
Abstract
Purpose
Awake craniotomy (AC) is the treatment of choice for the resection of brain tumors within eloquent brain regions for adults, but not much is known about its psychological impact on children and adolescents. Patient immaturity and difficulty in cooperating during surgery could result in psychological sequelae postoperatively, such as anxiety, panic, and worry.
Methods
In this review, we examined eight studies assessing AC performed on patients under 18 years of age (N = 85), noting exclusion criteria, interventions used, and psychological assessments implemented.
Results
Initial assessments of cognitive functioning and maturity were conducted primarily to determine patient eligibility for AC instead of an age restriction. No standardized interventions were used to minimize anxiety associated with AC. Interventions ranged from almost nothing specified to exposure to videos of the operating room, hypnosis, repeated meetings with psychologists and speech therapists, extensive meetings with the surgery team, and thorough exposure to the operating room theater. With a few exceptions, there were no standardized pre- and post-AC assessments of psychological sequelae. Qualitative evaluations indicated that most children and adolescents tolerated AC well, but one study indicated detrimental effects on school attendance postoperatively.
Conclusion
Given that most AC teams have a psychologist, it seems desirable to have pre- and post-AC psychological assessments using standardized measures of anxiety, trauma, and worry, as well as measures tailored to AC, such as time to return to school, worry about MRIs following surgery, and self-assessment of post-surgery functioning. In short, comprehensive psychological assessment of AC patients is clearly needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
How often do awake craniotomies in children and adolescents lead to trauma and worry
Awake craniotomy (AC) was introduced during the 1920s by renowned neurosurgeon, Dr. Wilder Penfield, to treat intractable epilepsy in adults in the USA. The revolutionary surgery aimed to preserve patient neurological functioning and monitor motor and somatosensory brain areas by keeping a patient conscious intraoperatively to guide surgeons in tissue removal [1, 2]. Although removing minimal tissue increased the chance of lesion recurrence, doing so was shown to effectively reduce cognitive deficits and ultimately improve the patient’s quality of life postoperatively [3, 4]. Penfield further advanced the field of neurosurgery by outlining the role of anesthetic techniques in monitoring a patient’s state of consciousness and pain level during a procedure. Using anesthetics allowed him to achieve optimal brain mapping while preserving patient comfort [5].
Since created, AC has evolved into a standard procedure for brain surgery in most hospitals and surgical centers worldwide. Modern AC is used to allow resection of lesions near eloquent cortical areas. Sometimes electrophysiological recordings are used for additional mapping during surgery [3]. Comparatively, few children undergo the procedure, so research concerning the benefits and risks of pediatric AC is lacking substantially [6]. As noted by Balogun et al. [7] some surgeons were hesitant to perform AC on patients less than 15 years of age due to differences in their brain structure. Children and adolescents have a larger number of small and unmyelinated fibers that require a higher charge density to evoke an adequate response to neurostimulation, which could harm them [7, 8]. However, as noted herein, children have been successfully operated on with AC who are as young as 7 years, and children under 15 years of age are eligible for AC in certain centers if they pass neurological, psychological, and behavior evaluations prior to the surgery [8].
Mishra et al. published a review of AC in children that provided a detailed description of the children’s preoperative team visit, preoperative workup, positioning of the child, and sedation protocol. However, they did not evaluate the influence of AC on children’s psychological sequelae caused by or related to the procedure [9].
The purpose of this manuscript is to evaluate the psychological consequences of AC in children. We examined any psychological sequelae prompted by the surgery to determine whether a patient’s age or other factors should influence AC eligibility. We reviewed published, peer-reviewed articles that addressed patients’ psychological functioning pre- and postoperatively, focusing particularly on worry, anxiety, and trauma symptoms, and their influence on the child’s overall functioning. We also examined psychological evaluations completed on pediatric patients with directed attention to the following:
-
1.
Were there standardized assessments of psychological functioning pre- and postoperatively?
