
Abstract
This review gives an overview of the disease spectrum of congenital diaphragmatic hernia (CDH). Etiological factors, prenatal predictors of survival, new treatment strategies and long-term morbidity are described. Early recognition of problems and improvement of treatment strategies in CDH patients may increase survival and prevent secondary morbidity. Multidisciplinary healthcare is necessary to improve healthcare for CDH patients. Absence of international therapy guidelines, lack of evidence of many therapeutic modalities and the relative low number of CDH patients calls for cooperation between centers with an expertise in the treatment of CDH patients. The international CDH Euro-Consortium is an example of such a collaborative network, which enhances exchange of knowledge, future research and development of treatment protocols.
Similar content being viewed by others


Introduction
Congenital diaphragmatic hernia (CDH) is a rare congenital anomaly of the diaphragm with an incidence of approximately 1 per 2,500 births. Typically, the abdominal organs will herniate into the chest cavity, with resulting maldevelopment of the alveoli and pulmonary vessels [1]. The defect is usually, reportedly in 84% of the cases, located on the left side of the diaphragm. Right-sided CDH and bilateral CDH, which occur in 14 and 2% of cases, are associated with a worse prognosis [2]. CDH can present as an isolated defect or in combination with other congenital anomalies, such as congenital heart disease or chromosomal anomalies [2].
The condition may be life threatening. Mortality rates in live-born patients range from 10 to 35% [3–6]. The true mortality may even be higher when taking into account antenatal death or termination of pregnancy [7]. Key determinants of mortality are the severity of pulmonary hypoplasia and the presence of pulmonary hypertension [1]. Smaller number and generations of airways, thickened alveolar septa, and abnormal architecture of the respiratory acinus characterize pulmonary hypoplasia. Pulmonary hypertension may result from the abnormal pulmonary vasculature associated with underdevelopment of the lung [8].
In the earlier days, CDH was regarded as a surgical emergency and postnatal care was mainly directed towards early repair of the defect [9]. The 1990s, however, saw improved survival rates from ‘delayed’ surgical repair, i.e. after 2 or 3 days’ physiologic stabilization with a ‘gentle’ ventilation strategy, such as permissive hypercapnia [4, 6]. This has now become the initial treatment strategy. The improved survival rates may also be related to advances in neonatal care, such as extra corporeal membrane oxygenation (ECMO) and inhaled nitric oxide (iNO) [3, 10, 11]. Nevertheless, surviving neonates still carry a substantial risk of developing secondary morbidity, such as cardiopulmonary, gastro-intestinal and neurological problems [12].
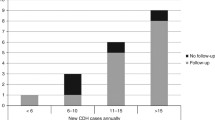
Recently, a number of reviews were published either dealing with specific center experience or reviewing the different treatment modalities [2, 13]. Progress in CDH is hampered by the relative low number in over 80% of centers (less than ten cases a year); the absence of international therapy guidelines and the lack of evidence of many therapeutic modalities. As a consequence, the problem of CDH can be classified as fivefold:
-
nearly absent knowledge of the etiology,
-
variability of phenotype and absence of accepted parameters of pre- and postnatal prediction of outcome and targeted intervention,
-
absence of properly designed clinical trials with enough power to determine optimal therapy for respiratory insufficiency and pulmonary hypertension,
-
lack of interdisciplinary structured follow-up and a database to evaluate morbidity throughout childhood and
-
translation of data of animal models of CDH for clinical practice.
In order to study these problems, the international CDH Euro-Consortium was started in 2006 to enhance collaboration in these areas of interest.
Etiology
Between the 4th and 12th week of gestation, the diaphragm arises from the septum transversum, the pleuroperitoneal folds, the esophageal mesentery, and partly from the thoracic body wall. The neuromuscular component of the diaphragm may be formed by myogenic cells and axons which coalesce with the pleuroperitoneal folds [14, 15].
Several hypotheses have been suggested in search for an explanation of the embryologic events that lead to defective development of the diaphragm. A strong candidate is mesenchymal malformation of the pleuroperitoneal folds [14]. Moreover, the ‘dual hit’ hypothesis has suggested that there is an early insult in lung development before diaphragm development, followed by further lung growth restriction later in gestation [16]. It is still not clear, however, whether the pulmonary hypoplasia induces or results from the diaphragmatic defect.
It is also believed that several genetic and environmental factors may play a role in the development of CDH. One such environmental factor, as evidenced from animal models of CDH, is retinoic acid (RA), a derivative from vitamin A. It has a key role in embryonic development, including the diaphragm and the lungs [17]. Disturbances in the RA pathway by gene knock-outs, teratogens or maternal vitamin A deficiency may lead to the development of CDH [14, 18, 19]. Furthermore, retinol plasma concentrations in CDH patients may be lower than those in healthy newborns [20]. At least, administration of RA at the end of pregnancy was found to stimulate alveolar development in rats with CDH [18].
Aneuploidies, genetic syndromes and structural abnormalities of chromosomes, such as deletions, duplications, inversions and translocations, may indicate the involvement of genetic factors. The most reported aneuploidies in CDH patients are trisomy 13, 18, 21 and 45X, the most reported genetic syndrome is Fryns syndrome [21, 22]. The transcription factor COUP-TF2, situated on chromosome 15q26, is one of the most likely candidate loci for CDH [23]. Essential for normal limb- and skeletal muscle development, COUP-TF2 is instrumental in the RA signaling pathway and interacts with other CDH candidate genes such as FOG2 [19, 24]. Mutations in FOG2 cause abnormal diaphragmatic development and pulmonary hypoplasia [25]. Thus, both genetic anomalies and disturbances in RA metabolism may be involved in the development of CDH.
Research questions
-
To determine the role of (epi) genetic deletions and duplications associated with CDH and their influence on pathways involved in pulmonary and diaphragm development.
-
To study other yet unidentified genetic mechanisms and possible candidate genes, which may cause abnormal embryonic development of lungs and diaphragm.
-
To investigate the specific role of the RA-pathway and the way in which maternal and/or neonatal disturbances in vitamin A metabolism may influence the severity of lung hypoplasia and outcome.
-
To study other possible signaling pathways in CDH lungs, which may be involved in pulmonary and diaphragm development.
-
To identify environmental factors, such as teratogenic factors, which may influence prenatal lung development.
Antenatal management
More-detailed ultrasound techniques allow for prenatal detection of CDH in almost 60% of the cases [26]. Several prenatal predictors have been proposed to determine postnatal chances of survival. These predictors may also be used to determine the need for fetal surgery.
