
Abstract
Recently, a once-daily dose of edoxaban (15-mg) has been approved for stroke prevention in non-valvular atrial fibrillation (NVAF) patients aged ≥ 80 years, in whom standard oral anticoagulants are not recommended because of high bleeding risk (HBR), based on the ELDERCARE-AF trial. However, information regarding the characteristics and clinical outcomes among such patients is limited. Thus, this study aimed to clarify the characteristics and event rates in elderly patients with NVAF and HBR defined by the ELDERCARE-AF criteria. Of the 7406 NVAF outpatients included in the J-RHYTHM Registry, 60 patients with creatinine clearance (CrCl) < 15 mL/min were excluded. The remaining 7346 patients (age, 69.7 ± 9.9 years; men, 70.9%; warfarin use, 78.7%) were divided into three groups: Group 1, aged < 80 years (n = 6165); Group 2, aged ≥ 80 years without HBR (n = 584); and Group 3, aged ≥ 80 years with HBR (at least one of the followings; CrCl, 15–30 mL/min, history of bleeding, body weight ≤ 45 kg, and antiplatelet use) (n = 597, eligible for 15-mg edoxaban). Patients in Group 3 had a higher prevalence of comorbidities, and therefore, both higher thromboembolic and bleeding risk scores than in the other groups. During the 2-year follow-up period, the incidence rates (per 100 person-years) of thromboembolism in Groups 1, 2, and 3 were 0.7, 1.5, and 2.1 (P < 0.001), major hemorrhage, 0.8, 1.2, and 2.0 (P < 0.001), and all-cause death, 0.8, 2.6, and 4.6 (P < 0.001), respectively. Adjusted hazard ratios of Group 3 were 1.64 (95% confidence interval 0.89–3.04, P = 0.116) for thromboembolism, 1.53 (0.85–2.72, P = 0.154) for major hemorrhage, and 1.84 (1.19–2.85, P = 0.006) for all-cause death compared with Group 1. The NVAF Patients aged ≥ 80 years with HBR defined by the ELDERCARE-AF criteria were certainly at a higher adverse event risk, especially for all-cause death. Clinical trial registration: The J-RHYTHM Registry is registered in the University Hospital Medicine Information Network (UMIN) Clinical Trials Registry (unique identifier: UMIN000001569) http://www.umin.ac.jp/ctr/.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Atrial fibrillation (AF) is the most common sustained arrhythmia in adult, particularly in those of advanced age. The prevalence of AF in the population aged ≥ 80 years is reportedly 7 to 14% in Western countries [1] and 2 to 3% in Japan [2]. The number of subjects with AF is expected to increase further with the aging of society [1, 2]. AF is a major risk factor for ischemic stroke and systemic embolism (SE) [3, 4] and aging itself is a potent risk factor for stroke [5]. Thus, anticoagulation therapy is generally recommended to prevent AF-related thromboembolism in patients with AF, especially in elderly patients. Because anticoagulation therapy has a trade-off between prophylaxis of thromboembolism and an increase in the bleeding risk, physicians often hesitate to prescribe an oral anticoagulant to avoid bleeding complications, especially in very elderly patients with a high bleeding risk. Although non-vitamin K antagonist oral anticoagulants (NOACs) reportedly have a lower bleeding risk than well-controlled warfarin [6], several patients who are ineligible candidates for approved doses of NOACs still exist in actual clinical settings. Recently, a once-daily dose of edoxaban (15-mg) has been approved in Japan for stroke prevention in non-valvular AF (NVAF) patients aged ≥ 80 years, in whom standard anticoagulation therapy is not recommended because of high bleeding risk, based on the Edoxaban Low-Dose for Elder Care Atrial Fibrillation Patients (ELDERCARE-AF) trial [7]. However, information regarding the characteristics and clinical outcomes among such patients remains limited in Japan [8, 9]. Therefore, we elucidated the characteristics and event rates in NVAF patients aged ≥ 80 years with high bleeding risk, who are now eligible for once-daily 15-mg edoxaban, and the impact of high bleeding risk for adverse events, using data of the J-RHYTHM Registry [10,11,12]. In addition, since the effectiveness and safety of edoxaban 15-mg versus placebo for very elderly NVAF patients with high bleeding risk were investigated in the ELDERCARE-AF trial [7], we elucidated event rates in patients who treated with warfarin and without oral anticoagulant in this study population.
