
Abstract
The study aimed to analyze the influence of the COVID-19 pandemic on mortality rates in patients with systemic autoimmune rheumatic diseases (SARD) in Mexico. We selected SARD-related deaths using National Open Data and Information from the Ministry of Health, Mexico, and ICD-10 codes. We assessed the observed compared to the predicted mortality values for 2020 and 2021, employing trends from 2010 to 2019 with joinpoint and prediction modelling analyses. Among 12,742 deaths due to SARD between 2010 and 2021, the age-standardized mortality rate (ASMR) increased significantly between 2010 and 2019 (pre-pandemic) (annual percentage change [APC] 1.1%; 95% CI 0.2–2.1), followed by a non-significant decrease during the pandemic period (APC 13.9%; 95% CI 13.9–5.3). In addition, the observed ASMR of 1.19 for 2020 for SARD and of 1.14 for 2021 were lower than the predicted values of 1.25 (95% CI 1.22–1.28) for 2020 and 1.25 (95% CI 1.20–1.30) for 2021. Similar findings were identified for specific SARD, mainly systemic lupus erythematosus (SLE), or by sex or age group. Interestingly, the observed mortality rates for SLE in the Southern region of 1.00 in 2020 and 1.01 in 2021 were both significantly greater than the predicted values of 0.71 (95% CI 0.65–0.77) in 2020 and 0.71 (95% CI 0.63–0.79). In Mexico, the observed SARD mortality rates were not higher than the expected values during the pandemic, except for SLE in the Southern region. No differences by sex or age group were identified.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Systemic autoimmune rheumatic diseases (SARD) comprise a heterogeneous group of disorders characterized by an altered immune response leading to inflammation and systemic involvement [1]. Despite recent advances in therapies, the burden of SARD remains high despite recent advances in therapies [2]. In Mexico, some SARD have experienced a decrease in mortality rates [3], others have exhibited an increase in mortality and hospitalizations [4,5,6].
Three years ago, the World Health Organization (WHO) announced that the world was experiencing a pandemic as a consequence of severe acute respiratory syndrome coronavirus (SARS-CoV-2) infection, denominating the COVID-19 pandemic. To date, this pandemic has had impressive and expansive consequences on the population.
The COVID-19 pandemic affected access to health services, with frequent avoidance of office visits and laboratory testing, particularly in the early months of the pandemic [7, 8]. Interruptions in taking disease-modifying antirheumatic drugs also commonly occur without the advice of a physician [8]. Racial and ethnic differences in COVID-19 outcomes have been reported in patients with SARD. African-American, Latin American, and Asian individuals have increased odds of hospitalization and ventilatory support [9].
Nationwide, indicative data leading to the precise allocation of resources and preventive actions for the most affected population are lacking. Thus, the objective of our study was to evaluate the trends and influence of COVID-19 on the mortality rates of subjects with SARD in Mexico from the years 2010–2021, with a specific assessment of SARD. In addition, variations in mortality rates according to age, sex, and geographic region among SARD patients were evaluated.
Methods
Study design and data sources
In this epidemiological study, data were acquired from the website of the National Institute of Statistics and Geography [INEGI] through the General Directorate of Health Information (DGIS) Open Access of the Ministry of Health (SSA) in Mexico [10]. This database collects death records from death certificates from across the country. The data were updated in December 2021. In addition, data from Mexican National Population Council (CONAPO) projections were gathered [11]. Age, sex, and geographic region were obtained. Geographic regions were categorized according to the INEGI groups. This study was approved by our Institutional Review Board (R-2022-2106-011).
Population selection
We selected information on SARD-related deaths among Mexican subjects aged 15 years or above from January 1, 2010, to December 31, 2021. Data on all-cause of mortality were collected using the 10th edition of the International Classification of Diseases (ICD-10). We included the following SDAR: systemic lupus erythematosus (SLE) (M32*), systemic sclerosis (SSc) (M34*), idiopathic inflammatory myopathies (IIM) (M33*), rheumatoid arthritis (RA) (M05-M06*), and antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) (M31*). Death certificates that did not provide geographical or sociodemographic data were excluded.
