
Abstract
Background
18F-Fluorodeoxyglucose (FDG) PET/CT is emerging as a tool in the diagnosis and evaluation of pulmonary sarcoidosis, however, there is limited consensus regarding its diagnostic performance and prognostic value.
Method
A meta-analysis was conducted with PubMed, Science Direct, MEDLINE, Scopus, and CENTRAL databases searched up to and including September 2023. 1355 studies were screened, with seventeen (n = 708 patients) suitable based on their assessment of the diagnostic performance or prognostic value of FDG-PET/CT. Study quality was assessed using the QUADAS-2 tool. Forest plots of pooled sensitivity and specificity were generated to assess diagnostic performance. Pooled changes in SUVmax were correlated with changes in pulmonary function tests (PFT).
Results
FDG-PET/CT in diagnosing suspected pulmonary sarcoidosis (six studies, n = 400) had a pooled sensitivity of 0.971 (95%CI 0.909–1.000, p = < 0.001) and specificity of 0.873 (95%CI 0.845–0.920)(one study, n = 169). Eleven studies for prognostic analysis (n = 308) indicated a pooled reduction in pulmonary SUVmax of 4.538 (95%CI 5.653–3.453, p = < 0.001) post-treatment. PFTs displayed improvement post-treatment with a percentage increase in predicted forced vital capacity (FVC) and diffusion capacity of the lung for carbon monoxide (DLCO) of 7.346% (95%CI 2.257–12.436, p = 0.005) and 3.464% (95%CI -0.205–7.132, p = 0.064), respectively. Reduction in SUVmax correlated significantly with FVC (r = 0.644, p < 0.001) and DLCO (r = 0.582, p < 0.001) improvement.
Conclusion
In cases of suspected pulmonary sarcoidosis, FDG-PET/CT demonstrated good diagnostic performance and correlated with functional health scores. FDG-PET/CT may help to guide immunosuppression in cases of complex sarcoidosis or where treatment rationalisation is needed.
Clinical relevance statement
FDG-PET/CT has demonstrated a high diagnostic performance in the evaluation of suspected pulmonary sarcoidosis with radiologically assessed disease activity correlating strongly with clinically derived pulmonary function tests.
Key Points
-
In diagnosing pulmonary sarcoidosis, FDG-PET/CT had a sensitivity and specificity of 0.971 and 0.873, respectively.
-
Disease activity, as determined by SUVmax, reduced following treatment in all the included studies.
-
Reduction in SUVmax correlated with an improvement in functional vital capacity, Diffusion Capacity of the Lungs for Carbon Monoxide, and subjective health scoring systems.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
Sarcoidosis is a multisystem inflammatory disease characterised by the growth of non-necrotising granulomas that can accumulate in virtually any organ in the body. The aetiology of the disease remains poorly understood, with a highly variable clinical course. It is estimated to occur in roughly 2 to 160 people per 100,000, with a varied geographic prevalence likely due to a combination of environmental factors and genetic susceptibility [1, 2]. Thoracic involvement affecting the mediastinal lymph nodes and lung parenchyma is the most common disease manifestation. Indeed, symptoms related to this are often the cause of the first presentation. Approximately 60 to 70% with pulmonary disease will see spontaneous resolution of symptoms before any intervention is implemented [3]. However, for patients where the disease persists, severity can range from asymptomatic nodal involvement to a progressive fibrotic process leading to eventual respiratory failure that is difficult to treat [4]. For this reason, the accurate and timely diagnosis of subclinical but active pulmonary sarcoidosis is important.
At present, the diagnosis of sarcoidosis is not standardized but is generally accepted based on three major criteria: (i) a clinically compatible picture with pathognomonic features, (ii) radiological evidence and (iii) a histological specimen demonstrating non-necrotising granulomatous disease [5]. The diverse spectrum of clinical presentations can make the diagnosis of sarcoidosis challenging for clinicians, particularly when disease activity can vary, and conventional markers are often inconclusive. CT is the standard diagnostic imaging test, with appearances ranging from an almost pathognomonic pattern of mediastinal and hilar nodal enlargement to more nonspecific nodal and pulmonary changes requiring further investigation [6]. Therefore, histological evidence is typically needed establish the final diagnosis.
