
Abstract
The middle fossa, cavernous sinus, and paraclival triangles consist of ten triangles. Their use in a surgical approach is vast; most are used as landmarks to access and identify other structures of surgical interest. Multiple labels, borders, and contents mentioned by different authors make understanding and reproduction challenging and confusing. This study aims to organize and clarify recent or most relevant publications and disclose our portrayal of the ten triangles using cadaveric dissection and simple and practical figures. Four middle fossa triangles, four cavernous sinus triangles, and two paraclival triangles were dissected and delineated in a cadaveric specimen. Drawings were simplified to eliminate confusion and evaluate the triangles effortlessly. Similarities and differences in triangle names, border limits, and contents are described in a precise form. The recognition of triangle landmarks allows for treating pathologies in a frequently distorted anatomy or challenging to access structure. That is why an accurate knowledge of the surgical anatomy should be mastered, and a safe approach should be accomplished.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
For years, there has been confusion when determining the name and border descriptions of the cavernous sinus and middle fossa triangles. Various authors have mentioned multiple names, border defining limits, and contents that cause confusion and learning distrust. For this reason, we present a brief revision of history, triangle differences, and similarities described in different publications. Finally, we explain a knowledgeable description using our point of view concerning each triangle using cadaveric dissection and simple figures.
Multiple publications mention the practical use of the triangles. Escudeiro et al. describe the utilization of the Parkinson´s triangle to access a cavernous sinus hemangioma [7]. Kusumi et al. used an extra-dural middle fossa approach to remove a schwannoma in the Glasscock triangle [21]. Ferrareze et al. performed an endoscopic endo-nasal approach through the oculomotor triangle to remove an extended pituitary tumor in the para-peduncular space [8]. Watanabe et al. access the anterior temporal fossa to the paranasal sinuses and nasal cavities through the anterolateral and anteromedial triangles in a microscopic and endoscopic approach [30]. For this reason, recognizing and comprehending the ten triangles´ anatomy are critical to a safe and successful surgical approach.
Materials and methods
We used a cadaveric specimen injected with red silicon for arteries and blue for veins. Specimen preserved in a 70% alcohol solution and refrigerated. A head holder was used to keep the head in the correct position. A Pico microscope (Zeiss) was used for intracranial visualization. Midas drill (Medtronic) was used to perform a cranio-orbital approach. Microsurgical instruments, bipolar, and 11 scalpels were used. Dissection was documented step by step with a DCLR camera Sony A6300. Additional processing was done with Photoshop (Adobe) and Helicon Focus. Dissection was made at the laboratory of the Centre Hospitalier Universitaire Vaudois.
We searched PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) for “cavernous sinus triangles,” “middle fossa triangles,” “paraclival triangles,” “oculomotor triangle,” “clinoidal triangle,” supratrochlear triangle,” “infratrochlear triangle,” “anteromedial triangle,” “anterolateral triangle,” “posteromedial triangle,” “posterolateral triangle,” inferomedial triangle” and “inferolateral triangle.” The most relevant or recently published articles were used. Also, remarkable book literature was considered. The name, borders, and contents were analyzed (Table 1).
According to our cadaveric specimens, digital drawings of the ten triangles were optimized and simplified, eliminating distracting surroundings. The digital application platform “Procreate” was used in all drawings.
Results
Oculomotor triangle
The oculomotor triangle (Hakuba´s triangle and medial triangle) is delimited by three dural folds forming the medial or interclinoid border, lateral or anterior petroclinoid border, and posterior, base, or posterior petroclinoid border. In addition to surrounding the entry point of the third cranial nerve to the roof of the cavernous sinus, it contains the horizontal portion of the intra-cavernous segment of the internal carotid artery (ICA) [5, 6, 10, 14] (Figs. 1, 2, 4) (Table 1).
Clinoid triangle
The clinoid triangle (Dolenc´s triangle, anteromedial triangle, and anterior triangle) is bounded on its medial border by the optic nerve, the lateral border by a line from the point of entry of the third cranial nerve in the roof of the cavernous sinus to its point of entry in the superior orbital fissure, and the posterior border, corresponding to a line joining the posterior limits of the medial and lateral borders. To visualize this triangle fully, it is necessary to drill the anterior clinoid process. It contains in its anterior portion the optic strut, in its medial portion the clinoid segment of the ICA, and in its posterior segment the roof of the cavernous sinus. [5, 6, 9, 10, 15] (Figs. 1, 2, 3, 4, 5) (Table 1).