Statistical analysis
Descriptive analyses are presented as frequencies with percentages. Age-standardized mortality rates (ASMR, per 100,000 inhabitants) were calculated using the age framework (15–75+ years) from 2010 to 2021 in the Mexican population using the direct standardization method. Initially, we determined the national trends of mortality in subjects with SARD by conducting a joinpoint analysis (piecewise linear regression) [12]. For the overall trend, one or more pieces of the annual percentage change (APC) with 95% confidence intervals (95% CI) were analyzed using a Monte Carlo permutation test. Then, in order to estimate the predicted mortality values in 2020 and 2021, derived from mortality values from 2010 to 2019 to contrast with the observed values, we carried out a predictive analysis employing linear models between years and ASMR. The predicted rate was compared with the observed rate and evaluated to determine whether the observed rate overlapped with the 95% CI of the predicted value. The SPSS Statistics (version 25; SPSS, Chicago, IL, USA) time series model with the expert modeler choice was utilized to predict the future trend of SARD mortality. Additionally, we performed a subgroup analysis for sex (female and male) and geographic region (Northern, Midwest, Central, and Southern). Subgroups with ≤ 20 deaths may have led to inaccurate calculations for mortality rates; therefore, these were not performed. All calculations were conducted using the joinpoint analysis (version 4.9.0.0) issued by the United States National Cancer Institute (http://surviellance.cancer.gov/joinpoint). A 2-sided p < 0.05 was considered statistically significant.
Results
Study population
Overall, 13,143 deaths among patients aged ≥ 15 years with SARD were recorded between 2010 and 2021. SLE was the most frequent common cause of death (67.8%) followed by SSc (19.5%), PM/DM (6.4%), RA (3.3%), and AAV (3.0%) (Table S1). The majority of deaths were in females (83.9%) overall and in every SARD. The majority of deaths occurred in persons aged between 15 and 54 years (67.4%) at the time of death for overall and specific SARD, with the exception of RA (28.5%). There were notable variations in the distribution of mortality among the geographic regions. Death due to SARD occurred overwhelmingly among the residents of the central region.
Influence of COVID-19 pandemic on ASMR
Overall analysis for SARD ASMR
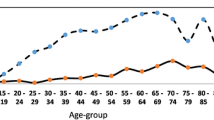
The ASMR (per 100,000 inhabitants) for SARD remained stable from 1.16 in 2010 to 1.16 in 2021, generating an average APC of 0.0% for 2010–2021 (95% CI − 1.8 to 1.8; p = 0.99). The ASMR and APC for mortality in Mexico in patients with SARD are shown in Table 1. Interestingly, in the trend-segment evaluation, we identified a significant uptrend of 1.3 (95% CI 0.3–2.3) from 2010 to 2019 and then a stable trend from 2019 to 2021. The observed ASMR of 1.23 for 2020 for SARD and of 1.16 for 2021 were nearly similar to the predicted values of 1.30 (95% CI 1.26–1.34) for 2020 and 1.30 (95% CI 1.25–1.30) for 2021 (Fig. 1a). Similar segmental trends have been observed in patients SLE patiens. Although the ASMR increased slightly from 0.77 in 2010 to 0.80 in 2021, the average APC was 0.3% (95% CI − 1.1 to 1.8; p = 0.654). The observed ASMR of 0.83 in 2020 and of 0.83 in 2021 were slightly lower than the predicted values of 0.86 (95% CI 0.84–0.88) in 2020 and of 0.86 (95% CI 0.83–0.89) in 2021 (Fig. 1b). The ASMR trend for SSc remained steady from 2010 to 2021 at an average APC of 0.3 (95% CI − 5.1 to 6.1) and without significant variation (Fig. 1c). The observed ASMR for 2020 and 2021 for SSc were marginally lower than the predicted rates for SSc (0.24 vs. 0.26 for 2020 and 0.24 vs. 0.26 for 2021). Similarly, mortality-rate trends were found for IIM, RA and AAV (Figs. 1d, e and f), in which the ASMR trend was stable from 2010–2021 at an average APC of − 3.7 (95% CI − 7.5 to 0.4), 0.3 (95% CI − 7.7 to 8.9), − 0.7 (95% CI − 11.6, 11.5) respectively. The observed ASMR for 2020 and 2021 for IIM, RA and AAV were slightly lower than the predicted values (0.07 vs. 0.8 for 2020 and 0.06 vs. 08 for 2021 for IIM, and 0.04 vs. 0.05 for 2020; 0.04 vs. 05 for 2021 for RA and 0.04 vs. 0.05 for 2020 and 0.02 vs. 0.5 for AAV).