Methods
Study design of the J-RHYTHM Registry
The J-RHYTHM Registry was conducted as a nationwide prospective observational study to investigate the status of warfarin therapy and optimal warfarin therapy in Japanese patients with AF [10]. The study design and baseline patient characteristics have been reported elsewhere [10, 11]. The study protocol conformed to the Declaration of Helsinki and was approved by the ethics committee of Japanese Society of Electrocardiology (H20-01) and each participating institution. Written informed consent was obtained from all participants at the time of enrollment. A consecutive series of outpatients with AF of any type were enrolled from 158 institutions, regardless of anticoagulant use. All the drugs and their dosages were selected at the discretion of the treating physicians. Patients with valvular AF (mechanical prosthetic valve and/or mitral stenosis) were excluded.
The anticoagulation intensity in patients treated with warfarin was determined at the time of enrollment (baseline) and at each visit during the follow-up period using the prothrombin time-international normalized ratio (PT-INR). The overall quality of anticoagulation therapy with warfarin during the follow-up period was evaluated using the time in therapeutic range calculated by the Rosendaal method [13]. The target PT-INR level was set at 1.6–2.6 for elderly patients aged ≥ 70 years and at 2.0–3.0 for patients aged < 70 years according to the Japanese guidelines [14].
Definition of high bleeding risk and grouping of patients
Patients with severe renal insufficiency with creatinine clearance (CrCl) < 15 mL/min were excluded from this subanalysis, as in the ELDERCARE-AF trial. High bleeding risk was defined as at least one of the followings: (i) low CrCl of 15–30 mL/min, (ii) history of bleeding in a critical area or organ or gastrointestinal bleeding, (iii) low body weight (≤ 45 kg), (iv) continuous use of nonsteroidal anti-inflammatory drugs (NSAIDs), and (v) current use of an antiplatelet drug, according to the ELDERCARE-AF trial (Table 1) [7].
The patients were divided into three groups based on age and the presence of high bleeding risk: patients aged < 80 years (Group 1), those aged ≥ 80 years without high bleeding risk (Group 2), and those aged ≥ 80 years with one or more high bleeding risks (Group 3, patients eligible for 15-mg edoxaban) (Table 1). Because a CHADS2 score ≥ 2 is not an essential criterion for the use of once-daily 15-mg edoxaban in the current package insert of edoxaban, patients with CHADS2 score of 1 and high bleeding risk were assigned to Group 3.
Follow-up and endpoints
Patients were followed up for 2 years or until an event occurred, whichever occurred first. The primary endpoints were thromboembolism, including symptomatic ischemic stroke, transient ischemic attack (TIA), and SE; major hemorrhage, including intracranial hemorrhage (ICH), gastrointestinal bleeding, and other hemorrhages requiring hospitalization; and all-cause and cardiovascular deaths. The diagnostic criteria for each event have been described elsewhere [10, 11]. The 2-year event rates in each group were calculated and compared between the subgroups of patients who were treated with warfarin and those who were not.
Statistical analyses
Data are presented as mean ± standard deviation (SD) or number (percentage). To compare the patient characteristics and event rates among three groups, the analysis of variance for continuous variables or Chi-square test for categorical variables was performed. The differences in event rates between the two subgroups were analyzed using the Chi-square test or Fisher’s exact test, as appropriate. Cumulative event-free rates were expressed using Kaplan–Meier curves and compared among the three groups using a log-rank test. Univariable and multivariable analyses using Cox proportional hazards models were performed to investigate the influence of age and high bleeding risk on adverse events. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Group 1 as a reference. The Cox proportional hazards assumption was verified using a log–log survival curve for all study outcomes. Explanatory variables for multivariable analysis were adopted based on the significantly different variables in patient characteristics and medications among three groups (Table 2), including age, sex, congestive heart failure, hypertension, diabetes mellitus, history of stroke or TIA, coronary artery disease, cardiomyopathy, congenital heart disease, chronic obstructive pulmonary disease, hyperthyroidism, warfarin use, AF type, and hemoglobin levels, except for components of the high bleeding risk. Two-tailed P-values of < 0.05 were considered statistically significant. All statistical analyses were performed using the SPSS software (version 23.0; IBM Corporation, Armonk, NY, USA).
