
Abstract
We conducted an observational study (FIRE) to understand the effectiveness and safety outcomes of ibrutinib in patients with chronic lymphocytic leukemia (CLL) in France, after a maximum follow-up of five years. Patients were included according to the French marketing authorization in 2016 (i.e. patients with relapsed or refractory CLL or to previously untreated CLL patients with deletion 17p and/or tumor protein p53 mutations unsuitable for chemoimmunotherapy) and could have initiated ibrutinib more than 30 days prior their enrolment in the study (i.e. retrospective patients) or between 30 days before and 14 days after their enrolment (i.e. prospective patients). The results showed that in the effectiveness population (N = 388), the median progression-free survival (PFS) was 53.1 (95% CI: 44.5–60.5) months for retrospective patients and 52.9 (95% CI: 40.3–60.6) months for prospective patients and no difference was shown between the PFS of patients who had at least one dose reduction versus the PFS of patients without dose reduction (p = 0.7971 for retrospective and p = 0.3163 for prospective patients). For both retrospective and prospective patients, the median overall survival was not reached. The most frequent treatment-emergent adverse event of interest was infections (57.6% retrospective; 71.4% prospective). A total of 14.6% of the retrospective patients and 22.4% of the prospective patients had an adverse event leading to death. Our findings on effectiveness were consistent with other studies and the fact that patients with dose reductions had similar PFS than patients without dose reduction is reassuring. No additional safety concerns than those already mentioned in previous studies could be noticed.
Trial registration ClinicalTrials.gov, NCT03425591. Registered 1 February 2018 – Retrospectively registered.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic lymphocytic leukemia (CLL) is the most common leukemia in adults in Western countries [1]. In 2019, the global age-standardized incidence rate was 1.28 cases per 100,000 persons [2]. The median age at diagnosis is 70 years old [3] and the disease is more common in male patients (global sex ratio: 1.4 men/women) [2].
A decade ago, targeted therapies have been developed with ibrutinib, a first-in-class, oral, once daily Bruton’s Tyrosine Kinase inhibitor (BTKi). Such therapies started to progressively replace first chemoimmunotherapy for relapsed CLL patients and then in first line treatment. Ibrutinib has been authorized in Europe in October 2014 and commercialized in France since November 21st, 2014. Currently, it is indicated in Europe for the treatment of all CLL and Waldenström’s macroglobulinaemia adult patients, and for the treatment of relapsed or refractory (R/R) MCL in adult patients [4, 5].
The efficacy of ibrutinib compared to chemoimmunotherapy-based treatment has been largely demonstrated in several clinical trials. Phase-3 studies (RESONATE-2 and RESONATE) showed that previously untreated patients with CLL and R/R CLL had better progression-free survival (PFS) and overall survival (OS) when treated with ibrutinib than with chlorambucil [6] or ofatumumab [7, 8]. Other trials showed similar results in CLL (ALLIANCE: ibrutinib alone or in combination with rituximab versus bendamustine with rituximab; ILLUMINATE: ibrutinib in combination with obinutuzumab versus chlorambucil with obinutuzumab; HELIOS: ibrutinib in combination with bendamustine and rituximab versus bendamustine and rituximab; and GLOW: first-line fixed-duration ibrutinib in combination with venetoclax versus chlorambucil with obinutuzumab) [9,10,11,12].
To complement these clinical trials results, the FIRE study was set up to investigate, in France, in real-life conditions, the effectiveness and safety of ibrutinib treatment in patients with CLL (including small lymphocytic lymphoma (SLL)), along with those with high-risk features (e.g. deletion (del)17p or tumor protein p53 (TP53) mutation; unmutated immunoglobulin heavy chain (IGHV) genes). Results of the second and third interim analyses were previously reported [13, 14]. In the second interim analysis, with a median follow-up of 17.4 months, the findings confirmed effectiveness in R/R patients with high-risk features and did not highlight additional adverse events (AE) than those documented in clinical trials [13, 15]. In the third interim analysis, with a median follow-up of 47.2 months, the results showed that ibrutinib was still an effective treatment for CLL patients and that patients who have received ibrutinib in earlier line of treatment had a better PFS [14]. Again, the effectiveness and safety profiles in this third interim analysis were consistent with the results of clinical trials. In this article, the objective was to report the final results of the FIRE study on effectiveness and safety outcomes for CLL patients, after a maximum follow-up of five years.
Methods
Study design
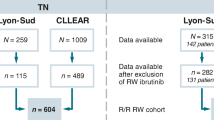
FIRE was a retro-prospective, non-interventional, multicenter study, implemented in France through specialized onco-haematology centres. A total of 65 centres participated in the study. The first CLL patient was included on May 12th, 2016, and the last visit of the last CLL patient occurred on July 26th, 2022. Patients were recruited in the study for about one year and were followed for up to five years.
