
Abstract
Background
Conservative/regenerative therapy for cruciate ligament ruptures can be considered as primary treatment. However, nowadays, the first option is almost always only surgical, although studies on the efficacy of intervention exist in the literature.
Objective
This scoping review aimed to map and summarize the literature to identify interventions with RegentK treatment available for cruciate ligament ruptures.
Methods
Four databases were searched until May 2022. Studies that considered anterior cruciate ruptures treated with the RegentK method could be included. All interventions and contexts were considered. No restrictions were applied regarding language, study design, or publication type. No grey literature and reference lists of included articles were identified. Results were presented in numerical and thematic form.
Results
From 245 initial records, 7 studies met the inclusion criteria. Most of the articles were randomized controlled trials (RCTs) and considered sports patients with cruciate ligament ruptures. The authors discuss only one range of interventions: conservative (n = 7); specifically, the conservative/regenerative RegentK treatment.
Conclusion
This is the first scoping review that provides a comprehensive overview of the topic. The results revealed clear gaps in primary research, confirming that current management is based on surgery. This review may be useful for overall management and may provide a starting point for future research.
Zusammenfassung
Hintergrund
Eine konservative/regenerative Behandlung bei Kreuzbandrupturen kann als primäre Therapie in Erwägung gezogen werden. Jedoch ist heutzutage fast immer eine rein chirurgische Behandlung die erste Option, auch wenn Studien zur Wirksamkeit der genannten Intervention in der Literatur vorhanden sind.
Ziel
Ziel des vorliegenden Scoping Review war es, eine Übersicht und Zusammenfassung über die Literatur zu geben, um Interventionen mit RegentK-Therapie zu erfassen, die bei Kreuzbandrupturen zur Verfügung stehen.
Methoden
Dazu wurden 4 Datenbanken bis Mai 2022 durchsucht. Hierbei konnten solche Studien in die Auswertung eingeschlossen werden, in denen mit der RegentK-Methode behandelte Kreuzbandrupturen geprüft wurden. Sämtliche Interventionen und Kontexte wurden berücksichtigt. In Bezug auf Sprache, Studiendesign oder Publikationstyp gab es keine Beschränkungen. Es wurden keine graue Literatur und Referenzlisten der eingeschlossenen Artikel identifiziert. Die Ergebnisse wurden in numerischer Form und thematisch dargestellt.
Ergebnisse
Von anfänglich 245 Datensätzen erfüllten 7 Studien die Einschlusskriterien. Bei den meisten Artikeln handelte es sich um randomisierte kontrollierte Studien (RCT), in denen Sportpatienten mit Kreuzbandrupturen berücksichtigt wurden. Von den Autoren wird nur eine Möglichkeit der Intervention erörtert: die konservative (n = 7); konkret, die konservative/regenerative RegentK-Therapie.
Schlussfolgerung
In der vorliegenden Arbeit handelt es sich um das erste Scoping Review, das einen umfassenden Überblick über das Thema gibt. Die Ergebnisse zeigen klare Mängel bei der Primärforschung, was bestätigt, dass die derzeitige Versorgung auf der chirurgischen Behandlung basiert. Dieses Review kann hilfreich in Bezug auf die Gesamtbehandlung sein und möglicherweise einen Ausgangspunkt für zukünftige Forschung bieten.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ruptures of the anterior cruciate ligament (ACL) of the knee are comparatively frequent injuries in various sports, especially in skiing and snowboarding, but also in soccer and other ball sports [1,2,3,4]. Currently, the standard treatment for ruptured ligaments is surgery, with the aim of stabilizing the ligament and improving function [5, 6]. However, research on conservative treatment of ACL rupture has provided evidence of similar long-term benefits compared to surgical treatment. In a 10-year follow-up study of matched pairs of 50 high-level athletes who had been treated either surgically or conservatively, no difference in function was obvious: both groups demonstrated an International Knee Documentation Committee (IKDC) score of 77.1 out of 100 possible score points [7]. In a randomized trial, 121 adolescents with ACL rupture were randomized to receive either immediate surgery or conservative treatment with subsequent surgery, if indicated. After the 2‑year trial, function was equal in both groups, and 23 out of 59 patients under conservative treatment received surgery later on [8]. A 5-year follow-up study of those patients demonstrated no significant differences in IKDC score compared to the surgical group, with the operated patients improving by 42.9 points and the conservatively treated patients by 44.9 points [9]. Surgery has been advocated as a measure to prevent future osteoarthritis. But this opinion is no longer supported by current scientific evidence, as long-term outcomes for osteoarthritis are similar between operated and conservatively treated patients [5]. These data have led a Swiss panel to advise against routine operation and call for conservative treatment instead, especially since the cost–benefit ratio of surgery for ACL ruptures is negative [5].