a All-cause age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for overall. b All-cause age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for SLE. c All-cause age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for SSc. d All-cause age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for IIM. e All-cause age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for RA. f All-cause Age-standardized mortality for systemic autoimmune rheumatic diseases in Mexico in 2010–2021 with comparisons between observed (blue line) vs. predicted (blue dots) mortality for 2020 and 2021 based on 2010–2019 trend for AAV. AAV antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, IIM idiopathic inflammatory myopathies, LCL lower confidence limits, RA rheumatoid arthritis, SLE systemic lupus erythematosus, SSc systemic sclerosis, UCL upper confidence limits
Subgroup analysis
By sex
As shown in Table 2, all-cause mortality for SARD remained stable across both sexes during the study period; however, segment trend variations were identified. The APC significantly increased in females from 2010 to 2019 (1.0; 95% CI 0.1–1.9), followed by a non-significant downward trend from 2019 to 2021. Similar mortality trends were observed in patients with SLE, while APC significantly increased in males from 2010 to 2019 (6.0; 95% CI 0.1–12.2), without change after that year. The observed ASMR rates were marginally lower than the expected levels for SARD in females (1.90 vs. 2.02 in 2020 and 1.79 vs. 2.02 in 2021). For other SARD, such as IIM, SSc, and RA, there were no segment-trend variations across both sexes during the study period and the observed ASMR values. Similarly, no differences were identified between the observed and predicted rates in IIM, SSc, RA, and AAV.
By geographic region
Subgroup analysis for geographic regions in Mexico found a significant increase in ASMR from 2013 to 2021 among decedents in the southern region for SLE (APC, 5.0; 95% CI 1.0–9.1) (Table 3). The increased mortality rates observed for SLE in the southern region from 1.00 in 2020 to 1.01 in 2021 were both significantly greater than the predicted levels in 0.71 (95% CI 0.65–0.77) in 2020 and 0.71 (95% CI 0.63–0.79). No other significant variations were identified during the pandemic period for overall SARD or specific SARD such as SSc. Analyses for IIM, RA and AAV for ASMR mortality segments were not performed because of the small sample sizes for these conditions.
No significant differences in mortality rates among age groups were identified during the study period for overall SARD and specific SARD (Table S2). However, the majority of deaths recorded were in the age group of 15–54 years for SARD, SLE, IIM and AAV.
Discussion
In this population-based analysis, we evaluated the trends of mortality for SARD and for five specific SARD (SLE, IIM, SSc, RA and AAV) from 2010 to 2021 to establish any possible influence of the COVID-19 pandemic on the deaths of patients with these disorders.
Surprisingly, we did not find an increase in the observed all-cause mortality among patients with SARD during the 2019–2021 period, which was not larger than the values predicted from the pre-pandemic trend, except for SLE in the Southern region of the country. These findings were also found across sex and age groups. However, for most SARD cases, the number of deaths during the study period was higher in the younger population. Our findings were similar to those described recently in a nationwide population-based study in another Latin American country, Brazil [13], which showed no change in the trends of overall mortality from SLE. In contrast, in a nationwide analysis using observed and predicted evaluations from the United States, the authors identified an excess of psoriasis and psoriatic arthritis (inflammatory chronic diseases) mortality during the COVID-19 pandemic [14].
The SARS-CoV-2 infection affected 763 million people and has been responsible for severe affectation in 300 million, in 3.3 million new cases and nearly 6.8 million deaths globally [15]. In Mexico, according to the existing literature, there is excess mortality in the context of the COVID-19 pandemic, which is attributed mainly to the high burden of cardiometabolic disorders in Mexico [16]. In addition, heterogeneity in the burden of mortality during the COVID-19 pandemic has been identified in our country [17]. Our findings identified a diversified effect of the pandemic across geographic regions in Mexico and found that the southern region of Mexico was the sole region in which the observed mortality rates outpaced the predicted values in SLE mortality during the pandemic period. This finding confirms that this region experienced higher death rates from some SARD, as previously reported [4, 5]. This is partly due to higher sociodemographic inequalities and limited access to health care.
Humans possess defense mechanisms against viral infections, including interferon (IFN). Rheumatic diseases are associated with high levels of IFN and viral infection. Inhibition of IFN may be desirable in certain autoimmune diseases, specifically SLE [18]. Type-I IFN immunity is essential for adequate protection, and harmful mutations as well as neutralizing auto-antibodies against IFN have seldom been identified, particularly in the severe manifestations of COVID-19 [19].
Recently, we learned that among patients with SLE and RA, there could be an increase in the risk and severity of COVID when there are pre-existing neutralizing autoantibodies against IFN-I, which are associated with severe COVID in at least 10–20%; in general, the discontinuation of therapy appears to participate in disease flares [20].