Patients could have initiated ibrutinib more than 30 days prior their enrolment in the study and been enrolled regardless of whether or not they were still receiving ibrutinib at the time of inclusion (i.e. retrospective patients), or they could have started ibrutinib between 30 days before and 14 days after their inclusion (i.e. prospective patients). The overall design of the study has been provided in Online Resource 1.
Study participants
Adults with a confirmed diagnosis of CLL and who initiated ibrutinib therapy on or after November 21st, 2014, or who planned to initiate ibrutinib within the next 14 days could participate in the study. Patients were included according to the French marketing authorization in 2016, corresponding either to patients with R/R CLL or to previously untreated CLL patients with del17p and/or TP53 mutations unsuitable for chemoimmunotherapy. Patients who were part of the ibrutinib Temporary Authorization for Use, who participated at the same time in another research study and who did not sign the Informed Consent Form were not eligible.
Outcomes
The primary outcome was the progression-free survival (PFS). Secondary outcomes included overall survival (OS), treatment responses, duration of response (DOR), time to best response / first response / next treatment, treatment discontinuation (permanent), dose reductions (i.e. temporary reduction followed by a dose increase or another dose reduction, and permanent dose reductions, but no temporary ibrutinib discontinuations followed by a restart at a lower dose), and safety. The definition of the different endpoints is provided in Online Resource 2. The safety analyses included AEs (i.e. untoward medical occurrence after exposure to a medicine, which is not necessarily caused by that medicine [16]), treatment-emergent adverse events (TEAE), treatment-emergent bleeding events and AEs leading to death.
Data collection
All data were collected through the medical records of the patients. The data were collected at different time points between inclusion and the end of the study (Online Resource 1). For patients who initiated ibrutinib therapy at least 31 days before their enrolment, data were also collected retrospectively except for AEs not related to ibrutinib. All investigators were trained to fill in the Electronic Case Report Form and on the use of the Electronic Data Capture System.
Sample size
We used the following hypothesis to calculate our sample size: a 30-month PFS rate of 76% [15]. Therefore, the PFS at 24 months was estimated to be 80%. Considering this 24-month PFS rate, a rate of censored patients during the first 24 months of 10% and a Confidence Interval (CI) half-width of 4.1%, 400 CLL patients needed to be included to estimate a two-sided 95% CIs for a PFS rate.
Data analysis and statistics
The statistical analysis on effectiveness parameters (e.g. PFS, OS, DOR, etc.) was performed on all included patients who met the inclusion and non-inclusion criteria and who took at least one dose of ibrutinib (effectiveness population). The statistical analysis on safety parameters was performed on all included patients who took at least one dose of ibrutinib (safety population).
Demographic information (i.e. age, gender), medical history and comorbidities, treatment history and subsequent treatment were obtained and summarized as frequency and percentage.
All time-to-event variables (i.e. PFS, OS, DOR, time to first response / best response / next therapy) were analysed using standard survival analysis methods, including Kaplan–Meier product-limit survival curve. Responses were assessed by physicians. The median time to event with two-sided 95% CIs was estimated. In addition, the PFS was also analysed by mutation status (i.e. mutated (del17p and/or TP53) vs. not mutated) and by dose reduction (i.e. patients with at least one dose reduction vs. no dose reduction). For the PFS by dose reduction, an exploratory logrank test with a level of significance of p = 0.05 was used to determine the effectiveness of ibrutinib among those who had at least one dose reduction vs. those who did not. All data were analysed by inclusion type (i.e. retrospective / prospective) with SAS® version 9.4 (SAS Institute, North Carolina, USA).
Results
Patients’ characteristics at ibrutinib initiation
A total of 388 patients was included in the effectiveness analysis (194 retrospective and 194 prospective) (Table 1). Most patients were male (66.5%), ≤ 75 years old (64.9%) and with an ECOG performance status of 0 or 1 (89.6%). Almost half of the patients (48.5%) had at least one medical history and comorbidity. Of those who underwent molecular and cytogenetic assessment, 58.2% (N = 156/268) had del17p and/or TP53 mutation and 30.0% (N = 81/270) del11q mutation. The median time between the initial diagnosis and the start of ibrutinib was 7.0 (range: 0.0–35.0) years. Most patients (85.3%, N = 331) were R/R patients. Among those who were previously treated, the median number of prior therapies was 2 (range: 1–7). All those who were previously untreated for CLL had del17p and/or TP53 mutations.