Results
Of a total of 7937 patients with AF enrolled in the J-RHYTHM Registry, 421 (5.3%) with valvular AF were excluded and 110 (1.5%) were lost to follow-up. Of the remaining 7406 patients with NVAF, 60 (0.8%) patients with CrCl < 15 mL/min were excluded. Consequently, 7346 patients (age, 69.7 ± 9.9 years; men, 70.9%) were included in this subanalysis and divided into three groups. The number of patients in each group was 6165, 584, and 597, respectively. The frequency of each high bleeding risk in Group 3 is shown in Table 1.
Patient characteristics and medications
The clinical characteristics of each group are shown in Table 2. The prevalence of permanent AF, coronary heart disease, chronic obstructive pulmonary disease, heart failure, hypertension, diabetes mellitus, prior stroke or TIA, and antiplatelet use was significantly different among the three groups. Both thromboembolic risk (CHADS2 and CHA2DS2-VASc scores) and bleeding risk (HAS-BLED score) therefore significantly differed among the three groups (Table 2). In addition, body weight, body mass index, diastolic blood pressure, CrCl, hemoglobin levels, warfarin dosage, and PT-INR were also significantly different among the groups.
Event rates
During the 2-year follow-up period (median: 753 days), thromboembolism, major hemorrhage, all-cause death, and cardiovascular death occurred in 125 (1.7%), 137 (1.9%), 185 (2.5%), and 62 (0.8%) patients, respectively. The corresponding incidence rates of these events were 0.85, 0.94, 1.26, and 0.42 /100 person-years, respectively, during a follow-up period of 14,641 person-years. The crude numbers and rates of adverse events in each group are summarized in Table 3. The rates of thromboembolism; major hemorrhage, including ICH and gastrointestinal bleeding; all-cause death; and cardiovascular death were significantly different among the three groups and highest in Group 3 (Table 3). In the Kaplan–Meier curves, the cumulative event-free rates for all adverse events were significantly different among the three groups (P < 0.001 for all, log-rank test), with the lowest event-free rates in Group 3 (Fig. 1).

Kaplan–Meier curves for thromboembolism (A), major hemorrhage (B), all-cause death (C), and cardiovascular death (D). P-values: comparison among groups using the log-rank test. G Group; HBR high bleeding risk
Event risk in patients with high bleeding risk
The unadjusted HRs for thromboembolism and all-cause death in Group 2 and for all adverse events in Group 3 were significantly higher than those in Group 1 on univariable analysis (Table 4). After adjusting for confounding factors in the multivariable analysis, the adjusted HR was significantly higher only for all-cause death in Group 3 than in Group 1 (Table 4).
Incidence rates and warfarin use
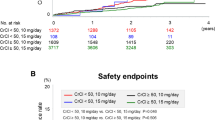
Incidence rates of adverse events in the subgroups regarding warfarin use are shown in Figs. 2 and 3. In Group 3, the incidence rates (per 100 person-years) of thromboembolism in patients with versus without warfarin were 1.7 and 3.6 (P = 0.106); major hemorrhage, 2.2 and 0.9 (P = 0.155) (Fig. 2 and Supplementary Figure); all-cause death, 3.6 and 8.5 (P = 0.004), and cardiovascular death, 1.1 and 2.2 (P = 0.248) (Fig. 3), respectively.

