
Abstract
Objective
To assess whether anthropometrics, clinical risk factors, and coronary artery calcium score (CACS) can predict the need of further testing after coronary CT angiography (CTA) due to non-diagnostic image quality and/or the presence of significant stenosis.
Methods
Consecutive patients who underwent coronary CTA due to suspected coronary artery disease (CAD) were included in our retrospective analysis. We used multivariate logistic regression and receiver operating characteristics analysis containing anthropometric factors: body mass index, heart rate, and rhythm irregularity (model 1); and parameters used for pre-test likelihood estimation: age, sex, and type of angina (model 2); and also added total calcium score (model 3) to predict downstream testing.
Results
We analyzed 4120 (45.7% female, 57.9 ± 12.1 years) patients. Model 3 significantly outperformed models 1 and 2 (area under the curve, 0.84 [95% CI 0.83–0.86] vs. 0.56 [95% CI 0.54–0.58] and 0.72 [95% CI 0.70–0.74], p < 0.001). For patients with sinus rhythm of 50 bpm, in case of non-specific angina, CACS above 435, 756, and 944; in atypical angina CACS above 381, 702, and 890; and in typical angina CACS above 316, 636, and 824 correspond to 50%, 80%, and 90% probability of further testing, respectively. However, higher heart rates and arrhythmias significantly decrease these cutoffs (p < 0.001).
Conclusion
CACS significantly increases the ability to identify patients in whom deferral from coronary CTA may be advised as CTA does not lead to a final decision regarding CAD management. Our results provide individualized cutoff values for given probabilities of the need of additional testing, which may facilitate personalized decision-making to perform or defer coronary CTA.
Key Points
• Anthropometric parameters on their own are insufficient predictors of downstream testing. Adding parameters of the Diamond and Forrester pre-test likelihood test significantly increases the power of prediction.
• Total CACS is the most important independent predictor to identify patients in whom coronary CTA may not be recommended as CTA does not lead to a final decision regarding CAD management.
• We determined specific CACS cutoff values based on the probability of downstream testing by angina-, arrhythmia-, and heart rate–based groups of patients to help individualize patient management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronary CT angiography (CTA) is a gatekeeper to rule out significant coronary artery stenosis, due to its high sensitivity and negative predictive value [1,2,3]. In the 2019 European Society of Cardiology Guideline for the diagnosis and management of chronic coronary syndromes, coronary CTA has a class I recommendation as the initial test for symptomatic patients in whom obstructive coronary artery disease (CAD) cannot be clinically excluded [4]. However, in case of irregular heart rate, significant obesity, or inadequate breath-hold, coronary CTA is not suggested since sufficient image quality (IQ) may not be reached (class III recommendation) [4]. Exact cutoff values for clinical factors potentially prohibiting sufficient evaluation of CAD using coronary CTA are scarce. Furthermore, in case of increasing likelihood of obstructive CAD, coronary CTA may not be the ideal choice due to the high pre-test probability of significant CAD [5,6,7,8,9]. However, there is limited information regarding patient characteristics in whom alternative diagnostic test should be applied instead of coronary CTA because of high probability of significant stenosis or foreseeable insufficient IQ of CTA [4].
Coronary calcium score (CACS) correlates with the presence of obstructive CAD and may also identify extensive calcifications, which may further hamper CTA analysis, due to partial volume effects and blooming artifacts [10,11,12]. However, there is minimal data on whether calcium score values may predict inadequate IQ of coronary CTA.
Therefore, we aimed to assess whether anthropometrics, parameters of the Diamond and Forrester pre-test likelihood test, and CACS can predict the need of further testing after coronary CTA [13]. Further, we wished to provide CACS cutoff values for given probabilities of downstream testing following coronary CTA.