Effectiveness
For retrospective patients, the median follow-up duration was 59.2 (range: 3.7 – 72.0) months with a median PFS of 53.1 (95% CI: 44.5 – 60.5) months (Table 2). PFS rates were 93.2%, 68.1% and 45.5% at month 12, 36 and 60 respectively (Fig. 1). The median OS was not reached (Table 2 and Fig. 2). The OS rates were 97.9%, 79.7% and 64.5% at month 12, 36 and 60 respectively. The median DOR was 59.5 (95% CI: 56.6 – NA) months (Table 2 and Online Resource 3). The median time to first response, best response and next therapy were 2.8 (95% CI: 2.4–3.0), 8.4 (95% CI: 6.7 – 9.4) and 50.1 (95% CI: 41.9 – 60.1) months (Table 2, Online Resources 4 and 5, and Fig. 3). By 60 months, 96.8% of the retrospective patients had a response to ibrutinib treatment: 40.7% had a complete response and 56.1% a partial response (Table 2). The disease progressed in 34.0% of the cases (until month 60).

Progression-free survival for CLL patients by type of inclusion (Effectiveness population, N = 388)

Time from ibrutinib initiation to overall survival for CLL patients by type of inclusion (Effectiveness population, N = 388)

Time to next therapy, excluding patients restarting ibrutinib as subsequent therapy, for CLL patients by type of inclusion (Effectiveness population, N = 388)
For prospective patients, the median follow-up duration was 58.5 (range: 0.1–68.7) months with a median PFS of 52.9 (95% CI: 40.3–60.6) months (Table 2). PFS rates were 83.5%, 61.1% and 45.1% at month 12, 36 and 60 respectively (Fig. 1). The median OS and the median DOR were not reached (Table 2, Fig. 2 and Online Resource 3). The OS rates were 87.6%, 74.2% and 63.3% at month 12, 36 and 60 respectively (Fig. 2). The median time to first response, best response and next therapy were 2.8 (95% CI: 2.6–2.9), 8.2 (95% CI: 5.0–10.6) and 50.6 (95% CI: 41.9–58.3) months respectively (Table 2, Online Resources 4 and 5, and Fig. 3). By 60 months, 96.6% of the prospective patients had a response to ibrutinib treatment: 38.2% had a complete response and 58.4% a partial response (Table 2). The disease progressed in 29.4% of the cases (until month 60).
When mutation status (del17p and/or TP53) was taken into account, the median PFS for retrospective patients with a mutation was 47.5 (95% CI: 35.8 – NA) months but was not reached for those without mutation (Fig. 4A). PFS rates were 96.3%, 60.4% and 39.3% at month 12, 36 and 60 respectively for those with mutation versus 91.1%, 74.0% and 58.2% for those without. For prospective patients, the median PFS for those with a mutation was 55.4 (95% CI: 34.8 – NA) months but was not reached for those without mutation (Fig. 4B). PFS rates were 87.4%, 60.9% and 44.1% at month 12, 36 and 60 respectively for those with mutation versus 79.6%, 63.1% and 54.5% for those without.

Progression-free survival for CLL patients according to mutation status (del17p and/or TP53) for retrospective patients (a) and prospective patients (b) (Effectiveness population, N = 388)
Dose reduction of ibrutinib
For 91.4% of the retrospective patients and 91.3% of the prospective patients, the daily dose of ibrutinib at initiation was 420 mg with a median overall treatment duration of 42.1 (range: 0.7–66.5) months for retrospective and 39.2 (range: 0.0–63.5) months for prospective patients. For retrospective patients, the median duration of treatment by ibrutinib until inclusion was 9.0 (range: 1.0–24.6) months. More than half of the patients had no dose modifications (56.1% of the retrospective and 58.7% of the prospective patients).
For those who had at least one dose modification (43.9% retrospective and 41.3% prospective), toxicity was the main reason of dosing change (56.3% retrospective and 64.2% prospective). Among those who had at least one dose reduction (36.1% retrospective and 37.1% prospective patients), the mean number of dose reduction was 1.5 (SD = 0.7) for retrospective patients and 1.3 (SD = 0.7) for prospective patients with a mean duration of 10.3 months (SD = 10.3) and 8.8 months (SD = 9.0) respectively. The PFS for patients with at least one dose reduction was 55.2 (95% CI: 39.7 – NA) months for the retrospective group and 49.1 (95% CI: 40.3 – NA) months for the prospective group versus 49.4 (95% CI: 44.5–61.5) and 52.9 (95% CI: 30.9-NA) months, respectively, for those with no dose reduction (63.9% retrospective and 62.9% prospective patients) (p = 0.7971 retrospective and p = 0.3163 prospective) (Table 2, Fig. 5A and B). The median time between treatment instauration and first dose reduction as first dose modification was 7.4 (range: 0.4–60.9) months for retrospective patients (N = 43) and 9.3 (range: 0.4–57.4) months for prospective patients (N = 51) (Table 2).

