
Abstract
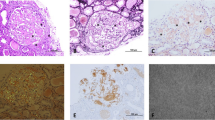
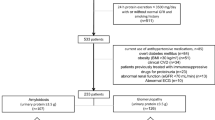
Secondary amyloidosis is the most frequent form of the systemic amyloidosis around the world. Data on frequency and nature of dyslipidemia in patients with secondary amyloidosis are not conclusive. We evaluated the lipid abnormalities and their association with clinical and laboratory characteristics of the patients with secondary amyloidosis. The reports of the kidney biopsies performed in our hospital were reviewed. Clinical and laboratory data of the patients with biopsy-proven secondary amyloidosis were analyzed retrospectively. A total of 102 patients were diagnosed as having secondary amyloidosis. Familial Mediterranean fever was the leading cause of secondary amyloidosis accounting for 42.2 % of the cases. The most frequent indication for kidney biopsy was the nephrotic range proteinuria. The most common clinical and laboratory characteristics at the time of the diagnosis were edema, proteinuria and impaired renal function. The frequency of the nephrotic range proteinuria and microscopic hematuria were 75.5 and 18.6 %, respectively. Dyslipidemia was found in 88 % of the cases. Serum lipids significantly correlated with estimated glomerular filtration rate (eGFR), but not with serum albumin or urine protein levels. We demonstrated that majority of the patients with secondary amyloidosis had serum lipid abnormalities. Dyslipidemia was closely associated with GFR in a manner that patients with advanced stage kidney disease had lower serum lipid levels.


Similar content being viewed by others

References
Glenner GG (1980) Amyloid deposits and amyloidosis. The beta-fibrilloses. N Engl J Med 302(23):1283–1292
Friman C, Pettersson T (1996) Amyloidosis. Curr Opin Rheumatol 8(1):62–71
Röcken C, Shakespeare A (2002) Pathology, diagnosis and pathogenesis of AA amyloidosis. Virchows Arch 440:111–122
Simms RW, Prout MN, Cohen AS (1994) The epidemiology of AL and AA amyloidosis. Baillieres Clin Rheumatol 8(3):627–634
Cohen AS (1968) Amyloidosis associated with rheumatoid arthritis. Med Clin North Am 52(3):643–653
Dilsen N, Konice M, Aral O, Ocal L (1990) The prevalence, importance and significance of amyloidosis with rheumatic diseases in Turkey. In: Natwig JB, Forre O, Husby G et al (eds) Amyloidosis. Kluwer, Dordrecht, pp 870–873
Schwimmer JA, Joseph RE, Appel GB (2003) Amyloid, fibrillary, and the glomerular deposition diseases in therapy. In: Wilcox CS, Brady HR (eds) Nephrology and hypertension. Saunders, Philadelphia, pp 253–261
Falk RH, Skinner M (2000) The systemic amyloidoses: an overview. Adv Intern Med 45:107–137
Husebekk A, Skogen B, Husby G et al (1985) Transformation of amyloid precursor SAA to protein AA and incorporation in amyloid fibrils in vivo. Scand J Immunol 21(3):283–287
Cunnane G (2001) Amyloid proteins in pathogenesis of AA amyloidosis. Lancet 358(9275):4–5
Gertz MA, Kyle RA (1991) Secondary systemic amyloidosis: response and survival in 64 patients. Medicine 70(4):246–256
Joss N, McLaughlin K, Simpson K et al (2000) Presentation, survival and prognostic markers in AA amyloidosis. QJM 93(8):535–542
Lachmann HJ, Goodman HJ, Gilbertson JA et al (2007) Natural history and outcome in systemic AA amyloidosis. N Engl J Med 356:2361–2371
Paydas S (1999) Report on 59 patients with renal amyloidosis. Int Urol Nephrol 31(5):619–631
Appel GB, Radhakrishnan Jai, D’Agati V (2008) Secondary glomerular disease. In: Brenner BM (ed) The kidney. Saunders, Philadelphia, pp 1100–1104