Materials and methods
Study participants
We retrospectively included patients who underwent coronary CTA in our Institution between April of 2016 and September of 2019 and who were reported in a structured reporting platform (Axis, Neumann Medical Ltd.) with all required clinical, anthropometric, and imaging data allowing convenient export and analysis of the data. In order to study only patients with suspected CAD, those with prior invasive or non-invasive testing for CAD were excluded from our analysis. We also excluded those who came for CTA of the left atrium and pulmonary veins before atrial ablation therapy; patients under 18 years; those with congenital or structural heart disease; those who underwent open heart surgery or transcatheter valve implantation, or pacemaker implantation; or those in whom evaluation of the CTA scans was not possible due to technical issues such as extravasation of contrast medium. Clinical characteristics and cardiovascular risk factors were obtained by standardized questionnaires before examination.
CACS measurement and coronary CTA scan protocol
Coronary CACS and CTA examinations were performed on a 256-slice scanner (Brilliance iCT 256, Philips Healthcare) with prospective ECG-triggered axial acquisition mode. For CACS, we used 120-kV tube voltage with 30–50-mAs tube current, and for coronary CTA 100–120 kV with 200–300-mAs tube current depending on patient anthropometrics. Image acquisition was performed with 128 × 0.625-mm detector collimation, and 270-ms gantry rotation time. For heart rate control, a maximum of 50–100 mg metoprolol was given orally and 5–20 mg intravenously, if necessary. In patients with a heart rate of < 80/min, mid-diastolic triggering was applied with 3–5% padding (73–83% of the R-R interval), and in those with ≥ 80/min, systolic triggering was chosen (35–45% of the R-R interval). Iomeprol contrast material (Iomeron 400, Bracco Imaging Ltd.) was used with 85–95 ml contrast agent at a flow rate of 4.5–5.5 ml/s from antecubital vein access via 18-gauge catheter using a four-phasic protocol [14]. Bolus tracking in the left atrium was used to obtain proper scan timing. 0.8 mg sublingual nitroglycerin was given between the CACS and coronary CTA examinations. Non-contrast data sets were reconstructed with a slice thickness and increment of 2.5 mm, while coronary CTA data sets were reconstructed with 0.8-mm slice thickness and 0.4-mm increment.
CACS was measured by a commercially available semi-automated software (HeartBeat-CS, Philips IntelliSpace Portal, Philips Healthcare). Coronary CTA examinations were evaluated by axial, multiplanar, and curved multiplanar reconstructions using commercially available software (Comprehensive Cardiac Analysis, Philips IntelliSpace Portal, Philips Healthcare). All examinations were evaluated physicians with level 3 or equivalent certification for coronary CTA. Luminal stenosis were classified into 6 groups: (1) normal—no luminal stenosis; (2) minimal—< 25% stenosis; (3) mild—25–49% stenosis; (4) moderate—50–69% stenosis; (5) severe—70–99% stenosis; and (6) occluded and were reported in a segment-based fashion into a structured reporting platform (Axis, Neumann Medical Ltd.) based on the guidelines of the Society of Cardiovascular Computed Tomography [15].
Outcome definitions
We aimed to study the influence of the various clinical parameters and CACS on the need for additional testing of CAD after coronary CTA. Therefore, we determined Outcome 1 as the need for further testing following coronary CTA due to inadequate IQ (non-diagnostic IQ of at least one coronary segment) and/or the presence of obstructive CAD (at least 50% luminal stenosis on any coronary on CTA). We did further sub-analyses to determine the cause of downstream testing. We determined Outcome 2 as non-diagnostic IQ of coronary CTA (in at least one coronary segment); and Outcome 3 as presence of at least 50% luminal stenosis on coronary CTA as these stenoses may be hemodynamically significant [16].
Model specifications
For all three outcomes, we built the following models. Model 1, clinical factors routinely evaluated during coronary CTA: body mass index (BMI), heart rate at scan, and any heart rhythm irregularity (sinus vs irregular) at scan which may reduce coronary CTA IQ. Model 2, parameters of Model 1 and characteristics of the Diamond and Forrester score used to asses pre-test probability of obstructive CAD: age, sex, and type of angina (typical, atypical, non-specific) [13]. Model 3, parameters of Model 2 including also CACS using categories of 0, 1–10, 11–100, 101–400, 401–1000, and > 1000 [17].