Progression-free survival for CLL patients with at least one ibrutinib dose reduction versus no dose reduction for retrospective patients (a) and prospective patients (b) (Effectiveness population, N = 388)
Overall, permanent ibrutinib discontinuation was observed in 119 retrospective patients (60.1%) and in 127 prospective patients (64.8%) (Table 2). The median time from ibrutinib initiation to permanent discontinuation was 28.7 (range: 0.7–62.8) months for retrospective patients and 18.0 (range: 0.1–61.1) months for prospective patients, and the main reasons for discontinuation were toxicity (43.5% retrospective and 42.0% prospective), disease progression (33.0% retrospective and 32.8% prospective) and death (5.2% retrospective and 10.1% prospective). Among retrospective patients who discontinued ibrutinib because of toxicity (N = 50), 5 (10.0%) patients had no prior line of treatment, 18 (36.0%) one prior line and 27 (54.0%) at least two prior lines. Among prospective patients (N = 50), 7 (14.0%) had no prior line of treatment, 21 (42.0%) one prior line and 22 (44.0%) two prior lines or more. After ibrutinib treatment, less than half (41.9% of the retrospective and 33.2% of the prospective patients) received a subsequent therapy (Table 1). The most frequent subsequent treatment was Venetoclax ± Rituximab for 54.2% of the retrospective and for 49.2% of the prospective patients. Ibrutinib was retaken by 14.5% of the retrospective and by 18.4% of the prospective patients.
Safety
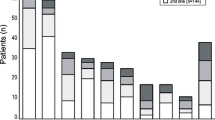
Almost all patients (85.9% of the retrospective and 99.5% of the prospective patients) had at least one TEAE (Table 3). For 17.7% of the retrospective and for 30.1% of the prospective patients, TEAEs were related to ibrutinib and considered by the investigators as serious. The most frequent TEAEs of interest were infections (57.6%), neoplasms (18.7%), diarrhoea (16.2%), and hypertension (14.6%) for retrospective patients and infections (71.4%), diarrhoea (28.6%), arthralgia/myalgia (26.5%) and neoplasms (26.0%) for prospective patients. A total of 16 retrospective patients (8.1%) and 22 prospective patients (11.2%) had atrial fibrillation or flutter. Regarding treatment-emergent bleeding event, 28.8% of the retrospective patients and 54.1% of the prospective patients had such events, and more bleeding events were noticed among patients under antithrombotic treatment. Bleeding events were considered as major for 2.0% of the retrospective patients and for 8.2% of the prospective patients. A total of 14.6% of the retrospective and 22.4% of the prospective patients had at least one AE leading to death with the most important preferred terms being general physical health deterioration for both groups (3.5% for retrospective and 2.0% for prospective patients) as well as septic shock (2.0%), sepsis (2.0%) and Richter’s transformation (2.0%) for prospective patients (Table 4). Other AEs leading to death are detailed in Table 4.
Discussion
Although clinical trials have always been the gold standard of proof regarding effectiveness and safety of new drugs, there is nowadays a great interest in real-world research since they represent patients in real-life settings. To our knowledge, FIRE was the largest French real-word study that assessed the effectiveness and safety of ibrutinib, in accordance with the French marketing authorization in 2016, for the treatment of CLL/SLL in patients who received at least one prior line of treatment, or who were previously untreated and had a del17p and/or TP53 mutation unsuitable for chemoimmunotherapy. In this extensive study, set up in 65 centres, 388 CLL/SLL patients (194 retrospective and 194 prospective) were included in the effectiveness population and followed-up for five years.
Our results are consistent with previous effectiveness findings [17, 18]. In a real-world multicenter retrospective study, conducted on 205 CLL patients treated with ibrutinib, the 12-months PFS and OS rates were 86.3% and 88.8% respectively [17]. In another study on long-term efficacy and safety with a median follow-up of 5 years, in which 31 treatment-naïve and 101 R/R patients were included, the median PFS in R/R patients was 51 months with a 5-year PFS rate of 44% [18]. The median OS was not reached and the OS rate at 5 years was 60%. In a UK/Ireland-based study, the one-year OS was 83.8% [19]. In the clinical trial RESONATE, only R/R CLL patients were included. When comparing the results at similar timepoints between RESONATE and FIRE, the one-year PFS and OS rates in RESONATE (84% and 90% respectively) as well as the 5-year PFS (40.0%) were similar to those of FIRE [7, 8, 20]. The ORR was also similar: 91% in RESONATE vs. 96.8% and 96.6% for retrospective and prospective patients, respectively, in FIRE [8] (Online Resource 6). However when comparing median PFS and OS, those in RESONATE were lower: 44.1 (95% CI: 38.5–56.2) months for the median PFS and 67.7 (95% CI: 61.0 – not reached) months for the median OS [8] (Online Resource 6). One explanation could be the longer follow-up period in RESONATE (6 years vs. 5 years). However, taking the fact that our results are included in the confidence intervals of the PFS and OS of RESONATE, our finding are consistent. Therefore, although the FIRE population is slightly different than the population in RESONATE (e.g. age, ECOG PS, mutations status, number of prior therapies), it is reassuring to see that our effectiveness results are similar to the results of clinical trials.