Fluoro-2-deoxyglucose-18 (FDG) positron emission tomography (PET/CT) has emerged as a sensitive method of detecting sites of inflammation, sometimes before morphological changes are visible on anatomical imaging [7]. FDG PET/CT has an established role in cardiac sarcoidosis diagnosis and assessment of disease activity [8]. It is unclear at present, how FDG PET/CT correlates with pulmonary involvement, lung function and treatment response. To date, no meta-analysis or systematic literature review has been published on this topic. The aim of this meta-analysis of the current literature was to (i) assess the diagnostic performance of FDG-PET/CT for patients with suspected pulmonary sarcoidosis and (ii) determine the correlation between FDG-PET/CT and other clinically relevant biomarkers.
Materials and Methods
Data sources and literature search
PubMed, Science Direct, MEDLINE, Scopus, and CENTRAL databases were searched from inception until the end of September 2023 (R.D. and M.McD.). Studies evaluating the diagnostic performance and/or prognostic value of F-18 FDG PET for pulmonary sarcoidosis in association with clinical markers of lung function were the focus of our literary review. Studies meeting the criteria for pulmonary sarcoidosis were defined as those involving sarcoidosis impacting both the lung parenchyma and the mediastinal nodes. Search terms were kept purposely vague to capture as many studies as possible and avoid excluding patients with concomitant cardiac, pulmonary and/or systemic sarcoidosis involvement:
“Positron Emission Tomography Computed Tomography”[Mesh] OR “Positron-Emission Tomography”[Mesh]) AND “Fluorodeoxyglucose F18”[Mesh]) AND “Sarcoidosis”[Mesh].
Study selection
Search results were entered into the systematic review software Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). Duplicates were automatically removed by the Covidence software, and eligibility assessment was performed independently by two physicians (R.D. and M.McD.). Study titles were initially reviewed separately for inclusion, and any differences in physician decision were resolved by consensus discussion. Studies which did not present original data were excluded. In addition, small group case reports, review articles, books, opinion pieces and editorials were excluded. Literature was excluded if it was not published in English. Once initial title screening was performed, studies were retrieved for review and assessed further based on the details of their abstract and the eligibility criteria that we have outlined below.
Diagnostic eligibility criteria and data extraction
All studies considered for inclusion in the diagnostic subgroup were required to assess histologically proven de-novo sarcoidosis patients prior to commencement of therapy. Patients were also accepted for inclusion if they were deemed to have sarcoidosis based on the American Thoracic Society/European Respiratory Society/World Association for Sarcoidosis and Other Granulomatosis Disorders (ATS/ERS/WASOG) criteria [5] (See Supplementary appendix). Publications which did not identify the presence of pulmonary sarcoidosis or used non-FDG PET tracers were excluded. Studies were examined and datapoints relating to the diagnostic accuracy of FDG-PET/CT including true positive/true negative/false positive/false negative or relevant sensitivity and specificity, were recorded, and tabulated.
Prognostic study eligibility criteria and data extraction
All studies considered for inclusion in the prognostic subgroup were required to assess either histologically proven sarcoidosis or clinically diagnosed sarcoid according to the ATS/ERS/WASOG criteria [5]. Radiological assessment was performed via FDG-PET/CT, excluding non-FDG-PET/CT tracers. Studies were required to perform a comparative assessment of disease severity through either serial FDG-PET/CTs or reassessment of functional scores following treatment. Semi-quantitative measurements of metabolic activity (maximum standardized uptake value, SUVmax) in lung parenchyma and/or mediastinal stations were recorded. No exclusion was placed on the time since initial sarcoid diagnosis, or the type/duration of treatments received. Corresponding functional scores such as FVC and DLCO at the start and completion of treatment were recorded and correlated with initial disease severity as assessed radiologically.
Quality and risk of bias assessment
Risk of bias assessment was carried out using the QUADAS-2 tool [9]. Two physicians performed this process independently and were blinded to each other’s evaluation. A structured list of ‘low concern’, ‘some concern’ and ‘high concern’ for risk of bias was generated in four main domains. Items included patient selection, index test used, reference standard, flow, and timing. When a full review was performed, any discrepancies in the risk of bias assessment were resolved via discussion. Results of this were then graphically displayed using the publicly available RobVis software [10].
Statistical analysis
Diagnostic subgroup analysis
The diagnostic performance as declared in the 6 included studies was used to generate a pooled forest plot of sensitivity scores. A result for specificity was calculated from the 1 eligible study. Descriptive statistics including positive likelihood ratio (LR + ) and diagnostic odds ratio (DOR) were generated from these values. Statistical analysis was done using Excel (Microsoft Corp.) and SPSS 29.0.1.0 (IBM Corp.).