Incidence rates of thromboembolism and major hemorrhage in each group. P-values: comparison between patients with and without warfarin in each group. *P < 0.05, **P < 0.001. HBR High bleeding risk

Incidence rates of all-cause and cardiovascular deaths in each group. P-values: comparison between patients with and without warfarin in each group. *P < 0.05, **P < 0.001. HBR High bleeding risk
Discussion
In the present study, the high-bleeding-risk was defined following the criteria of ELDERCARE-AF trial [9], but not following the conventional bleeding risk scores, e.g., HAS-BLED score [15]. The major findings of this study are as follows. First, patients aged ≥ 80 years with a high bleeding risk (Group 3) had a higher prevalence of comorbidities, and therefore, higher CHADS2 and CHA2DS2-VASc scores, as well as higher HAS-BLED score. Indeed, the rates of all adverse events, not limited to major hemorrhage, were certainly higher in Group 3 than in the other groups. Second, the unadjusted HRs for all adverse events were significantly higher in Group 3; however, the adjusted HR was significantly higher only for all-cause death in Group 3 than in patients aged < 80 years. Third, in Group 3, warfarin use was associated with lower all-cause mortality.
Characteristics of NVAF patients with high bleeding risk
In Group 3 of the present study, the current use of an antiplatelet drug was more prevalent (61.5%), followed by low body weight (≤ 45 kg, 33.7%), low CrCl (15–30 mL/min, 31.5%), and a history of bleeding (9.9%) among the five components of high bleeding risk (Table 1). Information regarding the continuous use of NSAIDs was not collected in this study. According to our previous report on the risk factors for bleeding in the J-RHYTHM Registry, prior bleeding, elderly (age > 65 years), labile INR, and antiplatelet use were independent risk factors for major bleeding among components of the HAS-BLED score [16]. In addition, low body weight, low CrCl values, and anemia were independent risk factors for all-cause death rather than for major hemorrhage [17,18,19]. In the present study, patients in Group 3 had lower body weight and CrCl levels according to the study design, and lower hemoglobin levels in addition to a higher prevalence of components of the conventional risk scores, as shown in Table 2. Inevitably, both thromboembolic risk (CHADS2 and CHA2DS2-VASc scores [20, 21]) and bleeding risk (HAS-BLED score [15]) in Group 3 were the highest among the three groups. These findings indicate that elderly patients with NVAF and a high bleeding risk defined by the ELDERCARE-AF criteria [7] also had a higher risk of thromboembolic events and all-cause death. Similar findings were reported in patients with acute myocardial infarction after percutaneous coronary intervention, in which the high bleeding risk criteria could be useful to identify patients at high ischemic risk along with high bleeding risk [22, 23].
The patient characteristics of Group 3 in the present study were similar to those of the ELDERCARE-AF trial [7] and the high-bleeding-risk group in a subanalysis of the All Nippon Atrial Fibrillation in the Elderly (ANAFIE) Registry [9]. Among the clinical variables, the frequency of comorbidities and CHADS2 and CHA2DS2-VASc scores were slightly lower in the present study than in the ELDERCARE-AF trial [7] and subanalysis of the ANAFIE Registry [9] (Supplementary Table 1). In contrast, the frequencies of non-paroxysmal AF and antiplatelet use were higher in the present study. Of note, the bleeding risk of Group 3 in the present study expressed by the HAS-BLED score was elevated only modestly (2.3 ± 0.9) and comparable with that in the ELDERCARE-AF trial [7] and subanalysis of the ANAFIE Registry [9] (Supplementary Table 1).
Recently, several subanalyses using cluster analysis were reported from the Japanese AF registries [24,25,26,27,28]. The clusters in each registry most similar to Group 3 in our study were as follows: the atherosclerotic comorbid cluster in the J-RHYTHM Registry [25], the very elderly cluster in the Fushimi AF Registry [26], the high mortality- and heart failure-risk cluster in the Shinken Database [27], and the cluster of the very elderly patients with a high prevalence of previous major bleeding in the ANAFIE Registry [28]. The patients in these clusters had not only higher bleeding events but also higher all-cause mortality than those in the other clusters [25,26,27,28], as in Group 3 of the present study.