Our efficacy results showed that patients with at least one dose reduction had a similar PFS than patients with no dose reduction, supporting the fact that CLL patients in France are well managed, follow-up and treated. Our results not only confirm those of previous real-world studies [19, 21, 22] but also encourage the idea that ibrutinib can still be administrated to patients presenting AEs. Therefore, if physicians need to modify the dose because of an AE, dose reduction may be the best option. Suggesting dose reductions to patients in need of dose modifications will thus reduce treatment discontinuation, increase patient adherence, improve patients outcome and on a long-term strategy decrease financial and economic burden. However, to obtain the best benefit from ibrutinib, it is important to promptly identify and manage AEs, and understand specific AEs that can be associated with the need for dose reductions.
The median time to first dose reduction was assessed in a retrospective chart review on first line and R/R CLL patients treated with ibrutinib either in academic practice or community network [23]. Their results (median time of 3.6 months overall) were lower than ours (7.4 and 9.3 months for retrospective and prospective patients respectively). Furthermore, a review on ibrutinib dose modifications in the management of CLL mentioned that in real-world settings, dose reductions over the first year was often noticed [24]. However, addressing the question of time in dose reduction still remains rare and unclear. Therefore, further research on this topic is necessary in order to better understand the role of time in dose reductions and ibrutinib outcome.
Moreover, our results showed that among patients who discontinued ibrutinib, toxicity was the main reason for around 40.0% of them. These results were similar to the one found in a Swedish retrospective study: 40.4% (19/47) [21]. However, a Danish retrospective study showed a higher rate: 54.7% (47/86) [17]. In RESONATE, the discontinuation rate due to toxicity was much lower 21.1% (32/152) (Online Resource 6). One explanation to this lower discontinuation rate due to AEs compared to the FIRE study could be that RESONATE is a clinical trial with eligibility criteria which promote inclusion of selected patient. Closer monitoring in clinical trials could be also another explanation. Although our results on discontinuation rates due to AEs differed from the one found in RESONATE, they illustrate the need of real-world research on long-term safety on heterogeneous population.
Among AEs noticed in our study, patients reported low rate of major bleeding events (2.0% retrospective and 8.2% prospective). This rate was five times less for retrospective patients but similar for prospective patients than the rate reported in RESONATE (10.0%) [8]. Of note, in FIRE, more patients had a bleeding / major bleeding event when they were under antithrombotic treatment. Explanations could be that bleeding events are side effects of such treatments, and in RESONATE, patients under anticoagulation containing warfarin were excluded. In addition, the rate of atrial fibrillation was similar for patients in the two studies (FIRE: 8.1% for retrospective and 11.2% for prospective patients; RESONATE: 12.0%) but the rate of hypertension was lower in FIRE than in RESONATE (FIRE: 14.6% for retrospective and 14.8% for prospective; RESONATE: 21.0%) [8]. Nevertheless, it is reassuring to see that there was no new AE observed and that the safety profile of ibrutinib in our study seems to be consistent with previous studies.
Finally, while the development and distribution of ibrutinib has transformed treatment expectations for CLL patients, at the time when our study was set up, in 2016, ibrutinib was used only in monotherapy, and therefore, patients usually needed to be continuously treated until disease progression or onset of AEs. Being continuously treated has several consequences, and hence, to reverse the situation and stop treatment once the illness is in remission, fixed-duration ibrutinib-combination therapies have been developed and had shown promising results [25, 26]. For instance, the GLOW clinical trial showed a 42-month PFS rate of 74.6% for previously untreated CLL patients under fixed-duration ibrutinib-venetoclax therapy, higher than our results in monotherapy at 42 months (± 60% for retrospective patients and slightly less than 60% for prospective patients), and similar findings on fatal AEs [25]. However, although GLOW is a clinical trial and had different inclusion criteria than ours, and therefore direct comparison should be done with caution, positive impacts of ibrutinib-combination treatment at fixed-durations still seem to add a real value to ibrutinib treatment as monotherapy which are encouraging for both patients and further research.
