
Abstract
Purpose
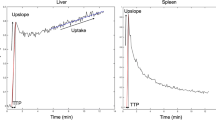
To assess liver perfusion-CT (P-CT) parameters derived from peak-splenic (PSE) versus peak-renal enhancement (PRE) maximum slope-based modelling in different levels of portal-venous hypertension (PVH).
Material and methods
Twenty-four patients (16 men; mean age 68 ± 10 years) who underwent dynamic P-CT for detection of hepatocellular carcinoma (HCC) were retrospectively divided into three groups: (1) without PVH (n = 8), (2) with PVH (n = 8), (3) with PVH and thrombosis (n = 8). Time to PSE and PRE and arterial liver perfusion (ALP), portal-venous liver perfusion (PLP) and hepatic perfusion-index (HPI) of the liver and HCC derived from PSE- versus PRE-based modelling were compared between the groups.
Results
Time to PSE was significantly longer in PVH groups 2 and 3 (P = 0.02), whereas PRE was similar in groups 1, 2 and 3 (P > 0.05). In group 1, liver and HCC perfusion parameters were similar for PSE- and PRE-based modelling (all P > 0.05), whereas significant differences were seen for PLP and HPI (liver only) in group 2 and ALP in group 3 (all P < 0.05).
Conclusion
PSE is delayed in patients with PVH, resulting in a miscalculation of PSE-based P-CT parameters. Maximum slope-based P-CT might be improved by replacing PSE with PRE-modelling, whereas the difference between PSE and PRE might serve as a non-invasive biomarker of PVH.
Key Points
• Peak-splenic enhancement is decreased and delayed in patients with portal-venous hypertension
• The maximum-slope method uses PSE to calculate arterial and portal-venous liver perfusion
• Peak-renal enhancement (PRE) is insensitive to PVH and might improve perfusion modelling
• The difference between PSE and PRE might serve as a non-invasive PVH biomarker





Similar content being viewed by others

References
Vollmar B, Siegmund S, Menger MD (1998) An intravital fluorescence microscopic study of hepatic microvascular and cellular derangements in developing cirrhosis in rats. Hepatology 27:1544–1553
Richter S, Mucke I, Menger MD, Vollmar B (2000) Impact of intrinsic blood flow regulation in cirrhosis: maintenance of hepatic arterial buffer response. Am J Physiol Gastrointest Liver Physiol 279:G454–G462
Gulberg V, Haag K, Rossle M, Gerbes AL (2002) Hepatic arterial buffer response in patients with advanced cirrhosis. Hepatology 35:630–634
Muto J, Shirabe K, Sugimachi K, Maehara Y (2014) Review of angiogenesis in hepatocellular carcinoma. Hepatol Res. doi:10.1111/hepr.12310
Fischer MA, Kartalis N, Grigoriadis A et al (2015) Perfusion computed tomography for detection of hepatocellular carcinoma in patients with liver cirrhosis. Eur Radiol. doi:10.1007/s00330-015-3732-1
Fischer MA, Leidner B, Kartalis N et al (2014) Time-resolved computed tomography of the liver: retrospective, multi-phase image reconstruction derived from volumetric perfusion imaging. Eur Radiol 24:151–161
Frampas E, Lassau N, Zappa M, Vullierme MP, Koscielny S, Vilgrain V (2013) Advanced Hepatocellular Carcinoma: early evaluation of response to targeted therapy and prognostic value of Perfusion CT and Dynamic Contrast Enhanced-Ultrasound. Preliminary results. Eur J Radiol 82:e205–e211
Morsbach F, Pfammatter T, Reiner CS et al (2013) Computed tomographic perfusion imaging for the prediction of response and survival to transarterial radioembolization of liver metastases. Investig Radiol 48:787–794
Ronot M, Asselah T, Paradis V et al (2010) Liver fibrosis in chronic hepatitis C virus infection: differentiating minimal from intermediate fibrosis with perfusion CT. Radiology 256:135–142
Pandharipande PV, Krinsky GA, Rusinek H, Lee VS (2005) Perfusion imaging of the liver: current challenges and future goals. Radiology 234:661–673
Miles KA, Hayball MP, Dixon AK (1993) Functional images of hepatic perfusion obtained with dynamic CT. Radiology 188:405–411
Materne R, Van Beers BE, Smith AM et al (2000) Non-invasive quantification of liver perfusion with dynamic computed tomography and a dual-input one-compartmental model. Clin Sci (Lond) 99:517–525
Cuenod C, Leconte I, Siauve N et al (2001) Early changes in liver perfusion caused by occult metastases in rats: detection with quantitative CT. Radiology 218:556–561
Blomley MJ, Coulden R, Dawson P et al (1995) Liver perfusion studied with ultrafast CT. J Comput Assist Tomogr 19:424–433
Tsushima Y, Funabasama S, Aoki J, Sanada S, Endo K (2004) Quantitative perfusion map of malignant liver tumors, created from dynamic computed tomography data. Acad Radiol 11:215–223
Awaya H, Mitchell DG, Kamishima T, Holland G, Ito K, Matsumoto T (2002) Cirrhosis: modified caudate-right lobe ratio. Radiology 224:769–774
Soresi M, Giannitrapani L, Cervello M, Licata A, Montalto G (2014) Non invasive tools for the diagnosis of liver cirrhosis. World J Gastroenterol 20:18131–18150
European Association For The Study Of The Liver, European Organisation For Research and Treatment of Cancer (2012) EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 56:908–943
Bruix J, Sherman M, American Association for the Study of Liver D (2011) Management of hepatocellular carcinoma: an update. Hepatology 53:1020–1022
Goetti R, Leschka S, Desbiolles L et al (2010) Quantitative computed tomography liver perfusion imaging using dynamic spiral scanning with variable pitch: feasibility and initial results in patients with cancer metastases. Investig Radiol 45:419–426
Weidekamm C, Cejna M, Kramer L, Peck-Radosavljevic M, Bader TR (2005) Effects of TIPS on liver perfusion measured by dynamic CT. AJR Am J Roentgenol 184:505–510
Kawanaka H, Akahoshi T, Kinjo N et al (2014) Effect of laparoscopic splenectomy on portal haemodynamics in patients with liver cirrhosis and portal hypertension. Br J Surg 101:1585–1593
Tsushima Y, Koizumi J, Yokoyama H, Takeda A, Kusano S (1998) Evaluation of portal pressure by splenic perfusion measurement using dynamic CT. AJR Am J Roentgenol 170:153–155
Ippolito D, Capraro C, Casiraghi A, Cestari C, Sironi S (2012) Quantitative assessment of tumour associated neovascularisation in patients with liver cirrhosis and hepatocellular carcinoma: role of dynamic-CT perfusion imaging. Eur Radiol 22:803–811
Acknowledgements
The scientific guarantor of this publication is Prof. Peter Aspelin. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The first author was financially supported by the Swiss Radiological Society. No other authors have received any funding. One of the authors has significant statistical expertise. Institutional Review Board approval was obtained. Written informed consent was waived by the Institutional Review Board.
In total 7/24 patients have been previously reported in Fischer MA, et al. Eur Radiol 24(1):151-61 and Fischer MA, et al. Eur Radiol 25(11): 3123-3132.
Methodology: retrospective, diagnostic study, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fischer, M.A., Brehmer, K., Svensson, A. et al. Renal versus splenic maximum slope based perfusion CT modelling in patients with portal-hypertension. Eur Radiol 26, 4030–4036 (2016). https://doi.org/10.1007/s00330-016-4277-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4277-7