The lung-to-head ratio (LHR), first described by Metkus et al. [29], is the most used prenatal predictor of survival in fetuses who have CDH [27–30]. It is obtained by dividing the contralateral lung area to the fetal head circumference [27]. Good predictive value has been reported for isolated cases of left-sided CDH, especially when the liver is in intrathoracic position [29, 31–33]. Others, however, doubt whether the LHR could predict postnatal outcome [34, 35]. A debatable point is the inter-observer variety that may occur. Moreover, suitability of the LHR as a predictor of survival in right-sided CDH has not yet been documented [36]. Furthermore, LHR may also dependent on the gestational age at measurement and may be less reliable in mid-gestation [30, 37]. The observed-expected LHR, which is independent of the timing of assessment, may therefore be regarded as a better prenatal predictor [38].
Recently, the fetal lung volume (FLV) has been proposed as a prenatal predictor of survival in fetuses with CDH. The lower the FLV, the lower the chance of survival and the higher the need for ECMO [39, 40]. It is mostly measured by magnetic resonance imaging (MRI), a reliable method with good interobserver agreement for measurement of the FLV [41]. Being dependent on the gestational age at measurement it is best described as a ratio of the measured volume to the expected volume [42]. Recently, the observer-to-expected FLV has been reported to be a better predictor of survival than the observed-to-expected LHR [43].
Until now, the LHR is usually considered in combination with the liver’s position to predict postnatal survival. In isolated cases of CDH, a LHR < 1.0 in combination with an intrathoracic position of the liver is considered unfavorable and warranting a fetal surgical intervention [27, 28]. The intervention is a fetal tracheal occlusion (FETO) procedure, based on the principle that plugging of the trachea, by means of a balloon, will enhance lung growth. Outcomes of FETO procedures in CDH pregnancies vary. Some studies reported higher survival rates after a FETO procedure, but others mentioned complications such as premature rupture of membranes or premature birth [28].
Prenatal prediction of survival confronts parents and doctors with difficult decisions on treatment strategies and possible prenatal interventions. So far, it is not yet clear which is the most reliable prenatal predictor of survival. Measurement of the FLV by MRI has shown promising results. However, the high costs and restricted availability of MRI systems may limit its clinical application.
Research questions
-
To determine sensitive and specific prenatal predictors of mortality and morbidity, which may be used to justify the need for fetal surgical intervention in specific cases of CDH.
-
To investigate the importance of routine fetal lung imaging, by either MRI or ultrasound, for predicting outcome.
Postnatal management
Critical care during the first hours of life
Prenatal diagnosis of CDH calls for delivery in a high-volume center with expertise in the care for newborns with CDH. A planned delivery, either an induced vaginal delivery or a caesarean section, is a good option because most babies with CDH immediately present with cardiorespiratory stress. Physical examination may reveal a barrel-shaped chest, a scaphoid abdomen, absence of breathing sounds at the ipsilateral side, shifted cardiac sounds, and bowel sounds in the chest. A chest X-ray may show subnormal lung expansion and herniated bowels, filled with air or fluid, at the side of the defect. A small abdominal cavity may be seen, as well as displacement of the heart and other mediastinal structures to the contralateral side. Liver herniation may appear as a large soft tissue mass in the thoracic cavity, in which case there is no intra-abdominal liver shadow.
Immediate intubation is almost always indicated. To further help lung expansion and decompression of the abdominal contents, a nasogastric tube with continuous or intermittent suction and an enema are indicated. Bag masking may lead to gastro-abdominal distension and therefore has to be avoided. Ventilation management in the delivery room consists of conventional mechanical ventilation or ventilation by ventilation bag. Peak pressures should be as low as possible, preferably below 25 cm H2O, with a FiO2 of 1.0.
Blood pressure support should be given to maintain arterial blood pressure levels at a normal level for gestational age. In case of severe right-to-left shunting, higher blood pressures (meaning above ≥50 mmHg) have to be pursued. In case of hypotension and/or poor perfusion, isotonic fluid therapy (10–20 ml/kg) may be given, preferentially based on cardiac ultrasounds evaluating function and contractility of the heart. Further blood pressure support consists of administration of inotropic agents, with dopamine, epinephrine, norepinephrine, and dobutamine as primary drugs of choice.
Newborns with CDH will be sedated and anaesthetized. Depth of sedation has to be evaluated by validated analgesia and sedation scoring systems, such as the COMFORT Scale [44]. Paralysis should be avoided, as it may have negative adverse effects on ventilation. However, paralyzing medical treatment may be used as a rescue therapy.
Ventilatory support
Pulmonary maldevelopment and asymmetry of the chest cavity seen in CDH makes ventilation a major challenge. Prolonged mechanical ventilation and oxygen toxicity may cause lung damage, which is predisposing to the development of chronic lung disease. In children, this is defined as pulmonary morbidity as a consequence of an acute neonatal respiratory disorder, and characterized by abnormal alveolarization and pulmonary vascular development [45–48]. Overdistension of the lungs and oxygen toxicity may be responsible for capillary leakage in the endothelium and epithelium, rupture of the basement membrane, leakage of fluid in the alveolar spaces, a general inflammatory response, and impaired surfactant secretion [2]. Moreover, genetic polymorphisms coding for vascular endothelial growth factor may be risk factors for developing chronic lung disease in newborns [49]. The best-known type of chronic lung disease in infants is bronchopulmonary dysplasia (BPD), which occurs mostly in premature and low-birth weight infants. Despite the fact that they are usually born at term, one-third of newborns with CDH will develop BPD versus 20% of preterm infants [46, 50, 51].
Researchers have sought to reduce the risk of ventilator-induced lung injury (VILI) and subsequent pulmonary morbidity by means of optimizing ventilation strategies. Since Wung et al. reported improved survival rates using a ‘gentle’ ventilation strategy, this has become the cornerstone for ventilation management in newborns with CDH [6, 52, 53]. ‘Gentle’ ventilation is based on low peak inspiratory pressures, oxygen saturations of >80%, and toleration of a rise in CO2 level. This strategy is also called permissive hypercapnia [2, 53]. Aggressive ventilation strategies with high peak inspiratory pressures cannot always be avoided, however, especially in centers without ECMO facilities.