Statistical analysis
Continuous variables are expressed as mean ± SD while categorical variables are expressed as frequencies and percentages. We performed multivariate logistic regression and receiver operating characteristics (ROC) analyses to examine the influence of the various factors (Models 1–3) on downstream testing following coronary CTA (Outcome 1) and also sub-analyses for the cause of downstream testing: inadequate IQ (Outcome 2) or the presence of at least 50% luminal stenosis on coronary CTA (Outcome 3). We calculated the R2 using the Nagelkerke method for the logistic regression models to enumerate the variation accountable to the investigated parameters. Sensitivity, specificity, positive and negative predictive values, and accuracy were derived from ROC analysis using Youden index. We compared the areas under curves (AUCs) for the abovementioned models using the DeLong’s test [18]. Finally, we conducted a simulation analyses, where we predicted the probability of further downstream testing for subgroups of the significant predictors of Outcome 1. For this, CACS was included as a continuous variable to allow reporting of exact CACS cutoff values for specific probabilities. All analyses were done in the R environment (version: 3.6.1) [5]. ROC analyses and R2 values were calculated using the ‘pROC’ (version: 1.15.3) and ‘rsq’ (1.1) packages respectively [6, 7]. Two-tailed p values smaller than 0.05 were considered significant.
Results
Patient characteristics
We included 6705 patients who underwent coronary CTA due to suspected CAD. One thousand one hundred fifty-eight patients were excluded due to known prior CAD, 1160 CTA scans due to imaging of the left atrium and pulmonary veins before atrial ablation therapy. Furthermore, 267 patients were excluded due to the presence of congenital or structural heart disease, and pacemaker electrodes, and due to any other indication of cardiac CTA. After exclusion, the final number of analyzed patients was 4120 (45.7% female, 57.9 ± 12.1 years). The mean BMI of the patients was 28.4 ± 7.7 kg/m2, and mean heart rate was 59.9 ± 9.1 bmp. Arrhythmia was present in 152 patients (3.7%). Detailed data on the cardiovascular risk factors and coronary CTA scan parameters are in Table 1. Altogether, 275 (6.7%) of the coronary CTA scans were non-diagnostic in at least one coronary segment. The main reasons for inadequate IQ were motion artifact (248/275, 90.2%), image noise (51/275, 18.5%), and heavy calcification (49/275, 17.8%). Obstructive (> 50% stenosis) coronary artery stenosis was detected in 1073/4120 (26.0%) of the included patients. In 1236/4120 (30.0%) of patients, downstream testing was suggested either because of non-diagnostic IQ or because of the presence of > 50% of stenosis on other coronary segments.
Factors contributing to the need for downstream testing following coronary CTA
Anthropometric parameters (Model 1) achieved weak diagnostic accuracy to identify patients referred to further testing (AUC = 0.56 [0.54–0.58]). Including parameters of the Diamond and Forrester score (Model 2) significantly improved the discriminatory power (AUC = 0.72 [0.70–0.74]; p < 0.001). Adding CACS (Model 3) further increased the diagnostic accuracy (AUC = 0.84 [0.83–0.86]; p < 0.001 compared to Model 1 and Model 2). Sensitivity, specificity, positive and negative predictive values, and accuracy of the models were the following: 39.1%, 72.5%, 73.9%, 73.5%, and 62.5% for Model 1; 65.4%, 68.4%, 47.0%, 82.2%, and 67.5% for Model 2; and 69.9%, 83.8%, 64.9%, 86.7%, and 79.6% for Model 3, respectively. Results are summarized in Fig. 1.

ROC curves of the various models for identifying those who need downstream testing, because of non-diagnostic IQ and/or the presence of significant coronary artery stenosis. Abbreviations: BMI, body mass index; CACS, coronary calcium score; HR, heart rate; IQ, image quality
In our final model, each additional beat per minute during the examination increased the odds of downstream testing by 1.03 (p < 0.001), the presence of any kind of heart rhythm irregularity by 2.12 (p < 0.001), atypical and typical angina by 1.29 and 1.64 (p < 0.01; p < 0.001; respectively), and CACS categories by CACS1–10: 2.46; CACS11–100: 4.23; CACS101–400: 12.34; CACS401–1000: 33.83; and CACS>1000: 164.90 (p < 0.001 for all). Detailed results can be found in Table 2.