Anterolateral aspect of the middle cranial fossa depicting the triangles formed in this region. The roof and lateral aspect of the orbit have been drilled. The Sylvian fissure is shown splittled. The retractor is over the temporal lobe. From medial to lateral, the clinoidal triangle has been exposed after an anterior clinoidectomy has been done. It is between the optic and the oculomotor nerves and posteriorly bordered by the tentorial edge (Not shown). The oculomotor triangle (OM) is the site where the oculomotor nerve becomes extradural by entering the upper portion of the lateral wall of the cavernous sinus. Its margins are the anterior petroclinoial dural fold extending from the ACP to the petrous apex and the posterior petroclinoidal dural folds extending from the posterior clinoidal process to the petrous apex and medially by the interclinoidal dural fold. The supratrochlear triangle (ST), the space between the oculomotor and the trochlear nerves, has a posterior border drawn by a line at the dural entry point of these two nerves. The infratrochlear triangle (IT/Parkinson’s triangle) is lateral to the oculomotor and medial to the trochlear nerve. Its posterior border is the tentorial edge between these two nerves. The anteromedial triangle’s (AM/Mullan’s triangle) boundaries are the ophthalmic division of the trigeminal nerve medially and the maxillary division laterally. Its base is formed by a line connecting the superior orbital fissure to the foramen rotundum over the bony middle cranial fossa wall. The anterolateral triangle (AT) is formed medially by the maxillary division of the trigeminal nerve and laterally by the mandibular division (V3). The base is formed by a line connecting the foramen rotundum and the foramen ovale. Posteriorly over the middle cranial fossa, the Posteromedial and the posterolateral triangles can be found. The first of these two, the Posteromedial Middle Fosa Triangle (AKA Kawase’s triangle), is bordered laterally by the medial margin of the greater superficial petrosal nerve (GSPN). The petrous ridge is found medially. Anteriorly its boundary is the mandibular division of the trigeminus and laterally by V3. Posteriorly, the limit is the arcuate eminence. The posterolateral middle fossa triangle (Glasscock) is located laterally to the line where the GSPN crosses under V3 and the foramen spinosum. Its lateral border is a line between the foramen spinosum and the geniculate ganglion. Its base is GSPN. The paraclival triangles are the Inferomedial and Inferolateral triangles (PCIM and PCIL). The inferomedial triangle contains the dura forming the posterior wall of the cavernous sinus. It is delimited medially by a line extending from the posterior clinoid process to the dural entry of the abducens nerve. Its lateral border is a line extending from the posterior clinoid process to the dural entry of the trochlear nerve. Its base is the line extending from the dural entry of the abducens nerve and the trochlear nerve. Over the posterior surface of the clivus and the temporal bone, we can find the Inferolateral triangle (PCIL). Its anterior border is a line extending from the dural entry of the abducens nerve and the trochlear nerve's dural entry. Its lateral border is a line extending from the entrance of the trochlear nerve and the petrosal vein. Its posterior border is a line extending from the dural entry of the abducens nerve to the petrosal vein

Oculomotor triangle: It is bordered anteriorly and posteriorly by the dural folds attached to the petrous apex and connected to the anterior clinoid process and posterior clinoid process (Anterior Petroclinoidal and Posterior petroclinoidal dural folds), respectively. Medially, its limit is the interclinoidal dural fold

Clinoidal triangle (Dolenc’s, Anteromedial triangle); Bordered on its lateral side by the oculomotor nerve and limited medially by the optic nerve, posteriorly limited by the tentorial edge

Drawing depicting the disposition of the triangles on the lateral wall of the cavernous sinus and middle cranial fossa

Anatomical dissection depicting the disposition of the triangles on the lateral wall of the cavernous sinus and middle cranial fossa
Supratrochlear triangle
The supratrochlear triangle (para-median triangle, para-medial triangle, superior triangle, and Fukushima´s triangle) corresponds to the space between the oculomotor and trochlear nerves at their medial and lateral borders, respectively, forming the posterior border with a line at the dural entry point of these nerves. Through this triangle, we can find the posterior curvature of the intra-cavernous segment of the ICA and, in some cases, the exit of the meningohypophyseal trunk, the inferolateral trunk, and, less frequently, the medial curve of the ICA. [5, 6, 11, 14, 28] (Figs. 4, 5, 6) (Table 1).