A new method, high frequency oscillatory ventilation (HFO), was proposed to increase survival and reduce BPD in newborns with CDH [53–57]. It effectively achieves adequate gas exchange by means of an oscillatory pump, which combines very high respiratory rates with low tidal volumes. HFO is claimed to reduce the severity of lung injury induced by mechanical ventilation, by promoting uniform lung inflation, reducing barotrauma, and decreasing the activity of inflammatory mediators [53, 58–61]. It is mostly indicated when hypercarbia persists, refractory to conventional ventilation. Nevertheless, some centers also use HFO as an initial ventilation strategy. Observational and retrospective studies have suggested that HFO is a safe ventilation strategy in preterm infants as well as in term neonates [53–56, 61]. However, a Cochrane review found only a borderline significant reduction in the rate of chronic lung disease in preterm infants with the elective use of HFO as compared with conventional ventilation [59]. A second Cochrane review described the use of HFO as a rescue therapy when conventional ventilation failed in term and near-term infants with severe pulmonary dysfunction. Only one trial compared these two ventilation strategies prospectively, resulting in no significant differences in outcome, need for ECMO, or complications [61, 62]. On the negative side, HFO may cause lung hyperinflation, which may give rise to higher alveolar and mean airway pressures in some patients. The adverse effects on venous return and pulmonary vascular resistance may then increase the risk of pulmonary barotrauma and hemodynamic instability [53].
So far, there are only retrospective studies comparing the use of HFO and conventional ventilation in newborns with CDH. In one such study the use of HFO prevented hyperventilation as well as the need for ECMO [55]. Other studies showed effective CO2 reduction and increased survival in neonates with CDH and a lower incidence of chronic lung disease with elective use of HFO. A limitation of these studies is that they compared different eras and that therapy protocol was not standardized. Therefore, the results might have been positively influenced by other improvements in neonatal medicine during the last decades [53, 55–57].
Although suggested in many papers, newborns with CDH have no surfactant deficiency [50]. Surfactant inactivation may result either from underdevelopment of the lungs or from mechanical ventilation and oxygen toxicity [63–66]. A large retrospective study reported no benefit of surfactant therapy in newborns with CDH. In fact, survival rates in surfactant-treated patients were lower, and both the need of ECMO and the incidence of chronic lung disease were higher [67]. Moreover, surfactant therapy may have adverse side effects such as severe hypotension. Therefore, the use of surfactant is not recommended.
Research questions
-
To investigate the best primary ventilation mode in newborns with CDH to prevent VILI and thus decreasing mortality and pulmonary morbidity.
-
To determine underlying (epi) genetic mechanisms, which may predispose newborns with CDH to develop chronic lung disease.
-
To investigate biomarkers, which may be used to determine the degree of VILI, lung repair, remodeling and possible compensatory lung growth.
-
To study pre- and postnatal factors, such as immunologic, nutritional and environmental factors, and their possible interactions with each other, which may contribute to postnatal lung repair.
Treatment of pulmonary hypertension
As stated before, pulmonary hypertension is a major cause of mortality in infants with CDH. Severe pulmonary hypertension usually presents several hours after birth, after an initial period of relative stability [68]. In healthy neonates, pulmonary vascular resistance decreases after birth as a result of oxygenation, shear stress and ventilation. This does not occur in all newborns with CDH, and the pulmonary vascular walls may remain thickened as a consequence. Pulmonary hypertension is essentially a reversible process, but may become chronic if treatment should fail. Chronic pulmonary hypertension is usually unresponsive to therapy and may lead to right ventricular failure and death. Apart from the initial morphological changes, the vascular changes that occur immediately after the neonatal period are due to hypoxia and hyperoxic exposure of the individual cells in addition to injury and inflammatory mediators. As such, we consider pulmonary hypertension to be a part of the disease spectrum in CDH patients and which we propose to name “pulmonary vascular disease”.
Treatment of pulmonary hypertension in infants with CDH is based on several underlying signaling pathways involved in the regulation of the vascular tone and the pathogenesis of pulmonary hypertension [69]. Nitric oxide (NO) is perhaps the best-known endothelial-derived vasodilator. Inhalation of NO (iNO) interferes with the cGMP pathway and results in vasodilatation by reducing intracellular calcium levels [70]. In 1992, iNO was introduced as a treatment for pulmonary hypertension. It may decrease the pulmonary vascular resistance and right ventricle afterload, without a decrease in arterial pressure [71]. Several randomized trials with iNO showed improved oxygenation and a lesser need of ECMO. However, iNO did not reduce mortality in infants with persistent pulmonary hypertension [72]. Also, a large RCT demonstrated no reduction in mortality and need of ECMO in infants with CDH [73]. As a negative effect, rebound pulmonary hypertension may occur if iNO is weaned. Although iNO is used as the golden standard for treating newborns with pulmonary hypertension, still some 30% of newborns with CDH do not respond to iNO treatment [74, 75]. However, although no data are available to show a constant effect in patients with CDH, so far all trials on iNO are severely underpowered for CDH. At present, the use of iNO as drug of choice for the treatment of persistent pulmonary hypertension is being questioned. Taking into account the concept of right ventricular workload, more attention is paid to the ductus of Botalli and potentially restriction of closure. In a number of studies, PGE1 is advised as first choice. However, no randomized controlled trails are available to prove its superiority.
Another therapeutic strategy that interferes with the cGMP pathway is Sildenafil, which is a PDE-5 inhibitor. Sildenafil may decrease the pulmonary artery pressure more effectively than does iNO. However, both are equally effective in decreasing the pulmonary vascular resistance [76]. Moreover, Sildenafil may increase the efficacy of iNO and may prevent rebound pulmonary hypertension during weaning of iNO [77]. In infants with CDH, Sildenafil improved cardiovascular function and oxygenation in pulmonary hypertension [78, 79].
Inhibition of PDE-3, which metabolizes cAMP, is another option for the treatment of pulmonary hypertension. Milrinone, a PDE-3 inhibitor, was found to decrease the pulmonary artery pressure and pulmonary resistance in animals. Milrinone improved oxygenation in neonates with severe persistent pulmonary hypertension of the newborn and poor iNO responsiveness [80]. So far, the use of Milrinone has not yet been described in infants with CDH.
Prostacyclin (PGI2) is an endothelial-derived vasodilator that decreases intracellular calcium levels and thus leads to vasodilatation [81]. Case reports described the successful use of prostaglandin treatment in neonates with pulmonary hypertension [82–84]. De Luca et al. published case reports on the use of epoprostenol and iloprost, respectively, in the treatment of pulmonary hypertension in infants with CDH. For both agents, the child’s clinical condition improved for several hours [78, 84].
Inhibitors of endothelin (ET), which is a potent vasoconstrictor produced in the vascular endothelium, may also improve pulmonary hypertension. In randomized controlled trials, Bosentan, a non-selective ET receptor antagonist, was reported to improve exercise capacity and hemodynamics in adults with pulmonary hypertension [85, 86]. A case report described the safe and effective use of bosentan in two neonates with pulmonary hypertension due to transposition of the great arteries [87]. Still, liver toxicity was reported as an important adverse effect of bosentan [86]. Sitaxsentan and ambrisentan are specific ET-A receptor antagonists which may be more effective and less hepatotoxic than bosentan [88, 89]. No randomized controlled trials have been carried out yet to test the effect of ET receptor antagonists in neonates.