Despite continuing deaths from COVID-19 in 2020 and 2021, the mortality from overall SARD and specific SARD remained stable, and the observed mortality rates were even lower than expected in Mexico. The reasons for these findings are unclear; however, some potential explanations are provided. First, reductions in the diagnosis of SARD with some possible displaced mortality and with some patients with SARD dying of COVID-19 before they had completed the final diagnosis of SARD, the latter complex conditions. Second, the deaths recorded as SARD, which were reduced during the pandemic period, may have been due to another cause, as the Mexican national vital statistics recorded only the underlying cause of death but not the contributing cause. Third, the majority of SARD deaths occurred in the younger population (aged 15–54 years). Considering that the older subjects were more prone to die from COVID-19 during the pandemic, this might reduce the number of deaths recorded as any SARD in the elderly, limiting the overall death in patients with SARD. Finally, the negative effects of pandemic control measures on mortality, such as delays in medical care, were probably more than offset by certain positive effects, such as personal hygiene and the implementation of social distancing, reducing some infections, an important risk factor for mortality in SARD, mainly in Latin American patients [21]. In this context, temporal variations in the occurrence of the leading cause of death originating from the COVID-19 pandemic in Mexico were analyzed, and some cause groups had notable declines in the expected pre-pandemic mortality, such as infectious, malignant skin, and musculoskeletal diseases (-5.0%) [22]. In addition, a multinational survey reported that patients with IIM had fewer COVID-19 cases than healthy controls, likely because of the protective behaviors adopted by this vulnerable population, including physical distancing and shielding [23]. Of 3502 patients with rheumatic diseases in patients inhabiting more than 19 Latin American countries, by means of a survey, more than one half of the patients had comorbidities, including hypertension. Antirheumatic therapy was discontinued in 23.4% of patients, and approximately 15% interrupted their comorbidity-associated treatment during the pandemic [24].
The strengths of this study are that, to the best of our knowledge, this is the first study to evaluate the impact of COVID-19 on SARD in Mexico. We standardized all mortality analyses by age, which provided a suitable comparison across Mexican regions with varied population structures. We used a nationwide registry with joinpoint analysis. However, this study has several limitations that should remind us to be considered when interpreting our findings. First, the inherent risk of bias in retrospective studies is applicable to our analysis. Second, we focused on trend mortality analysis, which is unable to quantify the exposure of risk factors that might contribute to the change in SARD tendencies. In addition, in our national database, only all-cause disease-specific data were available, making it impossible to analyze the specific impact of factors such as disease flares and treatments. Third, the case definition for each SARD-related death as the underlying cause of death was obtained from ICD-10 codes in contrast to better-quality clinical data, which is the reason for the level of diagnostic uncertainty and potential misclassification. However, ICD, which produces ICD-10 codes, was planned to foster worldwide equivalence in the acquisition and classification of information on mortality [25]. Notably, mortality data derived from ICD-10 are regularly utilized to determine mortality trends in epidemiological research evaluations of SARD [4, 5, 26, 27]. Fourth, miscoding of the cause of death cannot be ruled out using an administrative database, which may lead to underestimation. Finally, in our national dataset, only all-cause disease-specific causes of death were accessible, preventing further evaluation of the specific influence of determinants such as infections and other morbidities, including kidney disease and end-stage renal disease in patients with SLE. In agreement with our results, the current evidence does not strongly suggest that having immune-mediated inflammatory diseases increases the risk of developing severe COVID-19 [28]. However, although we did not observe any differential mortality in the COVID-19 period, our data raise concerns for undertreating SARD in the pandemic era, which may translate into worse outcomes in the long term. More research is needed to understand whether the patients not presenting to the healthcare system may have improved their compliance with medications in the COVID-19 era or whether they were slowly deteriorating at home. Additionally, the COVID-19 mass vaccination program in our country began in February 2021, which may have influenced our findings by 2021.
Conclusions
Our epidemiological population-based study in Mexico provided data on all-cause mortality rates in SARD patients during the COVID-19 pandemic. This study demonstrated a significantly lower observed mortality rate in terms of expected values during the COVID-19 pandemic for the overall SARD. However, the observed mortality rate was significantly higher than that expected for patients with SLE in the Southern region of Mexico. Our study did not find other variations among sexes, age groups, or other geographic regions. Our results can aid in clinical practice and public health actions, considering the observed mortality trends in Mexico. We also motivate further epidemiological analysis, mainly in the long term and considering confounders, to evaluate these trends for other nationalities to provide a brief overview of the regional approach and policy-decision markers for the current pandemic.