-
2.
Did the assessment go beyond standardized measures of generalized anxiety and panic to address the patient’s reaction to the surgery itself?
-
3.
Were psychological interventions implemented, such as hypnosis, used to minimize the psychological impact of AC?
Methods
Eight studies were collected regarding AC performed on children and adolescents under 18 years of age. The following key words and phrases were searched using Google Scholar, PsycINFO, and Academic Search Complete: glioblastoma in children, awake craniotomy surgery, awake brain surgery, awake craniotomy procedure, awake craniotomy in children, awake craniotomy in adults, psychological sequelae of awake craniotomy in children, psychological sequelae of awake craniotomy in adults, panic, anxiety caused by awake craniotomy, and psychological interventions during awake craniotomy. Information about the effects of AC in children and adolescents is presented in Table 1 and discussed in the main body of the paper. The table outlines the sedation protocol used, characteristics of patients in the sample, type of psychological assessments implemented, whether an intervention was used to reduce anxiety of the patient, and the conclusion reached about psychological sequelae prompted by AC.
Results
Number of patients in each study
Three papers examined single-case studies, two studies included 6–7 children, two included 17–18, and one included 28 patients. Thus, the small sample size per study generally prevented parametric analyses of predictors of response to treatments. Nevertheless, certain conclusions were clearly provided by the authors.
Sedation protocols implemented
Two types of sedation protocols were implemented: (a) the fully awake (FA) protocol, in which patients remained fully conscious throughout the entire procedure, and (b) the asleep-awake-asleep (AsAAs) protocol, in which patients were sedated upon opening and closing of the dura and skull but awakened during lesion resection. The AsAAs protocol is preferred by many centers due to patients’ experience of discomfort, pain, vibrations, and loud noise during the opening and closure of the cranium [10]. Bianco et al. note that the Maggiore della Carità University Hospital in Novara, Italy, has performed 27 brain surgeries using FA protocol since 2015, and there has been only one case of evident psychological strain during the closure phase of a long-lasting surgery [11]. As a result of this case, the hospital implements AsAAs protocol unless the surgery is brief and simple, the patient is ineligible for general anesthesia, or an intraoperative awakening is expected [11]. The FA protocol might be chosen in resource-limited countries as well [11]. Out of the eight studies reviewed, two primarily adhered to the FA protocol, four adhered to the AsAAs protocol, and two did not specify the sedation protocol implemented.
Exclusion criteria
The appropriateness of AC was often determined by a child’s maturity and cognitive abilities, which were generally measured by IQ, executive functioning, academic capabilities, language and memory skills, and manual dexterity [12]. In Alcaraz García-Tejedor et al., it was not specified what percent of possible candidates were excluded based on the above criteria [12]. One of the 28 children had to have the operation under general anesthesia due to severe intraoperative agitation. The pediatric psychiatrist did not contraindicate any child for AC in the study completed by Delion et al. [6]. Huguet et al. proposed AC for 18 patients and after psychological evaluation, AC was performed on 17 patients [13]. Riquin et al. included 7 patients who had AC, two of which had high levels of preoperative anxiety and were still included. The surgery took place without difficulty [14].
Interventions used to reduce anxiety of the patients
The study completed by Delion et al. involved 6 patients aged 11–17 years (Mean = 13.67), four of whom were teenagers [6]. The patients received hypnosis conditioning, neuropsychological examination by a speech therapist, psychiatric evaluation, and neuropsychiatric follow-ups in all cases. Members of the surgical team showed patients videos of the operating room preoperatively and introduced the children to another child their age who had undergone AC. Hypnosis conditioning was completed by the anesthetic team.
Klimek et al. illustrated the use of AC in a 9-year-old boy, which is presumed to be the first publication defying Pasquet’s (1954) position that “uncooperative adults and children under 10 years will not tolerate the application of local anesthesia, scalp incision and craniotomy” [15, 16]. The patient was thoroughly exposed preoperatively to the procedures used in the operating room. There was no discussion of psychological procedures used to minimize anxiety pre- and postoperatively, or information provided on psychological assessments used.