Prognostic subgroup analysis
SUVmax before and after treatment were recorded. A reduction in SUVmax was used as an indicator of disease response. All the recorded SUVmax scores were derived from published values in the mediastinum or lung parenchyma. The change in SUVmax (⍙SUVmax) following treatment in both the lung parenchyma and mediastinal stations was correlated with the change in functional vital capacity (⍙ FVC) and the diffusing capacity of the lung for carbon monoxide (⍙ DLCO). Pulmonary function scores were all reported as mean change in the percentage of predicted FVC or DLCO. Forest and funnel plots generated to assess the mean pooled effect size of SUVmax, FVC and DLCO. Radiological response to treatment, as assessed by SUVmax, was correlated with the change in pulmonary function using Pearson’s Coefficient (r). An r value of < 0.29 was scored as a weak correlation, 0.30–0.49 as a moderate correlation, and 0.50–1.00 as a strong correlation. In studies where discrete SUVmax and pulmonary function scores were provided for individual patients, a scatter plot relating discrete ⍙SUVmax to ⍙ FVC and ⍙ DLCO was created along with a line of best fit.
Quality-of-life analysis
Studies which provided quality-of-life (QOL) assessment scores were recorded along with mean standard deviation (SD). Short Form Health Survey Questionnaire (SF-36) mean scores were compared across studies and a mean change of > 10 was deemed significant. Statistical analysis was performed using Excel (Microsoft Corp.) and SPSS 29.0.1.0 (IBM Corp.).
Results
Literature search and selection of studies
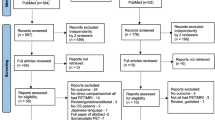
In total, 1355 studies were screened, with 63 deemed eligible for full text review following initial title and abstract screening. In total, 17 studies were deemed appropriate for inclusion. (Fig. 1) Study exclusion following full-text review were due to several reasons including study design, patient cohort and inadequate information relating to pulmonary sarcoidosis. The diagnostic subgroup analysis included 6 studies (Table 1) [11,12,13,14,15,16]. 11 studies were included in the prognostic section analysis (Table 2) [17,18,19,20,21,22,23,24,25,26,27,28].

Flow chart of the search for eligible studies on the diagnostic and prognostic performance of [18F]FDG-PET/CT or PET/CT for pulmonary sarcoidosis. Publication search concluded with 6 studies included for diagnostic subgroup analysis and 11 studies included for prognostic subgroup analysis
Utility of FDG-PET/CT in diagnosis of sarcoidosis
In the diagnostic subgroup, 6 studies evaluating 400 confirmed sarcoidosis patients were included. There was radiologically proven pulmonary involvement in 392 (95%) of the included patients with 54% males and a mean age of 44.7 years (Table 3). The majority of included studies examined patients with histologically proven de-novo sarcoidosis prior to the commencement of treatment. In the case of Lovinfosse and Nishiyama, an unspecified minority of patients were diagnosed as sarcoidosis based on the ATS/ERS/WASOG criteria [5, 11, 29]. The QUADAS-2 assessment demonstrated some concerns for bias and applicability for the included studies (Supplemental Figs. 1, 2). Bias due to lack of physician blinding to clinical details was deemed to be the greatest area of concern.
The sensitivity of FDG-PET/CT for the diagnosis of pulmonary sarcoidosis was 0.971 (95%CI 0.909–1.000, p = < 0.001) (Fig. 2). A single study reported a specificity of FDG-PET/CT in correctly differentiating pulmonary sarcoidosis from lymphoma (n = 169) of 0.873 (95%CI 0.845–0.920). The diagnostic odds ratio (DOR) and positive likelihood ratio (LR + ) was 223.57 (95%CI 111.64–447.71) and 7.646 (95%CI 5.70–10.00), respectively. The statistical heterogeneity as, reported by univariate I2 value, was 0.00 for the sensitivity forest plot.