Platelet-derived growth factors (PDGFs) are upregulated in pulmonary hypertension [90, 91]. Imatinib, a PDGF inhibitor, was reported to have a dose-dependent positive effect on right ventricle hypertrophy and reverse pulmonary vascular remodeling in patients with pulmonary hypertension [90, 92]. A recent case report described the use of a tyrosine kinase inhibitor in a newborn with CDH. It gradually decreased the pulmonary artery pressure and improved the child’s clinical condition [93].
Finally, the RhoA and Rho-kinase pathways are involved in maintaining the pulmonary vascular tone and their downstream effectors form a key pathway for the regulation of the vascular tone. In animal models, Fasudil, a Rho-kinase inhibitor, showed promising results in the treatment of pulmonary hypertension. Fasudil improved pulmonary hypertension, right ventricle hypertrophy and also reversed endothelial dysfunction in rats with pulmonary hypertension [94]. In another study, Fasudil generated a vasodilatory effect in rats that were unresponsive to iNO [95].
Research questions
-
To investigate mechanisms of pulmonary angiogenesis, which may explain the postnatal “maladaption” of the pulmonary circulation in newborns with CDH.
-
To investigate the physiology and regulation of the pulmonary vascular smooth muscle cells.
-
To identify new strategies and targets for therapy including the above-mentioned rho-kinase inhibitors, PDGF inhibitors, ET receptor antagonists, prostacyclin and phosphodiesterase inhibitors.
-
To determine biomarkers which may be used to determine the severity of “pulmonary vascular disease”.
-
To investigate echocardiographic markers to determine right ventricular function.
Long-term morbidity and multidisciplinary follow-up
Approximately 87% of CDH survivors have longer lasting associated morbidity, such as pulmonary, gastro-intestinal and neurological problems. Moreover, they are at risk of developing surgical problems in later life, such as CDH recurrence or bowel obstructions because of adhesions. Associated cardiac or chromosomal anomalies in children with CDH may involve a wide range of problems, which may need thorough multidisciplinary follow-up.
Pulmonary morbidity
Approximately 30–50% of CDH survivors develop long-term pulmonary sequelae, including chronic lung disease, persistent pulmonary hypertension, asthmatic symptoms, and recurrent respiratory tract infections [12, 50, 51, 96–98]. Pulmonary hypoplasia and lung damage due to mechanical ventilation predisposes newborns with CDH to develop chronic pulmonary symptoms. Patients who received ECMO and/or a patch repair are more likely to develop pulmonary complications [99]. Long-term pulmonary sequelae may be very diverse, ranging from full clinical recovery to impaired lung function, respiratory tract infections, cor pulmonale, and even death. Up to 33% of CDH patients are oxygen-dependent for a longer time, compared to 20% of premature and low-birth weight infants [45, 51, 99].
Forty-three percent of CDH patients are discharged home with diuretics, and 17% with bronchodilators [99]. Furthermore, during the first year of life, approximately 35% required bronchodilator and/or steroid therapy [99]. Half of the CDH survivors show asthma-like symptoms, such as wheezing and bronchospasm, at one point during childhood [98]. However, asthma-like symptoms seem to decline over the years. In 22% of adolscent survivors asthmatic symptoms have been reported [98].
CDH survivors are also at risk of developing recurrent pulmonary infections. Pneumonia occurs in 7% of infants during the first year of life [100]. RSV infection, which is the most common cause of respiratory distress in infants, may put CDH survivors at a higher risk. RSV vaccination may therefore be recommended [12]. However, studies indicated no significant differences in respiratory symptoms between CDH survivors and controls [50, 98].
Many studies report obstructive lung function abnormalities in CDH survivors; restrictive and combined obstructive/restrictive abnormalities are reported to a lesser extent [50, 98–103]. Lung function abnormalities occur in 28–52% [99, 100]. Longer duration of ventilation is associated with worse pulmonary function [50]. Furthermore, chest wall deformities, which occur in 46% of the patients, may be responsible for lung function anomalies [50, 98]. CDH survivors showed higher rates of bronchial hyperreactivity after provocation tests than controls [50, 98]. It is hypothesized that this is due to ventilation-induced lung damage rather than to pulmonary hypoplasia [50]. Apart from lung function anomalies, abnormalities on chest X-rays are reported in 33–80% of the patients [51, 99]. These include hyperlucency, hyperinflation, persistent lung hypoplasia, decreased pulmonary vascularity, persistent lung opacities, mediastinal shift, and abnormal diaphragmatic profile [2, 51, 96].
Lung function abnormalities in CDH survivors are relatively mild and usually improve over time, especially after the first 6 months [102]. This may well be due to compensatory growth of the lungs, as V/Q scans show no reduction in lung volume and a normal diffusion capacity [50]. CDH patients usually have a good exercise tolerance and 83% of adult survivors of CDH consider themselves as healthy [100, 104]. Still, there is much to say for thorough pulmonary follow-up and lung function tests in CDH survivors beyond the neonatal period, especially those with severe chronic lung disease. In milder cases, monitoring of pulmonary problems is important to assess treatment strategies. Previous research on lung function abnormalities in CDH survivors was mostly retrospective, and in small samples. These retrospective data also come from the era before gentle ventilation strategies and ECMO were used and are therefore not representative for the present-day population of patients with CDH. Research should therefore be directed toward prospective follow-up of lung function and good monitoring of medication use and pulmonary problems. New techniques allow us to perform lung function measurements at a very early age, from 6 months on. Lung function tests early in life are necessary to start timely treatment that may prevent further damage from chronic lung disease.
Gastro-intestinal morbidity
Gastroesophageal reflux (GER) is a common problem in CDH survivors. It may be a source of feeding problems, failure to thrive, esophagitis and respiratory problems if not treated adequately. Possible explanations of GER in CDH survivors are esophageal dysmotility, esophageal ectasia, maldevelopment or weakness of the crura, shortening of the esophagus, disruption of the angle of His, and a higher intra-abdominal pressure as a result of the return of the herniated viscera into the abdomen after surgical repair [105, 106].
The incidence of GER is 20–84% during the first year of life [107]. An incidence of 63% was reported in adult survivors of CDH, co-existing with a Barrett’s esophagus in 54% [108]. Up to 23% of affected infants need such a surgical correction, such as fundoplication [105, 106]. Risk factors for a fundoplication in CDH survivors are a patch repair and an intrathoracal position of the liver [105].
Intestinal obstruction occurs in 4.2–20% of CDH survivors, compared to 2.2% in other infants who had a laparotomy. This increased susceptibility may be due to postoperative transient paralysis of the bowels and intestinal kinking caused by the malrotation [107, 108]. Two-third of patients who had an intestinal obstruction needed surgical correction [108].