Our study has several strengths and limitations. First, FIRE was the largest real-word study on the effectiveness and safety of ibrutinib in France. Second, because of its real-world design, effectiveness and safety parameters were presented through descriptive data in a “real-life condition”, and therefore, our results complement those of clinical trials. Moreover, all consecutive patients who met the eligibility criteria and who had therapy-demanding disease were considered for inclusion in order to reduce selection bias. However, there might have been a bias in effectiveness results between retrospective and prospective patients since retrospective patients who died before enrolment were not included. Therefore, retrospective patients who were included in the study should be considered in “better” health than prospective patients. Nevertheless, it is reassuring to see that the results between the two groups are quite similar. In addition, because of the exclusion of retrospective patients who died before enrolment, it was difficult to pull data of retrospective patients together with the data of prospective patients. Furthermore, the number of AEs for retrospective patients have been underestimated since TEAEs that occurred before inclusion and that were not related to ibrutinib were not collected for these patients. Finally, our focus was on the effectiveness and safety profile of ibrutinib. Therefore, other aspects such as the quality of life of patients under ibrutinib were not considered in this article. Although data on quality of life might have been informative and complement the findings of this article, this whole topic will be discussed in a separate paper.
Conclusion
In conclusion, FIRE was a large real-word study, with a long follow-up period, that included many centres and CLL patients, and showed the effectiveness of ibrutinib on the PFS and OS, as well as on other effectiveness parameters. Dose modifications were mainly attributed to toxicity. However, it is reassuring to see that patients who had at least a dose reduction had a similar PFS than patients with no dose reduction, implying the fact that ibrutinib can still be administrated in case of AEs. No additional safety concerns than those already mentioned in other studies could be noticed. Finally, our results not only complement those of clinical trials, but they are also consistent with both results of clinical trials and other real-world studies.
Data availability
The data-sharing policy of the Janssen Pharmaceutical Companies of Johnson & Johnson is available at www.janssen.com/clinical-trials/transparency. Requests for access to the data from selected studies can be submitted through the Yale Open Data Access (YODA) Project site at yoda.yale.edu.
References
Hallek M (2017) Chronic lymphocytic leukemia: 2017 update on diagnosis, risk stratification, and treatment. Am J Hematol 92:946–965
Ou Y, Long Y, Ji L et al (2022) Trends in disease burden of chronic lymphocytic leukemia at the global, regional, and national levels from 1990 to 2019, and projections until 2030: a population-based epidemiologic study. Front Oncol 12:840616
The Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute. Cancer Stat Facts: Leukemia – Chronic Lymphocytic Leukemia (CLL). https://seer.cancer.gov/statfacts/html/clyl.html. Accessed 25 April 2023
Janssen-Cilag International NV (2014) IMBRUVICA [Summary of Product Characteristics]. Beerse, Belgium
European Medicines Agency. Imbruvica. https://www.ema.europa.eu/en/medicines/human/EPAR/imbruvica. Accessed 20 April 2023
Burger JA, Barr PM, Robak T et al (2020) Long-term efficacy and safety of first-line ibrutinib treatment for patients with CLL/SLL: 5 years of follow-up from the phase 3 RESONATE-2 study. Leukemia 34:787–798
Byrd JC, Brown JR, O’Brien S et al (2014) Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med 371:213–223
Munir T, Brown JR, O’Brien S et al (2019) Final analysis from RESONATE: Up to six years of follow-up on ibrutinib in patients with previously treated chronic lymphocytic leukemia or small lymphocytic lymphoma. Am J Hematol 94:1353–1363
Woyach JA, Ruppert AS, Heerema NA et al (2018) Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N Engl J Med 379:2517–2528
Chanan-Khan A, Cramer P, Demirkan F et al (2016) Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double-blind, phase 3 study. Lancet Oncol 17:200–211