Impact of high bleeding risk on adverse events in NVAF patients
As shown in Table 3 and Fig. 1, the rate of major hemorrhage in Group 3 was highest among the three groups, indicating that patients in Group 3 were certainly at a higher risk of bleeding events. Notably, the rate of ICH in Group 3 was comparable to that in Group 2 but higher than that in Group 1. In contrast, the rate of gastrointestinal bleeding in Group 3 was markedly higher than that in Group 2 (Table 3). These findings suggested that advanced age (≥ 80 years) itself was an important factor for the incidence of ICH, whereas other factors such as antiplatelet use, low body weight, and low CrCl could be more critical for the development of gastrointestinal bleeding.
In addition to major hemorrhage, the crude rates of thromboembolism, all-cause death, and cardiovascular death in Group 3 were the highest among the three groups. Accordingly, the unadjusted HRs for all adverse events in Group 3 were significantly higher than those in Group 1 (Table 4). However, after adjusting for confounding factors in the multivariable analysis, the significance of the HRs for thromboembolism, major hemorrhage, and cardiovascular death disappeared, and only the HR for all-cause death in Group 3 remained significantly higher than that in Group 1 (Table 4). These findings indicate that the components of high bleeding risk in the present analysis were strongly associated with all-cause death rather than bleeding events in elderly patients with NVAF. This seems reasonable, because low body weight and low CrCl were previously identified as risk factors for all-cause death [17, 18] and were not included in the conventional risk scores, such as the CHADS2, CHA2DS2-VASc, and HAS-BLED scores [15, 20, 21]. Accordingly, we propose that for the management of NVAF patients, physicians should be cautious of not only bleeding complications but also all-cause death comprehensively, when patients are very elderly and have high bleeding risks.
High bleeding risk and anticoagulation therapy
As shown in Fig. 2, the incidence rate of major hemorrhage in patients treated with warfarin in Group 3 was apparently higher than that in those without anticoagulation therapy, although the difference was not statistically significant. Conversely, the rate of thromboembolism in patients treated with warfarin in Group 3 was numerically lower than that in those without anticoagulation therapy; however, the difference was also not statistically significant (Fig. 2). These findings indicate that anticoagulation therapy with warfarin might be effective in preventing thromboembolism even in very elderly patients with a high bleeding risk, whereas the risk of bleeding could be enhanced by warfarin. However, this was not robustly evident in this study because of the small number of patients in each subgroup of Group 3. Thus, we compared the incidence rates of thromboembolism and major hemorrhage with those of the ELDERCARE-AF trial [7] and the high-bleeding-risk group in subanalysis of the ANAFIE Registry [9] (Supplementary Figure). Although the overall event rates were lower in our study than in the ELDERCARE-AF trial, similar trends were observed in the incidence rates of thromboembolism and major hemorrhage in the high-bleeding-risk patients in the present study (Group 3) and in the other two studies (Supplementary Figure). In contrast, all-cause death in patients treated with warfarin in Group 3 was significantly lower than that in those without warfarin therapy (Fig. 3). These results suggested that warfarin might have beneficial effects on outcomes even in elderly NVAF patients with a high bleeding risk in our cohort of the warfarin era, as we previously reported in very elderly NAVF patients aged ≥ 85 years [29].
In a recent report from Asia using a largest observational cohort in Taiwan [30], warfarin use was significantly associated with a lower risk of ischemic stroke and positive net clinical benefit, without an increased risk of ICH, compared with no anticoagulation therapy, among very elderly AF patients aged ≥ 90 years (age, 96.2 ± 2.7 years; men, 39.2%; CHA2DS2-VASc score, 5.3 ± 1.6; history of major bleeding, 8.6%) in the warfarin era (1996–2011) [30]. All-cause mortality was not mentioned in that study [30]. In contrast, NOACs were significantly associated with a lower risk of ICH compared with warfarin in the NOAC era (2012–2015). According to the above study [30] and the ELDERCARE-AF trial [7], NOACs would be more favorable choice than warfarin as anticoagulation therapy in the very elderly NVAF patients with a high bleeding risk in the current NOAC era.