The high incidence of GER and intestinal obstruction calls for long-term follow-up of gastro-intestinal problems in CDH survivors. Moreover, growth impairment is often reported in CDH survivors, especially in children who underwent an ECMO-procedure. Adequate treatment of GER and feeding problems may improve growth impairment [103, 104].
Neurological morbidity
Neurodevelopmental problems are often reported in CDH survivors [103]. These may be related to hypoxic brain injury and ECMO treatment. ECMO may be a risk factor for brain injury as it requires anticoagulant treatment and ligation of the carotid artery. Furthermore, there is a risk for hypoxic brain injury before and during ECMO [96]. In general, neurological sequelae occur in 10–30% of the children who underwent an ECMO-procedure [109, 110]. Nineteen percent of CDH survivors treated with ECMO had severe long-term neurodevelopmental problems, including speech problems and seizure disorders [111]. However, other studies reported ECMO was no risk factor for poor long-term neurological outcome [112, 113].
Sensoneurinal hearing loss is also reported in CDH survivors. Ototoxic medication for persistent pulmonary hypertension has been described as a risk factor for hearing loss. A recent study reported a 10% incidence of hearing problems in CDH survivors at the age of 3 years [114].
Motor problems are reported in 60% of CDH survivors during the first year of life and in 73% at the age of 3 years [103, 114]. Duration of ventilation was a predictor of motor problems at the age of 1 year. Language problems were detected in 60% of the children at the age of 3 years [114]. Social and behavioral problems were recorded in approximately 10% of the cases [114]. A study by Bouman et al. reported a mean IQ of 85 in CDH survivors, which is one standard deviation below the norm of 100. Also, only half of these children were at the expected school level [115].
Long-term neurodevelopmental follow-up is important in CDH survivors. Regular neurological, developmental and (neuro)psychological assessment by a specialized pediatrician and a child’s psychologist is recommended. In case of motor, cognitive, speech and behavorial problems, further treatment by a physiotherapist, a speech therapist or a child’s psychologist needs to be considered. Therefore, neurodevelopmental follow-up is preferably in the hands of a multidisciplinary team.
Research questions
-
To determine long-term postnatal pulmonary function and its course by performing lung function tests and radio diagnostic imaging in CDH survivors throughout childhood and into adult life.
-
To investigate environmental, nutritional and genetic risk factors for long-term morbidity in CDH survivors.
-
To study social behavior and neuropsychological development in CDH survivors.
-
To determine motor and cognitive development in CDH survivors.
-
To assess quality of life in CDH survivor and their parents.
Translational approach
Congenital diaphragmatic hernia is a severe congenital anomaly, which may contribute to significant disease burden for both parents and child. Early recognition of problems and improvement of treatment strategies may increase survival and prevent secondary morbidity. Therefore, excellent pre- and postnatal healthcare, standardized treatment protocols and a well-organized multidisciplinary follow-up are of high importance in this vulnerable group of patients. This calls for extensive collaboration between hospitals, also because of the small number of CDH patients. The CDH Euro-consortium, which is an international collaboration between 16 European high-volume centers with an expertise in the treatment of children with CDH, is an example of such a network. The CDH Euro-Consortium enhances exchange of knowledge, future research and development of state of the art protocols. Moreover, this has given rise to a central tissue bank which facilitates laboratory evaluation of (epi)genetic factors and specific biomarkers for chronic lung disease and pulmonary hypertension. Also, central development of CDH animal models may be achieved. Knowledge gained from a central tissue bank and animal models may eventually lead to improvements in health care [16].
Conclusion
This review aimed to give an overview of the disease spectrum of CDH. Survival rates have increased because of the many advances in neonatal care. However, much is still unknown about the possible etiology, the reliability of prenatal predictors of survival, ventilation strategies to reduce VILI, mechanisms of pulmonary hypertension, and long-term morbidity. Because CDH is a complex disease, which may have wide-ranging long-term sequelae, multidisciplinary healthcare is essential for both parents and child. Moreover, collaboration between centers, such as the CDH Euro-Consortium, is highly important for improvements in health care and enhancement of further research.
Abbreviations
- CDH:
-
Congenital diaphragmatic hernia
- ECMO:
-
Extra corporeal membrane oxygenation
- RA:
-
Retinoic acid
- LHR:
-
Lung-to-head ratio
- FLV:
-
Fetal lung volume
- FETO:
-
Fetal tracheal occlusion
- BPD:
-
Bronchopulmonary dysplasia
- HFO:
-
High frequency oscillation
- VILI:
-
Ventilator induced lung injury
- iNO:
-
Inhaled nitric oxide
- PGE1:
-
Prostaglandin
- cGMP:
-
Cyclic guanosine monophosphate
- PDE:
-
Phosphodiesterase
- cAMP:
-
Cyclic adenosine monophosphate
- PGI2:
-
Prostacyclin
- ET:
-
Endothelin
- PDGF:
-
Platelet-derived growth factor
- RSV:
-
Respiratory syncytial virus
- GER:
-
Gastroesophageal reflux
References
Lally KP (2002) Congenital diaphragmatic hernia. Curr Opin Pediatr 14(4):486–490
de Buys Roessingh AS, Dinh-Xuan AT (2009) Congenital diaphragmatic hernia: current status and review of the literature. Eur J Pediatr 168(4):393–406
Boloker J et al (2002) Congenital diaphragmatic hernia in 120 infants treated consecutively with permissive hypercapnea/spontaneous respiration/elective repair. J Pediatr Surg 37(3):357–366
Reyes C et al (1998) Delayed repair of congenital diaphragmatic hernia with early high-frequency oscillatory ventilation during preoperative stabilization. J Pediatr Surg 33(7):1010–1014 (discussion 1014-6)
Frenckner B et al (1997) Improved results in patients who have congenital diaphragmatic hernia using preoperative stabilization, extracorporeal membrane oxygenation, and delayed surgery. J Pediatr Surg 32(8):1185–1189