Supratrochlear triangle: Space bordered medially by the oculomotor nerve, laterally by the trochlear nerve. Its posterior border is the tentorial edge delimited by the dural entry point of these two nerves
Infratrochlear triangle
The infra-trochlear triangle (Parkinson's triangle, supero-lateral triangle) is bounded medially by the trochlear nerve, laterally by the ophthalmic division of the trigeminal nerve, and posteriorly by a line joining the posterior limit of the medial and lateral borders. It generally contains the origin of the meningohypophyseal trunk and the intra-cavernous portion of the sixth cranial nerve [4,5,6, 14, 17, 24, 29] (Figs. 1, 4, 5, 7) (Table 1).

Infratrochlear triangle (Parkinson’s triangle) Over the lateral wall of the cavernous sinus. This space is bordered medially by the trochlear nerve and laterally by the ophthalmic division of the trigeminal nerve. The base of this triangle is drawn by the tentorial between these two nerves
Anteromedial triangle
The anteromedial triangle’s (Mullan´s triangle and anterolateral) boundaries are formed by the ophthalmic division of the trigeminal nerve medially and the maxillary division of the trigeminal nerve laterally. The triangle base consists of the anterolateral wall of the bony middle cranial fossa formed by a line connecting the superior orbital fissure to the foramen rotundum. This corridor is well suited for exposing several important structures, including the superior orbital vein, sixth cranial nerve, sphenoid sinus, and ophthalmic vein. Further dissection within Mullan’s space allows for access to carotid-cavernous fistulas [3, 5, 12, 13, 26, 29] (Figs. 1, 4, 5, 8) (Table 1).

Anteromedial triangle (Mullan’s triangle); Its boundaries are the ophthalmic division of the trigeminal nerve medially and the maxillary division of the trigeminal nerve laterally. This space’s base is a line that connects the superior orbital fissure to the foramen rotundum over the bony middle cranial fossa
Anterolateral triangle
The anterolateral triangle (lateral triangle, far lateral triangle, lateral-most triangle) is formed medially by the maxillary division and laterally by the mandibular division of the trigeminal nerve. The base is identified via a line connecting the foramen rotundum and foramen ovale. The contents are the lateral wing of the sphenoid sinus, the Vidian nerve, and the pterygoid region. Far antero-inferior, the maxillary sinus can be exposed, and posteriorly, the infratemporal Eustachian tube can be exposed under the lateral and medial pterygoid muscles. This space exposes the lateral sphenoid wing, sphenoidal emissary vein, and cavernous-pterygoid venous anastomosis [4, 5, 12, 19, 25, 26, 29] (Figs. 1, 4, 5, 9) (Table 1).

Anterolateral triangle; The lower margin of the maxillary nerve constitutes its medial border. The upper surface of the mandibular nerve is the lateral border. Anteriorly its base is a line between the foramen ovale and foramen rotundum
Posterolateral triangle
The posterolateral triangle (Glasscock´s triangle and Paullus´s triangle) is formed by the anteromedial side of the lateral surface of the mandibular nerve distal to the point at which the greater superior petrosal nerve (GSPN) crosses below the lateral surface of the trigeminal nerve. The anterior margin of the GSPN forms the posterolateral side. It opens laterally to encompass the floor of the middle cranial fossa between these two structures [1]. It contains the posterior and lateral loops of the ICA in its petrous segment, greater and lesser petrosal nerves, tensor tympani muscle, Eustachian tube, and middle meningeal artery that passes through the foramen spinosum. Opening the floor of this triangle exposes the infratemporal fossa [5, 14, 28, 29] (Figs. 1, 4, 5, 10) (Table 1).

Posterolateral triangle (Glasscock, Paullus); Bordered medially by a line drawn between the point where the greater superficial petrosal nerve (GSPN) crosses under the mandibular division of the trigeminal nerve (V3) and the foramen spinosum, laterally; by a line drawn between the foramen spinosum and the geniculate ganglion. Its base is the GSPN
Posteromedial triangle
The posteromedial triangle (Kawase´s triangle, Kawase-Shiobara´s triangle, and Kanzaki´s triangle) was first described by Kawase [15, 16]. This triangle consists of a line between the hiatus fallopii and the dural ostium of the Meckel’s cave. Its posterior border is a line between the posterior border of the mandibular nerve and the center of the geniculate ganglion 15. Several structures surround it; at its lateral apex are the cochlea and anterior wall of the internal auditory canal (IAC), its anterior margin, the petrous carotid, and its medial margin, the clivus, and inferior petrosal sinus [16]. It contains the posterior cavernous sinus and the entry point to the posterior fossa exposed by performing an anterior petrosectomy. [5, 14, 28, 29] (Figs. 1, 4, 5, 11) (Table 1).