Huguet et al. comprehensively described their preoperative evaluation and preparation of patients [13]. All children had neurological exams and MRIs. Patients whose MRIs confirmed a supratentorial lesion in a functional area were candidates for AC. Psychological assessment and preparation were conducted by a certified psychologist across several meetings with the patient to ensure that the patient and family understood AC and its psychological implications. The number of preoperative meetings was determined on a case-by-case basis, but the meetings addressed anticipated emotions and concerns. During the surgery, a neuropsychologist had constant interactions with the patient.
In the study completed by Alcaraz García-Tejedor et al., more information was provided about the anesthetic and surgical procedures than about psychological interventions [12]. They expressed that an assessment was conducted by a neuropsychologist that focused on neuropsychological deficits, language deficits, and presenting symptoms. They also noted that pictures and videos were used to help explain AC to the children.
In addressing the needs of an 11-year-old female with significant distractibility and inability to follow commands, Labuschagne et al. developed a detailed hospital theater experience for this child that has now become standard practice at the Department of Surgery at the University of Witwatersrand, South Africa [17]. The intervention involved having the child experience as much as possible of the actual surgery procedures before undergoing the surgery. As they stated, “the patient was dressed in theatre attire and brought into the theatre on a theatre trolley. She was then transferred onto the theatre bed and positioned in the same manner as she would be for the actual surgery. Her head was placed on a horseshoe headrest, and she was made to lie in a semi-lateral position, as required for the surgery. A blood pressure cuff, pulse oximeter, nasal cannula with oxygen flow, and calf pumps were applied. She was then draped precisely as she would have been for the procedure. Theatre lighting was set as it would be for the surgical case.” (p. 1) [17]. In short, the simulated theater experience allowed the hospital staff to induce typical stress provoked by the procedure. Doing so allowed the surgical team to desensitize the patient to the hospital procedures while assessing her coping skills. The authors also emphasized the development of a strong bond with a speech therapist during the simulation. This relationship was presumably important in the child having no postoperative psychological symptoms or anxiety.
Standardized measures used to assess anxiety and panic symptoms
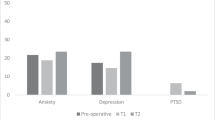
As seen in Table 1, the psychological assessment instruments used to evaluate pre- and postoperative anxiety generally were not standardized. The exceptions were present in the case study by Riquin et al., in which the Hamilton Anxiety Rating Scale [18], Global Assessment of Functioning (GAF) [19], and the Peds Quality of Life questionnaire (PedsQL) [20] were used to assess the overall functioning of an 8-year-old girl who had a resection of an intracerebral tumor [21]. This patient was a participant in a larger study by Riquin et al., but these measures were not reported in that paper [14].
In other studies, researchers implemented assessments of their own or briefly described the assessments completed. For instance, Huguet et al. provided detailed descriptions of the psychological outcomes of 17 children who underwent AC [13]. While standardized measures of anxiety and panic were not used, the detailed qualitative information provided about the psychological functioning of 8 of the 17 children was useful. One child was excluded preoperatively because of a diagnosis of OCD and recurrent depression, as psychological conditions were considered contraindications for AC by that team. Limited eligibility was seen in one patient who suffered from depression early in life and another who had pervasive developmental disorder. Two of the 17 AC patients died from tumor progression, ultimately preventing surgical staff from evaluating their emotional experience long-term. However, immediately after surgery, they did not present with negative emotions. Long-term follow-ups were available for eight of the 17 children in the form of psychological evaluations and were conducted at 3, 6, and 12 months postoperatively. Each patient met the surgeon, neurologist, psychologist, and neuropsychologist during these timepoints. The overall evaluation was positive for six children. Two children were content with the experience, but they persistently experienced disrupting feelings associated with it. One patient claimed that AC evoked fear and was painful, and the patient exhibited partial panic symptoms and persisting depressive thoughts postoperatively. This report should be respected for its frank and direct concern about the psychological effects of AC on children and adolescents since they state that AC carries a risk of its own psychological morbidity. They further note that AC needs to be considered as a potential traumatizing event and a possible cause for panic.