Forest plot demonstrating the observed pooled FDG-PET/CT sensitivity (n = 400) in detecting active pulmonary sarcoidosis. The overall effect size generated for the pooled study was 0.971 (Std. Error 0.0316, p = < 0.001, 95%CI 0.909–1.000). A heterogeneity score (I2) of 0.00 was generated for this plot
Utility of FDG-PET/CT in prognostic evaluation of sarcoidosis
A total of 11 studies evaluating 308 patients with confirmed sarcoidosis were included in the prognostic subgroup analysis. Radiologically evidence of pulmonary sarcoidosis was identified in 79% (n = 243) of the included population (Tables 2, 3). Of the included patients, 86% were histologically proven, with the remaining being diagnosed via ATS/ERS/WASOG criteria. Patients were distributed across radiographic Scadding Stages, with a total of 11, 71, 94, 59 and 46 classified as Stage 0, I, II, III and IV, respectively. Over 50% of the included patients were treated with glucocorticoid therapy as part of monotherapy, or in combination with other therapies such as methotrexate and hydroxychloroquine. In 36% of cases, patients were treated with infliximab or a biosimilar. Duration of treatment or previous failed treatments were not reported. The QUADAS-2 assessment demonstrated low concern for potential bias and applicability in the 11 included studies (Supplemental Figs. 3, 4).
Results of the reported change in SUVmax and pulmonary function are shown in Table 4. A reduction in SUVmax was noted across all the included studies following treatment. Reduction in lung parenchymal and mediastinal station SUVmax as generated by pooled forest and funnel plots were 4.538 (95%CI 5.653–3.453, p < 0.001) (Fig. 3, Supplemental Fig. 5) and 3.490 (95% CI 2.446–4.535, p < 0.001) (Supplemental Fig. 6), respectively. Pulmonary function improved following treatment; a pooled value for the percentage of predicted FVC and DLCO were 7.346% (95%CI 2.257–12.436, p = 0.005) and 3.464% (95%CI 0.205–7.132, p = 0.064), respectively (Table 4, Figs. 4/5). Heterogeneity I2 value remained low for all plots, with the highest reported value being 0.26 (Fig. 3). Reduction in lung parenchymal SUVmax strongly correlates with improvement in FVC (r = 0.644, p < 0.001) and DLCO (r = 0.582, p < 0.001) (Supplemental 7, 9). Scatter plots were generated for eligible studies but failed to identify a strong correlation in the case of FVC (n = 46, r = 0.005) or the DLCO (n = 45, r = 0.08) (Supplemental Figs. 8, 10).

Forest plot demonstrating the observed pooled average ⍙SUVmax (n = 259) following completion of treatment from baseline FDG-PET/CT imaging. The pooled observed reduction in SUVmax was 4.54 (95%CI 3.42–5.65). A heterogeneity score (I2) of 0.26 was generated for this plot

Forest plot demonstrating the observed pooled average ⍙FVC (n = 207) following completion of treatment from baseline FDG-PET/CT imaging. ⍙FVC values represent percentage of predicted FVC for each individual. The pooled observed increase in FVC was 7.35% (95%CI 2.26–12.44). A heterogeneity score (I2) of 0.00 was generated for this plot

Forest plot demonstrating the observed pooled average ⍙DLCO (n = 207) following completion of treatment from baseline FDG-PET/CT imaging. ⍙DLCO values represent the percentage of predicted DLCO for each individual. The pooled observed increase in FVC was 3.46% (95%CI −0.20–7.13). A heterogeneity score (I2) of 0.06 was generated for this plot
Quality-of-Life Analysis
Of the 17 studies, 4 included a QOL assessment by virtue of a patient-answered questionnaire. The Short Form Health Survey Questionnaire (SF-36) was utilised by 2 studies showing a mean improvement in the respondents subjective scoring (mean 47.15 vs. 37.95, p = > 0.05) as per supplemental Table 2. The Sarcoidosis Health Questionnaire (SHQ) was used by 1 study showing no change following treatment. Keijsers reported a binary symptom improvement in 10 of 12 patients following treatment [26]. Overall, QOL indicators as assessed by subjective health scoring systems improved in 75% of the studies assessed (four studies, n = 116).
Discussion
There is little consensus about the role of FDG-PET/CT in pulmonary sarcoidosis [30]. Our aim with this meta-analysis was to provide evidence-based data addressing how functional health outcomes relate to disease activity, as determined by FDG-PET/CT. In addition, we sought to define the diagnostic performance of FDG-PET/CT in cases of suspected pulmonary sarcoidosis [30].