Wung JT et al (1995) Congenital diaphragmatic hernia: survival treated with very delayed surgery, spontaneous respiration, and no chest tube. J Pediatr Surg 30(3):406–409
Stege G, Fenton A, Jaffray B (2003) Nihilism in the 1990 s: the true mortality of congenital diaphragmatic hernia. Pediatrics 112(3 Pt 1):532–535
Rottier R, Tibboel D (2005) Fetal lung and diaphragm development in congenital diaphragmatic hernia. Semin Perinatol 29(2):86–93
Harting MT, Lally KP (2007) Surgical management of neonates with congenital diaphragmatic hernia. Semin Pediatr Surg 16(2):109–114
Wilson JM et al (1997) Congenital diaphragmatic hernia–a tale of two cities: the Boston experience. J Pediatr Surg 32(3):401–405
Azarow K et al (1997) Congenital diaphragmatic hernia–a tale of two cities: the Toronto experience. J Pediatr Surg 32(3):395–400
Lally KP, Engle W (2008) Postdischarge follow-up of infants with congenital diaphragmatic hernia. Pediatrics 121(3):627–632
Waag KL et al (2008) Congenital diaphragmatic hernia: a modern day approach. Semin Pediatr Surg 17(4):244–254
Clugston RD et al (2006) Teratogen-induced, dietary and genetic models of congenital diaphragmatic hernia share a common mechanism of pathogenesis. Am J Pathol 169(5):1541–1549
Holder AM et al (2007) Genetic factors in congenital diaphragmatic hernia. Am J Hum Genet 80(5):825–845
Keijzer R et al (2000) Dual-hit hypothesis explains pulmonary hypoplasia in the nitrofen model of congenital diaphragmatic hernia. Am J Pathol 156(4):1299–1306
Ross SA et al (2000) Retinoids in embryonal development. Physiol Rev 80(3):1021–1054
Montedonico S et al (2008) Prenatal treatment with retinoic acid promotes pulmonary alveologenesis in the nitrofen model of congenital diaphragmatic hernia. J Pediatr Surg 43(3):500–507
Klaassens M et al (2005) Congenital diaphragmatic hernia and chromosome 15q26: determination of a candidate region by use of fluorescent in situ hybridization and array-based comparative genomic hybridization. Am J Hum Genet 76(5):877–882
Major D et al (1998) Retinol status of newborn infants with congenital diaphragmatic hernia. Pediatr Surg Int 13(8):547–549
Kantarci S et al (2006) Findings from aCGH in patients with congenital diaphragmatic hernia (CDH): a possible locus for Fryns syndrome. Am J Med Genet A 140(1):17–23
Tibboel D, Gaag AV (1996) Etiologic and genetic factors in congenital diaphragmatic hernia. Clin Perinatol 23(4):689–699
Lurie IW (2003) Where to look for the genes related to diaphragmatic hernia? Genet Couns 14(1):75–93
Klaassens M et al (2007) Prenatal detection and outcome of congenital diaphragmatic hernia (CDH) associated with deletion of chromosome 15q26: two patients and review of the literature. Am J Med Genet A 143A(18):2204–2212
Ackerman KG et al (2005) Fog2 is required for normal diaphragm and lung development in mice and humans. PLoS Genet 1(1):58–65
Gallot D et al (2007) Prenatal detection and outcome of congenital diaphragmatic hernia: a French registry-based study. Ultrasound Obstet Gynecol 29(3):276–283
Ba’ath ME, Jesudason EC, Losty PD (2007) How useful is the lung-to-head ratio in predicting outcome in the fetus with congenital diaphragmatic hernia? A systematic review and meta-analysis. Ultrasound Obstet Gynecol 30(6):897–906
Deprest J et al (2006) Current consequences of prenatal diagnosis of congenital diaphragmatic hernia. J Pediatr Surg 41(2):423–430
Metkus AP et al (1996) Sonographic predictors of survival in fetal diaphragmatic hernia. J Pediatr Surg 31(1):148–151 (discussion 151-2)
Hedrick HL et al. (2007) Liver position and lung-to-head ratio for prediction of extracorporeal membrane oxygenation and survival in isolated left congenital diaphragmatic hernia. Am J Obstet Gynecol 197(4):422 e1-4
Lipshutz GS et al (1997) Prospective analysis of lung-to-head ratio predicts survival for patients with prenatally diagnosed congenital diaphragmatic hernia. J Pediatr Surg 32(11):1634–1636
Jani J et al (2006) Prenatal prediction of survival in isolated left-sided diaphragmatic hernia. Ultrasound Obstet Gynecol 27(1):18–22
Laudy JA et al (2003) Congenital diaphragmatic hernia: an evaluation of the prognostic value of the lung-to-head ratio and other prenatal parameters. Prenat Diagn 23(8):634–639
Heling KS et al (2005) Reliability of the lung-to-head ratio in predicting outcome and neonatal ventilation parameters in fetuses with congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 25(2):112–118
Arkovitz MS et al (2007) Fetal lung-head ratio is not related to outcome for antenatal diagnosed congenital diaphragmatic hernia. J Pediatr Surg 42(1):107–110 (discussion 110-1)
Hedrick HL et al (2004) Right congenital diaphragmatic hernia: prenatal assessment and outcome. J Pediatr Surg 39(3):319–323 discussion 319-23
Yang SH et al (2007) Reliability of the lung-to-head ratio as a predictor of outcome in fetuses with isolated left congenital diaphragmatic hernia at gestation outside 24–26 weeks. Am J Obstet Gynecol 197(1):30 e1-7
Jani J et al (2008) Timing of lung size assessment in the prediction of survival in fetuses with diaphragmatic hernia. Ultrasound Obstet Gynecol 31(1):37–40
Gorincour G et al (2005) Prenatal prognosis of congenital diaphragmatic hernia using magnetic resonance imaging measurement of fetal lung volume. Ultrasound Obstet Gynecol 26(7):738–744
Neff KW et al (2007) Prediction of mortality and need for neonatal extracorporeal membrane oxygenation in fetuses with congenital diaphragmatic hernia: logistic regression analysis based on MRI fetal lung volume measurements. AJR Am J Roentgenol 189(6):1307–1311
Busing KA et al (2008) MR relative fetal lung volume in congenital diaphragmatic hernia: survival and need for extracorporeal membrane oxygenation. Radiology 248(1):240–246
Mahieu-Caputo D et al (2001) Fetal lung volume measurement by magnetic resonance imaging in congenital diaphragmatic hernia. BJOG 108(8):863–868
Jani J et al (2008) Value of prenatal magnetic resonance imaging in the prediction of postnatal outcome in fetuses with diaphragmatic hernia. Ultrasound Obstet Gynecol 32(6):793–799
Ista E et al (2005) Assessment of sedation levels in pediatric intensive care patients can be improved by using the COMFORT “behavior” scale. Pediatr Crit Care Med 6(1):58–63