Factors contributing to non-diagnostic image quality resulting in additional testing following coronary CTA
Adding risk factors (Model 2) and total CACS (Model 3) to anthropometric factors (Model 1) did not improve significantly the discriminatory power of finding non-diagnostic IQ of at least one coronary artery segment (AUC = 0.79 [0.78–0.83] for Model 1; AUC = 0.80 [0.78–0.83] for Model 2; AUC = 0.80 [0.78–0.83] for Model 3; all p > 0.05). Sensitivity, specificity, positive and negative predictive values, and accuracy of the models for non-diagnostic IQ were the following: 67.3%, 81.9%, 21.0%, 97.2%, and 80.9% for Model 1; 69.5%, 79.2%, 19.2%, 97.3%, and 78.6% for Model 2; 77.5%, 70.4% 15.8%, 97.8%, and 70.9% for Model 3. Results are summarized in Fig. 1.
After adjustment for Model 3, each extra beat per minute increased the odds of insufficient IQ by 1.07 (p < 0.001), irregular heart rhythm by 2.70 (p < 0.001), and CACS groups by CACS11–100: 1.53; CACS101–400: 2.07; CACS401–1000: 2.59; and CACS>1000: 3.11 (p < 0.05 for all), while male sex decreased the odds of inadequate IQ by 0.54 (p < 0.001). Detailed results can be found in Supplementary Table 1.
Factors contributing to the presence of significant stenosis resulting in further testing following coronary CTA
Anthropometric parameters (Model 1) proved to be insufficient in the discrimination of those with obstructive coronary artery stenosis (AUC = 0.56 [0.54–0.58]). Addition of the age, sex, and type of chest pain (Model 2) resulted in significantly higher diagnostic accuracy (AUC = 0.74 [0.72–0.75]; p < 0.001). Adding total CACS (Model 3) further improved diagnostic power (AUC = 0.87 [0.86–0.88]; p < 0.001). For significant coronary artery stenosis, as the outcome, sensitivity, specificity, positive and negative predictive values, and accuracy of the models were the following: 64.1%, 45.0%, 29.1%, 78.1%, and 50.0% for Model 1; 75.9% 60.6%, 40.4%, 87.7%, and 64.6% for Model 2; and 77.2% 82.3% 60.6%, 91.1%, and 81.0% for Model 3.
In the final model, each year of age increased the odds of significant coronary artery lesion by 1.01 (p = 0.04), male sex by 1.22 (p < 0.01), atypical and typical chest pain by 1.36 and 2.00 (p < 0.001), and coronary artery calcification by CACS1–10: 4.03; CACS11–100: 7.22; CACS101–400: 22.16; CACS401–1000: 60.34; and CACS>1000: 326.75 (p < 0.001 for all). Detailed results can be found in Supplementary Table 1.
Probability of downstream testing for specific CACS thresholds for given heart rates, presence of arrhythmia, and type of chest pain
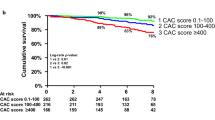
In our analysis of additional testing for any reason after coronary CTA (Outcome 1), type of chest pain, heart rate, and presence of heart rhythm irregularity proved to be independent predictors of further testing of CAD beyond total CACS. We simulated the probability of downstream testing for given CACS values for patient groups with non-specific, atypical and typical angina, sinus rhythm, or arrhythmia with heart rate of 50–60–70–80–90 bpm separately. Probability plots are presented in Fig. 2, while CACS cutoff values for specific probabilities of further testing are presented in Table 3.