FDG-PET/CT had a sensitivity and specificity of 0.97 and 0.87 in confirming suspected pulmonary sarcoidosis, consistent with those reported in prior literature [14, 30]. There was satisfactory agreement across the included studies with low heterogeneity. Distinguishing malignancy from inflammation on FDG-PET/CT is challenging due to the lack of specificity of FDG as a radiotracer. However, most published literature does not evaluate FDG-PET/CT’s false positive rate, making this difficult to quantify. Lovinfosse assessed the ability of four radiologists to correctly identify pulmonary sarcoidosis on FDG-PET/CT in 420 patients with hypermetabolic thoracic lymph nodes, including sarcoidosis and lymphoma (DLBCL and HL), reporting a specificity of 0.873 [29]. This suggests that FDG-PET/CT may reliably diagnose cases of suspected pulmonary sarcoidosis. There are limitations in the interpretation of a non-dedicated study for confirmation of diagnosis, and selection bias may affect the accuracy of this result. Given that FDG-PET/CT is a relatively source-constrained imaging modality, patients being considered would likely have a higher pre-test probability.
We decided to use SUVmax in assessing PET response to physician-chosen therapy and ultimate functional response. SUVmax is the most commonly used semiquantitative measurement of tracer avidity in a target lesion in clinical PET. It is based on the highest voxel signal intensity within a measured volume and can be affected by various factors including body weight, pharmacodynamics, radiotracer dose, uptake time, scanner type, reconstruction algorithm and acquisition time [31]. Despite its limitations, it remains the most commonly used semiquantitative measurement in clinical PET and has been shown to be a useful disease biomarker in the cardiac sarcoid literature [32]. Our results suggest that SUVmax is an independent variable that changes with treatment. All included studies reported a decrease in SUVmax from baseline, suggesting that it may be a useful imaging biomarker in the assessment of pulmonary sarcoid disease activity following treatment.
When we examined PFT change following treatment, there was an improvement in the percentage of predicted FVC and DLCO by 7.346% and 3.464%, respectively. FVC has long been considered an important functional marker of sarcoidosis disease activity. A decline in FVC, regardless of the objective amount, has been shown to correlate with a relapse or poor response to treatment [33]. However, an ongoing issue with using PFTs to guide treatment is that they do not declare reversible disease and can potentially misclassify efficacious treatments by virtue of their disease phenotype [34]. Moreover, PFTs represent an effort-dependent assessment prone to suboptimal results when patient cooperation and understanding is not achieved. All FDG-PET/CT included studies reported a reduction in SUVmax following treatment. This decrease was associated with an improvement in their functional scores, indicating that FDG-PET/CT observed treatment response may correlate with an improvement in functional health scores. This demonstrates the potential utility of FDG-PET/CT-derived markers of disease severity in cases where uncertainty exists over the reversibility of parenchymal inflammation. In addition, the significant functional improvement in these patients demonstrates the importance of prompt and appropriate treatment to avoid fibrotic transformation in the setting of inflammation [35].
Future studies examining of the role of FDG-PET/CT in sarcoidosis treatment response assessment could be explored using normalised FDG uptake scoring systems (e.g. Deauville in lymphoma and Hopkins’ criteria in lung cancer), allowing for a more reproducible comparison of disease activity [36, 37]. Volumetric PET methods may also provide a more comprehensive lung evaluation. Total lung glycolysis provides a volumetric measurement of regional lung activity [19, 38]. This is yet to be clearly defined and future study is necessary to establish the most accurate PET marker of lung disease progression [19].
In this meta-analysis, we sought to compare PET and functional disease response to patient quality of life scoring systems. In absence of any definitive severity scoring system, patient reported symptom burden remains an important marker of disease remission and relapse. In cases where there was recorded patient response, results were generally positive with 3 of 4 eligible studies demonstrating improvement in patient QOL scores. This may indicate an association between QOL indicators and radiologically observed disease activity which warrants further review.
While the findings of this meta-analysis point to a potential role for FDG-PET/CT in pulmonary sarcoid, it is important to recognise that this is likely beneficial only in selected cases. To our knowledge, no studies have demonstrated a comparative benefit of FDG-PET/CT over the standard CT diagnostic pathway. Indeed, routine CT Thorax with contrast has demonstrated comparable performance to FDG-PET/CT in the cases of stage I/II sarcoidosis—which constitutes the majority in our study cohort. FDG-PET/CT is likely be of most incremental benefit in assessing complex or advanced pulmonary sarcoid (Stage III/IV). However, studies have not yet confirmed its efficacy in this context [39]. Access to PET/CT is another consideration, given the significant differences in availability globally [40]. Future research would be beneficial to define the role of FDG-PET/CT in this particular patient cohort.