Data availability statement
The National open data and information from the Ministry of Health, Mexico can be accessed through this website: http://www.dgis.salud.gob.mx/contenidos/basesdedatos/Datos_Abiertos_gobmx.html.
Change history
10 June 2024
A Correction to this paper has been published: https://doi.org/10.1007/s00296-024-05625-1
References
Sarzi-Puttini P, Ceribelli A, Marotto D et al (2019) Systemic rheumatic diseases: from biological agents to small molecules. Autoimmun Rev 18:583–592. https://doi.org/10.1016/j.autrev.2018.12.009
Liu S, Wang B, Fan S et al (2022) Global burden of musculoskeletal disorders and attributable factors in 204 countries and territories: a secondary analysis of the Global Burden of Disease 2019 study. BMJ Open 12:e062183. https://doi.org/10.1136/bmjopen-2022-062183
Morales-Etchegaray I, Garcia-Carrasco M, Munguía-Realpozo P et al (2021) Changing trends in rheumatoid arthritis mortality in Mexico, from 1998 to 2017. Rheumatol Int 41:2225–2231. https://doi.org/10.1007/s00296-021-05013-z
Mendoza-Pinto C, Etchegaray-Morales I, Garcia-Carrasco M et al (2022) Twenty-year trends in all-cause mortality of patients with systemic lupus erythematosus in Mexico: results from a nationwide health registry. Lupus 31:382–391. https://doi.org/10.1177/09612033221078228
García-Carrasco M, Mendoza-Pinto C, Etchegaray-Morales I et al (2022) Temporal trends in mortality in patients with systemic sclerosis in public hospitals across Mexico from 1998–2017. Arch Med Res 53:610–616. https://doi.org/10.1016/j.arcmed.2022.07.005
Mendoza-Pinto C, Etchegaray-Morales I, Munguía-Realpozo P et al (2022) Trends in all-cause hospitalizations for systemic lupus erythematosus in Mexico, 2000–2019. Lupus 31:1679–1684. https://doi.org/10.1177/09612033221128745
Carbone T, Picerno V, Pafundi V et al (2022) Impact of the COVID-19 pandemic on the appropriateness of diagnostic pathways of autoimmune rheumatic diseases. J Rheumatol 49:219–224. https://doi.org/10.3899/jrheum.210611
George MD, Venkatachalam S, Banerjee S et al (2021) Concerns, healthcare use, and treatment interruptions in patients with common autoimmune rheumatic diseases during the COVID-19 pandemic. J Rheumatol 48:603–607. https://doi.org/10.3899/JRHEUM.201017
Gianfrancesco MA, Leykina LA, Izadi Z et al (2021) Association of race and ethnicity with COVID-19 outcomes in rheumatic disease: data from the COVID-19 global rheumatology alliance physician registry. Arthritis Rheumatol 73:374–380. https://doi.org/10.1002/art.41567
Datos abiertos. Secretaría de Salud/Dirección General de Información en Salud. http://www.dgis.salud.gob.mx/contenidos/basesdedatos/Datos_Abiertos_gobmx.html. Accessed 1 Dec 2022
Consejo Nacional de Población. Proyecciones de la población de México, 1950–2050 (CONAPO 2020). http://www.conapo.gob.mx/es/CONAPO/Proyecciones. Accessed 20 Nov 2022
Kim HJ, Fay MP, Feuer EJ, Midthune DN (2000) Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 19:335–351. https://doi.org/10.1002/(sici)1097-0258(20000215)19:3%3c335::aid-sim336%3e3.0.co;2-z
Rezende RPV, Mendonça de Santana F, Figueiredo CP (2022) Unchanged trend in mortality from systemic lupus erythematosus during the 2020 COVID-19 pandemic: a nationwide population-based study. Lupus 31:1020–1022
Liu Y, He X, Lee EY et al (2023) Excess psoriasis and psoriatic arthritis mortality during the COVID-19 pandemic in the United States: a nationwide population-based study from 2010 to 2021. J Eur Acad Dermatology Venereol 37:1221–1227. https://doi.org/10.1111/jdv.18978
2023 E 137 published 06 A Weekly epidemiological update on COVID-19 - 6 April 2023. https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---6-april-2023. Accessed 20 Apr 2023
Antonio-Villa NE, Bello-Chavolla OY, Fermín-Martínez CA et al (2022) Socio-demographic inequalities and excess non-COVID-19 mortality during the COVID-19 pandemic: a data-driven analysis of 1 069 174 death certificates in Mexico. Int J Epidemiol 51:1711–1721. https://doi.org/10.1093/ije/dyac184