The case study completed by Klimek et al. indicates that the child was evaluated by a child psychologist to assess eligibility for the procedure [15]. Other psychological components, such as nightmares, levels of cooperation, endurance, emotional reactions, and ability to concentrate on difficult tasks were noted solely for eligibility purposes [15]. No standardized measures of anxiety or panic were used to assess the 9-year-old pre- and postoperatively for the resection of a glioblastoma.
Some detail is provided on the 6 cases reported in the Delion et al. study, as the authors provided some very useful clinical data, such as time to return to school and the patient’s academic performance [6]. We believe that information on time to return to school, school grades, and ability to return to extracurricular activities would be useful to report. Authors of this study aided readers by outlining the types of assessment used to evaluate their patients, and five of the six were evaluated 3 months postoperatively. Two patients returned to school 6 months post-surgery, and one returned to school full-time 3 months post-surgery; one had not returned to school 6 months post-surgery and was being taught in a hospital school. In one case, post-secondary school was completed and the individual entered medical school. In sum, the surgeries were associated with absence from school for a number of months, and some verbal problems persisted. Reports of time to return to school and to various activities would be useful to note in any AC outcomes, following the lead of Delion et al. [6].
Alcaraz García-Tejedor et al. focused more on neurological evaluations and physical observations than psychological components of the procedure [12]. Their primary outcome measure was feasibility of AC, defined as the ability to complete the procedure without conversion to general anesthesia. Median age of the children was 14, and they showed that AC was feasible in 29 of the 30 cases, with only one patient converted to general anesthesia. No patients were excluded. New neurological deficits occurred in 20% of the patients, but the deficits were transient. The researchers did not assess the psychological impact of the AC, but there were no explicit complaints of emotional distress at a postoperative follow-up.
Discussion
There are no systematic evaluations of the psychological interventions used to minimize anxiety in children or adolescents undergoing AC, even though almost all of the studies reviewed herein emphasize the need for such interventions. Given the gravity of possible operation-induced trauma, it is understandable that control groups lacking an intervention to reduce anxiety were avoided. However, alternative interventions used to minimize trauma and anxiety should be evaluated in the future. Interventions that seemed to improve patient outcomes include hypnosis conditioning, rapport building, thorough exposure to the operating room, and surgical team preoperatively, introducing the patient to someone their age who has undergone a successful AC, showing the patient a video of an operation or recovery preoperatively, and simulating the operating theater experience preoperatively. These options could be evaluated as anxiety intervention procedures using standard experimental vs. control comparisons. Neuropsychologists were nearly always involved in the overall surgical intervention across all countries examined. Accordingly, they could help organize psychological evaluations and systematically collect preoperative, postoperative, and follow-up data.
The specifics of a child’s tumor will determine the extent to which psychological interventions can be used to minimize anxiety. If a patient presents with a large or a high-grade tumor, there will be little time for psychological preparation work as surgery would be ideally scheduled within a few days to relieve intracranial pressure and reduce the risk of further tumor growth. In short, there is a need to balance risk of anxiety and psychological interventions with the need for immediate surgery. Nonetheless, variations of the hospital theater experience at the University of Witwatersrand described above could presumably be implemented a day or two before surgery.