Therefore, what evidence-based conservative and regenerative interventions are available for athletes with ACL ruptures? To the authors’ knowledge, no review has been conducted to answer this study question and, as a result, there is no comprehensive overview for clinicians and researchers.
This study aimed to highlight and begin to fill this gap using a scoping review design. The synthesis of clinical data could add significant information for the overall management of athletes and could stimulate further research in this field.
As advocated by the Joanna Briggs Institute (JBI) [10], the scoping review approach can be used to map and clarify key concepts, identify gaps in the research knowledge base, and report on the types of evidence that address and inform practice in the field. These aims correspond to the objectives of this project. For this reason, other types of review, such as systematic reviews, umbrella reviews, or rapid reviews, were not considered methodologically effective.
This scoping review aimed to:
-
1.
provide a comprehensive overview of all studies addressing ACL regeneration interventions combined with conservative therapy and
-
2.
identify any gaps in knowledge on the topic.
Methods
The present scoping review was conducted following the JBI methodology [10] for scoping reviews. The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) [11] checklist was used for reporting.
Research team
To support robust and clinically relevant results, the research team included authors with expertise in evidence synthesis, quantitative and qualitative research methodology, sport, and musculoskeletal rehabilitation.
Review question
We formulated the following research question: “What is known from the existing literature on conservatively treated anterior cruciate ligament regeneration?”
Eligibility criteria
Inclusion criteria
Studies were eligible for inclusion if they met the following population, concept, and context (PCC) criteria.
Population.
Athletes of any age, practicing any type of sport at any level of performance (e.g., professional/elite, amateur/master/recreational) with any type of break were included. As we wanted to focus only on this particular subgroup of the sports population, the definition of “athlete” used in a single study was taken as the main criterion.
Concept.
Any intervention (preventive, conservative, pharmacological), except surgical, was considered.
Context.
This review considered studies conducted in any context. Types of evidence sources: this scoping review included any study design or type of publication. No time, geographic, setting, or language restrictions were applied.
Exclusion criteria
Studies that did not meet the specific PCC criteria were excluded.
Search strategy
An initial limited search of MEDLINE was performed through the PubMed interface to identify articles on the topic, and the index terms used to describe the articles were then used to develop a comprehensive search strategy for MEDLINE. The search strategy, which included all identified keywords and index terms, was adapted for use in Cochrane Central, Scopus, and PEDro, and reported in full in the Supporting Information File S1. In addition, grey literature (e.g., Google Scholar, direct contacts with experts in the field and sports medicine) and reference lists of all relevant studies were also searched. Searches were conducted on 9 May 2022, with no date limitation.
Study selection
Once the search strategy had been completed, search results were collated and imported to EndNote V.X9 (Clarivate Analytics, London, UK). Duplicates were removed using the EndNote deduplicator before the file containing a set of unique records was made available to reviewers for further processing. The selection process consisted of two levels of screening using Rayyan QCRI online software12: 1) a title and abstract screening and 2) a full-text selection. For both levels, two authors independently screened the articles with conflicts were resolved by a third author.
The entire selection process and reasons for exclusion were recorded and reported according to the latest published version of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA 2020) flow diagram.