Kinsella JP, Greenough A, Abman SH (2006) Bronchopulmonary dysplasia. Lancet 367(9520):1421–1431
Baraldi E, Filippone M (2007) Chronic lung disease after premature birth. N Engl J Med 357(19):1946–1955
Bancalari E, Claure N (2006) Definitions and diagnostic criteria for bronchopulmonary dysplasia. Semin Perinatol 30(4):164–170
Bancalari E, Claure N, Sosenko IR (2003) Bronchopulmonary dysplasia: changes in pathogenesis, epidemiology and definition. Semin Neonatol 8(1):63–71
Kwinta P et al (2008) Genetic risk factors of bronchopulmonary dysplasia. Pediatr Res 64:682–688
Ijsselstijn H et al (1997) Long-term pulmonary sequelae in children with congenital diaphragmatic hernia. Am J Respir Crit Care Med 155(1):174–180
Bos AP et al (1993) Radiographic evidence of bronchopulmonary dysplasia in high-risk congenital diaphragmatic hernia survivors. Pediatr Pulmonol 15(4):231–234
Clark RH et al (2001) Lung injury in neonates: causes, strategies for prevention, and long-term consequences. J Pediatr 139(4):478–486
Logan JW et al (2007) Mechanical ventilation strategies in the management of congenital diaphragmatic hernia. Semin Pediatr Surg 16(2):115–125
Robinson PD, Fitzgerald DA (2007) Congenital diaphragmatic hernia. Paediatr Respir Rev 8(4):323–334 (quiz 334-5)
Ng GY et al (2008) Reduction in ventilator-induced lung injury improves outcome in congenital diaphragmatic hernia? Pediatr Surg Int 24(2):145–150
Migliazza L et al (2007) Retrospective study of 111 cases of congenital diaphragmatic hernia treated with early high-frequency oscillatory ventilation and presurgical stabilization. J Pediatr Surg 42(9):1526–1532
Cacciari A et al (2001) High-frequency oscillatory ventilation versus conventional mechanical ventilation in congenital diaphragmatic hernia. Eur J Pediatr Surg 11(1):3–7
Sakurai Y et al (1999) Pulmonary barotrauma in congenital diaphragmatic hernia: a clinicopathological correlation. J Pediatr Surg 34(12):1813–1817
Henderson-Smart DJ et al (2007) Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants. Cochrane Database Syst Rev 3:CD000104
deLemos R et al (1992) The use of high-frequency oscillatory ventilation (HFOV) and extracorporeal membrane oxygenation (ECMO) in the management of the term/near term infant with respiratory failure. Early Hum Dev 29(1–3):299–303
Bhuta T, Clark RH, Henderson-Smart DJ (2001) Rescue high frequency oscillatory ventilation vs conventional ventilation for infants with severe pulmonary dysfunction born at or near term. Cochrane Database Syst Rev 1:CD002974
Clark RH, Yoder BA, Sell MS (1994) Prospective, randomized comparison of high-frequency oscillation and conventional ventilation in candidates for extracorporeal membrane oxygenation. J Pediatr 124(3):447–454
Cogo PE et al (2003) Pulmonary surfactant disaturated-phosphatidylcholine (DSPC) turnover and pool size in newborn infants with congenital diaphragmatic hernia (CDH). Pediatr Res 54(5):653–658
Cogo PE et al (2004) A dual stable isotope tracer method for the measurement of surfactant disaturated-phosphatidylcholine net synthesis in infants with congenital diaphragmatic hernia. Pediatr Res 56(2):184–190
Boucherat O et al (2007) Surfactant maturation is not delayed in human fetuses with diaphragmatic hernia. PLoS Med 4(7):e237
Janssen DJ et al (2003) Surfactant phosphatidylcholine pool size in human neonates with congenital diaphragmatic hernia requiring ECMO. J Pediatr 142(3):247–252
Van Meurs K (2004) Is surfactant therapy beneficial in the treatment of the term newborn infant with congenital diaphragmatic hernia? J Pediatr 145(3):312–316
Coppola CP, Gosche JR (2001) Oxygen-induced vasodilation is blunted in pulmonary arterioles from fetal rats with nitrofen-induced congenital diaphragmatic hernia. J Pediatr Surg 36(4):593–597
Humbert M, Sitbon O, Simonneau G (2004) Treatment of pulmonary arterial hypertension. N Engl J Med 351(14):1425–1436
Kinsella JP, Abman SH (2007) Inhaled nitric oxide in the premature newborn. J Pediatr 151(1):10–15
Coggins MP, Bloch KD (2007) Nitric oxide in the pulmonary vasculature. Arterioscler Thromb Vasc Biol 27(9):1877–1885
Fliman PJ et al (2006) Neonatal extracorporeal life support: impact of new therapies on survival. J Pediatr 148(5):595–599
Wessel DL et al (1997) Improved oxygenation in a randomized trial of inhaled nitric oxide for persistent pulmonary hypertension of the newborn. Pediatrics 100(5):E7
Clark RH et al (2000) Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. Clinical Inhaled Nitric Oxide Research Group. N Engl J Med 342(7):469–474
Goldman AP et al (1997) Early response to inhaled nitric oxide and its relationship to outcome in children with severe hypoxemic respiratory failure. Chest 112(3):752–758
Michelakis E et al (2002) Oral sildenafil is an effective and specific pulmonary vasodilator in patients with pulmonary arterial hypertension: comparison with inhaled nitric oxide. Circulation 105(20):2398–2403
Atz AM, Wessel DL (1999) Sildenafil ameliorates effects of inhaled nitric oxide withdrawal. Anesthesiology 91(1):307–310
De Luca D et al (2006) Transient effect of epoprostenol and sildenafil combined with iNO for pulmonary hypertension in congenital diaphragmatic hernia. Paediatr Anaesth 16(5):597–598
Noori S et al (2007) Cardiovascular effects of sildenafil in neonates and infants with congenital diaphragmatic hernia and pulmonary hypertension. Neonatology 91(2):92–100
McNamara PJ et al (2006) Milrinone improves oxygenation in neonates with severe persistent pulmonary hypertension of the newborn. J Crit Care 21(2):217–222
Wanstall JC, Jeffery TK (1998) Recognition and management of pulmonary hypertension. Drugs 56(6):989–1007
Kelly LK et al (2002) Inhaled prostacyclin for term infants with persistent pulmonary hypertension refractory to inhaled nitric oxide. J Pediatr 141(6):830–832
Ehlen M, Wiebe B (2003) Iloprost in persistent pulmonary hypertension of the newborn. Cardiol Young 13(4):361–363
De Luca D et al (2007) Iloprost as ‘rescue’ therapy for pulmonary hypertension of the neonate. Paediatr Anaesth 17(4):394–395
Channick RN et al (2001) Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 358(9288):1119–1123