Limitations
Few of the included studies examined QOL indicators in a comprehensive manner allowing for statistical correlation with radiologically assessed disease activity. With a more comprehensive review of symptom burden with standardized questionnaires (e.g. SF-36, SHQ), it may be possible to elucidate more nuanced associations between the location of disease and symptomatology [41].
Patients with established fibrotic versus non-fibrotic sarcoidosis were not clearly defined in this publication. This could have implications on the prognostic improvement that could be expected with immunosuppressive treatment if fibrotic transformation has already taken place. Moreover, the rate of PET/CT defined remission/recurrence following treatment remains poorly understood, with one low-volume study quoting a reduced recurrence in PET/CT responders (14.2% vs 61.5%, n = 10) [15]. Further research is needed to examine this relationship.
Conclusion
FDG-PET/CT has a good diagnostic performance in cases of suspected pulmonary sarcoidosis. FDG-PET/CT variables including relative change in SUVmax appear to correlate with an improvement in pulmonary function. FDG-PET/CT may be a useful adjunct to guide immunosuppression in cases of complex sarcoidosis or where treatment rationalisation is needed.
Abbreviations
- ATS/ERS/WASOG:
-
American Thoracic Society/European Respiratory Society/World Association for Sarcoidosis and Other Granulomatosis Disorders criteria
- DLCO:
-
Diffusion Capacity of the Lungs for Carbon Monoxide
- FDG PET/CT:
-
Fluoro-2-deoxyglucose-18 positron emission tomography
- FVC:
-
Functional vital capacity
- PFT:
-
Pulmonary function test
- QOL:
-
Quality-of-Life
- SD:
-
Standard Deviation
- SUVmax:
-
Standard uptake value maximum
References
Belperio JA, Shaikh F, Abtin FG et al (2022) Diagnosis and treatment of pulmonary sarcoidosis. JAMA 327:856. https://doi.org/10.1001/jama.2022.1570
Fidler LM, Balter M, Fisher JH, To T, Stanbrook MB, Gershon A (2019) Epidemiology and health outcomes of sarcoidosis in a universal healthcare population: a cohort study. Eur Respir J 54:1900444. https://doi.org/10.1183/13993003.00444-2019
Costabel U (2001) Sarcoidosis: clinical update. Eur Respir J 18:56S LP–68SS LP. https://doi.org/10.1183/09031936.01.18s320056
Ramachandraiah V, Aronow W, Chandy D (2017) Pulmonary sarcoidosis: an update. Postgrad Med 129:149–158. https://doi.org/10.1080/00325481.2017.1251818
Crouser ED, Maier LA, Wilson KC et al (2020) Diagnosis and detection of sarcoidosis. an official american thoracic society clinical practice guideline. Am J Respir Crit Care Med 201:e26–e51. https://doi.org/10.1164/rccm.202002-0251ST
Dhagat PK, Singh S, Jain M, Singh SN, Sharma RK (2017) Thoracic sarcoidosis: imaging with high resolution computed tomography. J Clin Diagn Res 11:TC15–TC18. https://doi.org/10.7860/JCDR/2017/24165.9459
Popević S, Šumarac Z, Jovanović D et al (2016) Verifying sarcoidosis activity: chitotriosidase versus ACE in sarcoidosis - a case-control study. J Med Biochem 35:390–400. https://doi.org/10.1515/jomb-2016-0017
Chareonthaitawee P, Beanlands RS, Chen W et al (2017) Joint SNMMI-ASNC expert consensus document on the role of 18F-FDG PET/CT in cardiac sarcoid detection and therapy monitoring. J Nucl Med 58:1341–1353. https://doi.org/10.2967/jnumed.117.196287
Whiting PF, Rutjes AWS, Westwood ME et al (2011) QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 155:529–536. https://doi.org/10.7326/0003-4819-155-8-201110180-00009
McGuinness LA, Higgins JPT (2021) Risk‐of‐bias VISualization (robvis): an R package and Shiny web app for visualizing risk‐of‐bias assessments. Res Synth Methods 12:55–61. https://doi.org/10.1002/jrsm.1411