Verine J, Mourad N, Desseaux K et al (2007) Clinical and histological characteristics of renal AA amyloidosis: a retrospective study of 68 cases with a special interest to amyloid-associated inflammatory response. Hum Pathol 38(12):1798–1809
Tuglular S, Yalcinkaya F, Paydas S et al (2002) A retrospective analysis for aetiology and clinical findings of 287 secondary amyloidosis cases in Turkey. Nephrol Dial Transplant 17(11):2003–2005
Bergesio F, Ciciani AM, Santostefano M et al (2007) Renal involvement in systemic amyloidosis–an Italian retrospective study on epidemiological and clinical data at diagnosis. Nephrol Dial Transplant 22(6):1608–1618
Ensari C, Ensari A, Tumer N et al (2005) Clinicopathological and epidemiological analysis of amyloidosis in Turkish patients. Nephrol Dial Transplant 20(8):1721–1725
Hawkins PN, Tan SY, Pepys MB (1998) The patient with amyloid or immunotactoid glomerulopathy. In: Davison AM, Cameron JS, Grünfeld JP, Kerr NSD, Ritz E, Winearls CG (eds) Oxford textbook of clinical nephrology. Oxford University Press, New York, pp 777–810
Nonoguchi H, Kohda Y, Fukutomi R et al (2009) A case with acute renal failure and subsequent nephrotic syndrome. Ren Fail 31(2):162–166
Navarro M, Bonet J, Bonal J et al (2006) Secondary amyloidosis with irreversible acute renal failure caused by visceral leishmaniasis in a patient with AIDS. Nefrologia 26(6):745–746
Amir AR, Sheikh SS (2006) Hodgkin’s lymphoma with concurrent systemic amyloidosis, presenting as acute renal failure, following lymphomatoid papulosis. J Nephrol 19(3):361–365
Huch KM, Wall BM, Cooke CR (1994) Case report: acute renal vein thrombosis in patients with spinal cord injury and secondary amyloidosis. Am J Med Sci 308(2):119–122
Yilmaz MI, Sonmez A, Saglam M et al (2008) ADMA levels correlate with proteinuria, secondary amyloidosis, and endothelial dysfunction. J Am Soc Nephrol 19(2):388–395
Cengiz K, Bakan A, Yilmaz H (2001) Lipoprotein abnormalities in patients with secondary renal amyloidosis. Int Urol Nephrol 32(4):615–619
Attman PO, Samuelsson O, Alaupovic P (2011) The effect of decreasing renal function on lipoprotein profiles. Nephrol Dial Transplant 26(8):2572–2575
Parikh NI, Hwang SJ, Larson MG et al (2006) Cardiovascular disease risk factors in chronic kidney disease: overall burden and rates of treatment and control. Arch Intern Med 166(17):1884–1891
Nasri H (2005) Serum C-reactive protein (CRP) in association with various nutritional parameters in maintenance hemodialysis patients. Bratisl Lek Listy 106(12):390–395
Shoji T, Masakane I, Watanabe Y, Iseki K, Tsubakihara Y, Committee of Renal Data Registry, Japanese Society for Dialysis Therapy (2011) Elevated non-high-density lipoprotein cholesterol (non-HDL-C) predicts atherosclerotic cardiovascular events in hemodialysis patients. Clin J Am Soc Nephrol 6(5):1112–1120
Ortega O, Rodriguez I, Gallar P et al (2002) Significance of high C-reactive protein levels in pre-dialysis patients. Nephrol Dial Transplant 17(6):1105–1109
Mihos CG, Artola RT, Santana O (2012) The pleiotropic effects of the hydroxy-methyl-glutaryl-CoA reductase inhibitors in rheumatologic disorders: a comprehensive review. Rheumatol Int 32:287–294
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Piskinpasa, S., Akoglu, H., Koc, E. et al. Revisiting secondary amyloidosis for an inadequately investigated feature: dyslipidemia. Rheumatol Int 33, 993–999 (2013). https://doi.org/10.1007/s00296-012-2496-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-012-2496-z