Rubin LJ (2002) Therapy of pulmonary hypertension: the evolution from vasodilators to antiproliferative agents. Am J Respir Crit Care Med 166(10):1308–1309
Goissen C et al (2008) Persistent pulmonary hypertension of the newborn with transposition of the great arteries: successful treatment with bosentan. Eur J Pediatr 167(4):437–440
Galie N et al (2005) Ambrisentan therapy for pulmonary arterial hypertension. J Am Coll Cardiol 46(3):529–535
Barst RJ et al (2006) Treatment of pulmonary arterial hypertension with the selective endothelin-A receptor antagonist sitaxsentan. J Am Coll Cardiol 47(10):2049–2056
Schermuly RT et al (2005) Reversal of experimental pulmonary hypertension by PDGF inhibition. J Clin Invest 115(10):2811–2821
Perros F et al (2008) Platelet-derived growth factor expression and function in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 178(1):81–88
Ghofrani HA, Seeger W, Grimminger F (2005) Imatinib for the treatment of pulmonary arterial hypertension. N Engl J Med 353(13):1412–1413
Frenckner B et al (2008) Platelet-derived growth factor inhibition—a new treatment of pulmonary hypertension in congenital diaphragmatic hernia? J Pediatr Surg 43(10):1928–1931
Abe K et al (2004) Long-term treatment with a Rho-kinase inhibitor improves monocrotaline-induced fatal pulmonary hypertension in rats. Circ Res 94(3):385–393
McNamara PJ et al (2008) Acute vasodilator effects of Rho-kinase inhibitors in neonatal rats with pulmonary hypertension unresponsive to nitric oxide. Am J Physiol Lung Cell Mol Physiol 294(2):L205–L213
Bagolan P, Morini F (2007) Long-term follow up of infants with congenital diaphragmatic hernia. Semin Pediatr Surg 16(2):134–144
Dotta A et al (2007) Lung volumes and distribution of ventilation in survivors to congenital diaphragmatic hernia (CDH) during infancy. Pediatr Pulmonol 42(7):600–604
Trachsel D et al (2005) Long-term pulmonary morbidity in survivors of congenital diaphragmatic hernia. Pediatr Pulmonol 39(5):433–439
Muratore CS et al (2001) Pulmonary morbidity in 100 survivors of congenital diaphragmatic hernia monitored in a multidisciplinary clinic. J Pediatr Surg 36(1):133–140
Vanamo K et al (1996) Long-term pulmonary sequelae in survivors of congenital diaphragmatic defects. J Pediatr Surg 31(8):1096–1099 discussion 1099-100
Stefanutti G et al (2004) Cardiopulmonary anatomy and function in long-term survivors of mild to moderate congenital diaphragmatic hernia. J Pediatr Surg 39(4):526–531
Koumbourlis AC, Wung JT, Stolar CJ (2006) Lung function in infants after repair of congenital diaphragmatic hernia. J Pediatr Surg 41(10):1716–1721
Gischler S et al (2009) Interdisciplinary structural follow-up of surgical newborns: a prospective evaluation. J Pediatr Surg (accepted)
Gischler S et al (2009) A prospective comparative evaluation of persistent respiratory morbidity in esophageal atresia and congenital diaphragmatic hernia survivors. J Pediatr Surg (accepted)
Diamond IR et al (2007) Predicting the need for fundoplication at the time of congenital diaphragmatic hernia repair. J Pediatr Surg 42(6):1066–1070
Su W et al (2007) Predictors of gastroesophageal reflux in neonates with congenital diaphragmatic hernia. J Pediatr Surg 42(10):1639–1643
Arena F et al (2008) Gastrointestinal sequelae in survivors of congenital diaphragmatic hernia. Pediatr Int 50(1):76–80
Vanamo K et al (1996) Long-term gastrointestinal morbidity in patients with congenital diaphragmatic defects. J Pediatr Surg 31(4):551–554
Peetsold MG et al (2009) The long-term follow-up of patients with a congenital diaphragmatic hernia: a broad spectrum of morbidity. Pediatr Surg Int 25(1):1–17
McNally H et al (2006) United Kingdom collaborative randomized trial of neonatal extracorporeal membrane oxygenation: follow-up to age 7 years. Pediatrics 117(5):e845–e854
Davis PJ et al (2004) Long-term outcome following extracorporeal membrane oxygenation for congenital diaphragmatic hernia: the UK experience. J Pediatr 144(3):309–315
Jaillard SM et al (2003) Outcome at 2 years of infants with congenital diaphragmatic hernia: a population-based study. Ann Thorac Surg 75(1):250–256
Nield TA et al (2000) Neurodevelopmental outcome at 3.5 years of age in children treated with extracorporeal life support: relationship to primary diagnosis. J Pediatr 136(3):338–344
Friedman S et al (2008) Neurodevelopmental outcomes of congenital diaphragmatic hernia survivors followed in a multidisciplinary clinic at ages 1 and 3. J Pediatr Surg 43(6):1035–1043
Bouman NH et al (2000) Children with congenital diaphragmatic hernia are at risk for lower levels of cognitive functioning and increased emotional and behavioral problems. Eur J Pediatr Surg 10(1):3–7
Acknowledgment
The authors thank J. Hagoort for his editorial assistance.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
On behalf of the CDH Euro-Consortium.
D. Tibboel presented the work at the 21st congress of the Asian Association of Pediatric Surgeons, Bangkok, Thailand, 16–19 November 2008.
The CDH Euro-Consortium
The CDH Euro-Consortium
Coordinating center
ErasmusMC-Sophia
Rotterdam, The Netherlands
Department of Paediatric Surgery and Genetics
D. Tibboel, I. Reiss, S. Gischler, H. Ijsselstijn, A. De Klein, R. Rottier
Participants
Belgium, Leuven, University Hospital KU Leuven, K. Allegaert and J. Deprest; Germany, Mannheim, Universitätsklinikum Mannheim, T. Schaible and L. Wessel; Italy, Rome, Bambino Gesu Children’s Hospital, P. Bagolan and I. Capolupo; the Netherlands, Nijmegen, UMC St. Radboud, A. van Heijst and R. Wijnen; Spain, Madrid, Hospital Universitario La Paz, J. Tovar; Portugal, Braga, University of Minho, J. Correia-Pinto; Portugal, Porto, Hospital S Joao, M. Gorett Silva; Portugal, Lisboa, Hospital de D Estefania, M. Serelha; Portugal, Amadora, Hospital Fernando Fonseca, R. Barroso; Portugal, Lisboa, Hospital de Santa Maria, J. Sladanha; Portugal, Almada, Hospital Garcia Orta, M. Lopes Primo; Portugal, Coimbra, Hospital Pediatrico de Coimbra, J. Peixoto; United Kingdom, London, King’s College, A. Greenough and K. Nicolaides.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
van den Hout, L., Sluiter, I., Gischler, S. et al. Can we improve outcome of congenital diaphragmatic hernia?. Pediatr Surg Int 25, 733–743 (2009). https://doi.org/10.1007/s00383-009-2425-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2425-8