Nishiyama Y, Yamamoto Y, Fukunaga K et al (2006) Comparative evaluation of 18F-FDG PET and 67Ga scintigraphy in patients with sarcoidosis. J Nucl Med 47:1571–1576. http://www.ncbi.nlm.nih.gov/pubmed/17015889
Keijsers RG, Grutters JC, van Velzen-Blad H, van den Bosch JM, Oyen WJ, Verzijlbergen FJ (2010) 18F-FDG PET patterns and BAL cell profiles in pulmonary sarcoidosis. Eur J Nucl Med Mol Imaging 37:1181–1188. https://doi.org/10.1007/s00259-009-1376-6
Keijsers RG, Verzijlbergen FJ, Oyen WJ et al (2009) 18F-FDG PET, genotype-corrected ACE and sIL-2R in newly diagnosed sarcoidosis. Eur J Nucl Med Mol Imaging 36:1131–1137. https://doi.org/10.1007/s00259-009-1097-x
Braun JJ, Kessler R, Constantinesco A, Imperiale A (2008) 18F-FDG PET/CT in sarcoidosis management: review and report of 20 cases. Eur J Nucl Med Mol Imaging 35:1537–1543. https://doi.org/10.1007/s00259-008-0770-9
Maturu VN, Agarwal R, Aggarwal AN et al (2014) Dual-time point whole-body 18 F-fluorodeoxyglucose PET/CT imaging in undiagnosed mediastinal lymphadenopathy. Chest 146:e216–e220. https://doi.org/10.1378/chest.14-1827
Lovinfosse P, Ferreira M, Withofs N et al (2022) Distinction of lymphoma from sarcoidosis on 18 F-FDG PET/CT: evaluation of radiomics-feature–guided machine learning versus human reader performance. J Nucl Med 63:1933–1940. https://doi.org/10.2967/jnumed.121.263598
Yakar A, Yakar F, Sezer M et al (2015) Use of PET-CT for the assessment of treatment results in patients with sarcoidosis. Wien Klin Wochenschr 127:274–282. https://doi.org/10.1007/s00508-014-0647-9
Vorselaars ADM, Crommelin HA, Deneer VHM et al (2015) Effectiveness of infliximab in refractory FDG PET-positive sarcoidosis. Eur Respir J 46:175–185. https://doi.org/10.1183/09031936.00227014
Schimmelpennink MC, Vorselaars ADM, Veltkamp M, Keijsers RGM (2019) Quantification of pulmonary disease activity in sarcoidosis measured with 18F-FDG PET/CT: SUVmax versus total lung glycolysis. EJNMMI Res 9:54. https://doi.org/10.1186/s13550-019-0505-x
Schimmelpennink MC, Vorselaars ADM, van Beek FT et al (2018) Efficacy and safety of infliximab biosimilar Inflectra® in severe sarcoidosis. Respir Med 138:S7–S13. https://doi.org/10.1016/j.rmed.2018.02.009
Mostard RLM, Verschakelen JA, Van Kroonenburgh MJPG et al (2013) Severity of pulmonary involvement and 18F-FDG PET activity in sarcoidosis. Respir Med 107:439–447. https://doi.org/10.1016/j.rmed.2012.11.011
Sobic-Saranovic DP, Grozdic IT, Videnovic-Ivanov J et al (2013) Responsiveness of FDG PET/CT to treatment of patients with active chronic sarcoidosis. Clin Nucl Med 38:516–521. https://doi.org/10.1097/RLU.0b013e31828731f5
Milman N, Graudal N, Loft A, Mortensen J, Larsen J, Baslund B (2012) Effect of the TNF-α inhibitor adalimumab in patients with recalcitrant sarcoidosis: a prospective observational study using FDG-PET. Clin Respir J 6:238–247. https://doi.org/10.1111/j.1752-699X.2011.00276.x
Maturu VN, Rayamajhi SJ, Agarwal R, Aggarwal AN, Gupta D, Mittal BR (2016) Role of serial F-18 FDG PET/CT scans in assessing treatment response and predicting relapses in patients with symptomatic sarcoidosis. Sarcoidosis Vasc Diffus Lung Dis 33:372–380
Keijsers RG, Verzijlbergen EJ, van den Bosch JM et al (2011) 18F-FDG PET as a predictor of pulmonary function in sarcoidosis. Sarcoidosis Vasc Diffus Lung Dis 28:123–129. http://www.ncbi.nlm.nih.gov/pubmed/22117503
Keijsers RGM, Verzijlbergen JF, Van Diepen DM, van den Bosch JMM, Grutters JC (2008) 18F-FDG PET in sarcoidosis: an observational study in 12 patients treated with Infliximab. Sarcoidosis Vasc Diffus Lung Dis 25:143–150
Chen H, Jin R, Wang Y, Li L, Li K, He Y (2018) The utility of 18F-FDG PET/CT for monitoring response and predicting prognosis after glucocorticoids therapy for sarcoidosis. Biomed Res Int 2018:1823710. https://doi.org/10.1155/2018/1823710