Posteromedial triangle (Kawase, Kawase-Shiobara, Kanzaki); recent descriptions mentioned a quadrilateral. Its limits are; Laterally, the medial margin of the greater superficial petrosal nerve. Medially; the petrous ridge, anteriorly the mandibular (V3) division of the trigeminal nerve. Posteriorly, the arcuate eminence
Inferomedial paraclival triangle
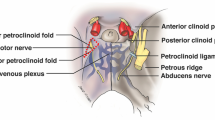
The infero-medial triangle is one of two paraclival triangles of the skull base. It is delimited medially by a line from the posterior clinoid process to the dural entry of the abducens nerve, laterally by a line from the posterior clinoid process to the dural entry of the trochlear nerve, and a base by a line from the dural entry of the abducens nerve and the trochlear nerve. Its contents are the posterior genu of the internal carotid artery and the dorsal meningeal artery [5, 6, 14, 32] (Figs. 4, 12) (Table 1).

Image depicting the paraclival triangles; Inferomedial and inferolateral. The inferomedial triangle is delimited by the posterior clinoid process, the trochlear nerve's dural entrance, and the abducens nerve's dural entrance. The inferolateral triangle is delimited anteriorly; by a line between the entry point of the trochlear nerve (CN IV) to the dural entry point of the abducens nerve (CN VI) at Dorello’s canal. Posteriorly, it’s bordered by a line between the dural entry point CN VI at Dorello’s canal and the superior petrosal vein at the superior petrosal sinus. Its superior border is the line drawn between the entry point of CN IV at the tentorium and the superior petrosal vein at the superior petrosal sinus
Inferolateral paraclival triangle
The inferolateral triangle consists anteriorly of a line from the abducens nerve's dural entry and the trochlear nerve's dural entry, laterally with a line from the entrance of the trochlear nerve and the petrosal vein, posteriorly with a line from the dural entry of the abducens nerve to the petrosal vein. Its contents are the porus trigeminus [5, 6, 14, 18] (Figs. 4, 12) (Table 1).
Discussion
Claudius Galen (119–199 a.d.), a confidant of royalty and physician to the gladiators, dissected animals and quietly transposed his findings to human anatomy. Those animals had parasellar carotid retia bathed in venous blood, which humans do not have. Winslow took it upon himself to name it ‘‘cavernous sinus’’ (CS), two sinus cavernosi, one on each side, two orbitary sinuses, one on each side, and all these sinuses communicate with each other, and with the great lateral sinuses [23].
He thought that it would resemble the corpus cavernosum of the penis, which, in turn, he imagined to be a large, single, trabeculated venous cavern. His presumed concept of a single, large, trabeculated venous cavern persists today, becoming the most extended enduring myth in medical science [23].
Wepfer, in 1658, described the intra-cavernous internal carotid artery as passing through deep and conspicuous space [31].
Dorland, in 1985, found in a case of a long-standing arteriovenous fistula that the engorged and thickened ‘‘arterialized’’ veins were readily noted to be neither cavernous nor a dural sinus but a plexus of veins [23].
Schafer and Thane, in 1849; Anson, in 1953; Ferner, in 1963; Netter, in 1953, with beautiful drawings, they depict a plexus and call it CS, Anson in 1953 drew a single channel and called it a “plexus,” Spalteholtz, in 1938, drew a plexus with extension along the carotid canal on one page and a single large cavern on another page both labeled CS, Ferner, in 1963 drew a plexus with the actual extensions and labeled it CS [23].
Hamby, in 1966; Knosp et al., in 1987; Parkinson, in 1972; Taptas, in 1949, called the term CS inappropriate [23].
In 1965, Parkinson, the first deviser of the triangular space around CS, described the triangle between the trochlear and ophthalmic nerves to safely approach a lesion located at the internal carotid artery. Since Parkinson, several studies by clinical anatomists and neurosurgeons devised the triangular spaces around the CS. Since his pioneering studies, several critical triangular relationships formed by the convergence and divergence of cranial nerves have been described in the CS, in the middle cranial fossa, and in the paraclival region. Parkinson proposed the replacement of the ‘‘parasellar plexus of veins’’ in the ‘‘lateral sellar compartment’’ with the “parasellar plexus” because the plexus is present from early fetal life onward (Knosp et al., 1987; Solasol et al., 1966) extends about the sella in front of, behind, and beneath the pituitary beyond the lateral sellar compartments [22].