Probability plot of downstream testing following coronary CTA by type of angina, heart rhythm regularity, heart rate, and total CACS. Abbreviations: CACS, coronary calcium score; HR, heart rate
Discussion
Our results indicate that anthropometric parameters on their own are insufficient to identify patients in whom additional testing of CAD after coronary CTA is highly probable. Classical risk factors of the Diamond and Forrester pre-test probability score gave additional power to the prediction. However, inclusion of total CACS significantly improved the diagnostic accuracy providing excellent discriminatory power to identify patients by whom deferral of coronary CTA may be recommended as a final diagnostic decision regarding CAD could not be made. In case of non-specific angina, CACS above 435, 756, and 944; in atypical angina CACS above 381, 702, and 890; and in typical angina CACS above 316, 636, and 824 correspond to 50%, 80%, and 90% probability of further testing for patients with sinus rhythm of 50 bpm. However, higher heart rates, and presence of heart rhythm irregularity, significantly decrease these cutoffs (p < 0.001); therefore, strict heart rate control is still advised. Our results provide individualized cutoff values for given probabilities of downstream testing, which may help personalize decision-making in whom alternative tests may be beneficial as coronary CTA does not lead to a final clinical decision. Future prospective studies are warranted to assess the effect of applying CACS as a gatekeeper for coronary CTA on patient management and outcomes and also on the healthcare system.
One of the new recommendations of the European Society of Cardiology in 2019 is the endorsement of coronary CTA as an initial non-invasive test for those by whom clinical assessment alone is not enough to rule out obstructive CAD [4]. These recommendations follow previous initiatives of the National Institute of Health and Care Excellence in the UK, where coronary CTA is recommended as the initial diagnostic test in stable chest pain patients [9]. In compliance with the guidelines, it is prognosticated that a 700% increase in coronary CTA delivery is required in the UK alone [4]. In order to decrease the burden of the healthcare systems, identification of patients in whom coronary CTA does not lead to a final diagnostic decision-may be needed, as these patients may benefit more from alternative tests.
When analyzing the predictors of further testing of CAD, heart rate, presence of heart rhythm irregularity, type of chest pain, and coronary artery calcium were all significant independent predictors. From all these factors, coronary calcification was by far the most prominent predictor (OR = 33.83 for CACS401–1000 and OR = 164.90, for those with CACS>1000). These results were mainly driven by the ability of CACS to predict obstructive CAD which needs further testing or intervention, as in our sub-analysis predicting non-diagnostic IQ, the model with simple anthropometric parameters had the same diagnostic accuracy as more complex models incorporating risk factor and CACS.
Coronary artery calcification has been reported to be an important predictor of significant coronary artery stenosis [10, 19,20,21,22]. Until now, only some risk-predicting score systems such as the Multi-Ethnic Study of Atherosclerosis risk score implanted CACS into their models, even though a recent study reported that CACS is the most important predictor of CAD-related outcomes [23]. Our results are in line with these findings, since beyond age, male sex, and type of chest pain, CACS proved to be the most prominent predictor of obstructive coronary artery stenosis as depicted by coronary CTA (OR = 60.34 for those with CACS401–1000 and OR = 326.75 for CACS>1000). These results indicate that routine assessment of CACS before coronary CTA may allow the identification of patients in whom coronary CTA alone may be not enough for the evaluation of CAD, as in these cases the probability of finding at least 50% lumen stenosis potentially being hemodynamically significant and therefore needing further assessment is very high.
Coronary artery calcification may also cause blooming and beam-hardening artifacts resulting in a virtual increase of the plaque volume, and therefore leading to the overestimation of the stenosis and increase of false positive results [12, 24]. Several studies investigated the influence of CACS on the accuracy of coronary CTA. Most of them reported a CACS score > 400 as a threshold for prominent decrease in diagnostic accuracy [7, 25,26,27,28,29,30,31,32]. However, all of them used 64-slice or dual-source CT. Based on our results, in case of a 256-slice CT scanner, CACS did not prove to have additional role in the prediction of insufficient IQ. Above CACS, higher heart rate and arrhythmia were important contributors of insufficient IQ, since in 90.2% of the cases non-diagnostic IQ was due to motion artifact. Moreover, after adjustment for the main cardiovascular risk factors and CACS, heart rate (OR = 1.07), and arrhythmia (OR = 2.70), proved to be important predictors of non-diagnostic IQ. Even though 256-slice CT scanners permit better partial and temporal resolution, rhythm control and optimal heart rate are still important for achieving diagnostic IQ in all coronary artery segments.
