
Abstract
Purpose
H-type anorectal malformations (ARM) are extremely rare in males. Herein, we have described our experience of managing this variety.
Methods
From September 1993 to February 2009, seven boys with H-type ARM were managed in the Department of Pediatric Surgery, Chittagong Medical College and Hospital, Chittagong, Bangladesh. Clinical features, operative procedures and outcomes were analyzed.
Results
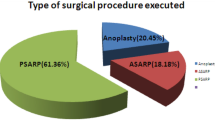
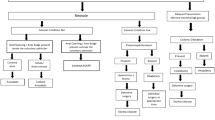
Age ranged from 1 day to 4 years. The passage of meconium was seen in urine of four boys, through ectopic openings in the perineum in three boys. One patient had a round worm passing through an ectopic opening. Three boys’ perineum showed meconium dots/streak along scrotal raphe. Anus was absent in all. Two patients had rectopenilurethral (RPU) and rectoscrotal (RS) fistula; two boys had anoscrotal and anoperineal fistula; one boy had pinhole anus with RS and RPU fistula. One boy had rectoperineal and RS fistula. One patient had rectobulbar urethral fistula with meconium filled chamber between the two hemiscrotum. Two boys had associated anomalies. Five boys had primary procedure with anterior sagittal approach—anoplasty (ASAP) and anorectoplasty (ASARP). Two patients had pelvic colostomy and ASARP in one and PSARP in one. One patient died postoperatively. One boy developed anal stenosis and needed redo. Five children have regular bowel movements and they are growing well.
Conclusion
Thorough clinical examination may identify the anatomical variations of male H-type ARM, and for the treatment of which primary ASAP or ASARP gives good results.






Similar content being viewed by others

References
Holschneider A, Hutson J, Pena A et al (2005) Preliminary report on the international conference for the development of standards for the treatment of anorectal malformations. J Pediatr Surg 40:1521–1526
Rintala RJ, Mildh L, Lindahl H (1996) H-type anorectal malformations: incidence and clinical characteristics. J Pediatr Surg 31(4):559–562
White JJ, Haller JAJ, Scott JR et al (1978) N-type anorectal malformations. J Pediatr Surg 12:95–102
Chatterjee SK, Talukder BC (1980) Double termination of the alimentary tract: a second look. J Pediatr Surg 15:623–627
Tsuchida Y, Saito S, Honna T et al (1984) Double termination of the alimentary tract in females: a report of 12 cases and a literature review. J Pediatr Surg 19:292–296
Kumar B, Sharma SB, Agrawal LD (2008) Congenital urethral hypoplasia with urethral fistula without imperforate anus: report of two cases. Afr J Paediatr Surg 5:37–39
Chatterjee SK (2006) Rare/regional varients. In: Holschneider AM, Hutson JM (eds) Anorectal malformations in children, chap 15. Springer, Berlin, pp 253–262
Banu T, Hannan JM, Aziz MA, Hoque M (2008) Anovestibular fistula with normal anus. J Pediatr Surg 43:526–529
Wakhlu A, Pandey A, Prasad A et al (1997) Perineal canal. Pediatr Surg Int 12(4):283–285
Moore SW, Alexander A et al (2008) The spectrum of anorectal malformations in Africa. Pediatr Surg Int 24(6):677–683
Aleem AA, Sheikh SEI, Mokhtar A et al (1985) Perineal groove and canal in males and females: a third look. Z Kinderchir 40:303–307
Rintala RJ, Jarvinen NJ (1996) Congenital funnel anus. J Pediatr Surg 31:1308–1310
Kluth D, Hillen M, Lambrecht W (1995) The principle of normal and abnormal hindgut development. J Pediatr Surg 30:1143–1147
Stephens FD, Donnellan WL (1977) “H-type” urethroanal fistula. J Pediatr Surg 12:95–102
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Banu, T., Hoque, M., Laila, K. et al. Management of male H-type anorectal malformations. Pediatr Surg Int 25, 857–861 (2009). https://doi.org/10.1007/s00383-009-2433-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2433-8