Browder and Parkinson performed the first cavernous sinus approaches to treat carotid-cavernous fistula. [2]
Parkinson, Dolenc, Taptas, and Umansky were pioneers in describing the surgical entry points into the sinus as triangular corridors. This geometric construct has been adopted as nomenclature for the region by most neurosurgeons [27].
Currently, cavernous sinus approaches are performed for basilar tip aneurysms, carotid-ophthalmic aneurysms, pituitary adenomas, some trigeminal neuromas, and other tumors in the region [20].
Although the anatomy of the cavernous sinus has been well described, the sinus remains a challenging and unfamiliar place for many neurosurgeons.
Conclusion
Concise knowledge of the ten triangles is a strict requirement for any remarkable neurosurgeon. New surgical trans-triangle techniques or access pathways could be used to board different pathologies. We have left out measurements of each triangle to evade the premise of this simplified study. To thoroughly study each triangle profoundly, we advise you to investigate specific publications that only concentrate on each triangle or group of triangles.
Data availability
All data generated or analysed during this study are included in this published article.
Abbreviations
- CS:
-
Cavernous sinus
- GSPN:
-
Greater superior petrosal nerve
- ICA:
-
Internal carotid artery
- IAC:
-
Internal auditory canal
References
Al-Mefty O (1989) Surgery of the cranial base. Kluwer Academia Publishers, Boston
Browder J (1937) Treatment of carotid artery cavernous sinus fistula: report of a case. Arch Ophthalmol 18:95–102
Conti M, Prevedello DM, Madhok R, Faure A, Ricci UM, Schwarz A, Robert R, Kassam AB (2008) The antero-medial triangle: the risk for cranial nerves ischemia at the cavernous sinus lateral Wall. Anatomic cadaveric study. Clin Neurol Neurosurg 110(7):682–686
Day JD, Fukushima T, Giannotta SL (1996) Innovations in surgical approach: lateral cranial base approaches. Clin Neurosurg 43:72–90
Dolenc VV (2003) Microsurgical anatomy and surgery of the central skull base. Springer, Wien
Drazin D, Wang JM, Alonso F, Patel DM, Granger A, Shoja MM, Loukas M, Oskouian RJ, Tubbs RS (2017) intracranial anatomical triangles: a comprehensive illustrated review. Cureus 9(10):e1741
Escudeiro GP, Leal RTM, Leal da Silveira R, Landeiro JA (2019) Cavernous sinus hemangioma: surgical aspects. World Neurosurg 123:156
Ferrareze Nunes C, Lieber S, Truong HQ, Zenonos G, Wang EW, Snyderman CH, Gardner PA, Fernandez-Miranda JC (2018) Endoscopic endonasal transoculomotor triangle approach for adenomas invading the parapeduncular space: surgical anatomy, technical nuances, and case series. J Neurosurg: 1–11. (Advance online publication.)
Fujimoto Y, Ikeda H, Yamamoto S (1992) Pterional transcavernous approach for large basilar top aneurysm: significance of the exposure of Dolenc’s triangle. Surg Cereb Stroke 20:191–195
Gallardo FC, Bustamante JL, Martin C, Targa Garcia AA, Feldman SE, Pastor F, Orellana MC, Rubino PA, Quilis Quesada V (2021) Intra- and extradural anterior clinoidectomy: anatomy review and surgical technique step by step. Surg Radiol Anat SRA 43(8):1291–1303
Goel A (1997) The extradural approach to lesions involving the cavernous sinus. Br J Neurosurg 11(2):134–138
Granger A, Bricoune O, Rajnauth T, Kimball D, Kimball H, Tubbs RS, Loukas M (2018) Anterolateral triangle: a cadaveric study with neurosurgical significance. Cureus 10(2):e2185
Hakuba A, Tanaka K, Suzuki T, Nishimura S (1989) A combined orbitozygomatic infratemporal epidural and subdural approach for lesions involving the entire cavernous sinus. J Neurosurg 71(5 Pt 1):699–704