While most authors of the studies reviewed herein emphasize the need to conduct psychological evaluations of the children and adolescents who are potential candidates for AC, the percent of children or adolescents screened out for AC often was not specified. Mishra et al. noted specific contraindications that led them to conclude absolutely that children or adolescents should not have AC [9]. Those absolute contraindications were as follows: patient/parental refusal to consent; uncooperative child; mental retardation; agitated child; profound dysphasia or language problem; learning/cognitive disabilities. Future research should include specification of the number of patients excluded and exclusion criteria to help researchers evaluate whether more children could successfully undergo AC than was originally presumed.
The literature observed lacks several details that would likely improve psychological evaluations of children and adolescents for AC. For instance, there was no explicit mention of whether patients’ tumors were cancerous and whether patients had undergone AC in the past. In addition, repeated unsuccessful surgeries could potentially make patients feel hopeless about their recovery process and the results of the procedure, which could exacerbate psychological sequelae prompted by AC. It is also recommended that all psychological evaluations take patient concerns about MRIs into consideration since many individuals expressed anxiety over completing MRI scans and may respond negatively to MRI results. An overall evaluation of the patient’s quality of life and time needed to return to varied important activities such as school (part-time; full-time), exercise (modified; non-modified), and other extracurricular activities should also be implemented. The minutes spent in each activity as well as the total minutes spent in preoperative preparation could be correlated with anxiety and worry scales. Lastly, documenting the type and extent of preoperative interventions used to minimize anxiety in the children and adolescents would be beneficial as well. Pre- and post-standardized measures of psychological functioning have not been used routinely, and if used, could contribute significantly to the literature on psychological functioning of the children and adolescents undergoing AC. Not only would it be helpful to have standardized measures of anxiety, panic, and worry for children and adolescents undergoing AC, but also it would be helpful to have measures that specifically address memories of the brain operation and post-surgery functioning. We suggest the Modified Penn State Worry Questionnaire for Children and Adolescent [22], the Youth Anxiety Measure for DSM-V [23], or the Screen for Child Anxiety Related Emotional Disorders [24]. The Modified Penn State Worry Questionnaire for Children (PSWQ-C) is a 14-item self-report questionnaire to assess worry in children and adolescents aged seven to seventeen. It measures the tendency of youth to engage in excessive, generalized, and uncontrollable worry. Examples include “My worries really bother me,” and “I know I should not worry but I just can’t help it.” The PSWQ-C is readable at the second-grade level and it has excellent internal consistency with an alpha of 0.89. The Youth Anxiety Measure for DSM-V has 28 items in the first part of the measure to assess the major anxiety disorders of the DSM-V such as separation anxiety, social anxiety, and panic disorder; the second part containing 22 items is used to measure specific phobias and agoraphobia. Cronbach’s alpha for the total scale was excellent for both clinical and non-clinical samples, 0.93 and 0.92., and parent child agreement in a clinical sample was quite good, 0.69 for major anxiety disorders, and 0.70 for phobias. The Screen for Child Anxiety and Related Disorders is a 41-item scale that is composed of the following five factors: panic/somatic symptoms, generalized anxiety disorder, separation anxiety disorder, social anxiety disorder, and school avoidance. The alphas were above 0.78 reflecting good internal consistency. The parent–child correlation for the total anxiety scale was 0.32 with a much higher correlation for those individuals older than 12 (0.43) compared to those children aged 9–12 years (0.03). Given the desirability to assess worry in children and adolescents undergoing AC, the Penn State Worry Questionnaire for