Further studies are warranted to validate event rates and the effect of oral anticoagulants on outcomes in very elderly NVAF patients with a high bleeding risk, as defined by the ELDERCARE-AF criteria, in the NOAC era.
Limitation
This study has several limitations. First, it was a post hoc analysis of data from the J-RHYTHM Registry [11, 12] and was, therefore, hypothesis-generating in nature. Second, the study subjects were recruited from only 158 institutions in Japan, and most of the participating physicians specialized in cardiology and management of cardiac arrhythmias. Therefore, these results may not be generalizable to the entire Japanese population with NVAF. In addition, because all study participants were Japanese, these data may not necessarily be applicable to other racial/ethnic groups. Third, changes in drugs, dosages, and drug adherence during the follow-up period were not considered in the analysis. Fourth, NSAID use, frailty, dementia, or a history of fall was not evaluated, because these data were not collected; therefore, the high bleeding risk might have been underestimated. Fifth, although only patients with a CHADS2 score ≥ 2 were included in the ELDERCARE-AF trial based on its entry criteria [7], 67 patients aged ≥ 80 years with high bleeding risk and a CHADS2 score of 1 were included in Group 3 of the present study based on the current package insert of edoxaban, in which a CHADS2 score ≥ 2 is not an essential criterion for the use of once-daily 15-mg edoxaban in Japan. However, the influence of the 67 patients on adverse events might be small, because all event rates were comparable between the 597 patients in Group 3 and the 530 patients after excluding 67 patients with a CHADS2 score of 1 (Supplementary Table 2). Finally, data from the warfarin era were used for the present analysis. Therefore, caution should be exercised when extrapolating the present results to patients with NVAF in the NOAC era. In addition, although warfarin use was significantly associated with lower all-cause mortality in Group 3 (Fig. 3), causality cannot be determined from this study because of observational nature.
Conclusions
The NVAF patients aged ≥ 80 years with one or more high bleeding risks were certainly at a higher risk of adverse events, especially all-cause death. A high bleeding risk as defined by the ELDERCARE-AF criteria was strongly associated with all-cause death rather than major hemorrhage in very elderly patients with NVAF.
Data availability
The deidentified participant data will be shared on a request basis. Please directly contact the corresponding author to request data sharing.
References
Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS (2006) Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 114:119–125
Inoue H, Fujiki A, Origasa H, Ogawa S, Okumura K, Kubota I, Aizawa Y, Yamashita T, Atarashi H, Horie M, Ohe T, Doi Y, Shimizu A, Chishaki A, Saikawa T, Yano K, Kitabatake A, Mitamura H, Kodama I, Kamakura S (2009) Prevalence of atrial fibrillation in the general population of Japan: an analysis based on periodic health examination. Int J Cardiol 137:102–107
Wolf PA, Abbott RD, Kannel WB (1991) Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 22:983–988
Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG (1995) Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med 155:469–473
Marinigh R, Lip GY, Fiotti N, Giansante C, Lane DA (2010) Age as a risk factor for stroke in atrial fibrillation patients: implications for thromboprophylaxis. J Am Coll Cardiol 56:827–837
Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, Camm AJ, Weitz JI, Lewis BS, Parkhomenko A, Yamashita T, Antman EM (2014) Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 383:955–962