Data extraction and data synthesis
Data extraction was conducted using an ad-hoc data extraction form which was developed a priori, based on the JBI data extraction tool. Key information (authors, country, year of publication, study design, patient characteristics, PFD, type of intervention, and related procedures) on the selected articles were collected. Descriptive analyses were performed, and the results were presented numerically. Studies identified and included were reported as frequency and percentage, and the description of the search decision-making process was mapped. In addition, extracted data were summarized in tabular form according to the main characteristics.
Results
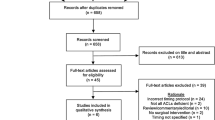
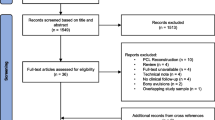
As presented in the PRISMA 2020 flow diagram (Fig. 1), from 245 records identified in the initial literature searches, 238 were excluded and 7 articles were included. The reasons for exclusion and the corresponding references are reported in online Supporting Information Tables 1 and 2 (online supplementary information).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram [12]. (From Page et al. [13]. For more information, visit: http://www.prisma-statement.org/.) aConsider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). bIf automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools
Characteristics of included studies
Table 3 synthesizes the main characteristics of the studies. To provide a transparent report, Supporting Information File S1 shows the complete extracted data for each included study. They are all randomized controlled trials except for two, which are case series. However, the majority of subjects were male and the intervention was always, when present, conservative. There are no active study protocols to date. The studies were all carried out in Salzburg, Austria.
Participants
Table 1 summarizes the data on subjects of different age groups with anterior cruciate ligament ruptures practicing different types of sports and with various levels of participation. In all articles, the authors defined the participants as sportingly active, but the level of performance was not clearly reported. With regard to ACL rupture, knee instability and pain were the most commonly explored symptom. Pain was not clearly reported in all studies, but in most cases, athletes suffered from it. In one study, it was evaluated. In two studies by Litscher G. et al. [6, 18], temperature was measured after RegentK treatment.
Discussion
In the present scoping review, we mapped and summarized the literature on RegentK or Khalifa therapy interventions in patients with acute anterior cruciate ligament rupture. Among the seven included articles, the majority focused on multiple or high-impact sports. As already pointed out by other authors, a large number of epidemiological studies have been published which report a high prevalence of rupture of the relaxed ligament. However, research on conservative or regenerative treatment of the anterior cross-ligament (ACL) is still scarce. The present scoping review confirmed that only a few authors have evaluated the efficacy of conservative and regenerative interventions dedicated to this population. Notably, only seven primary studies are currently available evaluating the efficacy of the conservative approach. Analyzed studies indicate that RegentK therapy improves functional parameters such as passive mobility of the knee joint and quadriceps strength. Ofner et al. [15, 19] show that all but 1 patient increased their walking speed in a range of 3 to 68% (mean 18%), also increasing their stride length (range 0–38 cm, mean 10 cm). This improvement is explained mechanistically due to the RegentK treatment improving activation of the gastrocnemius and, consequently, this general muscular strategy can stabilize the injured knee joint [20]. This agrees with current literature that observes immediate effects of manual therapy after just a single treatment, which suggests that the underlying mechanism is composed of rapid-response processes rather than complex metabolic phenomena. These rapid adaptations could include changes in synovial fluid such as, for example, cytokine and keratin sulphate [21], increased exchanges between synovial fluid and between synovial fluid and cartilage matrix, or an increase in synovial turnover [22, 23] as well as fluid mobilization in the lymphatic system [24]. Litscher G et al. [14, 16, 18], RegentK brings local effects but also potentially neurovegetative system effects, and a very significant increase in temperature on the injured knee was observed after RegentK, as opposed to common physiotherapy which elicited no local or systemic changes. Based on current knowledge, our literature search revealed few publications on the subject, confirming that the first treatment option remains surgery.
Research implications and suggestions for clinical practice
Anterior cruciate rupture patients are a unique group of patients who have higher functional demands and may require a different and specific approach.