Moreno C, Greil R, Demirkan F et al (2019) Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in frst-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 20:43–56
Niemann C, Munir T, Moreno C et al (2022) Residual disease kinetics among patients with high-risk factors treated with first-line fixed-duration ibrutinib plus venetoclax (Ibr+Ven) versus chlorambucil plus obinutuzumab (Clb+O): the glow study. Blood 140:228–230
Dartigeas C, Slama B, Doyle M et al (2022) FIRE study: real-world effectiveness and safety of ibrutinib in clinical practice in patients with CLL and MCL. Clin Hematol Int 4:65–74
Dartigeas C, Ysebaert L, Feugier P et al (2022) Overall and subgroup results from the third interim analysis of FIRE, a real-world study of ibrutinib treatment for CLL/SLL in France. Blood 140(S1):9906–9907
Byrd JC, Furman RR, Coutre SE et al (2015) Three-year follow-up of treatment-naive and previously treated patients with CLL and SLL receiving single-agent ibrutinib. Blood 125:2497–2506
European Medicines Agency. Adverse Event. https://www.ema.europa.eu/en/glossary/adverse-event#:~:text=An%20untoward%20medical%20occurrence%20after,necessarily%20caused%20by%20that%20medicine. Accessed 25 January 2024
Aarup K, Rotbain EC, Enggaard L et al (2020) Real-world outcomes for 205 patients with chronic lymphocytic leukemia treated with ibrutinib. Eur J Haematol 105:646–654
O’Brien S, Furman RR, Coutre S et al (2018) Single-agent ibrutinib in treatment-naive and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood 131:1910–1919
UK Cll Forum (2016) Ibrutinib for relapsed/refractory chronic lymphocytic leukemia: a UK and Ireland analysis of outcomes in 315 patients. Haematologica 101:1563–1572
Brown JR, Hillmen P, O’Brien S et al (2014) Updated efficacy including genetic and clinical subgroup analysis and overall safety in the phase 3 RESONATETM trial of ibrutinib versus ofatumumab in previously treated chronic lymphocytic leukemia/small lymphocytic lymphoma. Blood 124:3331–3331
Winqvist M, Andersson P-O, Asklid A et al (2019) Long-term real-world results of ibrutinib therapy in patients with relapsed or refractory chronic lymphocytic leukemia: 30-month follow up of the Swedish compassionate use cohort. Haematologica 104:e208–e210
Mato AR, Timlin C, Ujjani C et al (2018) Comparable outcomes in chronic lymphocytic leukaemia (CLL) patients treated with reduced-dose ibrutinib: results from a multi-centre study. Br J Haematol 181:259–261
Hou J-Z, Ryan K, Du S et al (2021) Real-world ibrutinib dose reductions, holds and discontinuations in chronic lymphocytic leukemia. Future Oncol 17:4959–4969
Hardy-Abeloos C, Pinotti R, Gabrilove J (2020) Ibrutinib dose modifications in the management of CLL. J Hematol Oncol 13:66
Niemann C, Munir T, Moreno C et al (2023) Fixed-duration ibrutinib-venetoclax versus chlorambucil-obinutuzumab in previously untreated chronic lymphocytic leukaemia (GLOW): 4-year follow-up from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 24:1423–1433
Tam C, Allan JN, Siddiqi T et al (2022) Fixed-duration ibrutinib plus venetoclax for first-line treatment of CLL: primary analysis of the CAPTIVATE FD cohort. Blood 139:3278–3289
Acknowledgements
We would like to thank all patients who participated in this study as well as the FIRE investigators group and staff from the study centres. Medical writing assistance and statistical analysis were provided by ICTA PM (medical writing: Joëlle Castellani, PhD; statistical analysis: Simon Paternotte and Edwige Yon).
Investigators of the FIRE Study are listed by alphabetical order:
ADIKO Didier (Hôpital Robert Boulin, Libourne), AGAPE Philippe (Institut de Cancérologie René Gauducheau, Saint Herblain), AUGER QUITTET Sophie (Clinique Clémentville, Montpellier), BAREAU Benoît (Policlinique Sevigne, Cesson-Sévigné), BENBRAHIM Omar (Centre Hospitalier Régional d’Orléans, La Source), BERNARD Philippe (Clinique Sainte-Marguerite, Hyères), BESCOND Charles (Centre Hospitalier de Cholet, Cholet), BIJOU Fontanet (Institut Bergonie, Bordeaux), BOUDIN Laurys (Service de Santé des Armées, Toulon), CAILLERES Sylvie (Centre Hospitalier d’Aix-en-Provence, Aix-en-Provence), CALMETTES Claire (Centre Hospitalier de Périgueux, Périgueux), CARTRON Guillaume (Hôpital Saint-Eloi, Montpellier), COSTELLO Régis (Hôpital de la Conception, Marseille), DAVID Selva (Hôpital Privé du Grand Narbonne, Montredon des Corbières), DELAUNAY Jacques (Centre