Okumura K, Akao M, Yoshida T, Kawata M, Okazaki O, Akashi S, Eshima K, Tanizawa K, Fukuzawa M, Hayashi T, Akishita M, Lip GYH, Yamashita T (2020) Low-dose edoxaban in very elderly patients with atrial fibrillation. N Engl J Med 383:1735–1745
Ide Y, Ogawa H, Ishigami K, Ikeda S, Doi K, Hamatani Y, Fujino A, An Y, Ishii M, Iguchi M, Masunaga N, Esato M, Tsuji H, Wada H, Hasegawa K, Abe M, Lip GYH, Akao M (2021) Clinical characteristics and outcomes of very elderly patients with atrial fibrillation at high bleeding risk- the Fushimi AF Registry. Circ Rep 3:629–638
Okumura K, Yamashita T, Akao M, Atarashi H, Ikeda T, Koretsune Y, Shimizu W, Suzuki S, Tsutsui H, Toyoda K, Hirayama A, Yasaka M, Yamaguchi T, Teramukai S, Kimura T, Morishima Y, Takita A, Inoue H (2022) Oral anticoagulants in very elderly nonvalvular atrial fibrillation patients with high bleeding risks: ANAFIE Registry. JACC Asia 2:720–733
Atarashi H, Inoue H, Okumura K, Yamashita T, Origasa H (2011) Investigation of optimal anticoagulation strategy for stroke prevention in Japanese patients with atrial fibrillation -the J-RHYTHM Registry study design. J Cardiol 57:95–99
Atarashi H, Inoue H, Okumura K, Yamashita T, Kumagai N, Origasa H (2011) Present status of anticoagulation treatment in Japanese patients with atrial fibrillation -a report from the J-RHYTHM Registry. Circ J 75:1328–1333
Inoue H, Okumura K, Atarashi H, Yamashita T, Origasa H, Kumagai N, Sakurai M, Kawamura Y, Kubota I, Matsumoto K, Kaneko Y, Ogawa S, Aizawa Y, Chinushi M, Kodama I, Watanabe E, Koretsune Y, Okuyama Y, Shimizu A, Igawa O, Bando S, Fukatani M, Saikawa T, Chishaki A (2013) Target international normalized ratio values for preventing thromboembolic and hemorrhagic events in Japanese patients with non-valvular atrial fibrillation: results of the J-RHYTHM Registry. Circ J 77:2264–2270
Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E (1993) A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost 69:236–239
JCS Joint Working Group (2014) Guidelines for pharmacotherapy of atrial fibrillation (JCS 2013): Digest version. Circ J 78:1997–2021
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY (2010) A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 138:1093–1100
Tomita H, Okumura K, Inoue H, Atarashi H, Yamashita T, Origasa H (2015) Assessment of risk factors for bleeding in Japanese patients with non-valvular atrial fibrillation receiving warfarin treatment: a subanalysis of the J-RHYTHM Registry (letter). Int J Cardiol 201:308–310
Inoue H, Kodani E, Atarashi H, Okumura K, Yamashita T, Origasa H (2016) Impact of body mass index on the prognosis of Japanese patients with non-valvular atrial fibrillation. Am J Cardiol 118:215–221
Kodani E, Atarashi H, Inoue H, Okumura K, Yamashita T, Origasa H (2018) Impact of creatinine clearance on outcomes in patients with non-valvular atrial fibrillation: a subanalysis of the J-RHYTHM Registry. Eur Heart J Qual Care Clin Outcomes 4:59–68
Kodani E, Inoue H, Atarashi H, Okumura K, Yamashita T, Origasa H (2020) Impact of hemoglobin concentration and platelet count on outcomes of patients with non-valvular atrial fibrillation: a subanalysis of the J-RHYTHM Registry. Int J Cardiol 302:81–87
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ (2001) Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 285:2864–2870
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ (2010) Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial fibrillation. Chest 137:263–272
Sotomi Y, Hikoso S, Nakatani D, Suna S, Dohi T, Mizuno H, Okada K, Kida H, Oeun B, Sunaga A, Sato T, Kitamura T, Sakata Y, Sato H, Hori M, Komuro I (2021) Prevalence of the Japanese high bleeding risk criteria and its prognostic significance for fatal bleeding in patients with acute myocardial infarction. Heart Vessels 36:1484–1495