Isolan GR, Krayenbühl N, de Oliveira E, Al-Mefty O (2007) Microsurgical anatomy of the cavernous sinus: measurements of the triangles in and around it. Skull Base Off J North Am Skull Base Soc 17(6):357–367
Kawase T, Shiobara R, Toya S (1991) Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients. Neurosurgery 28(6):869–876
Kawase T, Toya S, Shiobara R, Mine T (1985) Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg 63(6):857–861
Kayalioglu G, Govsa F, Erturk M, Pinar Y, Ozer MA, Ozgur T (1999) The cavernous sinus: topographic morphometry of its contents. Surg Radiol Anat SRA 21(4):255–260
Kimball H, Kimball D, Blihar D, Zurada A, Tubbs RS, Loukas M (2021) The inferolateral surgical triangle of the cavernous sinus: a cadaveric and mri study with neurosurgical significance. World Neurosurg 149:e154–e159
Kobayashi S (2005) Neurosurgery of complex vascular lesions and tumors. Thieme, New York
Krisht A, Barnett DW, Barrow DL, Bonner G (1994) The blood supply of the intracavernous cranial nerves: an anatomic study. Neurosurgery 34(2):275–279
Kusumi M, Oka H, Aliabadi H, Sato S, Kumabe T (2016) The appropriate surgical approach to a greater petrosal nerve schwannoma in the setting of temporal lobe edema. World Neurosurg 85.
Parkinson D (1987) The cavernous sinus. In: Dolenc VV (ed) The cavernous sinus. Springer, New York, pp 3–29
Parkinson D (1998) Lateral sellar compartment O.T. (cavernous sinus): history, anatomy, terminology. Anatom Rec 251(4):486–490
Peltier J, Fichten A, Havet E, Foulon P, Page C, Le Gars D (2010) Microsurgical anatomy of the medial tentorial artery of Bernasconi–Cassinari. Surg Radiol Anat SRA 32(10):919–925
Quinones-Hinojosa A. (2012). Schmidek and Sweet - Operative Neurosurgical Techniques: Indications, Methods and Results. Elsevier - Health Sciences Division.
Rhoton AL (2002) The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery 51(suppl_4):S1-375
Umansky F, Nathan H (1982) The lateral wall of the cavernous sinus. With special reference to the nerves related to it. J Neurosurg 56(2):228–234
Wanibuchi M, Friedman A, Fukushima T (2011) Photo atlas of skull base dissection (1st ed.). Thieme.
Watanabe A, Nagaseki Y, Ohkubo S, Ohhashi Y, Horikoshi T, Nishigaya K, Nukui H (2003) Anatomical variations of the ten triangles around the cavernous sinus. Clin Anat (New York NY) 16(1):9–14
Watanabe K, Passeri T, Hanakita S, Giammattei L, Zomorodi AR, Fava A, Abbritti R, Labidi M, Champagne PO, Fukushima T, Froelich S (2021) Extradural anterior temporal fossa approach to the paranasal sinuses, nasal cavities through the anterolateral and anteromedial triangles: combined microscopic and endoscopic strategy. Acta Neurochir 163(8):2165–2175
Wepfer J (1675) Observaiones anatomicae, ex cadaveribus corum, quos sustulit apoplexia, cum exercitations de Ejus Loco Affecto. Schafhausen.
Wysiadecki G, Radek M, Tubbs RS, Iwanaga J, Walocha J, Brzeziński P, Polguj M (2021) Microsurgical anatomy of the inferomedial paraclival triangle: contents, topographical relationships and anatomical variations. Brain Sci 11(5):596
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors reviewed the manuscript. VRC-H: wrote the main manuscript and prepared all the documents. AC: contributed to the main manuscript. DBH: Prepared Figs. 1 and 5 and contributed to the main manuscript. BAS-B: contributed to the main manuscript. PAG-Z: contributed to the main manuscript. CAP-C: contributed to the main manuscript. EJV-P: contributed to the main manuscript. DTS-R: contributed to the main manuscript. LAC-A: contributed to the main manuscript. JJR-H: contributed to the main manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval and consent to participate
Ethical approval Anatomical study with cadaver heads and human subject approval was obtained from the Centre Hospitalier Universitaire Vaudois prior to the commencement of the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chavez-Herrera, V.R., Campero, Á., Ballesteros-Herrera, D. et al. Microsurgical and illustrative anatomy of the cavernous sinus, middle fossa, and paraclival triangles: a straightforward, comprehensive review. Surg Radiol Anat 45, 389–400 (2023). https://doi.org/10.1007/s00276-023-03105-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-023-03105-y