García-Guerrero VM, Beltrán-Sánchez H (2021) Heterogeneity in excess mortality and its impact on loss of life expectancy due to COVID-19: evidence from Mexico. Can Stud Popul 48:165–200. https://doi.org/10.1007/s42650-021-00051-1
Rönnblom L (2016) The importance of the type I interferon system in autoimmunity. Clin Exp Rheumatol 34:21–24
Manry J, Bastard P, Gervais A et al (2022) The risk of COVID-19 death is much greater and age dependent with type I IFN autoantibodies. Proc Natl Acad Sci U S A 119:e2200413119. https://doi.org/10.1073/pnas.2200413119
Larionova R, Byvaltsev K, Kravtsova O et al (2022) SARS-Cov2 acute and post-active infection in the context of autoimmune and chronic inflammatory diseases. J Transl Autoimmun 5:100154. https://doi.org/10.1016/j.jtauto.2022.100154
Rúa-Figueroa Í, López-Longo J, Galindo-Izquierdo M et al (2017) Incidence, associated factors and clinical impact of severe infections in a large, multicentric cohort of patients with systemic lupus erythematosus. Semin Arthritis Rheum 47:38–45. https://doi.org/10.1016/j.semarthrit.2017.01.010
Palacio-Mejía LS, Hernández-Ávila JE, Hernández-Ávila M et al (2022) Leading causes of excess mortality in Mexico during the COVID-19 pandemic 2020–2021: a death certificates study in a middle-income country. Lancet Reg Heal Am 13:100303. https://doi.org/10.1016/j.lana.2022.100303
Hoff LS, Ravichandran N, Shinjo SK et al (2023) COVID-19 severity and vaccine breakthrough infections in idiopathic inflammatory myopathies, other systemic autoimmune and inflammatory diseases, and healthy controls: a multicenter cross-sectional study from the COVID-19 vaccination in autoimmune diseases. Rheumatol Int 43:47–58. https://doi.org/10.1007/s00296-022-05229-7
Fernández-Ávila DG, Barahona-Correa J, Romero-Alvernia D et al (2022) Impact of COVID-19 pandemic on patients with rheumatic diseases in Latin America. Rheumatol Int 42:41–49. https://doi.org/10.1007/s00296-021-05014-y
International Classification of Diseases (ICD). https://icd.who.int/browse10/2010/en#/. Accessed 10 Jan 2023
Raymond WD, Lester S, Preen DB et al (2021) Hospitalisation for systemic lupus erythematosus associates with an increased risk of mortality in Australian patients from 1980 to 2014: a longitudinal, population-level, data linkage, cohort study. Lupus Sci Med 8:e000539. https://doi.org/10.1136/lupus-2021-000539
Kerola AM, Kazemi A, Rollefstad S et al (2022) All-cause and cause-specific mortality in rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis: a nationwide registry study. Rheumatology 61:4656–4666. https://doi.org/10.1093/rheumatology/keac210
Fagni F, Simon D, Tascilar K et al (2021) COVID-19 and immune-mediated inflammatory diseases: effect of disease and treatment on COVID-19 outcomes and vaccine responses. Lancet Rheumatol 3:e724–e736. https://doi.org/10.1016/S2665-9913(21)00247-2
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Study conception and study supervision: PM-R, CM-R, IE-M and JCS-P. Study design and data analysis: PM-R, CM-P, IE-M and JA-A. Manuscript drafting: PM-R, CM-R, JO-S and ER-L. Critical review of the manuscript: SM-M and MG-C. Data interpretation and manuscript approval: All authors.
Corresponding author
Ethics declarations
Conflict of interest
All authors do not have any conflict of interest.
Ethical approval
The study was reviewed by the Local Ethics Research Committee of the Centro de Investigación Biomédica de Oriente (CIBIOR), Puebla, Mexico (R-2022-2106-011). The results of this study have not been reported in any congress.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised due to retrospective open access order.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Munguía-Realpozo, P., Mendoza-Pinto, C., Etchegaray-Morales, I. et al. Trends in mortality in patients with systemic autoimmune rheumatic diseases (SARD) during the COVID-19 pandemic in Mexico. Rheumatol Int 43, 1611–1619 (2023). https://doi.org/10.1007/s00296-023-05371-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-023-05371-w