Our simulation results revealed that no single CACS cutoff can be provided as the type of chest pain, arrhythmia, and heart rate all significantly change the probability of requiring further downstream testing either because of insufficient IQ or because of presence of significant stenosis. Our tables may help the decision-making at an individual level.
Our study has some limitations. First of all, it is a single-center, retrospective study using only one vendor system; therefore, our results are only generalizable to other populations and other machinery with caution. Second, we have no information on the results of downstream testing. However, our aim was not to assess the diagnostic accuracy of coronary CTA, since the high sensitivity and negative predictive value of this modality are already well-known, but to assess in whom coronary CTA may not be beneficiary as it does not lead to a final diagnostic decision. Third, fractional flow reserve analysis of the CTA images was not done, which could have decreased the referrals to further testing. However, most centers do not have access to this technology yet and therefore fractional flow reserve-based outcomes would limit the generalizability of the results. Finally, it is a single-vendor study; therefore, the effect of anthropometrics might be different on other machines.
In conclusion, routine evaluation of CACS before coronary CTA may be advised as it significantly increases the diagnostic accuracy to identify patients in whom further testing will be needed following coronary CTA. Deferral of these patients to other diagnostic modalities might be beneficial as coronary CTA does not lead to a final decision regarding CAD management.
Abbreviations
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- CACS:
-
Coronary calcium score
- CAD:
-
Coronary artery disease
- CI:
-
Confidence interval
- CTA:
-
Computed tomography angiography
- HR:
-
Heart rate
- IQ:
-
Image quality
- OR:
-
Odds ratio
- ROC:
-
Receiver operating curve
References
Budoff MJ, Dowe D, Jollis JG et al (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 52:1724–1732
Meijboom WB, Meijs MF, Schuijf JD et al (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52:2135–2144
Paech DC, Weston AR (2011) A systematic review of the clinical effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of suspected coronary artery disease. BMC Cardiovasc Disord 11:32
Knuuti J, Wijns W, Saraste A et al (2020) 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 41:407–477
Arbab-Zadeh A, Miller JM, Rochitte CE et al (2012) Diagnostic accuracy of computed tomography coronary angiography according to pre-test probability of coronary artery disease and severity of coronary arterial calcification. The CORE-64 (Coronary Artery Evaluation Using 64-Row Multidetector Computed Tomography Angiography) International Multicenter Study. J Am Coll Cardiol 59:379–387
Brodoefel H, Burgstahler C, Tsiflikas I et al (2008) Dual-source CT: effect of heart rate, heart rate variability, and calcification on image quality and diagnostic accuracy. Radiology 247:346–355
Budoff MJ, Jollis JG, Dowe D, Min J, VCT Study Group (2013) Diagnostic accuracy of coronary artery calcium for obstructive disease: results from the ACCURACY trial. Int J Cardiol 166:505–508
den Dekker MA, de Smet K, de Bock GH, Tio RA, Oudkerk M, Vliegenthart R (2012) Diagnostic performance of coronary CT angiography for stenosis detection according to calcium score: systematic review and meta-analysis. Eur Radiol 22:2688–2698
Vavere AL, Arbab-Zadeh A, Rochitte CE et al (2011) Coronary artery stenoses: accuracy of 64-detector row CT angiography in segments with mild, moderate, or severe calcification--a subanalysis of the CORE-64 trial. Radiology 261:100–108
McClelland RL, Chung H, Detrano R, Post W, Kronmal RA (2006) Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 113:30–37
Boas FE, Fleischmann D (2012) CT artifacts: causes and reduction techniques. Imaging Med 4:229–240
Kalisz K, Buethe J, Saboo SS, Abbara S, Halliburton S, Rajiah P (2016) Artifacts at cardiac CT: physics and solutions. Radiographics 36:2064–2083
Diamond GA, Forrester JS (1979) Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 300:1350–1358
Karady J, Panajotu A, Kolossvary M et al (2017) The effect of four-phasic versus three-phasic contrast media injection protocols on extravasation rate in coronary CT angiography: a randomized controlled trial. Eur Radiol 27:4538–4543