Catherine de Sienne, Nantes), DELETTE Caroline (Hôpital Sud, Salouel), DELMER Alain (Centre Hospitalier Universitaire de Reims, Reims), DENNETIERE Sophie (Centre Hospitalier de Compiègne, Compiègne), DRENOU Bernard (Hôpital Emile Muller, Mulhouse), EL YAMANI Abderrazak (Centre Hospitalier de Blois, Blois), FITOUSSI Olivier (Policlinique Bordeaux Nord Aquitaine, Bordeaux), FLECK Emmanuel (Hôpital Saint-Louis, La Rochelle), FLEURY Joël (Pole Santé République, Clermont-Ferrand), GUTNECHT Jean (Centre Hospitalier Intercommunal de Fréjus Saint-Raphaël, Fréjus), HACINI Maya (Centre Hospitalier Métropole Savoie Chambéry, Chambéry), JOURDAN Éric (Hôpital Caremeau, Nîmes), KAPHAN Régis (Hôpital Pierre Nouveau, Cannes), KARSENTI Jean-Michel (Hôpital de l’Archet, Nice), LABOUREY Jean-Luc (Centre Hospitalier de Carcassonne, Carcassonne), LAUNAY Vincent (Hôpital Yves le Foll, Saint-Brieuc), LE CALLOCH Ronan (Centre Hospitalier de Cornouaille, Quimper), LEDUC Isabelle (Centre Hospitalier d’Abbeville, Abbeville), LEFRERE François (Hôpital Necker Enfants Malade, Paris), LE GALL Stevan (Centre Hospitalier Intercommunal des Alpes du Sud, Gap), LE GOFF Marielle (Clinique Victor Hugo, Le Mans), LEGOUFFE Éric (Institut de Cancérologie – Centre ONCOGARD, Nîmes), LE GOUILL Steven (Hôpital Hotel Dieu et HME, Nantes), LEPRETRE Stéphane (Centre Henri Becquerel, Rouen), LIU Jixing (Centre Hospitalier de Valence, Valence), LUTTIAU MOTARD Carine (Centre Hospitalier Georges Renon, Niort), MOLDOVAN Marius (Hôpital Nord Franche Comté, Belfort), MOLINA Lysiane (Centre Hospitalier Universitaire Grenoble, Grenoble), MOULLET Isabelle (Clinique de la Sauvegarde, Lyon), PEYRADE Frédéric (Centre Antoine Lacassagne, Nice), QUITTET Philippe (Centre Hospitalier d’Alès, Alès), RE Daniel (Hôpital d’Antibes Juan les Pins, Antibes), ROLAND Virginie (Hôpital Saint-Jean, Perpignan), ROOS-WEIL Damien (Centre Hospitalier Pitié Salpetrière, Paris), SAAD Alain (Centre Hospitalier de Béziers, Béziers), SAAD Hussam (Hôpital Augustin Morvan, Brest), SENECAL Delphine (Medipole de Savoie, Challes-les-Eaux), THANNBERGER Alexia (Hôpital Broussais, Saint-Malo), THIEBLEMONT Catherine (Hôpital Saint-Louis, Paris), TOURNILHAC Olivier (Centre Hospitalier Estaing, Clermont-Ferrand), VISANICA Sorin (UNEOS – Hôpital Robert Schuman, Vantoux).
Funding
This study, including statistical support and writing assistance, was sponsored by Janssen-Cilag Ltd.
Author information
Authors and Affiliations
Consortia
Contributions
VL provided the study design. Investigation and data collection were performed by CD, AQ, LY, MSD, BA, BS, KLD, ST, ET, HO, LV, SG, JVM, PF and VL. SD and MD contributed to data interpretation. VL, SD and MD contributed to the manuscript preparation. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Since this study was non-interventional, no approval from an Ethics Committee was needed in France at the time that the study was set up (before the implementation of the Jardé Law). However, the study was conducted in accordance with the principles stated in the Declaration of Helsinki and an Informed Consent Form was obtained from all patients prior their participation in the study.
Competing interests
CD has received honoraria from Abbvie, AstraZeneca, Beigene, Janssen and Lilly. AQ has received honoraria from Abbvie, AstraZeneca, Beigene and Janssen. LY has received honoraria from Abbvie, AstraZeneca, Beigene, BMS/Celgene, Gilead/Kite, Janssen and Roche. MSD has received honoraria from Abbvie, Astra Zeneca, Beigene and Janssen. KLD has received honoraria from Janssen, Abbvie, AstraZeneca, Roche, Incyte and Takeda. ET has received honoraria from Abbvie, AstraZeneca, Beigene and Janssen. PF has received honoraria from Abbvie, Amgen, AstraZeneca, Beigene, Gilead, Janssen and LoxoLilly. VL has received honoraria from Abbvie, Astra Zeneca, Amgen, MSD, Janssen, Beigene and Lilly. SD is an employee of Janssen and reports stock ownership of Johnson & Johnson. MD is an employee of Janssen. BA, BS, ST, HO, LV, SG, and JVM have nothing to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dartigeas, C., Quinquenel, A., Ysebaert, L. et al. Final results on effectiveness and safety of Ibrutinib in patients with chronic lymphocytic leukemia from the non-interventional FIRE study. Ann Hematol (2024). https://doi.org/10.1007/s00277-024-05666-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00277-024-05666-3