Children seems very appropriate for such individuals, and it seems appropriate to also use the Youth Anxiety Measure as it measures DSM-V anxiety disorders, and it has much higher parent–child agreement than the Screen for Child Anxiety and Related Disorders. However, we believe it is crucial to conduct more specific assessments of content more related to the AC, and we provided specific scales to measure (1) the amount of intervention time used to prevent anxiety associated with AC, (2) anxiety regarding memories of the brain operation assessed 1 week after the AC, e.g., assessing anxiety when I first heard I was going to have a brain operation, and assessing anxiety when I first learned I would be awake during surgery, (3) assessment of specific worries about tumor recurrence, seizures, side effects of medications, etc., 1 week and 3 months after surgery, (4) measures of functioning 1 month post-surgery, e.g., ability to speak clearly, ability to use read for long periods of time, (5) assessment of number of weeks before return to school part-time and full-time, and weeks before return to physical education and competitive sports. Such assessment measures appear below in Tables 2, 3, 4, 5, and 6. The rating scale measures are included in Tables 2, 3, 4, 5, and 6 to assist researchers in having specific targeted measures to evaluate the impact of AC on children and adolescents. These measures are proposed to allow a clinician to monitor progress in a concrete quantitative manner of anxiety of memories of AC, specific worries of tumor recurrence and side effects of anti-seizure mediations, verbal and attention functioning post- surgery, and weeks before return to school and athletic events. If all children receiving AC in a large hospital were evaluated using such targeted measures, the aggregated data could be used to help a clinician provide individual feedback to parents and children on how an individual patient fared compared to large numbers of other children receiving AC. Finally, it seems important for both clinicians and researchers to document the type of intervention(s) used to reduce postoperative anxiety and worry, and the amount of time used to implement the intervention(s) to allow for subsequent intervention comparison and evaluation.
Qualitative data reviewed herein indicated that most children and adolescents appear to tolerate AC well, but one study indicated detrimental effects on school attendance postoperatively. Additionally, there have been no studies with systematic evaluation of anxiety, worry, and PTSD post-surgery. With data from scales suggested herein with samples of children who had AC, as well as open-ended interviews to allow the children or adolescents to express any worries or concerns regarding the AC, one can conduct a systematic evaluation of the potential for anxiety and worry following AC.
Conclusions
Returning to the three initial questions posed in the “Introduction” section of this paper, first we can unequivocally state that there were no standardized assessments of psychological functioning pre- and postoperatively. Second, in one study, the assessments did go beyond standardized measures of generalized anxiety and panic to address the patient’s reaction to the surgery itself as seen in the case of Delion’s measures of time to return to school and academic performance. Third, quite varied psychological interventions such as hypnosis and exposure to the operating room theater were used to minimize anxiety and worry in patients. Unfortunately, the interventions varied greatly and there was no way to systematically evaluate the effectiveness of the interventions to reduce anxiety and worry. It seems an opportune time to systematically evaluate the effectiveness of psychological interventions used in concert with AC, and standardized assessments of worry and DSM-V anxiety disorders are suggested along with measures designed to assess time spent in the psychological intervention used to reduce anxiety regarding AC, worries specifically related to AC, tumor recurrence, seizures, and weeks before return to academic and athletic functioning after AC.
References
Nguyen JD, Duong H (2022) Neurosurgery, sensory homunculus. Statpearls [internet]. StatPearls Publishing
Penfield W, Boldrey E (1937) Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain J Neurol 60:389–443