Leipsic J, Abbara S, Achenbach S et al (2014) SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 8:342–358
Wu FZ, Wu MT (2015) 2014 SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 9:e3
Budoff MJ, Shaw LJ, Liu ST et al (2007) Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol 49:1860–1870
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845
McClelland RL, Jorgensen NW, Budoff M et al (2015) 10-year coronary heart disease risk prediction using coronary artery calcium and traditional risk factors: derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) with validation in the HNR (Heinz Nixdorf Recall) study and the DHS (Dallas Heart Study). J Am Coll Cardiol 66:1643–1653
Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE (2018) Coronary calcium score and cardiovascular risk. J Am Coll Cardiol 72:434–447
Lehmann N, Erbel R, Mahabadi AA et al (2018) Value of progression of coronary artery calcification for risk prediction of coronary and cardiovascular events: result of the HNR study (Heinz Nixdorf recall). Circulation 137:665–679
Ferencik M, Pencina KM, Liu T et al (2017) Coronary artery calcium distribution is an independent predictor of incident major coronary heart disease events: results from the Framingham Heart Study. Circ Cardiovasc Imaging 10:e006592
Ambale-Venkatesh B, Yang X, Wu CO et al (2017) Cardiovascular event prediction by machine learning: the multi-ethnic study of atherosclerosis. Circ Res 121:1092–1101
Boas E (2012) CT artifacts: causes and reduction techniques. Imaging Med 4
Morgan-Hughes GJ, Roobottom CA, Owens PE, Marshall AJ (2005) Highly accurate coronary angiography with submillimetre, 16 slice computed tomography. Heart 91:308–313
Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA (2005) Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 46:552–557
Diederichsen AC, Petersen H, Jensen LO et al (2009) Diagnostic value of cardiac 64-slice computed tomography: importance of coronary calcium. Scand Cardiovasc J 43:337–344
Meijs MF, Meijboom WB, Prokop M et al (2009) Is there a role for CT coronary angiography in patients with symptomatic angina? Effect of coronary calcium score on identification of stenosis. Int J Cardiovasc Imaging 25:847–854
Meng L, Cui L, Cheng Y et al (2009) Effect of heart rate and coronary calcification on the diagnostic accuracy of the dual-source CT coronary angiography in patients with suspected coronary artery disease. Korean J Radiol 10:347–354
Palumbo AA, Maffei E, Martini C et al (2009) Coronary calcium score as gatekeeper for 64-slice computed tomography coronary angiography in patients with chest pain: per-segment and per-patient analysis. Eur Radiol 19:2127–2135
Scheffel H, Alkadhi H, Plass A et al (2006) Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol 16:2739–2747
Yerramasu A, Lahiri A, Venuraju S et al (2014) Diagnostic role of coronary calcium scoring in the rapid access chest pain clinic: prospective evaluation of NICE guidance. Eur Heart J Cardiovasc Imaging 15:886–892
Funding
Open access funding provided by Semmelweis University (SE). Project no. NVKP_16-1-2016-0017 (“National Heart Program”) has been implemented with the support provided from the National Research, Development and Innovation Fund of Hungary, financed under the NVKP_16 funding scheme. The research was financed by the Higher Education Institutional Excellence Programme of the Ministry for Innovation and Technology in Hungary, within the framework of the Therapeutic Development Thematic Programme of the Semmelweis University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Márton Kolossváry.
Conflict of interest
The authors of this manuscript declare relationships with the following companies: Márton Kolossváry and Pál Maurovich-Horvat are shareholders in Neumann Medical Ltd., whose structured reporting platform was used during the study.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board due to the retrospective nature of the study.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Retrospective
• Diagnostic or prognostic study
• Performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 19 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Simon, J., Száraz, L., Szilveszter, B. et al. Calcium scoring: a personalized probability assessment predicts the need for additional or alternative testing to coronary CT angiography. Eur Radiol 30, 5499–5506 (2020). https://doi.org/10.1007/s00330-020-06921-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-06921-7