
Abstract
Introduction
Pediatric pituitary neoplasms and associated pituitary apoplexy are uncommon. There are few reports in pediatric patients of pituitary apoplexy causing focal arterial compression or diffuse vasospasm resulting in cerebral infarction, and the acute, focal neurological deficits associated with stroke differ from the typical presentation of an apoplectic pituitary tumor. We report the first case of a teenage female with an apoplectic macroprolactinoma presenting with stuttering cerebral infarction secondary to compression of the internal carotid artery (ICA).
Case
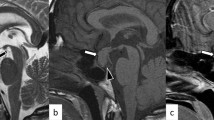
A 14-year-old female was transferred from an outside facility after presenting with right hand paresthesias and word-finding difficulty that eventually progressed to include right upper extremity weakness and mental status changes. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed an apoplectic macroprolactinemia and diffusion-weighted imaging showed acute stroke in the left anterior and middle cerebral artery distributions. Evaluation of the cerebral vasculature with MRA showed focal compression of the left supraclinoid ICA. Despite prompt surgical decompression, the patient developed right lower extremity weakness in addition to her other deficits though her deficits improved after inpatient rehabilitation.
Conclusions
In the pediatric population, there is only one other case of pituitary apoplexy presenting with stroke, which was secondary to vasospasm. We present the first case of pituitary apoplexy presenting with stroke secondary to ICA compression. Though rare, it is important to consider that pituitary apoplexy may present with non-classical symptoms such as ischemic stroke even in pediatric patients.


Similar content being viewed by others

References
Mindermann T, Wilson CB (1995) Pediatric pituitary adenomas. Neurosurgery 36(2):259–268, discussion 269
Banerjee C, Snelling B, Hanft S, Komotar RJ (2014) Bilateral cerebral infarction in the setting of pituitary apoplexy: a case presentation and literature review. Pituitary 26:26
Atkinson JL, Nippoldt TB (2002) Pituitary neurologic surgery: a unique subspecialty in evolution. Endocr Pract 8(5):356–361
Nawar RN, AbdelMannan D, Selman WR, Arafah BM (2008) Pituitary tumor apoplexy: a review. J Intensive Care Med 23(2):75–90
Chang CV, Felicio AC, Toscanini AC, Teixeira MJ, Cunha-Neto MB (2009) Pituitary tumor apoplexy. Arq Neuropsiquiatr 67(2A):328–333
Chng E, Dalan R (2013) Pituitary apoplexy associated with cabergoline therapy. J Clin Neurosci 20(12):1637–1643
Knoepfelmacher M, Gomes MC, Melo ME, Mendonca BB (2004) Pituitary apoplexy during therapy with cabergoline in an adolescent male with prolactin-secreting macroadenoma. Pituitary 7(2):83–87
Randeva HS, Schoebel J, Byrne J, Esiri M, Adams CB, Wass JA (1999) Classical pituitary apoplexy: Clinical features, management and outcome. Clin Endocrinol 51(2):181–188
Semple PL, Jane JA Jr, Laws ER Jr (2007) Clinical relevance of precipitating factors in pituitary apoplexy. Neurosurgery 61(5):956–961
Sarwar KN, Huda MS, Van de Velde V, Hopkins L, Luck S, Preston R, McGowan BM, Carroll PV, Powrie JK (2013) The prevalence and natural history of pituitary hemorrhage in prolactinoma. J Clin Endocrinol Metab 98(6):2362–2367
Fraioli B, Esposito V, Palma L, Cantore G (1990) Hemorrhagic pituitary adenomas: Clinicopathological features and surgical treatment. Neurosurgery 27(5):741–747
Tarapore PE, Sughrue ME, Blevins L, Auguste KI, Gupta N, Kunwar S (2011) Microscopic endonasal transsphenoidal pituitary adenomectomy in the pediatric population. J Neurosurg Pediatr 7(5):501–509
Mehrazin M (2007) Pituitary tumors in children: Clinical analysis of 21 cases. Childs Nerv Syst 23(4):391–398
Molitch ME, Cowen L, Stadiem R, Uihlein A, Naidich M, Russell E (2012) Tumors invading the cavernous sinus that cause internal carotid artery compression are rarely pituitary adenomas. Pituitary 15(4):598–600
Hirsch WL, Sekhar LN, Lanzino G, Pomonis S, Sen CN (1993) Meningiomas involving the cavernous sinus: Value of imaging for predicting surgical complications. AJR Am J Roentgenol 160(5):1083–1088
Chuang CC, Chang CN, Wei KC, Liao CC, Hsu PW, Huang YC, Chen YL, Lai LJ, Pai PC (2006) Surgical treatment for severe visual compromised patients after pituitary apoplexy. J Neurooncol 80(1):39–47
Rajasekaran S, Vanderpump M, Baldeweg S, Drake W, Reddy N, Lanyon M, Markey A, Plant G, Powell M, Sinha S, Wass J (2011) UK guidelines for the management of pituitary apoplexy. Clin Endocrinol 74(1):9–20
Bujawansa S, Thondam SK, Steele C, Cuthbertson DJ, Gilkes CE, Noonan C, Bleaney CW, Macfarlane IA, Javadpour M, Daousi C (2014) Presentation, management and outcomes in acute pituitary apoplexy: a large single-centre experience from the United Kingdom. Clin Endocrinol 80(3):419–424
Pozzati E, Frank G, Nasi MT, Giuliani G (1987) Pituitary apoplexy, bilateral carotid vasospasm, and cerebral infarction in a 15-year-old boy. Neurosurgery 20(1):56–59
Chokyu I, Tsuyuguchi N, Goto T, Chokyu K, Chokyu M, Ohata K (2011) Pituitary apoplexy causing internal carotid artery occlusion—Case report. Neurol Med Chir 51(1):48–51
Rosenbaum TJ, Houser OW, Laws ER (1977) Pituitary apoplexy producing internal carotid artery occlusion. Case report. J Neurosurg 47(4):599–604
Acknowledgments
The authors would like to thank Mary Soper for assistance in preparing this manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kasl, R.A., Hughes, J., Burrows, A.M. et al. Pediatric ischemic stroke from an apoplectic prolactinoma. Childs Nerv Syst 31, 1387–1392 (2015). https://doi.org/10.1007/s00381-015-2712-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-015-2712-8