Umeda Y, Demura Y, Morikawa M et al (2011) Prognostic value of dual‐time‐point 18F‐fluorodeoxyglucose positron emission tomography in patients with pulmonary sarcoidosis. Respirology 16:713–720. https://doi.org/10.1111/j.1440-1843.2011.01966.x
Lovinfosse P, Ferreira M, Withofs N et al (2022) Distinction of lymphoma from sarcoidosis on 18F-FDG PET/CT: evaluation of radiomics-feature guided machine learning versus human reader performance. J Nucl Med 63:1933–1940. https://doi.org/10.2967/jnumed.121.263598
Vender RJ, Aldahham H, Gupta R (2022) The role of PET in the management of sarcoidosis. Curr Opin Pulm Med 28:485–491. https://doi.org/10.1097/MCP.0000000000000892
Adams MC, Turkington TG, Wilson JM, Wong TZ (2010) A systematic review of the factors affecting accuracy of SUV measurements. AJR Am J Roentgenol 195:310–320. https://doi.org/10.2214/AJR.10.4923
Subramanian M, Swapna N, Ali AZ et al (2021) Pre-treatment myocardial 18FDG uptake predicts response to immunosuppression in patients with cardiac sarcoidosis. JACC Cardiovasc Imaging 14:2008–2016. https://doi.org/10.1016/j.jcmg.2020.11.016
Korsten P, Strohmayer K, Baughman RP, Sweiss NJ (2016) Refractory pulmonary sarcoidosis. Clin Pulm Med 23:67–75. https://doi.org/10.1097/CPM.0000000000000136
Obi ON (2023) Pulmonary sarcoidosis: beyond restriction and forced vital capacity Ann Am Thorac Soc 20:24–26. https://doi.org/10.1513/AnnalsATS.202208-731ED
Bonham CA, Strek ME, Patterson KC (2016) From granuloma to fibrosis: sarcoidosis associated pulmonary fibrosis. Curr Opin Pulm Med 22:484–491. https://doi.org/10.1097/MCP.0000000000000301
Kinahan PE, Fletcher JW (2010) Positron emission tomography-computed tomography standardized uptake values in clinical practice and assessing response to therapy. Semin Ultrasound CT MR 31:496–505. https://doi.org/10.1053/j.sult.2010.10.001
Sarikaya I, Albatineh AN, Sarikaya A (2020) Revisiting Weight-Normalized SUV and Lean-Body-Mass–Normalized SUV in PET Studies. J Nucl Med Technol 48:163–167. https://doi.org/10.2967/jnmt.119.233353
Zhang P, Chen W, Zhao K et al (2023) Tumor to liver maximum standardized uptake value ratio of FDG-PET/CT parameters predicts tumor treatment response and survival of stage III non-small cell lung cancer. BMC Med Imaging 23:107. https://doi.org/10.1186/s12880-023-01067-6
Keijsers RGM, Grutters JC (2020) In Which Patients with Sarcoidosis Is FDG PET/CT Indicated? J Clin Med 9:890. https://doi.org/10.3390/jcm9030890
Park J, Chang KJ, Seo YS et al (2014) Tumor SUVmax Normalized to Liver Uptake on (18)F-FDG PET/CT Predicts the Pathologic Complete Response After Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Nucl Med Mol Imaging 48:295–302. https://doi.org/10.1007/s13139-014-0289-x
Hendrick DJ, Blackwood RA, Black JM (1976) Chest pain in the presentation of sarcoidosis. Br J Dis Chest 70:206–210. https://doi.org/10.1016/0007-0971(76)90030-9
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Guarantor
The specific guarantor of this publication is Dr David J Murphy.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Not applicable
Ethical approval
Institutional Review Board approval was not required because this study was a meta-analysis of published works.
Study subjects or cohorts overlap
None
Methodology
-
Meta-analysis
Additional information
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Donnelly, R., McDermott, M., McManus, G. et al. Meta-analysis of [18F]FDG-PET/CT in pulmonary sarcoidosis. Eur Radiol (2024). https://doi.org/10.1007/s00330-024-10949-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00330-024-10949-4