD, Snyder CL (2010) 15-Year experience in the treatment of rectal prolapse in children. J Pediatr Surg 45:1607–1609
Potter DD, Bruny JL, Allshouse MJ, Narkewicz MR, Soden JS, Partrick DA (2010) Laparoscopic suture rectopexy for full-thickness anorectal prolapse in children: an effective outpatient procedure. J Pediatr Surg 45:2103–2107
Antao B, Bradley V, Roberts JP, Shawis R (2005) Management of rectal prolapse in children. Dis Colon Rectum 48:1620–1625
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koivusalo, A.I., Pakarinen, M.P., Rintala, R.I. et al. Dynamic defecography in the diagnosis of paediatric rectal prolapse and related disorders. Pediatr Surg Int 28, 815–820 (2012). https://doi.org/10.1007/s00383-012-3125-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-012-3125-3