Matsumoto T, Saito Y, Sato T, Yamashita D, Suzuki S, Saito K, Wakabayashi S, Kitahara H, Sano K, Kobayashi Y (2023) Diagnostic ability of Japanese version of high bleeding risk criteria for ischemic outcomes in patients with acute myocardial infarction. Heart Vessels. https://doi.org/10.1007/s00380-023-02303-3
Inohara T, Piccini JP, Mahaffey KW, Kimura T, Katsumata Y, Tanimoto K, Inagawa K, Ikemura N, Ueda I, Fukuda K, Takatsuki S, Kohsaka S (2019) A cluster analysis of the Japanese multicenter outpatient registry of patients with atrial fibrillation. Am J Cardiol 124:871–878
Watanabe E, Inoue H, Atarashi H, Okumura K, Yamashita T, Kodani E, Kiyono K, Origasa H (2021) Clinical phenotypes of patients with non-valvular atrial fibrillation as defined by a cluster analysis: a report from the J-RHYTHM registry. Int J Cardiol Heart Vasc 37:100885
Ogawa H, An Y, Nishi H, Fukuda S, Ishigami K, Ikeda S, Doi K, Ide Y, Hamatani Y, Fujino A, Ishii M, Iguchi M, Masunaga N, Esato M, Tsuji H, Wada H, Hasegawa K, Abe M, Tsukahara T, Lip GYH, Akao M (2021) Characteristics and clinical outcomes in atrial fibrillation patients classified using cluster analysis: the Fushimi AF Registry. Europace 23:1369–1379
Suzuki S, Yamashita T, Otsuka T, Arita T, Yagi N, Kishi M, Semba H, Kano H, Matsuno S, Kato Y, Uejima T, Oikawa Y, Matsuhama M, Iida M, Inoue T, Yajima J (2021) Identifying risk patterns in older adults with atrial fibrillation by hierarchical cluster analysis: a retrospective approach based on the risk probability for clinical events. Int J Cardiol Heart Vasc 37:100883
Suzuki S, Yamashita T, Akao M, Atarashi H, Ikeda T, Okumura K, Koretsune Y, Shimizu W, Tsutsui H, Toyoda K, Hirayama A, Yasaka M, Yamaguchi T, Teramukai S, Kimura T, Morishima Y, Takita A, Inoue H (2023) Clinical phenotypes of older adults with non-valvular atrial fibrillation not treated with oral anticoagulants by hierarchical cluster analysis in the ANAFIE Registry. PLoS ONE 18:e0280753
Kodani E, Atarashi H, Inoue H, Okumura K, Yamashita T, Origasa H (2015) Use of warfarin in elderly patients with non-valvular atrial fibrillation -subanalysis of the J-RHYTHM Registry-. Circ J 79:2345–2352
Chao TF, Liu CJ, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Liao JN, Chung FP, Chen TJ, Lip GYH, Chen SA (2018) Oral anticoagulation in very elderly patients with atrial fibrillation: a nationwide cohort study. Circulation 138:37–47
Funding
The J-RHYTHM Registry was supported by a grant from the Japan Heart Foundation (12080025).
Author information
Authors and Affiliations
Consortia
Contributions
Kodani contributed to the statistical analyses and wrote the manuscript. Inoue, Atarashi, Okumura, and Yamashita are on the Executive Committee of the J-RHYTHM Registry, and they planned and supervised the study comprehensively and edited the manuscript, as appropriate. Origasa contributed as a statistical advisor.
Corresponding author
Ethics declarations
Conflict of interest
Dr. Kodani received remuneration from Daiichi-Sankyo; Dr. Inoue received remuneration from Daiichi-Sankyo; Dr. Atarashi received remuneration from Daiichi-Sankyo; Dr. Okumura received remuneration from Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi-Sankyo, Johnson & Johnson, and Medtronic; and Dr. Yamashita received research funding from Bayer Healthcare, Bristol-Meyers Squibb, and Daiichi-Sankyo and remuneration from Bayer Healthcare, Bristol-Myers Squibb, Daiichi-Sankyo, Novartis, Ono Pharmaceutical, Otsuka Pharmaceutical, and Toa Eiyo. Dr. Origasa received remuneration from Johnson & Johnson. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kodani, E., Inoue, H., Atarashi, H. et al. Characteristics and outcomes in elderly patients with non-valvular atrial fibrillation and high bleeding risk: subanalysis of the J-RHYTHM Registry. Heart Vessels 39, 330–339 (2024). https://doi.org/10.1007/s00380-023-02343-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-023-02343-9