Indeed, as with other disorders, such as musculoskeletal disorders [25], several factors, both intrinsic and extrinsic, must be taken into account. Therefore, after an individual assessment, a specific intervention plan must be defined. The overall management must be specific and adapted to the person. In order to provide better guidance for clinical practice and fill current gaps, more high-quality research should be performed. It is important to emphasize that these suggestions are not recommendations or evidence. Scoping reviews are not conducted to develop reliable clinical guidelines and recommendations, but implications for practice in terms of indications provided from a clinical perspective may be provided.
Strengths and limitations
Addressing the evidence gap
To our knowledge, this is the first study to map and summarize the literature to identify available interventions for conservative/regenerative therapy for anterior cruciate rupture, RegentK. We used a scoping review design. We answered a relevant research question by identifying the volume and distribution of the evidence base. We also mapped key concepts and research priorities within the literature.
Methodology
An extensive search strategy in the main databases with very broad inclusion criteria was conducted. Moreover, to conduct the review, we followed the JBI manual. To describe the selection process, we applied the updated PRISMA 2020, and for reporting we used the PRISMA for checklist scoping reviews.
Clinical practice
Although this is a scoping review [10], we did not assess the methodological quality of the individual studies, and it is not possible to draw conclusions on the most effective intervention for ACL ruptures with RegentK therapy, we have provided as complete an overview as possible. It must be emphasized that this is a therapy that can only be used by one person and that its content is not further defined. Consequently, the results of previous existing studies cannot be independently verified.
Conclusion
This scoping review identified seven studies exploring and discussing the interventions available for conservative/regenerative therapy of cruciate ligament rupture. The results showed a larger number of RCTs addressing this topic. The authors extensively discussed RegentK therapy as a possible alternative to surgery or standard physiotherapy. Of these, the conservative approach was the one suggested. The results of the present study showed that suggestions for clinical practice were basically supported by the transferability of results from the non-athletic population or expert opinion. A further limitation is the limited knowledge of the technique and its application, which largely resides by one person. Therefore, there is a great need for primary research that considers individual characteristics, sport-related variables, and is within the framework of multidisciplinary management.
References
Delincé P, Ghafil D (2012) Anterior cruciate ligament tears: conservative or surgical treatment? A critical review of the literature. Knee Surg Sports Traumatol Arthrosc 20(1):48–61
Kvist J (2004) Rehabilitation following anterior cruciate ligament injury: current recommendations for sports participation. Sports Med 34(4):269–280
Muaidi QI, Nicholson LL, Refshauge KM, Herbert RD, Maher CG (2007) Prognosis of conservatively managed anterior cruciate ligament injury: a systematic review. Sports Med 37(8):703–716
Waldén M, Atroshi I, Magnusson H, Wagner P, Hägglund M (2012) Prevention of acute knee injuries in adolescent female football players: cluster randomised controlled trial. BMJ 344:e3042
Vavken P, Leumann A, Hügle T, Valderrabano V, Pagenstert G. Kreuzband und Arthrose: Was können wir aus den Tiermodellen lernen, und was ist die klinische Evidenz beim Menschen. https://www.bisp-surf.de/Record/PU201401000827/HierarchyTree?hierarchy=JO00000001295
Litscher G, Ofner M, He W, Wang L, Gaischek I (2013) Acupressure at the Meridian Acupoint Xiyangguan (GB33) Influences Near-Infrared Spectroscopic Parameters (Regional Oxygen Saturation) in Deeper Tissue of the Knee in Healthy Volunteers. Evid Based Complement Alternat Med 2013:370341
Ten year follow-up study comparing conservative versus operative treatment of anterior cruciate ligament ruptures. A matched-pair analysis of high level athletes—PubMed. https://pubmed-ncbi-nlm-nih-gov.ezproxy.unibo.it/18603576/. Accessed 9 June 2022
Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS (2010) A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med 363(4):331–342
Treatment for acute anterior cruciate ligament tear: five year outcome of randomised trial—PubMed. https://pubmed-ncbi-nlm-nih-gov.ezproxy.unibo.it/23349407/. Accessed 9 June 2022
Peters Joanna Briggs Institute Reviewer’s Manual, JBI—Google Scholar. https://scholar-google-com.ezproxy.unibo.it/scholar_lookup?hl=en&publication_year=2020&author=MDJ+Peters&author=C+Godfrey&author=P+McInerney&author=Z+Munn&author=AC+Tricco&author=H+Khalil&title=Joanna+Briggs+Institute+Reviewer%27s+Manual%2C+JBI. Accessed 9 June 2022
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D et al (2018) PRISMA extension for scoping reviews (PRISMA-scR): checklist and explanation. Ann Intern Med 169(7):467–473
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Litscher G, Litscher D, Ofner M, Gaischek I, Malliga DE (2014) RegentK and physiotherapy-electrodermal mapping. Medicines 1(1):22–31
Ofner M, Strutzenberger G, Alexander N, Kastner A, Schwameder H (2017) RegentK improves the gait mechanics of patients with acute anterior cruciate ligament rupture immediately after application: clinical trial. Complement Med Res 24(2):90–96
Litscher G, Litscher D, Ofner M, Gaischek I, Malliga DE (2014) Temperature measurements in rehabilitation in patients with completely ruptured anterior cruciate ligament before and after regentK and physiotherapy. Medicines 1(1):12–21
Ofner M, Kastner A, Wallenboeck E, Pehn R, Schneider F, Groell R, Szolar D, Walach H, Litscher G, Sandner-Kiesling A (2014) Manual khalifa therapy improves functional and morphological outcome of patients with anterior cruciate ligament rupture in the knee: a randomized controlled trial. Evid Based Complement Alternat Med. https://doi.org/10.1155/2014/462840
Litscher G, Ofner M, Litscher D (2013) Manual khalifa therapy in patients with completely ruptured anterior cruciate ligament in the knee: first results from near-infrared spectroscopy. N Am J Med Sci 5(5):320–324
Ofner M, Kastner A, Schwarzl G, Schwameder H, Alexander N, Strutzenberger G et al (2018) RegentK and physiotherapy support knee function after anterior cruciate ligament rupture without surgery after 1 year: a randomized controlled trial. Complement Med Res 25(1):30–37
Morgan KD, Donnelly CJ, Reinbolt JA (2014) Elevated gastrocnemius forces compensate for decreased hamstrings forces during the weight-acceptance phase of single-leg jump landing: implications for anterior cruciate ligament injury risk. J Biomech 47(13):3295–3302
Cameron ID, Stafford B, Cumming RG, Birks C, Kurrle SE, Lockwood K et al (2000) Hip protectors improve falls self-efficacy. Age Ageing 29(1):57–62
Noël G, Verbruggen LA, Barbaix E, Duquet W (2000) Adding compression to mobilization in a rehabilitation program after knee surgery. A preliminary clinical observational study. Man Ther 5(2):102–107
A rationale for the treatment of back pain and joint pain by manual therapy—PubMed. https://pubmed-ncbi-nlm-nih-gov.ezproxy.unibo.it/1454864/. Accessed 26 June 2022
Eisenhart AW, Gaeta TJ, Yens DP (2003) Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries. J Am Osteopath Assoc 103(9):417–421
Lin I, Wiles L, Waller R, Goucke R, Nagree Y, Gibberd M et al (2020) What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med 54(2):79–86
Acknowledgements
The authors would like to thank Thomas Shelby for support in the early stages of the project.
Funding
Open access funding provided by Alma Mater Studiorum - Università di Bologna within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
Roberto Tedeschi proposed the revision project and identified the framework. Roberto Tedeschi and Federica Giorgi proposed the methodology. Roberto Tedeschi identified the research strategy. Federica Giorgi extracted and analyzed the data. Roberto Tedeschi and Federica Giorgi supervised the methodology. All authors conducted the revision and developed the first and subsequent drafts of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
R. Tedeschi and F. Giorgi declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information

Scan QR code & read article online
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tedeschi, R., Giorgi, F. What is known about the RegentK regenerative treatment for ruptured anterior cruciate ligament? A scoping review. Manuelle Medizin 61, 181–187 (2023). https://doi.org/10.1007/s00337-023-00953-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00337-023-00953-y