Bonhomme V, Franssen C, Hans P (2009) Awake craniotomy. Eur J Anaesthesiol| EJA 26:906–912
Hejrati N, Spieler D, Samuel R, Regli L, Weyerbrock A, Surbeck W (2019) Conscious experience and psychological consequences of awake craniotomy. World neurosurgery 129:e381–e386
Penfield W (1986) Combined regional and general anesthesia for craniotomy and cortical exploration: part I. Neurosurg Considerations Int Anesthesiol Clin 24:1–11
Delion M, Terminassian A, Lehousse T, Aubin G, Malka J, N’Guyen S, Mercier P, Menei P (2015) Specificities of awake craniotomy and brain mapping in children for resection of supratentorial tumors in the language area. World neurosurgery 84:1645–1652
Balogun JA, Khan OH, Taylor M, Dirks P, Der T, Snead OC III, Weiss S, Ochi A, Drake J, Rutka JT (2014) Pediatric awake craniotomy and intra-operative stimulation mapping. J Clin Neurosci 21:1891–1894
Kayama T (2012) The guidelines for awake craniotomy guidelines committee of the Japan awake surgery conference. Neurol Med Chir 52:119–141
Mishra N, Sokhal S, Rath GP, Chandra PS (2021) Awake craniotomy in children. Fundamentals Pediatr Neuroanesthesia 435–450
Palese A, Skrap M, Fachin M, Visioli S, Zannini L (2008) The experience of patients undergoing awake craniotomy: in the patients’ own words. A Qualitative Sudy Cancer Nursing 31:166–172
Bianco A, Sacchetti M, Panzarasa G (2020) Letter to the Editor regarding “Conscious experience and psychological consequences of awake craniotomy.” World Neurosurgery 133:447–447
Alcaraz García-Tejedor G, Echániz G, Strantzas S, Jalloh I, Rutka J, Drake J, Der T (2020) Feasibility of awake craniotomy in the pediatric population. Pediatr Anesth 30:480–489
Huguet L, Lohkamp L-N, Beuriat P-A, Desmurget M, Bapteste L, Szathmari A, Mottolese C, Di Rocco F (2020) Psychological aspects of awake brain surgery in children—interests and risks. Childs Nerv Syst 36:273–279
Riquin E, Dinomais M, Malka J, Lehousse T, Duverger P, Menei P, Delion M (2017) Psychiatric and psychologic impact of surgery while awake in children for resection of brain tumors. World neurosurgery 102:400–405
Klimek M, Verbrugge S, Roubos S, Van Der Most E, Vincent A, Klein J (2004) Awake craniotomy for glioblastoma in a 9-year-old child. Anaesthesia 59:607–609
Pasquet A (1986) Combined regional and general anesthesia for craniotomy and cortical exploration: part II. Neurosurg Considerations Int Anesthesiol Clin 24:12–20
Labuschagne J, Lee C-A, Mutyaba D, Mbanje T, Sibanda C (2020) Awake craniotomy in a child: assessment of eligibility with a simulated theatre experience. Case Rep Anesthesiol
Hamilton M (1959) The assessment of anxiety scales by rating (1955). Br J Med Psychol 32:52–55
Hall RC (1995) Global assessment of functioning: a modified scale. Psychosomatics 36:267–275
Varni JW, Seid M, Rode CA (1999) The PedsQL™: measurement model for the pediatric quality of life inventory. Med Care 126–139
Riquin E, Martin P, Duverger P, Menei P, Delion M (2017) A case of awake craniotomy surgery in an 8-year-old girl. Childs Nerv Syst 33:1039–1042
Chorpita BF, Tracey SA, Brown TA, Collica TJ, Barlow DH (1997) Assessment of worry in children and adolescents: an adaptation of the Penn State Worry Questionnaire. Behav Res Ther 35:569–581
Muris P, Simon E, Lijphart H, Bos A, Hale W, Schmeitz K (2017) The youth anxiety measure for DSM-5 (YAM-5): development and first psychometric evidence of a new scale for assessing anxiety disorders symptoms of children and adolescents. Child Psychiatry Hum Dev 48:1–17
Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M (1999) Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry 38:1230–1236
Funding
This review was supported in part by an APA-Wells Fargo Graduate Student Mentoring Award to K. D. O’Leary.
Author information
Authors and Affiliations
Contributions
K. D. O’Leary conceived the idea of the need for a review, guided the search process, and wrote the manuscript; A. J. Philippopoulos, A. S. Koslofsky, and Y. Ahmed searched for AC articles, discussed them with this team, prepared tables, and contributed to the manuscript text and reference section.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
O’Leary, K.D., Philippopoulos, A.J., Koslofsky, A. et al. How often do awake craniotomies in children and adolescents lead to panic and worry?. Childs Nerv Syst 40, 359–370 (2024). https://doi.org/10.1007/s00381-023-06117-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-023-06117-6